Lagged Association of Ambient Outdoor Air Pollutants with Asthma-Related Emergency Department Visits within the Pittsburgh Region

 ,
, 
 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
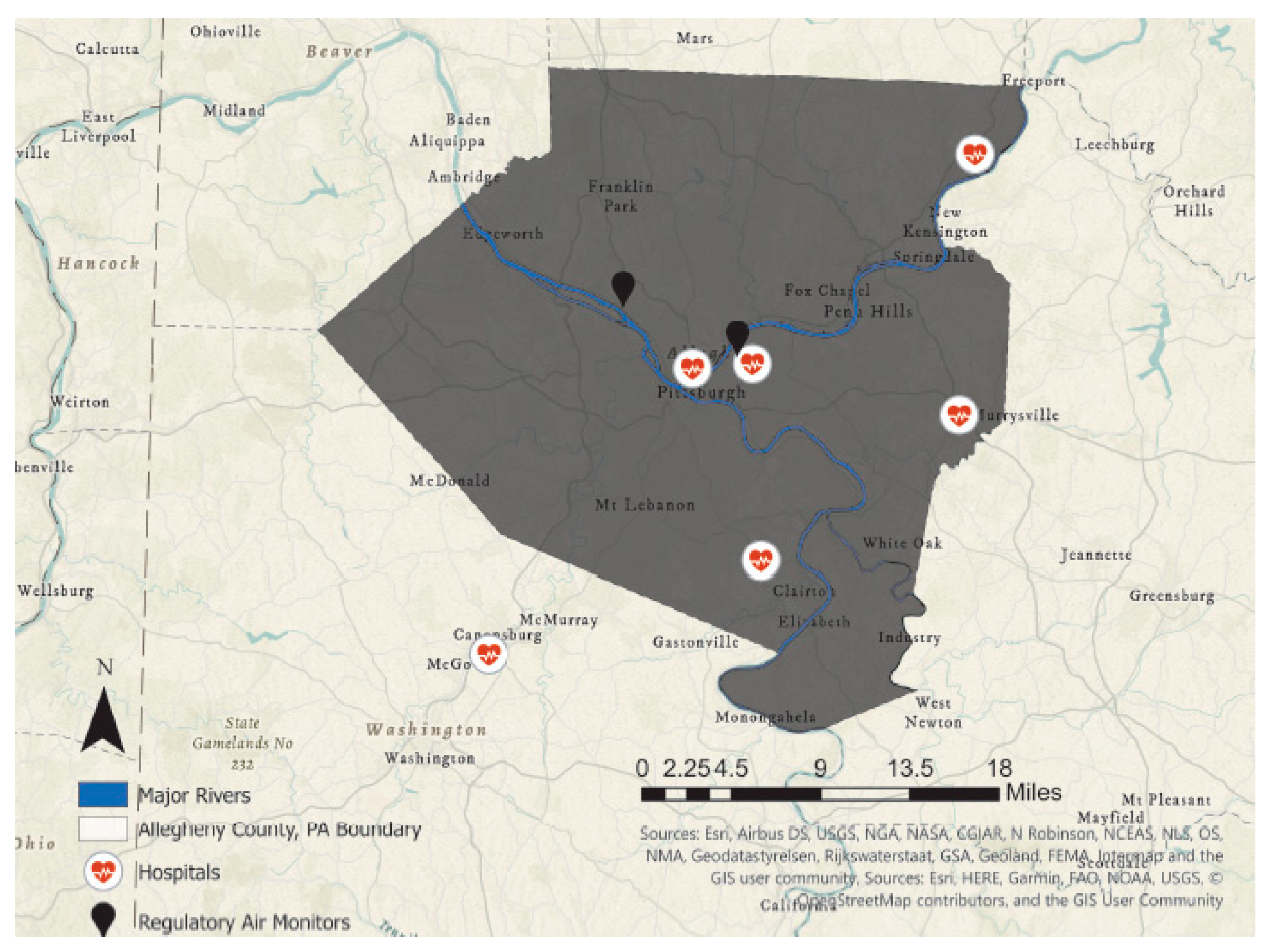
2.1. Environmental Exposure Measures
2.2. Statistical Analysis
3. Results
3.1. Air Pollution Data
3.2. Children Ages 5–17 Years
3.3. Adults Aged 18 Years and Older
3.4. Summary
4. Discussion
5. Study Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hamanaka, R.B.; Mutlu, G.M. Particulate Matter Air Pollution: Effects on the Cardiovascular System. Front. Endocrinol. Lausanne 2018, 9, 680. [Google Scholar] [CrossRef] [Green Version]
- Chen, R.; Peng, R.D.; Meng, X.; Zhou, Z.; Chen, B.; Kan, H. Seasonal variation in the acute effect of particulate air pollution on mortality in the China Air Pollution and Health Effects Study (CAPES). Sci. Total Environ. 2013, 450, 259–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuo, C.Y.; Chan, C.K.; Wu, C.Y.; Phan, D.; Van Chan, C.L. The short-term effects of ambient air pollutants on childhood asthma hospitalization in Taiwan: A national study. Int. J. Environ. Res. Public Health 2019, 16, 203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, H.R.; de Leon, A.P.; Bland, J.M.; Bower, J.S.; Emberlin, J.; Strachan, D.P. Air pollution, pollens, and daily admissions for asthma in London 1987–92. Thorax 1998, 53, 842–848. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peel, J.L.; Tolbert, P.E.; Klein, M.; Metzger, K.B.; Flanders, W.D.; Todd, K.; Mulholland, J.A.; Ryan, P.B.; Frumkin, H. Ambient air pollution and respiratory emergency department visits. Epidemiology 2005, 16, 164–174. [Google Scholar] [CrossRef]
- Strickland, M.J.; Darrow, L.A.; Klein, M.; Flanders, W.D.; Sarnat, J.A.; Waller, L.A.; Sarnat, S.E.; Mulholland, J.A.; Tolbert, P.E. Short-term associations between ambient air pollutants and pediatric asthma emergency department visits. Am. J. Respir. Crit. Care Med. 2010, 182, 307–316. [Google Scholar] [CrossRef] [Green Version]
- Barnett, G.A.; Williams, M.G.; Schwartz, J.; Neller, H.A.; Best, L.T.; Petroeschevsky, L.A.; Simpson, W.R. Air pollution and child respiratory health: A case-crossover study in Australia and New Zealand. Am. J. Respir. Crit. Care Med. 2005, 171, 1272–1278. [Google Scholar] [CrossRef]
- Zheng, X.Y.; Ding, H.; Jiang, L.N.; Chen, S.W.; Zheng, J.P.; Qiu, M.; Zhou, Y.X.; Chen, Q.; Guan, W.J. Association between Air pollutants and asthma emergency room visits and hospital admissions in time series studies: A systematic review and meta-Analysis. PLoS ONE 2015, 10, e0138146. [Google Scholar] [CrossRef]
- Son, J.Y.; Lee, J.T.; Park, Y.H.; Bell, M.L. Short-term effects of air pollution on hospital admissions in Korea. Epidemiology 2013, 24, 545–554. [Google Scholar] [CrossRef]
- Malig, B.J.; Pearson, D.L.; Chang, Y.B.; Broadwin, R.; Basu, R.; Green, R.S.; Ostro, B. A time-stratified case-crossover study of ambient ozone exposure and emergency department visits for specific respiratory diagnoses in California (2005–2008). Environ. Health Perspect. 2016, 124, 745–753. [Google Scholar] [CrossRef] [Green Version]
- Pereira, A.A.; Pollard, S.L.; Locke, R.; Romero, K.; Lima, J.J.; Hansel, N.N.; Checkley, W.; GASP Study Investigators. Association between exhaled carbon monoxide and asthma outcomes in Peruvian children. Respir. Med. 2018, 145, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.; Chen, Y.; Burnett, R.T.; Villeneuve, P.J.; Krewski, D. Effect of short-term exposure to gaseous pollution on asthma hospitalisation in children: A bi-directional case-crossover analysis. J. Epidemiol. Community Health 2003, 57, 50–55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodman, J.E.; Kennedy, E.M.; Seeley, M. Do individuals with asthma experience airway hyper-responsiveness after exposure to nitrogen dioxide? Regul. Toxicol. Pharmacol. 2017, 89, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Glad, J.A.; Brink, L.L.; Talbott, E.O.; Lee, P.C.; Xu, X.; Saul, M.; Rager, J. The relationship of ambient ozone and PM2.5 levels and asthma emergency department visits: Possible influence of gender and ethnicity. Arch. Environ. Occup. Heal. 2012, 67, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Pennsylvania-State of the Air | American Lung Association. Available online: http://www.stateoftheair.org/city-rankings/states/pennsylvania/ (accessed on 6 April 2020).
- Gharibi, H.; Entwistle, M.R.; Ha, S.; Gonzalez, M.; Brown, P.; Schweizer, D.; Cisneros, R. Ozone pollution and emergency department visits in the Central Valley, California, USA, during June to September of 2015: A time-stratified case-crossover analysis. J. Asthma 2019, 56, 1037–1048. [Google Scholar] [CrossRef]
- Fauroux, B.; Sampil, M.; Quénel, P.; Lemoullec, Y. Ozone: A trigger for hospital pediatric asthma emergency room visits. Pediatr. Pulmonol. 2000, 30, 41–46. [Google Scholar] [CrossRef]
- Gleason, J.A.; Fagliano, J.A. Associations of daily pediatric asthma emergency department visits with air pollution in Newark, NJ: Utilizing time-series and case-crossover study designs. J. Asthma 2015, 52, 815–822. [Google Scholar]
- Jaakkola, J.J.K. Case-crossover design in air pollution epidemiology. Eur. Respir. J. 2003, 21, 81–85. [Google Scholar] [CrossRef]
- Maclure, M. The Case-Crossover Design: A Method for Studying Transient Effects on the Risk of Acute Events. Am. J. Epidemiol. 1991, 133, 144–153. [Google Scholar] [CrossRef]
- Shmool, J.L.; Michanowicz, D.R.; Cambal, L.; Tunno, B.; Howell, J.; Gillooly, S.; Roper, C.; Tripathy, S.; Chubb, L.G.; Eisl, H.M.; et al. Saturation sampling for spatial variation in multiple air pollutants across an inversion-prone metropolitan area of complex terrain. Environ. Heal. A Glob. Access Sci. Source 2014, 13, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Larsen, L.C.; Shah, M. A context-intensive approach to imputation of missing values in data sets from networks of environmental monitors. J. Air Waste Manage. Assoc. 2016, 66, 38–52. [Google Scholar] [CrossRef] [PubMed]
- Junninen, H.; Niska, H.; Tuppurainen, K.; Ruuskanen, J.; Kolehmainen, M. Methods for imputation of missing values in air quality data sets. Atmos. Environ. 2004, 38, 2895–2907. [Google Scholar] [CrossRef]
- Plaia, A.; Bondì, A.L. Single imputation method of missing values in environmental pollution data sets. Atmos. Environ. 2006, 40, 7316–7330. [Google Scholar] [CrossRef]
- Le, H.Q.; Batterman, S.A.; Wahl, R.L. Reproducibility and imputation of air toxics data. J. Environ. Monit. 2007, 9, 1358–1372. [Google Scholar] [CrossRef] [PubMed]
- Teague, W.G.; Phillips, B.R.; Fahy, J.V.; Wenzel, S.E.; Fitzpatrick, A.M.; Moore, W.C.; Hastie, A.T.; Bleecker, E.R.; Meyers, D.A.; Peters, S.P.; et al. Baseline Features of the Severe Asthma Research Program (SARP III) Cohort: Differences with Age. J. Allergy Clin. Immunol. Pract. 2018, 6, 545–554.e4. [Google Scholar] [CrossRef]
- Hopke, P.K.; Croft, D.; Zhang, W.; Lin, S.; Masiol, M.; Squizzato, S.; Thurston, S.W.; van Wijngaarden, E.; Utell, M.J.; Rich, D.Q. Changes in the acute response of respiratory diseases to PM 2.5 in New York State from 2005 to 2016. Sci. Total Environ. 2019, 677, 328–339. [Google Scholar] [CrossRef] [PubMed]
- Anenberg, S.C.; Henze, D.K.; Tinney, V.; Kinney, P.L.; Raich, W.; Fann, N.; Malley, C.S.; Roman, H.; Lamsal, L.; Duncan, B.; et al. Estimates of the global burden of ambient PM2:5, ozone, and NO2 on asthma incidence and emergency room visits. Environ. Health Perspect. 2018, 126, 107004. [Google Scholar] [CrossRef] [Green Version]
- Krall, R.J.; Mulholland, A.J.; Russell, G.A.; Balachandran, S.; Winquist, A.; Tolbert, E.P.; Waller, A.L.; Sarnat, E.S. Associations between source-specific fine particulate matter and emergency department visits for respiratory disease in four U.S. cities. Environ. Health Perspect. 2017, 125, 97–103. [Google Scholar] [CrossRef]
- Esposito, S.; Tenconi, R.; Lelii, M.; Preti, V.; Nazzari, E.; Consolo, S.; Patria, M.F. Possible molecular mechanisms linking air pollution and asthma in children. BMC Pulm. Med. 2014, 14, 31. [Google Scholar] [CrossRef] [Green Version]
- Kuo, C.Y.; Pan, R.H.; Chan, C.K.; Wu, C.Y.; Phan, D.V.; Chan, C.L. Application of a time-stratified case-crossover design to explore the effects of air pollution and season on childhood asthma hospitalization in cities of differing urban patterns: Big data analytics of government open data. Int. J. Environ. Res. Public Health 2018, 15, 647. [Google Scholar] [CrossRef] [Green Version]
- Entwistle, M.R.; Gharibi, H.; Tavallali, P.; Cisneros, R.; Schweizer, D.; Brown, P.; Ha, S. Ozone pollution and asthma emergency department visits in Fresno, CA, USA, during the warm season (June–September) of the years 2005 to 2015: A time-stratified case-crossover analysis. Air Qual. Atmos. Health 2019, 1–12. [Google Scholar] [CrossRef]
- Analitis, A.; De’Donato, F.; Scortichini, M.; Lanki, T.; Basagana, X.; Ballester, F.; Astrom, C.; Paldy, A.; Pascal, M.; Gasparrini, A.; et al. Synergistic effects of ambient temperature and air pollution on health in europe: Results from the PHASE project. Int. J. Environ. Res. Public Health 2018, 15, 1856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, K.; Glonek, G.; Hansen, A.; Williams, S.; Tuke, J.; Salter, A.; Bi, P. The effects of air pollution on asthma hospital admissions in Adelaide, South Australia, 2003–2013: Time-series and case-crossover analyses. Clin. Exp. Allergy 2016, 46, 1416–1430. [Google Scholar] [CrossRef] [PubMed]
- Bateson, T.F.; Schwartz, J. Children’s response to air pollutants. J. Toxicol. Environ. Health Part A Curr. Issues 2008, 71, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Mirowsky, J.E.; Dailey, L.A.; Devlin, R.B. Differential expression of pro-inflammatory and oxidative stress mediators induced by nitrogen dioxide and ozone in primary human bronchial epithelial cells. Inhal. Toxicol. 2016, 28, 374–382. [Google Scholar] [CrossRef] [Green Version]
- Epidemiology, Pathophysiology, Clinical Evaluation, and Treatment of Carbon Monoxide Poisoning in Child, Infant, and Fetus. Available online: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pmc/articles/PMC5530151/ (accessed on 21 April 2020).
- Ryter, S.W.; Choi, A.M.K. Carbon Monoxide in Exhaled Breath Testing and Therapeutics. J. Breath Res. 2013, 7, 017111. [Google Scholar] [CrossRef] [Green Version]
- Canova, C.; Torresan, S.; Simonato, L.; Scapellato, M.L.; Tessari, R.; Visentin, A.; Lotti, M.; Maestrelli, P. Carbon monoxide pollution is associated with decreased lung function in asthmatic adults. Eur. Respir. J. 2010, 35, 266–272. [Google Scholar] [CrossRef]
- Halpin, D.M.; Meltzer, E.O.; Pisternick-Ruf, W.; Moroni-Zentgraf, P.; Engel, M.; Zaremba-Pechmann, L.; Casale, T.; FitzGerald, J.M. Peak expiratory flow as an endpoint for clinical trials in asthma: A comparison with FEV1. Respir. Res. 2019, 20, 159. [Google Scholar] [CrossRef] [Green Version]
- Evans, K.A.; Halterman, J.S.; Hopke, P.K.; Fagnano, M.; Rich, D.Q. Increased ultrafine particles and carbon monoxide concentrations are associated with asthma exacerbation among urban children. Environ. Res. 2014, 129, 11–19. [Google Scholar] [CrossRef] [Green Version]
- Chevalier, A.; Gheusi, F.; Delmas, R.; Ordóñez, C.; Sarrat, C.; Zbinden, R.; Thouret, V.; Athier, G.; Cousin, J.M. Atmospheric Chemistry and Physics Influence of altitude on ozone levels and variability in the lower troposphere: A ground-based study for western Europe over the period 2001–2004. Atmos. Chem. Phys 2007, 7, 4326. [Google Scholar] [CrossRef] [Green Version]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Byrwa-Hill, B.M.; Venkat, A.; Presto, A.A.; Rager, J.R.; Gentile, D.; Talbott, E. Lagged Association of Ambient Outdoor Air Pollutants with Asthma-Related Emergency Department Visits within the Pittsburgh Region. Int. J. Environ. Res. Public Health 2020, 17, 8619. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228619
Byrwa-Hill BM, Venkat A, Presto AA, Rager JR, Gentile D, Talbott E. Lagged Association of Ambient Outdoor Air Pollutants with Asthma-Related Emergency Department Visits within the Pittsburgh Region. International Journal of Environmental Research and Public Health. 2020; 17(22):8619. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228619
Chicago/Turabian StyleByrwa-Hill, Brandy M., Arvind Venkat, Albert A. Presto, Judith R. Rager, Deborah Gentile, and Evelyn Talbott. 2020. "Lagged Association of Ambient Outdoor Air Pollutants with Asthma-Related Emergency Department Visits within the Pittsburgh Region" International Journal of Environmental Research and Public Health 17, no. 22: 8619. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17228619