The Microbial Quality and Safety of Blenderised Enteral Nutrition Formula: A Systematic Review

 , ,
, ,
Abstract
:1. Introduction
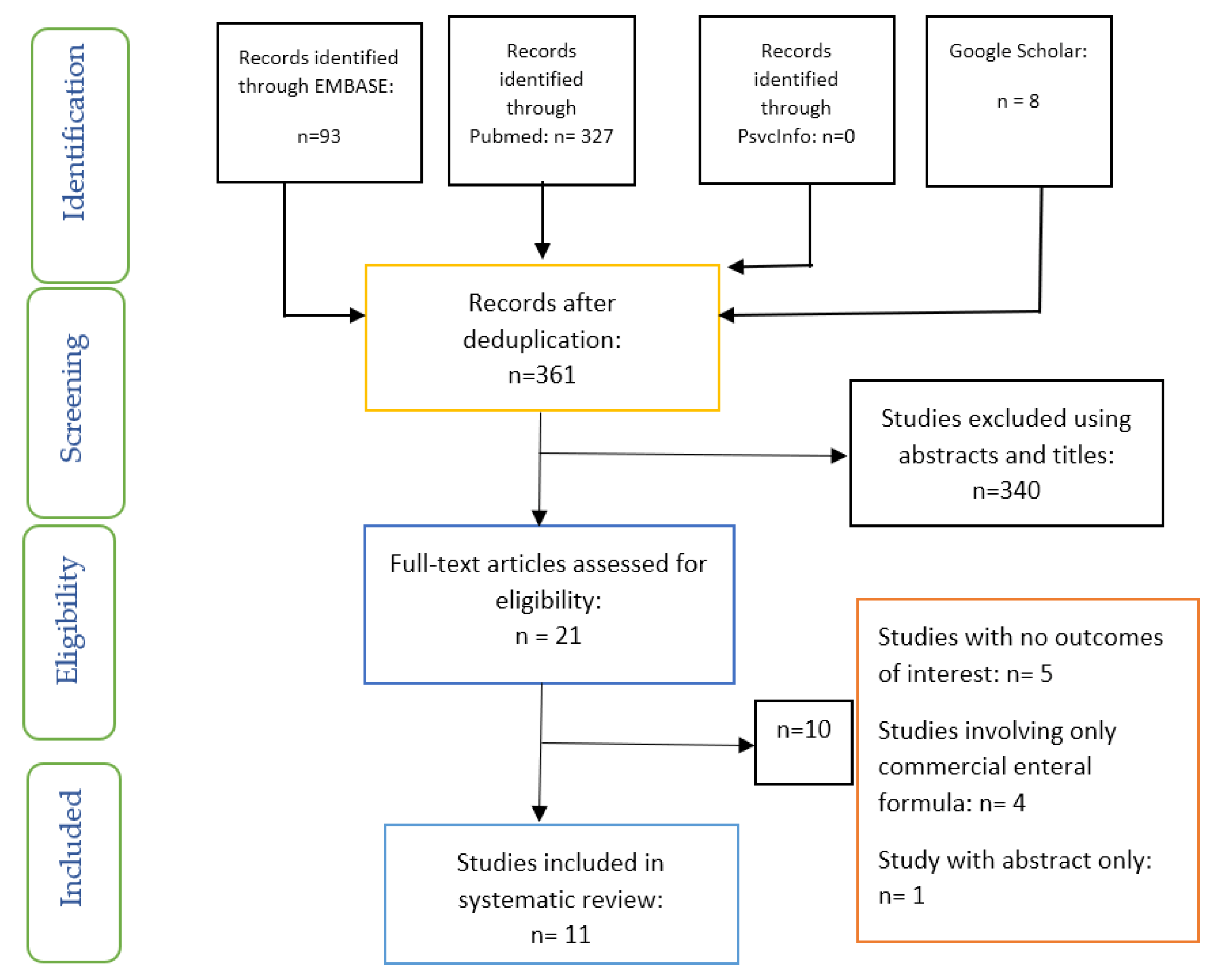
2. Methods
3. Types of Studies and Samples
4. Inclusion and Exclusion Criteria
5. Type of Intervention
6. Types of Outcome Measures
Primary Outcomes
7. Search Strategy
8. Data Extraction
9. Evaluation of Quality
10. Results
10.1. The Effect of Storage Time on Microbial Quality of Blenderised ENF
10.2. Microbial Quality of Blenderised ENF versus Commercial ENF
11. Discussion
12. Limitations
13. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
| Vieira et al., 2016 | |
|---|---|
| 1. Were the criteria for inclusion in the sample clearly defined? | YES |
| 2. Were the study subjects and the setting described in detail? | YES—commercial and non-commercial enteral feeds |
| 3. Was the exposure measured in a valid and reliable way? | NOT APPLICABLE |
| 4. Were objective, standard criteria used for measurement of the condition? | YES |
| 5. Were confounding factors identified? | NO |
| 6. Were strategies to deal with confounding factors stated? | NOT APPLICABLE |
| 7. Were the outcomes measured in a valid and reliable way? | YES |
| 8. Was an appropriate statistical analysis used? | YES |
References
- National Collaborating Centre for Acute Care. Nutrition Support in Adults Oral Nutrition Support, Enteral Tube Feeding and Parenteral Nutrition. 2006. Available online: https://www.nice.org.uk/guidance/cg32/evidence/full-guideline-194889853 (accessed on 13 June 2020).
- Ojo, O. Enteral feeding for nutritional support in critically ill patients. Br. J. Nurs. 2017, 26, 666–669. [Google Scholar] [CrossRef] [Green Version]
- Jazayeri, S.M.H.; Ostadrahimi, A.; Safaiyan, A.; Hashemzadeh, S.; Salehpour, F. Standard Enteral Feeding Improves Nutritional Status Compared with Hospital-Prepared Blended Formula Among Intensive Care Unit (ICU) Patients. Prog. Nutr. 2016, 18, 22–25. Available online: https://mattioli1885journals.com/index.php/progressinnutrition/article/view/4308 (accessed on 21 June 2020).
- Zadák, Z.; Kent-Smith, L. Basics in clinical nutrition: Commercially prepared formulas. e-SPEN Eur. e-J. Clin. Nutr. Metab. 2009, 4, e212–e215. [Google Scholar] [CrossRef]
- NICE. Healthcare-Associated Infections: Prevention and Control in Primary and Community Care. 2012. Available online: https://www.nice.org.uk/guidance/cg139 (accessed on 1 June 2020).
- Hurt, R.T.; Varayil, J.E.; Epp, L.M.; Pattinson, A.K.; Lammert, L.M.; Lintz, J.E.; Mundi, M.S. Blenderized Tube Feeding Use in Adult Home Enteral Nutrition Patients. Nutr. Clin. Pr. 2015, 30, 824–829. [Google Scholar] [CrossRef]
- Ma, R.K.M.; Gardner, G. Home Enteral Nutrition: Updates, Trends, and Challenges. Nutr. Clin. Pr. 2017, 32, 712–721. [Google Scholar] [CrossRef]
- Sullivan, M.M.; Sorreda-Esguerra, P.; Platon, M.B.; Castro, C.G.; Chou, N.R.; Shott, S.; Comer, G.M.; Alarcon, P. Nutritional analysis of blenderized enteral diets in the Philippines. Asia Pac. J. Clin. Nutr. 2004, 13, 385–391. [Google Scholar]
- Brown, S. Guidelines on blended diet. Nurs. Child. Young People 2015, 27, 14–15. [Google Scholar] [CrossRef]
- Azadbakht, L.; Jolfaie, N.R.; Rouhani, M.H.; Mirlohi, M.; Babashahi, M.; Abbasi, S.; Adibi, P.; Esmaillzadeh, A. Comparison of Energy and Nutrient Contents of Commercial and Noncommercial Enteral Nutrition Solutions. Adv. Biomed. Res. 2017, 6, 131. [Google Scholar] [CrossRef]
- Bennett, K.; Hjelmgren, B.; Piazza, J. Blenderized Tube Feeding: Health Outcomes and Review of Homemade and Commercially Prepared Products. Nutr. Clin. Pr. 2020, 35, 417–431. [Google Scholar] [CrossRef]
- Pentiuk, S.; O’Flaherty, T.; Rd, K.S.; Willging, P.; Kaul, A. Pureed by Gastrostomy Tube Diet Improves Gagging and Retching in Children with Fundoplication. J. Parenter. Enter. Nutr. 2011, 35, 375–379. [Google Scholar] [CrossRef]
- Gallagher, K.; Flint, A.; Mouzaki, M.; Carpenter, A.; Haliburton, B.; Bannister, L.; Norgrove, H.; Hoffman, L.; Mack, D.; Stintzi, A.; et al. Blenderized Enteral Nutrition Diet Study: Feasibility, Clinical, and Microbiome Outcomes of Providing Blenderized Feeds Through a Gastric Tube in a Medically Complex Pediatric Population. J. Parenter. Enter. Nutr. 2018, 42, 1046–1060. [Google Scholar] [CrossRef]
- Ojo, O.; Feng, Q.-Q.; Ojo, O.O.; Wang, X.-H. The Role of Dietary Fibre in Modulating Gut Microbiota Dysbiosis in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Nutrients 2020, 12, 3239. [Google Scholar] [CrossRef]
- Carter, H.; Johnson, K.; Johnson, T.W.; Spurlock, A. Blended tube feeding prevalence, efficacy, and safety: What does the literature say? J. Am. Assoc. Nur. Pract. 2018, 30, 150–157. [Google Scholar] [CrossRef]
- Epp, L.; Lammert, L.; Vallumsetla, N.; Hurt, R.T.; Mundi, M.S. Use of Blenderized Tube Feeding in Adult and Pediatric Home Enteral Nutrition Patients. Nutr. Clin. Pr. 2016, 32, 201–205. [Google Scholar] [CrossRef]
- Madden, A.; Baines, S.; Bothwell, S.; Chen, E.; Goh, S.; Jerome, L.; Sommariva-Nagle, C.; Szychta, M. A laboratory-based evaluation of tube blocking and microbial risks associated with one blended enteral feed recipe. J. Hum. Nutr. Diet. 2019, 32, 667–675. [Google Scholar] [CrossRef]
- Bischoff, S.C.; Austin, P.; Boeykens, K.; Chourdakis, M.; Cuerda, C.; Jonkers-Schuitema, C.; Lichota, M.; Nyulasi, I.; Schneider, S.M.; Stanga, Z.; et al. ESPEN guideline on home enteral nutrition. Clin. Nutr. 2020, 39, 5–22. [Google Scholar] [CrossRef] [Green Version]
- Ojo, O.; Bowden, J. Infection control in enteral feed and feeding systems in the community. Br. J. Nurs. 2012, 21, 1070–1075. [Google Scholar] [CrossRef]
- Jalali, M.; Sabzghabaee, A.M.; Badri, S.S.; Soltani, H.A.; Maracy, M.R. Bacterial contamination of hospital-prepared enteral tube feeding formulas in Isfahan, Iran. J. Res. Med. Sci. 2009, 14, 149–156. [Google Scholar]
- Patchell, C.J.; Anderton, A.; Holden, C.; Macdonald, A.; George, R.H.; Booth, I.W. Reducing bacterial contamination of enteral feeds. Arch. Dis. Child. 1998, 78, 166–168. [Google Scholar] [CrossRef] [Green Version]
- Health Protection Agency. Health Protection in the 21st Century-Understanding the Burden of Disease; HPA: London, UK, 2005. [Google Scholar]
- Gill, K.J.; Gill, P. Contaminated enteral feeds. Br. Med. J. 1981, 282, 1971. [Google Scholar] [CrossRef] [Green Version]
- Borghi, R.; Araujo, T.D.; Vieira, R.I.A.; De Souza, T.T.; Waitzberg, D.L. ILSI Task Force on enteral nutrition; estimated composition and costs of blenderized diets. Nutr. Hosp. 2013, 28, 2033–2038. [Google Scholar]
- Johnson, T.W.; Milton, D.L.; Johnson, K.; Carter, H.; Hurt, R.T.; Mundi, M.S.; Epp, L.; Spurlock, A.L. Comparison of Microbial Growth Between Commercial Formula and Blenderized Food for Tube Feeding. Nutr. Clin. Pr. 2019, 34, 257–263. [Google Scholar] [CrossRef]
- Moazen, M.; Rahmdel, S.; Abdollahzadeh, S.M.; Ranjbar Zahedani, M.; Mazloomi, S.M. Microbiological quality of commercial enteral feedings used in two public hospitals in Shiraz, Iran. J. Health Sci. Surveill. System. 2014, 2, 49–53. [Google Scholar]
- Morrow, E.; Griffiths, P.; Rao, G.G.; Flaxman, D. “Somebody else’s problem?” Staff perceptions of the sources and control of meticillin-resistant Staphylococcus aureus. Am. J. Infect. Control. 2010, 39, 284–291. [Google Scholar] [CrossRef]
- Milton, D.L.; Johnson, T.W.; Johnson, K.; Murphy, B.; Carter, H.; Hurt, R.T.; Mundi, M.S.; Epp, L.; Spurlock, A.Y.; Hussey, J. Accepted Safe Food-Handling Procedures Minimizes Microbial Contamination of Home-Prepared Blenderized Tube-Feeding. Nutr. Clin. Pr. 2020, 35, 479–486. [Google Scholar] [CrossRef]
- Mahinkazemi, M.; Tarighat-Esfanjani, A.; Safaiyan, A. Bacterial contamination and nutritional adequacy of enteral tube feedings in Iran. Prog. Nutr. 2017, 19, 283–290. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Methley, A.M.; Campbell, S.M.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; et al. Chapter 7: Systematic Reviews of Etiology and Risk. 2017. Available online: https://reviewersmanual.joannabriggs.org/ (accessed on 2 May 2020).
- Arias, M.L.; Monge, R.; Chávez, C. Microbiological contamination of enteral feeding solutions used in Costa Rican hospitals. Arch. Latinoam. Nutr. 2003, 53, 277–281. [Google Scholar]
- Baniardalan, M.; Sabzghabaee, A.M.; Jalali, M.; Badri, S. Bacterial Safety of Commercial and Handmade Enteral Feeds in an Iranian Teaching Hospital. Int. J. Prev. Med. 2014, 5, 604–610. [Google Scholar]
- Mokhalalati, J.K.; Druyan, M.E.; Shott, S.B.; Comer, G.M. Microbial, nutritional and physical quality of commercial and hospital prepared tube feedings in Saudi Arabia. Saudi Med. J. 2004, 25, 331–341. [Google Scholar] [PubMed]
- Pinto, R.O.M.; Correia, E.F.; Pereira, K.C.; Sobrinho, P.D.S.C.; Da Silva, D.F.; Costa, P.D.S. Microbiological quality and safe handling of enteral diets in a hospital in Minas Gerais, Brazil. Braz. J. Microbiol. 2015, 46, 583–589. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, M.; Sorreda-Esguerra, P.; Santos, E.; Platon, B.; Castro, C.; Idrisalman, E.; Chen, N.; Shott, S.; Comer, G. Bacterial contamination of blenderized whole food and commercial enteral tube feedings in the Philippines. J. Hosp. Infect. 2001, 49, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Vieira, M.M.C.; Santos, V.F.N.; Bottoni, A.; Morais, M.B. Nutritional and microbiological quality of commercial and homemade blenderized whole food enteral diets for home-based enteral nutritional therapy in adults. Clin. Nutr. 2018, 37, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Anderton, A.; Howard, J.P.; Scott, D.W. Microbiological control in enteral feeding. Summary of a guidance document prepared on behalf of the Committee of the Parenteral and Enteral Nutrition Group of the British Dietetic Association. Hum. Nutr. Appl. Nutr. 1986, 40, 163–167. [Google Scholar]
- Bankhead, R.; Boullata, J.I.; Brantley, S.; Corkins, M.; Guenter, P.; Krenitsky, J.; Lyman, B.; Metheny, N.A.; Mueller, C.; Robbins, S.; et al. A.S.P.E.N. Enteral Nutrition Practice Recommendations. J. Parenter. Enter. Nutr. 2009, 33, 122–167. [Google Scholar] [CrossRef] [Green Version]

| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Population or Problem | Patients (adults) on blended tube feeding or blenderised enteral nutrition formula | Studies involving children aged below 18 years |
| Intervention | Blended enteral nutrition formula at 0 h time point | Individuals on normal oral dietary intake |
| Comparator | Commercial enteral nutrition formula or Blended enteral nutrition formula at later h time point | Parenteral nutrition, parenteral plus enteral nutrition |
| Outcomes | Primary Outcomes: a. Microbial counts of bacteria contamination in blenderised ENF and commercial ENF; b. Microbial counts of bacteria contamination in blenderised ENF over time. | Qualitative outcomes such as patient feelings |
| Types of Study | Quantitative studies | Letters, comments, reviews, qualitative studies |
| Citation | Country | Aim/Objective of Study | Study Design | Study Method/Sample Size/Description | Age (Years) | Study Results/Conclusion |
|---|---|---|---|---|---|---|
| Arias et al. [33] | Costa Rica | To assess the level of microbial contamination in enteral feeds in hospitals. | In-vitro experimental study | A total of 124 enteral feeding solutions were assessed. Overall, 50% of the samples were made from commercial formula (Ensure®) and the remaining 50% were solutions prepared at the nutritional hospital services. | Not Applicable | The level of gram-negative bacteria in the enteral feed samples varied from 103 to 107 CFU/mL. Enterobacter cloacae, Escherichia coli, Serratia sp. and Klebsiella pnuemoniae were the most frequently isolated coliforms. Pseudomonas sp. was isolated in more than 70% of the samples made from commercial solutions, fruits and vegetables. |
| Baniardalan et al. [34] | Iran | To evaluate and compare the bacteria safety of hand-made blenderised ENF and commercial ENF. | In-vitro experimental study | Seventy samples including 21 handmade formulas sampled at two sampling times (the time of preparation and 18 h after preparation, and 28 commercial ENF) were studied. | Not Applicable | The microbial safety of enteral feeding solutions in this hospital was found to be much lower than the standard values. |
| Jalali et al. [20] | Iran | To evaluate the microbial quality of blenderized ENF in two university hospitals. | In-vitro experimental study | A total of 152 samples (76 samples each at the time of preparation and 18 h following preparation) were collected. Standard plate count, coliform count and Staphylococcus aureus count in all samples were conducted. The presence of Salmonella spp. and Listeria spp. were also examined. | Not Applicable | It was found that most of the BTF in the hospitals were not safe. Compared to standard levels, the BTFs were found to be highly contaminated and this could be a source of significant risk in the development of food-borne disease or nosocomial infection. |
| Johnson et al. [25] | USA | To compare microbial levels of a standard commercial formula (CF), a BTF made using baby food (BTF-BF), and a BTF prepared from blending whole food (BTF-WF). | In-vitro experimental study | Three tube-feeding formulas (CF, BTF-BF, BTF-WF) were compared for the growth of aerobic microorganisms, S. aureus, coliforms, and E. coli, at zero hour, 2 h, and 4 h after tube feed preparation. | Not Applicable | It was found that BTF recipe selection and adherence to safe food handling provide a safe feeding that is comparable to CF in the hospital setting. |
| Madden et al. [17] | UK | To examine the risks of blended feed in providing nutritionally adequate intake. | In-vitro experimental study | The blended feed was made using three different methods (professional, jug and stick blenders) and three storage procedures. Feed samples were diluted and bacterial colony-forming units (CFU) were counted. | Not Applicable | The level of bacterial contamination was a concern. However, this was not due to the methods of preparation or storage used. |
| Milton et al. [28] | USA | To examine the procedure for minimising bacterial growth of BTF. | In-vitro experimental study | BTF was assessed for the growth of aerobic microorganisms including; Escherichia coli, Staphylococcus aureus, and coliforms at baseline, 24-h, and 48-h intervals after preparation for a total of 150 colony forming units (CFU) counts performed. | Not Applicable | It was concluded that safe food-handling procedures can reduce bacterial contamination of BTF and can also reduce the risk of food-borne infection in HEN patients. |
| Mahinkazemi et al. [29] | Iran | To examine bacterial contaminations of enteral feeding (EF). | In-vitro experimental study | A total of 54 EF samples; 36 blenderised tube feedings (BTFs) and 18 commercial powder feedings (CPFs) of patients in the intensive care units were examined. | Not Applicable | The issues of quality, safety, and the appropriate type of enteral nutrition formulas are essential based on the bacterial contamination of CPFs. |
| Mokhalalati et al. [35] | Saudi Arabia | To compare the microbial safety of BTF and commercially prepared formulas (CPF). | In-vitro experimental study | Eighteen samples of BTF were collected from 3 hospitals. Samples of a CPF were also collected for comparison. | Not Applicable | BTFs are highly contaminated and may increase the risk of nosocomial infections. |
| Pinto et al. [36] | Brazil | To assess the microbiological quality and aseptic conditions in the preparation and administration of handmade and commercial ENF. | In-vitro experimental study | Twenty-five samples of enteral diets were analysed, 13 of them were non-industrialized diets (prepared in the hospital facility) and 12 were industrialized diets, collected in two different times (immediately after the completion preparation (T0) and after administration to the patient (T1). There were 50 sample units, each of them containing at least100 mL of the diet. | Not Applicable | The microbial quality of the enteral feeds was not satisfactory. The aseptic conditions in the hospital concerning preparation and handling of enteral diets increases the risks of cross-contamination. |
| Sullivan et al. [37] | Philippines | To assess the microbial quality of BTF. | In-vitro experimental study | Two feedings were prepared on three separate days at four hospitals. The tube feedings were either blended foods or commercial products. Samples of each feeding were collected for coliform count and standard plate count at the time of preparation and different times after preparation. | Not Applicable | The microbial quality of most of the hospital-prepared enteral tube feedings was not within the published guidelines for microbial safety. |
| Vieira et al. [38] | Brazil | To evaluate the microbial quality of commercial ENF and blenderised whole foods ENF. | Cross-sectional study | A total of 66 samples of commercial (CD, n = 33) and noncommercial (NCD, n = 33) enteral diets were collected at the homes of patients on HEN. | 73 years (20–100 years) | The homemade blenderised ENF contained high levels of bacterial contamination. |
| Citation | Level of Microbial Contamination of Blenderised ENF | Level of Microbial Contamination of Commercial ENF | Comments |
|---|---|---|---|
| Arias et al. [33] | ↑ | ↑ | The concentration of gram negative rods found in the samples of enteral feeding solutions ranged from 103 to 107 CFU/mL, significantly exceeding the permissible level (102 CFU/mL or less). There were no differences in the levels of contamination of the formulas. Blenderised ENF made from fruits or cooked vegetables showed contamination levels as high as the ones present in the commercial based solutions (Ensure®). |
| Baniardalan et al. [34] | ↑ | ↑ | The contamination of commercial formulas in all three microbiological samples was significantly more than that for handmade samples. Overall, 76% of handmade samples had total viable counts greater than 103 CFU/g compared to 96% of commercial formulas at the time of preparation. |
| Jalali et al. [20] | ↑ | Not Applicable | In the standard plate count, 97% of the samples had counts greater than 103 CFU/g, while 71% had counts greater than 104 CFU/g at the time of preparation. |
| Johnson et al. [25] | Total bacterial count was well below acceptable limits | Total bacterial count was well below acceptable limits | All 3 feeding formulas at zero hour, 2 h, and 4 h for each of the 3 sampling dates were acceptable for human consumption. |
| Madden et al. [17] | ↑ | Not Applicable | The bacterial load of Enterobacteriaceae of approximately half of the blended feeds was categorised as unsatisfactory (i.e., CFU/g > 104), with no clear pattern of association with preparation or storage method. |
| Milton et al. [28] | At time of preparation and after 24 h, 10% had a CFU count of >104, and, at 48 h, 12% exceeded 104 CFUs. | Not Applicable | The result showed that 88% of the samples met the US Food Code criteria for safe food consumption; 10.7% met guidelines for marginal safety by other standards; and 1.3% slightly exceeded 105 CFUs. |
| Mahinkazemi et al. [29] | Bacterial contamination (S. aureus, coliform) of blenderised ENF at the time of preparation and 18 h after preparation were <101 CFU and <2 MPN/g, respectively. | Overall, 33% of commercial ENF which were prepared in the wards had coliform contamination of 6.41 ± 2.43 MPN/g and E. coli was detected. | The presence of E. coli and coliforms in 33.3% of commercial ENF showed that these were at an unacceptable level of contamination. |
| Mokhalalati et al. [35] | ↑ | ↓ | Overall, 86% of standard blenderised ENF and therapeutic blenderised ENF had Aerobic Plate Count (APC) >104 CFU/g, while for all commercial ENFs, APC was not detectable (<10 CFU/g) at all times. The maximum coliform count for any blenderised ENF sample from sites 1 and 2 was 50 CFU/g. Coliform counts for all Commercial ENFs were non detectable (<10 CFU/g). |
| Pinto et al. [36] | ↑ | ↑ | Both kinds of blenderised ENF and commercial ENF showed contamination by coliforms and Pseudomonas spp. Listeria spp. was detected in only one sample of handmade diets. However, contamination was significantly higher in the blenderised ENF (p < 0.05) compared with Commercial ENF. |
| Sullivan et al. [37] | ↑ | Not Applicable | Overall, 38% of blenderised ENF had coliform counts greater than 10 MPN/g, and 92% of the samples had standard plate counts greater than 103 CFU/g. There were significant increases in mean coliform and standard plate counts over 4 h. |
| Vieira et al. [38] | ↑ | Samples of powder commercial ENF complied less when compared to liquid commercial ENF. | Only 6% of samples of blenderised ENF met the standard for coliform. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ojo, O.; Adegboye, A.R.A.; Ojo, O.O.; Wang, X.; Brooke, J. The Microbial Quality and Safety of Blenderised Enteral Nutrition Formula: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 9563. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249563
Ojo O, Adegboye ARA, Ojo OO, Wang X, Brooke J. The Microbial Quality and Safety of Blenderised Enteral Nutrition Formula: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(24):9563. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249563
Chicago/Turabian StyleOjo, Omorogieva, Amanda Rodrigues Amorim Adegboye, Osarhumwese Osaretin Ojo, Xiaohua Wang, and Joanne Brooke. 2020. "The Microbial Quality and Safety of Blenderised Enteral Nutrition Formula: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 24: 9563. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249563