Is Environmental and Occupational Particulate Air Pollution Exposure Related to Type-2 Diabetes and Dementia? A Cross-Sectional Analysis of the UK Biobank




Abstract
:1. Introduction
2. Materials and Methods
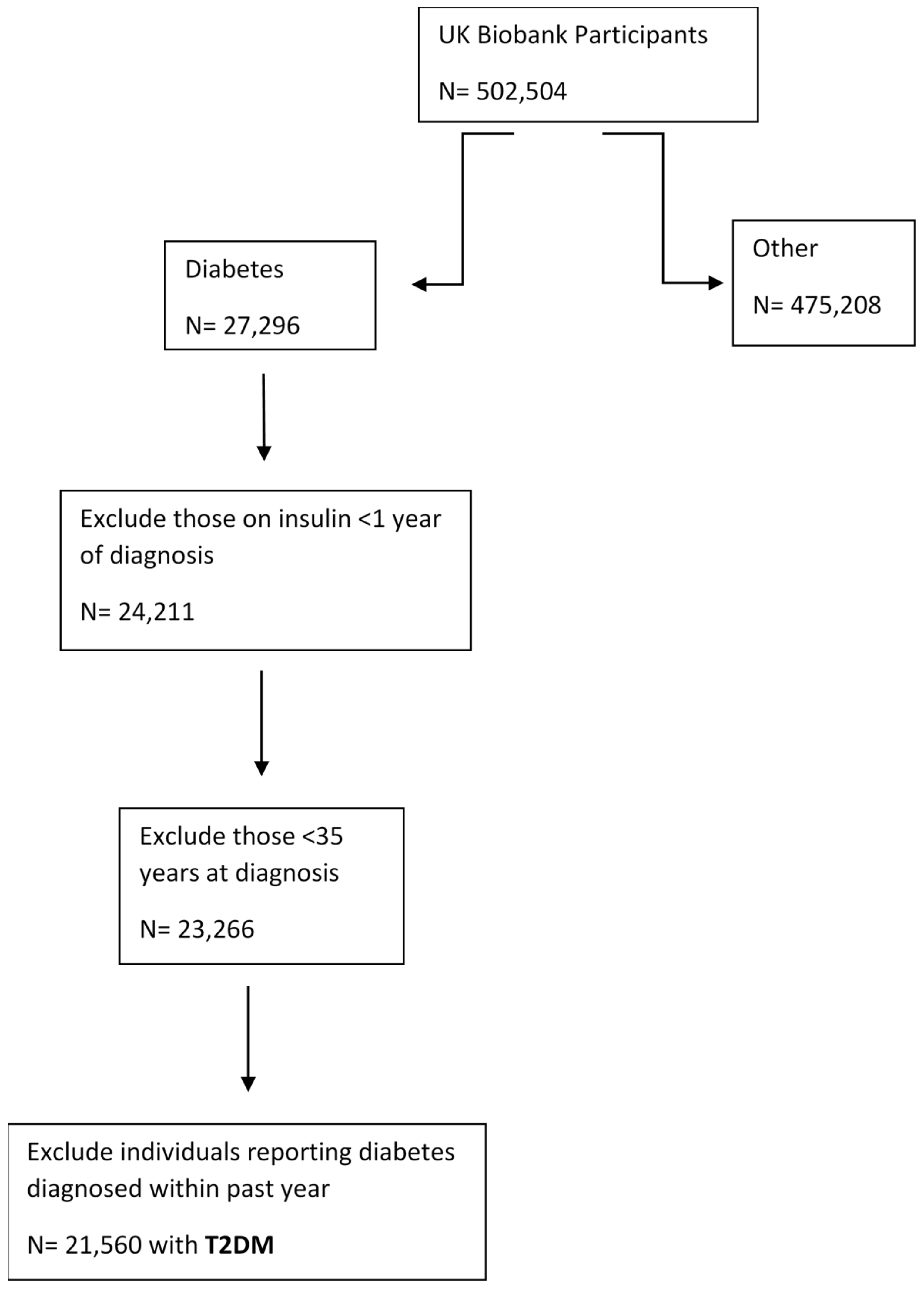
2.1. Population and Study Design
2.2. Disease Categories
2.3. Environmental and Occupational Variables
2.4. Occupational Variables and ACE JEM
2.5. Covariates
2.6. Statistical Analyses
2.7. Sensitivity Analyses
3. Results
3.1. Characteristics of the Study Population
3.2. Association between Particulate Air Pollution (PM2.5) and T2DM and Dementia
3.3. Association between Occupational Exposure and T2DM and Dementia
3.4. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Stone, V.; Miller, M.R.; Clift, M.J.D.; Elder, A.; Mills, N.L.; Moller, P.; Schins, R.P.F.; Vogel, U.; Kreyling, W.G.; Alstrup Jensen, K.; et al. Nanomaterials Versus Ambient Ultrafine Particles: An Opportunity to Exchange Toxicology Knowledge. Environ. Health Perspect. 2017, 125, 106002. [Google Scholar] [CrossRef] [PubMed]
- Jovanovic-Andersen, Z. Health effects of long-term exposure to air pollution: An overview of major respiratory and cardiovascular diseases and diabetes. Chem. Ind. Chem. Eng. Q. 2012, 18, 617–622. [Google Scholar] [CrossRef]
- WHO. Air Pollution and Cancer; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- Donaldson, K.; Stone, V. Current hypotheses on the mechanisms of toxicity of ultrafine particles. Annali Dell’Istituto Superiore Di Sanita 2003, 39, 405–410. [Google Scholar]
- Eze, I.C.; Schaffner, E.; Fischer, E.; Schikowski, T.; Adam, M.; Imboden, M.; Tsai, M.; Carballo, D.; von Eckardstein, A.; Kunzli, N.; et al. Long-term air pollution exposure and diabetes in a population-based Swiss cohort. Environ. Int. 2014, 70, 95–105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teichert, T.; Vossoughi, M.; Vierkotter, A.; Sugiri, D.; Schikowski, T.; Schulte, T.; Roden, M.; Luckhaus, C.; Herder, C.; Kramer, U. Association between traffic-related air pollution, subclinical inflammation and impaired glucose metabolism: Results from the SALIA study. PLoS ONE 2013, 8, e83042. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.; Bai, Y.; Xu, X.; Sun, L.; Wang, A.; Wang, T.Y.; Maurya, S.K.; Periasamy, M.; Morishita, M.; Harkema, J.; et al. Exaggerated effects of particulate matter air pollution in genetic type II diabetes mellitus. Part Fibre Toxicol. 2014, 11, 27. [Google Scholar] [CrossRef] [Green Version]
- Jung, C.R.; Lin, Y.T.; Hwang, B.F. Ozone, particulate matter, and newly diagnosed Alzheimer’s disease: A population-based cohort study in Taiwan. J. Alzheimer’s Dis. JAD 2015, 44, 573–584. [Google Scholar] [CrossRef] [Green Version]
- Moulton, P.V.; Yang, W. Air pollution, oxidative stress, and Alzheimer’s disease. J. Environ. Public Health 2012, 2012, 472751. [Google Scholar] [CrossRef]
- Calderon-Garciduenas, L.; Franco-Lira, M.; Mora-Tiscareno, A.; Medina-Cortina, H.; Torres-Jardon, R.; Kavanaugh, M. Early Alzheimer’s and Parkinson’s disease pathology in urban children: Friend versus Foe responses—It is time to face the evidence. Biomed. Res. Int. 2013, 2013, 161687. [Google Scholar] [CrossRef]
- Dimakakou, E.; Johnston, J.H.; Streftaris, G.; Cherrie, W.J. Exposure to Environmental and Occupational Particulate Air Pollution as a Potential Contributor to Neurodegeneration and Diabetes: A Systematic Review of Epidemiological Research. Int. J. Environ. Res. Public Health 2018, 15, 1704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, T.L.; Lin, Y.T.; Hwang, B.F.; Nakayama, S.F.; Tsai, C.H.; Sun, X.L.; Ma, C.; Jung, C.R. Fine particulate matter is a potential determinant of Alzheimer’s disease: A systemic review and meta-analysis. Environ. Res. 2019, 177, 108638. [Google Scholar] [CrossRef] [PubMed]
- Seaton, A.; Tran, L.; Chen, R.; Maynard, R.L.; Whalley, L.J. Pollution, Particles, and Dementia: A Hypothetical Causative Pathway. Int. J. Environ. Res. Public Health 2020, 17, 862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, K.V.; Frier, B.M.; Strachan, M.W. The relationship between type 2 diabetes and cognitive dysfunction: Longitudinal studies and their methodological limitations. Eur. J. Pharmacol. 2004, 490, 169–175. [Google Scholar] [CrossRef]
- Van Himbergen, T.M.; Beiser, A.S.; Ai, M.; Seshadri, S.; Otokozawa, S.; Au, R.; Thongtang, N.; Wolf, P.A.; Schaefer, E.J. Biomarkers for insulin resistance and inflammation and the risk for all-cause dementia and Alzheimer disease: Results from the Framingham Heart Study. Arch. Neurol. 2012, 69, 594–600. [Google Scholar] [CrossRef] [Green Version]
- Biessels, G.J.; Despa, F. Cognitive decline and dementia in diabetes mellitus: Mechanisms and clinical implications. Nat. Rev. Endocrinol. 2018, 14, 591–604. [Google Scholar] [CrossRef]
- Arnold, S.E.; Arvanitakis, Z.; Macauley-Rambach, S.L.; Koenig, A.M.; Wang, H.Y.; Ahima, R.S.; Craft, S.; Gandy, S.; Buettner, C.; Stoeckel, L.E.; et al. Brain insulin resistance in type 2 diabetes and Alzheimer disease: Concepts and conundrums. Nat. Rev. Neurol. 2018, 14, 168–181. [Google Scholar] [CrossRef]
- Neophytou, A.M.; Costello, S.; Picciotto, S.; Brown, D.M.; Attfield, M.D.; Blair, A.; Lubin, J.H.; Stewart, P.A.; Vermeulen, R.; Silverman, D.T.; et al. Diesel Exhaust, Respirable Dust, and Ischemic Heart Disease: An Application of the Parametric g-formula. Epidemiology 2019, 30, 177–185. [Google Scholar] [CrossRef]
- Gallagher, L.G.; Ray, R.M.; Li, W.; Psaty, B.M.; Gao, D.L.; Thomas, D.B.; Checkoway, H. Occupational exposures and mortality from cardiovascular disease among women textile workers in Shanghai, China. Am. J. Ind. Med. 2012, 55, 991–999. [Google Scholar] [CrossRef] [Green Version]
- Garshick, E.; Laden, F.; Hart, J.E.; Moy, M.L. Respiratory symptoms and intensity of occupational dust exposure. Int. Arch. Occup. Environ. Health 2004, 77, 515–520. [Google Scholar] [CrossRef] [Green Version]
- De Sio, S.; Rosati, M.V.; Cherubini, E.; Ciarrocca, M.; Baccolo, T.P.; Grimaldi, F.; Caciari, T.; Tomao, E.; Tomei, F. Occupational exposure to urban pollutants and plasma insulin. Saudi Med. J. 2005, 26, 416–420. [Google Scholar] [PubMed]
- Tan, C.; Wang, Y.; Lin, M.; Wang, Z.; He, L.; Li, Z.; Li, Y.; Xu, K. Long-term high air pollution exposure induced metabolic adaptations in traffic policemen. Environ. Toxicol. Pharmacol. 2018, 58, 156–162. [Google Scholar] [CrossRef] [PubMed]
- Dimakakou, E.; Johnston, H.J.; Streftaris, G.; Cherrie, J.W. Evaluation of the Suitability of an Existing Job-Exposure Matrix for the Assessment of Exposure of UK Biobank Participants to Dust, Fumes, and Diesel Exhaust Particulates. Int. J. Environ. Res. Public Health 2020, 17, 4919. [Google Scholar] [CrossRef] [PubMed]
- Sadhra, S.S.; Kurmi, O.P.; Chambers, H.; Lam, K.B.; Fishwick, D.; Occupational, C.R.G. Development of an occupational airborne chemical exposure matrix. Occup. Med. (Lond.) 2016, 66, 358–364. [Google Scholar] [CrossRef] [Green Version]
- Sudlow, C.; Gallacher, J.; Allen, N.; Beral, V.; Burton, P.; Danesh, J.; Downey, P.; Elliott, P.; Green, J.; Landray, M.; et al. UK Biobank: An Open Access Resource for Identifying the Causes of a Wide Range of Complex Diseases of Middle and Old Age. PLoS Med. 2015, 12, e1001779. [Google Scholar] [CrossRef] [Green Version]
- Falconer, C.L.; Cooper, A.R.; Flint, E. Patterns and correlates of active commuting in adults with type 2 diabetes: Cross-Sectional evidence from UK Biobank. BMJ Open 2017, 7, e017132. [Google Scholar] [CrossRef]
- Eeftens, M.; Beelen, R.; de Hoogh, K.; Bellander, T.; Cesaroni, G.; Cirach, M.; Declercq, C.; Dėdelė, A.; Dons, E.; de Nazelle, A.; et al. Development of Land Use Regression models for PM(2.5), PM(2.5) absorbance, PM(10) and PM(coarse) in 20 European study areas; results of the ESCAPE project. Environ. Sci. Technol. 2012, 46, 11195–11205. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria. 2019. Available online: https://www.R-project.org/ (accessed on 21 December 2020).
- Sadhra, S.; Kurmi, O.P.; Sadhra, S.S.; Lam, K.B.; Ayres, J.G. Occupational COPD and job exposure matrices: A systematic review and meta-analysis. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 725–734. [Google Scholar] [CrossRef] [Green Version]
- Akaike, H. Akaike’s Information Criterion. In International Encyclopedia of Statistical Science; Lovric, M., Ed.; Springer: Berlin/Heidelberg, Germany, 2011; p. 25. [Google Scholar] [CrossRef]
- Liu, C.; Yang, C.; Zhao, Y.; Ma, Z.; Bi, J.; Liu, Y.; Meng, X.; Wang, Y.; Cai, J.; Kan, H.; et al. Associations between long-term exposure to ambient particulate air pollution and type 2 diabetes prevalence, blood glucose and glycosylated hemoglobin levels in China. Environ. Int. 2016, 92–93, 416–421. [Google Scholar] [CrossRef] [Green Version]
- Yang, M.; Cheng, H.; Shen, C.; Liu, J.; Zhang, H.; Cao, J.; Ding, R. Effects of long-term exposure to air pollution on the incidence of type 2 diabetes mellitus: A meta-analysis of cohort studies. Environ. Sci. Pollut. Res. Int. 2020, 27, 798–811. [Google Scholar] [CrossRef]
- Fu, P.; Guo, X.; Cheung, F.M.H.; Yung, K.K.L. The association between PM(2.5) exposure and neurological disorders: A systematic review and meta-analysis. Sci. Total Environ. 2019, 655, 1240–1248. [Google Scholar] [CrossRef] [PubMed]
- Lao, X.Q.; Guo, C.; Chang, L.-Y.; Bo, Y.; Zhang, Z.; Chuang, Y.C.; Jiang, W.K.; Lin, C.; Tam, T.; Lau, A.K.H.; et al. Long-term exposure to ambient fine particulate matter (PM2.5) and incident type 2 diabetes: A longitudinal cohort study. Diabetologia 2019, 62, 759–769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, B.-Y.; Fan, S.; Thiering, E.; Seissler, J.; Nowak, D.; Dong, G.-H.; Heinrich, J. Ambient air pollution and diabetes: A systematic review and meta-analysis. Environ. Res. 2020, 180, 108817. [Google Scholar] [CrossRef] [PubMed]
- Smargiassi, A.; Sidi, E.A.L.; Robert, L.-E.; Plante, C.; Haddad, M.; Gamache, P.; Burnett, R.; Goudreau, S.; Liu, L.; Fournier, M.; et al. Exposure to ambient air pollutants and the onset of dementia in Québec, Canada. Environ. Res. 2020, 190, 109870. [Google Scholar] [CrossRef]
- Lee, M.; Schwartz, J.; Wang, Y.; Dominici, F.; Zanobetti, A. Long-term effect of fine particulate matter on hospitalization with dementia. Environ. Pollut. 2019, 254, 112926. [Google Scholar] [CrossRef]
- Chen, H.; Kwong, J.C.; Copes, R.; Hystad, P.; van Donkelaar, A.; Tu, K.; Brook, J.R.; Goldberg, M.S.; Martin, R.V.; Murray, B.J.; et al. Exposure to ambient air pollution and the incidence of dementia: A population-based cohort study. Environ. Int. 2017, 108, 271–277. [Google Scholar] [CrossRef]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Tzivian, L.; Dlugaj, M.; Winkler, A.; Weinmayr, G.; Hennig, F.; Fuks, K.B.; Vossoughi, M.; Schikowski, T.; Weimar, C.; Erbel, R.; et al. Long-term air pollution and traffic noise exposures and mild cognitive impairment in older adults: A cross-sectional analysis of the Heinz Nixdorf recall study. Environ. Health Perspect. 2016, 124, 1361–1368. [Google Scholar] [CrossRef] [Green Version]
- Cullen, B.; Newby, D.; Lee, D.; Lyall, D.M.; Nevado-Holgado, A.J.; Evans, J.J.; Pell, J.P.; Lovestone, S.; Cavanagh, J. Cross-sectional and longitudinal analyses of outdoor air pollution exposure and cognitive function in UK Biobank. Sci. Rep. 2018, 8, 12089. [Google Scholar] [CrossRef]
- Connolly, V.; Unwin, N.; Sherriff, P.; Bilous, R.; Kelly, W. Diabetes prevalence and socioeconomic status: A population based study showing increased prevalence of type 2 diabetes mellitus in deprived areas. J. Epidemiol. Community Health 2000, 54, 173. [Google Scholar] [CrossRef] [Green Version]
- Russ, T.C.; Stamatakis, E.; Hamer, M.; Starr, J.M.; Kivimäki, M.; Batty, G.D. Socioeconomic status as a risk factor for dementia death: Individual participant meta-analysis of 86,508 men and women from the UK. Br. J. Psychiatry 2013, 203, 10–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haffner, S.M.; D’Agostino, R.; Saad, M.F.; Rewers, M.; Mykkänen, L.; Selby, J.; Howard, G.; Savage, P.J.; Hamman, R.F.; Wagenknecht, L.E.; et al. Increased insulin resistance and insulin secretion in nondiabetic African-Americans and Hispanics compared with non-Hispanic whites. The Insulin Resistance Atherosclerosis Study. Diabetes 1996, 45, 742–748. [Google Scholar] [CrossRef] [PubMed]
- Rhee, E.J. Diabetes in Asians. Endocrinol. Metab. (Seoul) 2015, 30, 263–269. [Google Scholar] [CrossRef] [Green Version]
- Colberg, S.R.; Sigal, R.J.; Fernhall, B.; Regensteiner, J.G.; Blissmer, B.J.; Rubin, R.R.; Chasan-Taber, L.; Albright, A.L.; Braun, B.; American College of Sports, M.; et al. Exercise and type 2 diabetes: The American College of Sports Medicine and the American Diabetes Association: Joint position statement. Diabetes Care 2010, 33, e147–e167. [Google Scholar] [CrossRef] [Green Version]
- Westreich, D.; Greenland, S. The Table 2 Fallacy: Presenting and Interpreting Confounder and Modifier Coefficients. Am. J. Epidemiol. 2013, 177, 292–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nordentoft, M.; Rod, N.H.; Bonde, J.P.; Bjorner, J.B.; Madsen, I.E.H.; Pedersen, L.R.M.; Cleal, B.; Magnusson Hanson, L.L.; Nexo, M.A.; Pentti, J.; et al. Effort-reward imbalance at work and risk of type 2 diabetes in a national sample of 50,552 workers in Denmark: A prospective study linking survey and register data. J. Psychosom. Res. 2020, 128, 109867. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, C.H.; Spiegelman, D.; Manson, J.; Schernhammer, E.S.; Colditz, G.A.; Kawachi, I. Work characteristics and incidence of type 2 diabetes in women. Am. J. Epidemiol. 2007, 165, 175–183. [Google Scholar] [CrossRef]
- Hendryx, M.; Luo, J.; Chojenta, C.; Byles, J.E. Exposure to heavy metals from point pollution sources and risk of incident type 2 diabetes among women: A prospective cohort analysis. Int. J. Environ. Health Res. 2019, 10, 1–12. [Google Scholar] [CrossRef]
- Huang, L.-Y.; Hu, H.-Y.; Wang, Z.-T.; Ma, Y.-H.; Dong, Q.; Tan, L.; Yu, J.-T. Association of Occupational Factors and Dementia or Cognitive Impairment: A Systematic Review and Meta-Analysis. J. Alzheimer’s Dis. 2020, 1–11, Preprint. [Google Scholar] [CrossRef]
- Helmer, C.; Letenneur, L.; Rouch, I.; Richard-Harston, S.; Barberger-Gateau, P.; Fabrigoule, C.; Orgogozo, J.M.; Dartigues, J.F. Occupation during life and risk of dementia in French elderly community residents. J. Neurol. Neurosurg. Psychiatry 2001, 71, 303–309. [Google Scholar] [CrossRef] [Green Version]
- Santibáñez, M.; Bolumar, F.; García, A.M. Occupational risk factors in Alzheimer’s disease: A review assessing the quality of published epidemiological studies. Occup. Environ. Med. 2007, 64, 723–732. [Google Scholar]
- Park, R.M.; Schulte, P.A.; Bowman, J.D.; Walker, J.T.; Bondy, S.C.; Yost, M.G.; Touchstone, J.A.; Dosemeci, M. Potential occupational risks for neurodegenerative diseases. Am. J. Ind. Med. 2005, 48, 63–77. [Google Scholar] [CrossRef] [PubMed]
- Gunnarsson, L.G.; Bodin, L. Occupational Exposures and Neurodegenerative Diseases-A Systematic Literature Review and Meta-Analyses. Int. J. Environ. Res. Public Health 2019, 16, 337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koeman, T.; Schouten, L.J.; van den Brandt, P.A.; Slottje, P.; Huss, A.; Peters, S.; Kromhout, H.; Vermeulen, R. Occupational exposures and risk of dementia-related mortality in the prospective Netherlands Cohort Study. Am. J. Ind. Med. 2015, 58, 625–635. [Google Scholar] [CrossRef] [PubMed]
- Meo, S.A.; Al-Khlaiwi, T.; Abukhalaf, A.A.; Alomar, A.A.; Alessa, O.M.; Almutairi, F.J.; Alasbali, M.M. The Nexus between Workplace Exposure for Wood, Welding, Motor Mechanic, and Oil Refinery Workers and the Prevalence of Prediabetes and Type 2 Diabetes Mellitus. Int. J. Environ. Res. Public Health 2020, 17, 3992. [Google Scholar] [CrossRef] [PubMed]
- Ritz, B.; Hoffmann, B.; Peters, A. The Effects of Fine Dust, Ozone, and Nitrogen Dioxide on Health. Dtsch. Arzteblatt Int. 2019, 51–52, 881–886. [Google Scholar] [CrossRef] [PubMed]
- Peters, S.; Vermeulen, R.; Portengen, L.; Olsson, A.; Kendzia, B.; Vincent, R.; Savary, B.; Lavoué, J.; Cavallo, D.; Cattaneo, A.; et al. SYN-JEM: A Quantitative Job-Exposure Matrix for Five Lung Carcinogens. Ann. Occup. Hyg. 2016, 60, 795–811. [Google Scholar] [CrossRef] [Green Version]
- Schraufnagel, D.E. The health effects of ultrafine particles. Exp. Mol. Med. 2020, 52, 311–317. [Google Scholar] [CrossRef]


{kind=link}
| Baseline Variable | Grouping | All Subjects | Dementia | Type 2 Diabetes Mellitus | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | % (with NA’s) | % | n | % (Out of 502,504) | % (Out of the Diseased) | n | % (Out of 502,504) | % (Out of the Diseased) | ||
| Sex | ||||||||||
| All | 502,504 | 100 | 100 | 534 | 0.11 | 100 | 21,560 | 4.30 | 100 | |
| Male | 273,382 | 45.60 | 45.60 | 309 | 0.06 | 57.87 | 13,036 | 2.60 | 60.46 | |
| Female | 229,122 | 54.40 | 54.40 | 225 | 0.04 | 42.13 | 8524 | 1.70 | 39.54 | |
| Missing | - | - | - | - | - | - | - | - | - | |
| Age recruitment | ||||||||||
| All | 502,504 | 100 | 100 | 534 | 0.11 | 100 | 21,560 | 4.30 | 100 | |
| (36–46) | 77,177 | 15.36 | 15.36 | 30 | 0.01 | 5.62 | 1132 | 0.23 | 5.25 | |
| (46–56) | 151,241 | 30.10 | 30.10 | 81 | 0.02 | 15.17 | 4704 | 0.94 | 21.82 | |
| (56–66) | 220,407 | 43.86 | 43.86 | 275 | 0.05 | 51.50 | 11,597 | 2.31 | 53.79 | |
| (66–73) | 53,679 | 10.68 | 10.68 | 148 | 0.03 | 27.71 | 4127 | 0.82 | 19.14 | |
| Missing | - | - | - | - | - | - | - | - | - | |
| Ethnicity | ||||||||||
| (All-Missing) | 501,606 | |||||||||
| All | 502,504 | 100 | 100 | 533 | 0.11 | 100 | 21,559 | 4.13 | 100 | |
| White | 472,695 | 94.24 | 94.24 | 504 | 0.10 | 94.55 | 18,828 | 3.75 | 87.33 | |
| Mixed | 2958 | 0.59 | 0.59 | 4 | 0.00 | 0.75 | 137 | 0.03 | 0.64 | |
| Asian | 11,456 | 2.28 | 2.28 | 5 | 0.00 | 0.94 | 1442 | 0.28 | 6.69 | |
| Black | 8061 | 1.61 | 1.61 | 10 | 0.00 | 1.87 | 684 | 0.13 | 3.17 | |
| Others | 6436 | 1.28 | 1.28 | 10 | 0.00 | 1.87 | 468 | 0.09 | 2.17 | |
| Missing | 898 | 0.17 | - | 1 | 0.00 | - | 1 | 0.00 | - | |
| SES | ||||||||||
| (All-Missing) | 501,881 | |||||||||
| All | 502,504 | 100 | 100 | 533 | 0.09 | 100 | 21,529 | 4.28 | 100 | |
| 1 | 100,658 | 20.03 | 20.10 | 85 | 0.02 | 15.95 | 3215 | 0.64 | 14.93 | |
| 2 | 100,098 | 19.92 | 19.90 | 71 | 0.01 | 13.32 | 3586 | 0.71 | 16.66 | |
| 3 | 100,382 | 19.98 | 20.00 | 96 | 0.02 | 18.01 | 3978 | 0.79 | 18.48 | |
| 4 | 100,367 | 19.97 | 20.00 | 116 | 0.02 | 21.76 | 4499 | 0.89 | 20.89 | |
| 5 | 100,376 | 19.97 | 20.00 | 165 | 0.03 | 30.96 | 6251 | 1.24 | 29.04 | |
| Missing | 623 | 0.12 | - | 1 | 0.00 | - | 31 | 0.01 | - | |
| BMI | ||||||||||
| (All-Missing) | 499,503 | |||||||||
| All | 502,504 | 100 | 100 | 517 | 0.10 | 100 | 21,345 | 4.24 | 100 | |
| < 18.5 | 2374 | 0.47 | 0.50 | 3 | 0.00 | 0.58 | 19 | 0.00 | 0.09 | |
| 18.5–24.9 | 157,631 | 31.37 | 31.60 | 144 | 0.03 | 27.85 | 2049 | 0.41 | 9.60 | |
| 25–29.9 | 214,485 | 42.68 | 42.90 | 230 | 0.05 | 44.49 | 7276 | 1.45 | 34.09 | |
| ≥ 30 | 125,013 | 24.88 | 25.00 | 140 | 0.03 | 27.08 | 12,001 | 2.40 | 56.22 | |
| Missing | 3001 | 0.60 | - | 17 | 0.00 | - | 215 | 0.04 | - | |
| BP | ||||||||||
| (All-Missing) | 498,639 | |||||||||
| All | 502,504 | 100 | 100 | 524 | 0.10 | 100 | 21,430 | 4.26 | 100 | |
| No | 387,531 | 77.12 | 77.7 | 325 | 0.06 | 62.02 | 7308 | 1.45 | 34.10 | |
| Unknown | 637 | 0.13 | 0.10 | 3 | 0.00 | 0.57 | 20 | 0.00 | 0.09 | |
| Yes | 110,525 | 21.99 | 22.20 | 196 | 0.04 | 37.40 | 14,102 | 2.81 | 65.80 | |
| Missing | 3811 | 0.76 | - | 10 | 0.00 | - | 130 | 0.00 | - | |
| Diet changes | ||||||||||
| (All-Missing) | 501,717 | |||||||||
| All | 502,504 | 100 | 100 | 533 | 0.11 | 100 | 21,560 | 4.30 | 100 | |
| No | 296,798 | 59.06 | 59.20 | 272 | 0.05 | 51.03 | 5474 | 1.09 | 25.39 | |
| Unknown | 1443 | 0.29 | 0.30 | 4 | 0.00 | 0.75 | 78 | 1.02 | 0.36 | |
| Yes, illness | 57,550 | 11.45 | 11.50 | 132 | 0.03 | 24.77 | 12,164 | 2.43 | 56.42 | |
| Yes, other | 145,826 | 29.02 | 29.10 | 125 | 0.02 | 23.45 | 3844 | 0.77 | 17.83 | |
| Missing | 887 | 0.18 | - | 1 | 0.00 | - | - | - | - | |
| Physical activity | ||||||||||
| (All-Missing) | 490,724 | |||||||||
| All | 502,504 | 100 | 100 | 507 | 0.10 | 100 | 20,610 | 4.10 | 100 | |
| Low | 163,988 | 32.63 | 33.40 | 232 | 0.05 | 45.76 | 8636 | 1.76 | 41.90 | |
| Moderate | 203,130 | 40.42 | 41.40 | 161 | 0.03 | 31.75 | 7890 | 1.61 | 38.28 | |
| High | 123,606 | 24.60 | 25.20 | 114 | 0.02 | 22.49 | 4084 | 0.83 | 19.82 | |
| Missing | 11,780 | 2.34 | - | 27 | 0.00 | - | 950 | 0.19 | - | |
| T2DM | Dementia | |||
|---|---|---|---|---|
| OR (95% CI) ** | OR (95% CI) ** | OR (95% CI) ** | OR (95% CI) ** | |
| Univariable Model 1 | Multivariable * Model 2 | Univariable Model 1 | Multivariable * Model 2 | |
| PM2.5 | 1.13 (1.12–1.15) | 1.02 (1.00–1.03) | 1.18 (1.09–1.28) | 1.06 (0.96–1.16) |
| Sex (female) a | ||||
| Male | 1.88 (1.82–1.93) | 1.83 (1.77–1.89) | 1.64 (1.38–1.95) | 1.55 (1.28–1.89) |
| Age | 1.06 (1.06–0.07) | 1.07 (1.07–1.08) | 1.09 (1.08–1.11) | 1.08 (1.07–1.10) |
| Ethnic background (White) | ||||
| Asian | 3.47 (3.28–3.68) | 3.80 (3.52–4.09) | - | - |
| Black | 2.24 (2.06–2.42) | 1.64 (1.48–1.81) | - | - |
| Mixed | 1.17 (0.98–1.38) | 1.38 (1.11–1.70) | - | - |
| Other | 1.89 (1.72–2.08) | 1.64 (1.48–1.81) | - | - |
| Townsend deprivation (1) | ||||
| 2 | 1.13 (1.07–1.18) | 1.06 (1.01–1.12) | 0.84 (0.61–1.15) | 0.76 (0.54–1.08) |
| 3 | 1.25 (1.19–1.31) | 1.13 (1.07–1.19) | 1.13 (0.85–1.52) | 1.02 (0.74–1.41) |
| 4 | 1.42 (1.36–1.49) | 1.18 (1.11–1.24) | 1.37 (1.04–1.82) | 1.38 (1.02–1.89) |
| 5 (most deprived) | 2.02 (1.94–2.11) | 1.37 (1.29–1.44) | 1.95 (1.50–2.54) | 1.79 (1.31–2.46) |
| BMI (< 18.5) | ||||
| ≥ 30 | 13.15 (8.64–21.43) | 12.53 (7.64–22.44) | - | - |
| 25–29.9 | 4.35 (2.85–7.08) | 4.70 (2.86–8.42) | - | - |
| 18.5–24.9 | 1.63 (1.07–2.66) | 2.23 (1.35–3.99) | - | - |
| Dietary changes (No) | ||||
| Unknown | 3.05 (2.40–3.80) | 2.08 (1.52–2.77) | 3.03 (0.93–7.12) | 1.76 (0.29–5.67) |
| Yes, because of illness | 14.26 (13.80–14.75) | 11.22 (10.81–11.65) | 2.51 (2.03–3.08) | 1.86 (1.46–2.35) |
| Yes, because of other | 1.44 (1.38–1.50) | 1.36 (1.30–1.43) | 0.94 (0.75–1.15) | 0.96 (0.75–1.20) |
| Physical activity (Low) | ||||
| High | 0.61 (0.59–0.64 | 0.76 (0.73–0.79) | 0.94 (0.75–1.15) | 0.96 (0.75–1.20) |
| Moderate | 0.73 (0.70–0.75) | 0.88 (0.85–0.91) | 0.94 (0.75–1.15) | 0.96 (0.75–1.20) |
| Father’s history (No) | ||||
| Do not know | 1.71 (1.62–1.80) | 1.23 (1.16–1.31) | 2.23 (1.68–2.90) | 1.65 (1.20–2.23) |
| Prefer not to answer | 1.86 (1.34–2.52) | 1.07 (0.66–1.65) | 3.28 (0.54–10.20) | 1.98 (0.29–7.65) |
| Yes | 2.35 (2.27–2.44) | 2.37 (2.27–2.48) | 1.23 (0.82–1.77) | 1.30 (0.85–1.91) |
| Mother’s history (No) | ||||
| Do not know | 1.63 (1.53–1.74) | 1.06 (0.97–1.15) | 1.67 (1.10–2.43) | 0.99 (0.60–1.53) |
| Prefer not to answer | 1.78 (1.24–2.47) | 0.93 (0.54–1.53) | 6.00 (1.49–15.72) | 5.07 (1.10–15.59) |
| Yes | 1.06 (1.03–1.09) | 1.08 (1.05–1.12) | 1.03 (0.77–1.37) | 1.07 (0.77–1.45) |
| T2DM | ||
|---|---|---|
| (P × L) *** | OR (95% CI) Univariable | OR (95% CI) Multivariable * |
| Dust a | 1.11 (1.00–1.22) | 0.93 (0.88–0.98) |
| Fumes a | 1.60 (1.29–1.96) | 1.01 (0.95–1.07) |
| Diesel a | 27.69 (13.47–55.35) | 1.07 (0.99–1.15) |
| Mineral Dust a | 1.35 (1.16–1.57) | 0.91 (0.86–0.97) |
| Biological Dust a | 0.78 (0.78–1.13) | 0.95 (0.89–1.02) |
| DEMENTIA | ||
| (P × L) *** | OR (95% CI) Univariable | OR (95% CI) Multivariable ** |
| Dust a | 1.51 (0.73–2.72) | 1.02 (0.71–1.45) |
| Fumes a | 1.80 (0.26–5.98) | 1.25 (0.84–1.84) |
| Diesel a | 1.22 (0.00–414.36) | 0.98 (0.56–1.62) |
| Mineral Dust a | 1.69 (0.49–4.08) | 1.02 (0.66–1.51) |
| Biological Dust a | 2.74 (1.07–5.57) | 0.97 (0.58–1.52) |
| T2DM | Dementia | |
|---|---|---|
| (P × L) *** | OR (95% CI) Multivariable * | OR (95% CI) Multivariable ** |
| Dust a | 1.01 (0.96–1.06) | 1.14 (0.79–1.61) |
| Fumes | 1.24 (1.17–1.31) | 1.57 (1.06–2.27) |
| Diesel | 1.31 (1.22–1.41) | 1.26 (0.72–2.05) |
| Mineral Dust | 1.11 (1.04–1.17) | 1.26 (0.83–1.86) |
| Biological Dust | 0.90 (0.84–0.96) | 0.95 (0.55–1.44) |
| T2DM * | Dementia ** | |
|---|---|---|
| OR (95% CI) | OR (95% CI) | |
| (PL-max) *** | 1.10 (1.05–1.15) | 1.40 (1.00–1.95) |
| (PL-max) | 0.96 (0.91–1.01) | 1.20 (0.85–1.69) |
| Workplace very dusty | 1.01 (0.93–1.09) | 1.04 (0.48–2.24) |
| Workplace with fumes | 0.95 (0.87–1.03) | 1.15 (0.48–2.54) |
| Workplace with diesel | 0.99 (0.90–1.09) | 1.54 (0.58–3.67) |
| Cumulative Occupational Exposure Over Years—Standardised Values (Standardised (P × L) * Years) *** | T2DM OR (95% CI) Univariable | T2DM OR (95% CI) Multivariable * | Dementia OR (95% CI) Univariable | Dementia OR (95% CI) Multivariable ** |
|---|---|---|---|---|
| Dust | 1.09 (1.06–1.11) | 1.00 (0.97–1.03) | 1.00 (0.54–1.23) | 0.95 (0.49–1.21) |
| Fumes | 1.07 (1.04–1.09) | 0.98 (0.95–1.01) | 0.99 (0.46–1.19) | 0.95 (0.42–1.18) |
| Diesel engine exhaust | 1.07 (1.05–1.09) | 0.98 (0.94–1.01) | 1.10 (0.86–1.20) | 1.08 (0.83–1.18) |
| Mineral dust | 1.08 (1.05–1.10) | 1.01 (0.97–1.03) | 1.07 (0.73–1.23) | 1.05 (0.69–1.22) |
| Biological dust | 1.05 (1.02–1.07) | 1.00 (0.97–1.03) | 0.12 (0.00–0.58) | 0.02 (0.00–4.70) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dimakakou, E.; Johnston, H.J.; Streftaris, G.; Cherrie, J.W. Is Environmental and Occupational Particulate Air Pollution Exposure Related to Type-2 Diabetes and Dementia? A Cross-Sectional Analysis of the UK Biobank. Int. J. Environ. Res. Public Health 2020, 17, 9581. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249581
Dimakakou E, Johnston HJ, Streftaris G, Cherrie JW. Is Environmental and Occupational Particulate Air Pollution Exposure Related to Type-2 Diabetes and Dementia? A Cross-Sectional Analysis of the UK Biobank. International Journal of Environmental Research and Public Health. 2020; 17(24):9581. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249581
Chicago/Turabian StyleDimakakou, Eirini, Helinor J. Johnston, George Streftaris, and John W. Cherrie. 2020. "Is Environmental and Occupational Particulate Air Pollution Exposure Related to Type-2 Diabetes and Dementia? A Cross-Sectional Analysis of the UK Biobank" International Journal of Environmental Research and Public Health 17, no. 24: 9581. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17249581