Knowledge and Practice of Preventive Measures for Oral Health Care among Male Intermediate Schoolchildren in Abha, Saudi Arabia

Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Petersen, P.E. Continuous improvement of oral health in the 21st century: The approach of the WHO Global Oral Health Programme. Zhonghua Kouqiang Yi Xue Za Zhi 2004, 39, 441–444. [Google Scholar]
- Togoo, R.A.; Yaseen, S.; Zakirulla, M.; Nasim, V.S.; Al Zamzami, M. Oral hygiene knowledge and practices among school children in a rural area of southern Saudi Arabia. Int. J. Contemp. Dent. 2012, 3, 57–62. [Google Scholar]
- Ali, M.S.; Hussain, T.; Ara, G.; Zehra, N. Oral health awareness and practices of school going children aged 11 to 16 years in a squatter settlement of Karachi. J. Dow Univ. Health Sci. 2015, 9, 71–75. [Google Scholar]
- Varenne, B.; Petersen, P.E.; Ouattara, S. Oral health behaviour of children and adults in urban and rural areas of Burkina Faso, Africa. Int. Dent. J. 2006, 56, 61–70. [Google Scholar] [CrossRef]
- Amarlal, D.; Devdas, K.; Priya, M.; Venkatachalapathy, A. Oral health attitudes, knowledge and practice among school children in Chennai, India. J. Educ. Ethic Dent. 2013, 3, 26. [Google Scholar] [CrossRef]
- Al-Ansari, J.; Honkala, E.; Honkala, S. Oral health knowledge and behavior among male health sciences college students in Kuwait. BMC Oral Heal. 2003, 3, 2. [Google Scholar] [CrossRef] [Green Version]
- Al-Hussaini, R.; Al-Kandari, M.; Hamadi, T.; Al-Mutawa, A.; Honkala, S.; Memon, A. Dental health knowledge, attitudes and behaviour among students at the Kuwait University Health Sciences Centre. Med. Princ. Pract. 2003, 12, 260–265. [Google Scholar] [CrossRef]
- Jamjoom, H. Preventive oral health knowledge and practice in Jeddah, Saudi Arabia. J. King Abdulaziz Univ. Sci. 2001, 9, 17–25. [Google Scholar] [CrossRef] [Green Version]
- Farsi, J.; Farghaly, M.; Farsi, N. Oral health knowledge, attitude and behaviour among Saudi school students in Jeddah city. J. Dent. 2004, 32, 47–53. [Google Scholar] [CrossRef]
- Hebbal, M.; Ankola, A.V.; Vadavi, D.; Patel, K. Evaluation of knowledge and plaque scores in school children before and after health education. Dent. Res. J. 2011, 8, 189–196. [Google Scholar] [CrossRef]
- Wyne, A.H. Oral health knowledge and sources of information among male secondary school children in Riyadh. Saudi Dent. J. 2005, 17, 140–145. [Google Scholar]
- Gao, J.; Ruan, J.; Zhao, L.; Zhou, H.; Huang, R.; Tian, J. Oral health status and oral health knowledge, attitudes and behavior among rural children in Shaanxi, western China: A cross-sectional survey. BMC Oral Health 2014, 14, 144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smyth, E.; Caamano, F.; Fernández-Riveiro, P. Oral health knowledge, attitudes and practice in 12-year-old schoolchildren. Medicina Oral Patología Oral y Cirugia Bucal 2007, 12, 614–620. [Google Scholar]
- Dakhili, S.; Alsuwaidi, N.O.; Saeed, S.; Murad, S.B.; Mohammad, D.; Muttappallymyalil, J.; Prasad, P.; Gopakumar, A.; Khan, F.A. Oral hygiene: Association between knowledge and Practice among school going children in Ajman, United Arab Emirates. Am. J. Res. Commun. 2014, 2, 39–48. [Google Scholar]
- Al Subait, A.A.; Alousaimi, M.; Geeverghese, A.; Ali, A.; El Metwally, A. Oral health knowledge, attitude and behavior among students of age 10–18years old attending Jenadriyah festival Riyadh; a cross-sectional study. Saudi J. Dent. Res. 2016, 7, 45–50. [Google Scholar] [CrossRef] [Green Version]
- Zhu, L.; Petersen, P.E.; Wang, H.-Y.; Bian, J.-Y.; Zhang, B.-X. Oral health knowledge, attitudes and behaviour of children and adolescents in China. Int. Dent. J. 2003, 53, 289–298. [Google Scholar] [CrossRef]
- Salahshour, V.N.; Abredari, H.; Sajadi, M.; Sabzaligol, M.; Karimy, M. The effect of oral health promotion program on early dental decay in students: A cluster randomized controlled trial. J. Caring Sci. 2019, 8, 105–110. [Google Scholar] [CrossRef] [Green Version]
- Zavras, A.I.; Vrahopoulos, T.P.; Souliotis, K.; Silvestros, S.; Vrotsos, I. Advances in oral health knowledge of Greek navy recruits and theirsocioeconomic determinants. BMC Oral Health 2002, 2, 4. [Google Scholar] [CrossRef] [Green Version]
- Sharda, A.J.; Shetty, S. Relationship of periodontal status and dental caries status with oral health knowledge, attitude and behavior among professional students in India. Int. J. Oral Sci. 2009, 1, 196–206. [Google Scholar] [CrossRef]
- Maida, C.A.; Marcus, M.; Hays, R.D.; Coulter, I.D.; Ramos-Gomez, F.; Lee, S.Y.; McClory, P.S.; Van, L.V.; Wang, Y.; Shen, J.; et al. Child and adolescent perceptions of oral health over the life course. Qual. Life Res. 2015, 24, 2739–2751. [Google Scholar] [CrossRef] [Green Version]
- Udoye, E.A.C. Oral health related knowledge and behavior among nursing students in a nigerian tertiary hospital. Int. J. Dent. Sci. 2012, 7, 2. [Google Scholar]
- Al-Darwish, M.S. Oral health knowledge, behaviour and practices among school children in Qatar. Dent. Res. J. 2016, 13, 342. [Google Scholar] [CrossRef] [PubMed]
- Wahengbam, P.P.; Kshetrimayum, N.; Wahengbam, B.S.; Nandkeoliar, T.; Lyngdoh, D. Assessment of oral health knowledge, attitude and self-care practice among adolescents—A state wide cross- sectional study in Manipur, North Eastern India. J. Clin. Diagn. Res. 2016, 10, ZC65–ZC70. [Google Scholar] [PubMed]
- Calcagnile, F.; Pietrunti, D.; Pranno, N.; Di Giorgio, G.; Ottolenghi, L.; Vozza, I. Oral health knowledge in pre-school children: A survey among parents in central Italy. J. Clin. Exp. Dent. 2019, 11, e327–e333. [Google Scholar] [CrossRef]
- Saldūnaitė, K.; Bendoraitienė, E.A.; Slabšinskienė, E.; Vasiliauskienė, I.; Andruškevičienė, V.; Zūbienė, J. The role of parental education and socioeconomic status in dental caries prevention among Lithuanian children. Medicina 2014, 50, 156–161. [Google Scholar] [CrossRef]
- Sharda, A.J.; Shetty, S.; Ramesh, N.; Sharda, J.; Bhat, N.; Asawa, K. Oral health awareness and attitude among 12–13 years old school children in Udaipur, India. Int. J. Dent. Clin. 2011, 3, 16–19. [Google Scholar]
- Kaur, M.; Grewal, N. Status of oral health awareness in Indian children as compared to Western children: A thought provoking situation (A pilot study). J. Indian Soc. Pedod. Prev. Dent. 2007, 25, 15. [Google Scholar] [CrossRef]
- Al-sadhan, S.A. Oral health practices and dietary habits of intermediate school children in Riyadh, Saudi Arabia. Saudi Dent. J. 2003, 15, 81–87. [Google Scholar]
- Ahmed, N.A.M.; Astrøm, A.N.; Skaug, N.; Petersen, P.E. Dental caries prevalence and risk factors among 12-year old schoolchildren from Baghdad, Iraq: A post-war survey. Int. Dent. J. 2007, 57, 36–44. [Google Scholar] [CrossRef]
- Graça, S.R.; Albuquerque, T.S.; Luis, H.S.; Assunção, V.A.; Malmqvist, S.; Cuculescu, M.; Slusanschi, O.; Johannsen, G.; Galuscan, A.; Podariu, A.C.; et al. Oral Health Knowledge, Perceptions, and Habits of Adolescents from Portugal, Romania, and Sweden: A Comparative Study. J. Int. Soc. Prev. Community Dent. 2019, 9, 470–480. [Google Scholar]
- Blaggana, A.; Grover, V.; Anjali, A.K.; Blaggana, V.; Tanwar, R.; Kaur, H.; Haneet, R.K. Oral health knowledge, attitudes and practice behaviour among secondary school children in Chandigarh. J. Clin. Diagn. Res. 2016, 10, ZC01–ZC06. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Items | No. | % | Mean | Standard Deviation |
|---|---|---|---|---|
| Age groups | 14 | 1.2 | ||
| 12–13 | 16 | 5.3 | ||
| 13–14 | 179 | 33.1 | ||
| 14–15 | 101 | 18.7 | ||
| 15–16 | 147 | 27.2 | ||
| ≥16 | 97 | 15.5 | ||
| Nationality | ||||
| Saudi | 465 | 86.2 | ||
| Non-Saudi | 75 | 13.8 | ||
| School type | ||||
| Public | 450 | 83.3 | ||
| Private | 90 | 16.7 | ||
| Question | Answer | All | Saudi | Non-Saudi | p-Value | |||
|---|---|---|---|---|---|---|---|---|
| No. | % | No. | % | No. | % | |||
| Do you know the importance of good oral health for general health? | Yes | 443 | 82.2 | 372 | 80 | 71 | 94.6 | p < 0.05 |
| No | 97 | 17.8 | 93 | 20 | 4 | 5.4 | ||
| What are the functions of the teeth? | Chewing and eating | 98 | 18.5 | 92 | 19.7 | 6 | 8 | p < 0.001 |
| Speech | 64 | 11.8 | 62 | 13.3 | 2 | 2.7 | ||
| Appearance | 88 | 16.2 | 82 | 17.7 | 6 | 8 | ||
| All of the above | 290 | 53.5 | 229 | 49.3 | 61 | 81.3 | ||
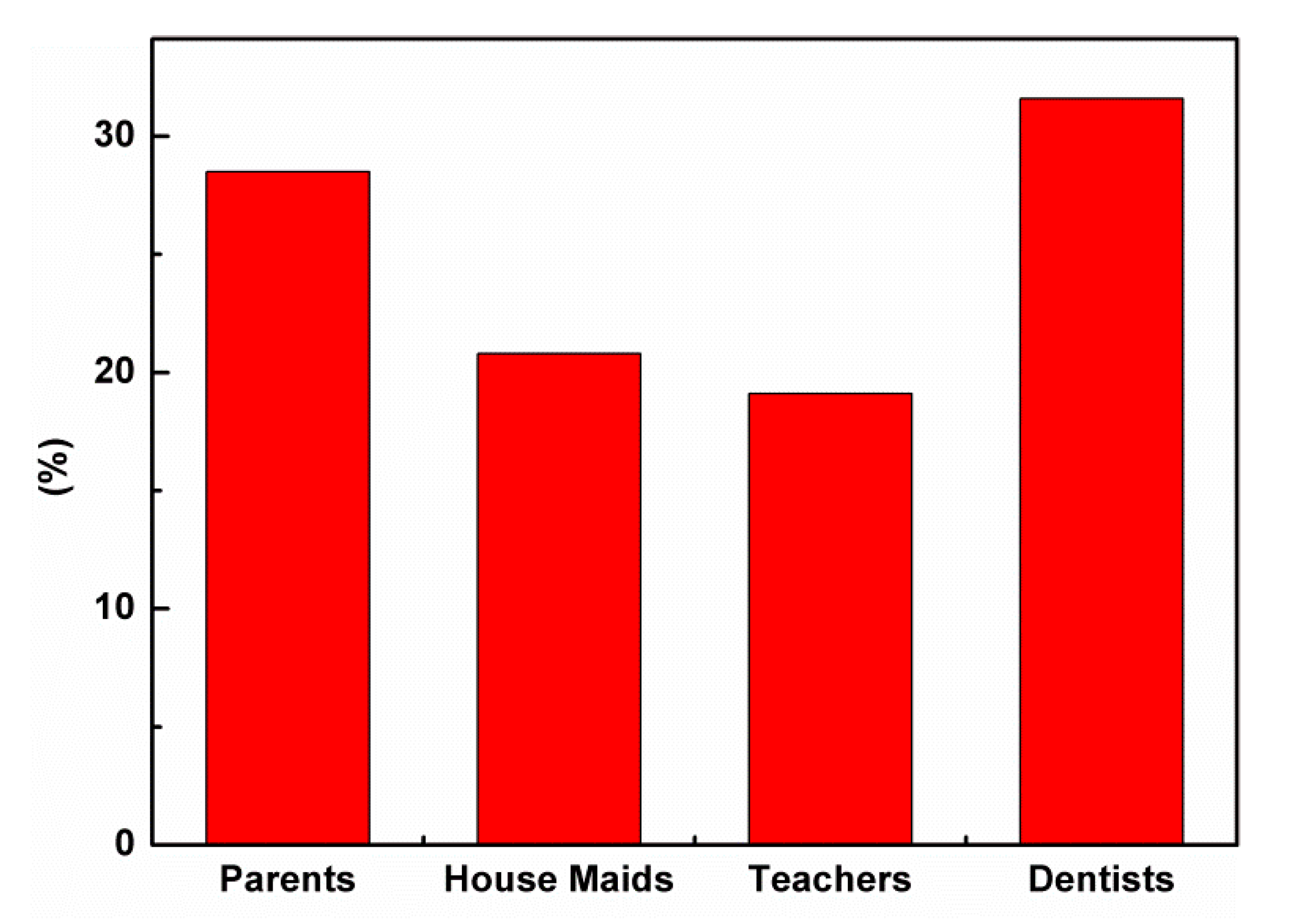
| Where did you get the information about dental health? | Parents | 154 | 28.5 | 113 | 24.3 | 41 | 54.6 | p < 0.001 |
| House maids | 112 | 20.8 | 109 | 23.4 | 3 | 4 | ||
| Teachers | 103 | 19.1 | 99 | 21.3 | 4 | 5.3 | ||
| Dentists | 171 | 31.6 | 144 | 31 | 27 | 36 | ||
| Do you know the substance “fluoride”? | Yes | 198 | 36.6 | 140 | 30.1 | 58 | 77.3 | p < 0.001 |
| No | 342 | 63.4 | 325 | 69.9 | 17 | 22.6 | ||
| Why should fluoride be added to toothpaste? | To give a pleasant taste | 44 | 22.2 | 37 | 26.4 | 7 | 12.1 | p < 0.001 |
| To whiten the teeth | 69 | 34.8 | 63 | 45 | 6 | 10.3 | ||
| To prevent dental caries | 58 | 29.3 | 15 | 10.7 | 43 | 74.1 | ||
| To act as a preservative | 27 | 13.7 | 25 | 17.9 | 2 | 3.5 | ||
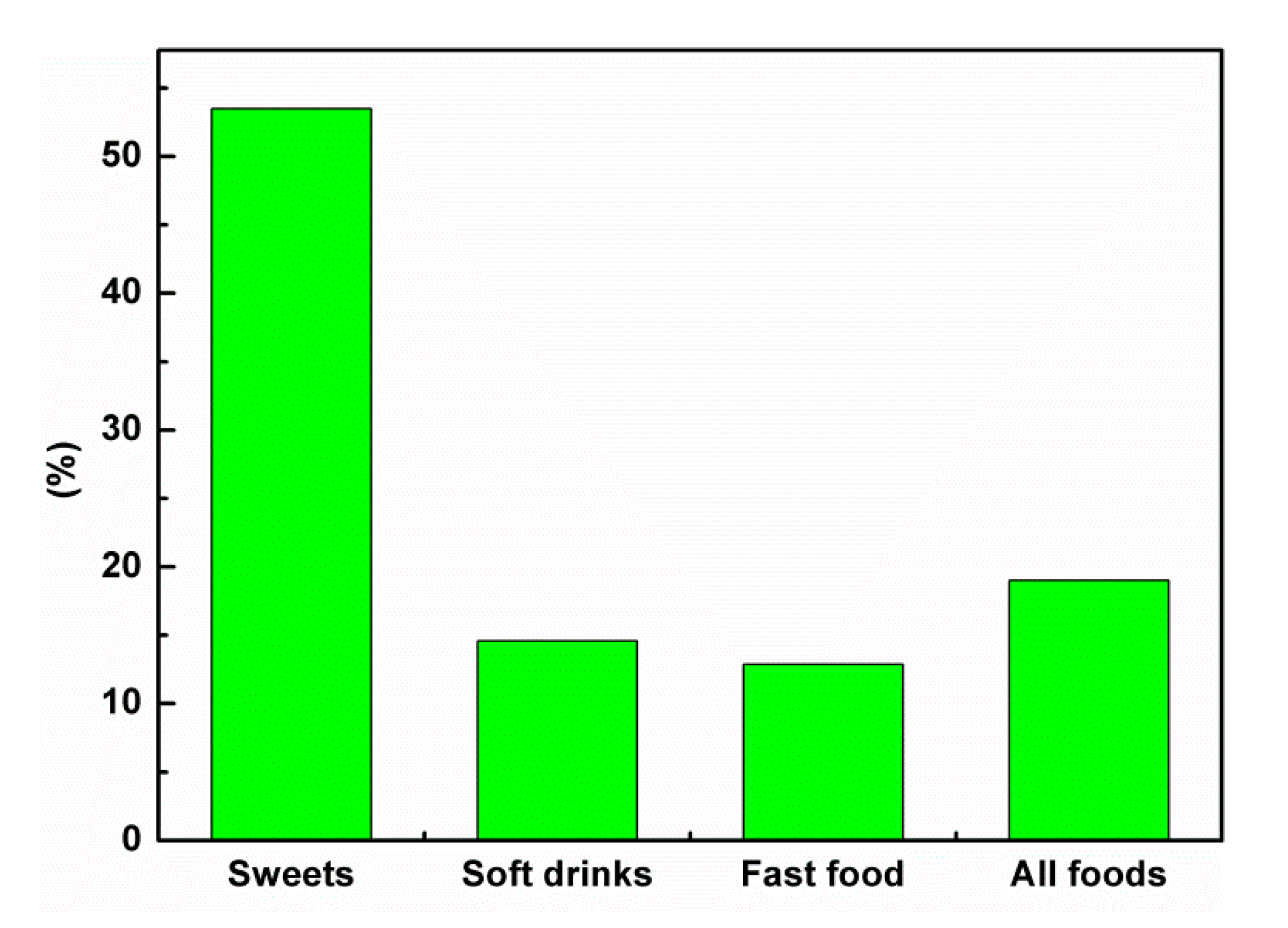
| Which of the following causes tooth decay? | Sweets | 289 | 53.5 | 278 | 59.8 | 11 | 14.7 | p < 0.001 |
| Soft drinks | 79 | 14.6 | 72 | 15.5 | 7 | 9.3 | ||
| Fast food | 70 | 12.9 | 66 | 14.2 | 4 | 5.3 | ||
| All of the above | 102 | 19 | 49 | 10.5 | 53 | 70.7 | ||
| When do you know that your tooth is decayed? | Black and brown spots on the tooth | 72 | 13.3 | 18 | 3.9 | 54 | 72 | p < 0.001 |
| Cavity in the tooth | 98 | 18.1 | 97 | 20.9 | 1 | 1.3 | ||
| Pain in the tooth | 254 | 47.1 | 243 | 52.2 | 11 | 14.7 | ||
| Swelling around the tooth | 116 | 21.5 | 107 | 23 | 9 | 12 | ||
| Do you know that it is necessary to take care of your gums? | Yes | 436 | 80.7 | 367 | 78.9 | 69 | 92 | p < 0.05 |
| No | 104 | 19.3 | 98 | 21.1 | 6 | 8 | ||
| Items | All | Saudi | Non-Saudi | p-Value | ||||
|---|---|---|---|---|---|---|---|---|
| Question | Answer | No. | % | No. | % | No | % | |
| When do you eat sweets? | With meals | 50 | 9.3 | 12 | 2.6 | 38 | 50.7 | p < 0.001 |
| In-between meals | 318 | 58.8 | 309 | 66.4 | 9 | 12 | ||
| Do not eat | 33 | 6.1 | 14 | 3.1 | 19 | 25.3 | ||
| After meals | 139 | 25.8 | 130 | 27.9 | 9 | 12 | ||
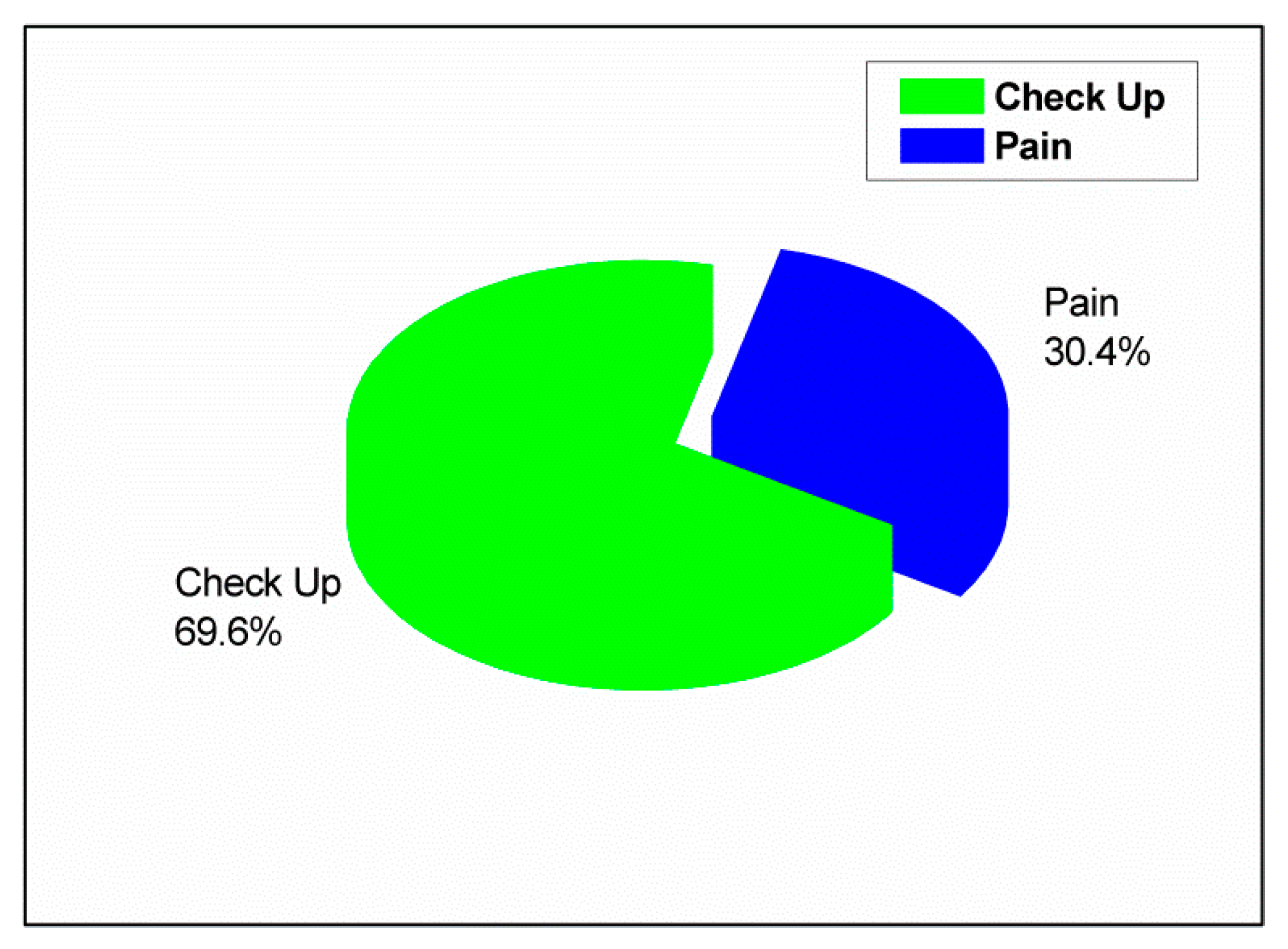
| When do you visit a dentist? | Dental checkup | 165 | 30.4 | 107 | 23.1 | 58 | 77.3 | p < 0.001 |
| During an emergency when there is pain | 375 | 69.6 | 358 | 76.9 | 17 | 22.7 | ||
| How often do you visit a dentist for checkup? | Once in six months | 70 | 42.4 | 15 | 14 | 55 | 94.8 | p < 0.001 |
| Once in a year | 11 | 6.7 | 10 | 9.3 | 1 | 1.7 | ||
| Once in two years | 9 | 5.4 | 9 | 8.4 | 0 | 0 | ||
| Occasionally | 75 | 45.5 | 73 | 68.3 | 2 | 3.5 | ||
| Why do you not you visit a dentist? | Carelessness | 257 | 47.6 | 227 | 48.9 | 13 | 17.3 | p < 0.001 |
| Fear | 130 | 24 | 114 | 24.5 | 9 | 12 | ||
| No dental problems | 121 | 22.4 | 95 | 20.4 | 49 | 65.4 | ||
| Time-consuming | 32 | 6 | 29 | 6.2 | 4 | 5.3 | ||
| How do you clean your teeth? | Toothbrush and toothpaste | 429 | 79.4 | 358 | 77 | 71 | 94.7 | p < 0.05 |
| Miswak | 96 | 17.8 | 94 | 20.2 | 2 | 2.7 | ||
| Toothpicks | 9 | 1.7 | 8 | 1.7 | 1 | 1.3 | ||
| Tooth powder and finger | 6 | 1.1 | 5 | 1.1 | 1 | 1.3 | ||
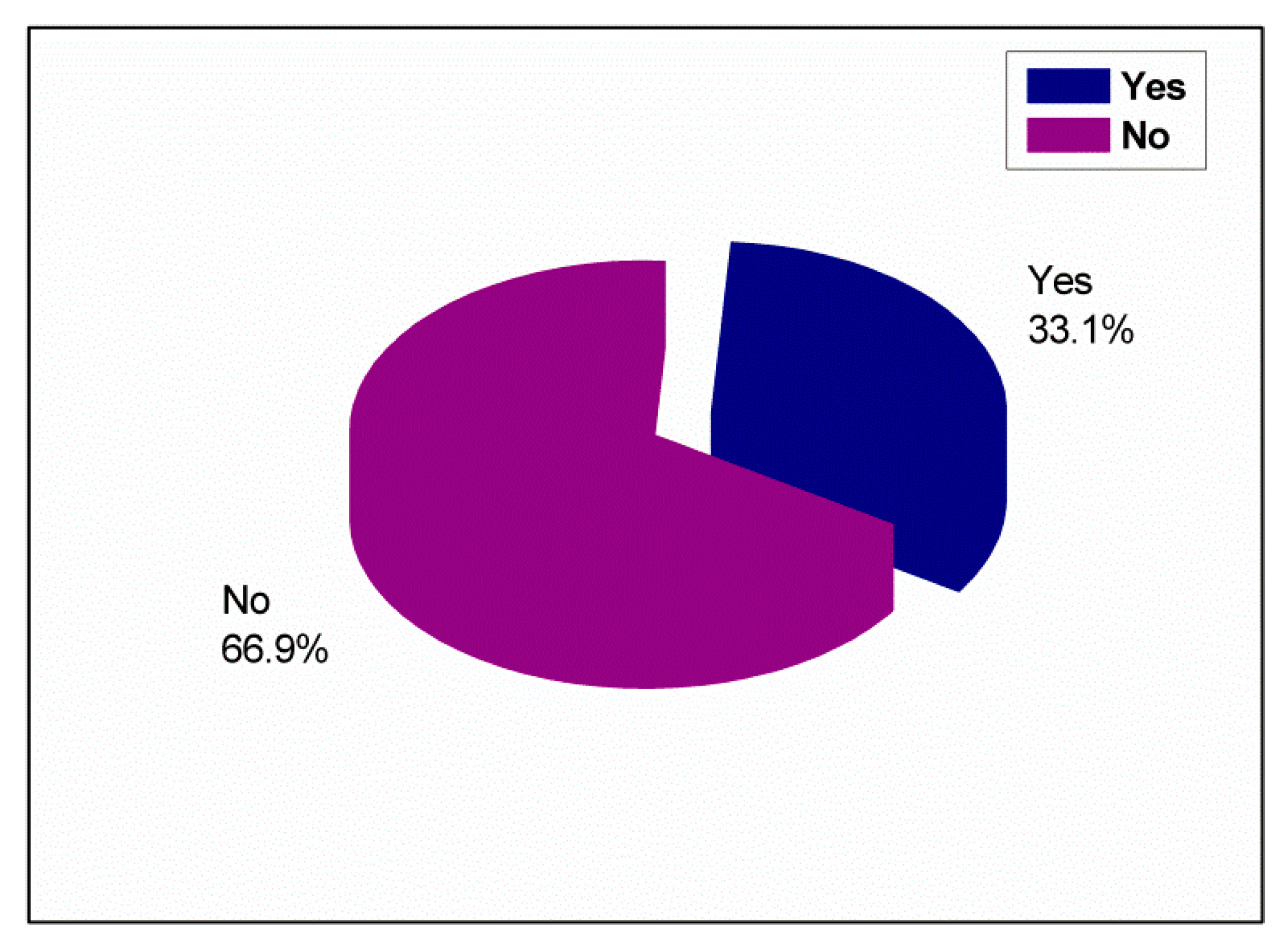
| Do you brush your teeth daily? | Yes | 179 | 33.1 | 118 | 25.4 | 61 | 81.3 | p < 0.001 |
| No | 361 | 66.9 | 347 | 74.6 | 14 | 18.7 | ||
| How many times do you brush your teeth daily? | Once | 90 | 50.2 | 84 | 71.2 | 6 | 9.8 | p < 0.001 |
| Twice | 64 | 35.8 | 16 | 13.5 | 48 | 78.7 | ||
| After each meal | 20 | 11.2 | 14 | 11.9 | 6 | 9.8 | ||
| More than three times | 5 | 2.8 | 4 | 3.4 | 1 | 1.7 | ||
| When do you brush your teeth? | Morning only | 12 | 6.7 | 7 | 5.9 | 5 | 8.2 | p < 0.001 |
| Evening only | 10 | 5.6 | 9 | 7.6 | 1 | 1.7 | ||
| Morning and evening | 77 | 43.1 | 27 | 22.9 | 50 | 82 | ||
| At any time | 80 | 44.6 | 75 | 63.6 | 5 | 8.1 | ||
| What type of toothbrush do you use? | Hard | 15 | 8.4 | 14 | 11.9 | 1 | 1.7 | p < 0.001 |
| Soft | 54 | 30.1 | 10 | 8.5 | 44 | 72.1 | ||
| Medium | 12 | 6.7 | 2 | 1.6 | 10 | 16.4 | ||
| Do not know | 98 | 54.8 | 92 | 78 | 6 | 9.8 | ||
| Do you use dental floss? | Yes | 120 | 22 | 81 | 17.4 | 39 | 52 | p < 0.001 |
| No | 420 | 78 | 384 | 82.6 | 36 | 48 | ||
| Do you use mouthwash? | Yes | 197 | 36.5 | 142 | 30.5 | 55 | 73.3 | p < 0.001 |
| No | 343 | 63.5 | 323 | 69.5 | 20 | 26.6 | ||
| How do you keep your gums healthy? | Brushing teeth with mouth wash | 88 | 16.3 | 36 | 7.7 | 52 | 69.3 | p < 0.001 |
| Rinsing the mouth with water after meals | 339 | 62.7 | 336 | 72.3 | 3 | 4 | ||
| Using mouthwash only | 54 | 10 | 50 | 10.8 | 4 | 5.3 | ||
| Taking vitamins | 59 | 11 | 43 | 9.2 | 16 | 21.4 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Qahtani, S.M.; Razak, P.A.; Khan, S.D. Knowledge and Practice of Preventive Measures for Oral Health Care among Male Intermediate Schoolchildren in Abha, Saudi Arabia. Int. J. Environ. Res. Public Health 2020, 17, 703. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17030703
Al-Qahtani SM, Razak PA, Khan SD. Knowledge and Practice of Preventive Measures for Oral Health Care among Male Intermediate Schoolchildren in Abha, Saudi Arabia. International Journal of Environmental Research and Public Health. 2020; 17(3):703. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17030703
Chicago/Turabian StyleAl-Qahtani, Saad Masood, Pervez Abdul Razak, and Siraj DAA Khan. 2020. "Knowledge and Practice of Preventive Measures for Oral Health Care among Male Intermediate Schoolchildren in Abha, Saudi Arabia" International Journal of Environmental Research and Public Health 17, no. 3: 703. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17030703