Development of the Rehabilitation Health Policy, Systems, and Services Research Field: Quantitative Analyses of Publications over Time (1990–2017) and across Country Type



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
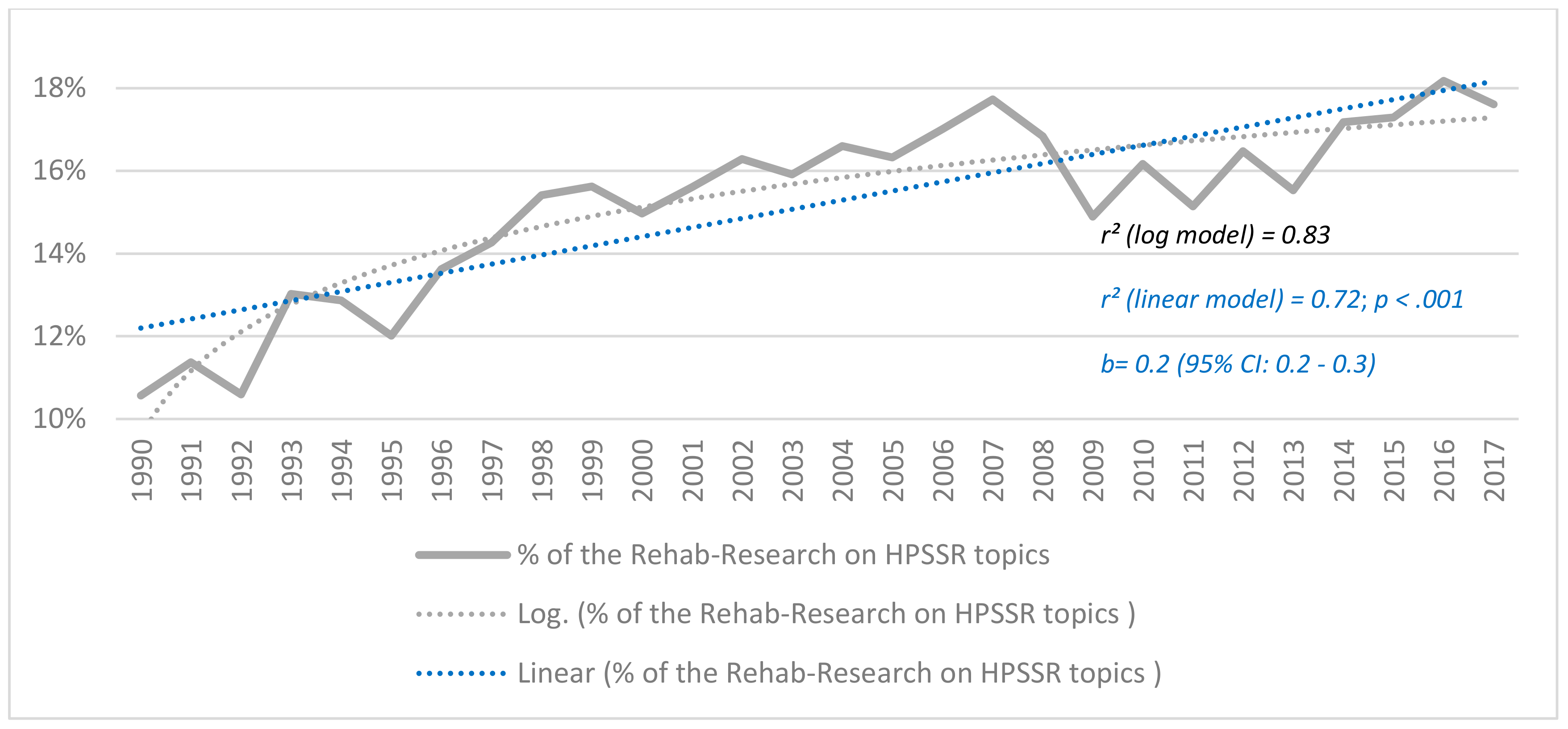
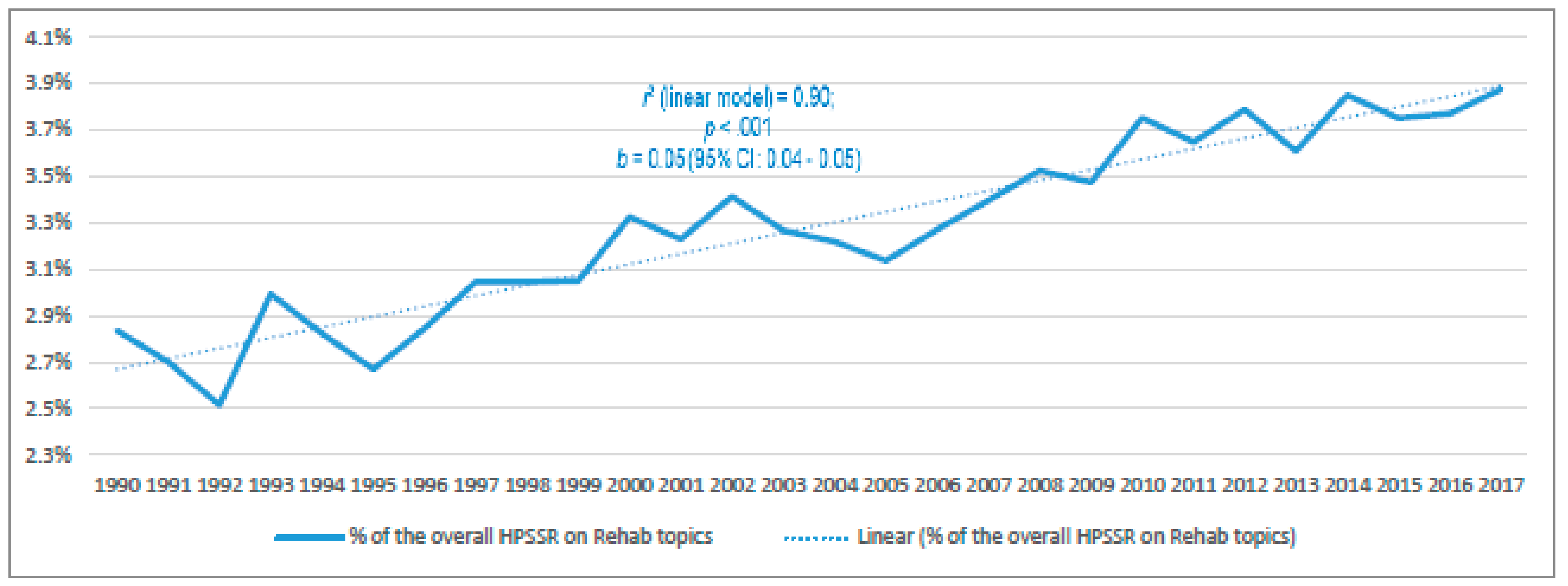
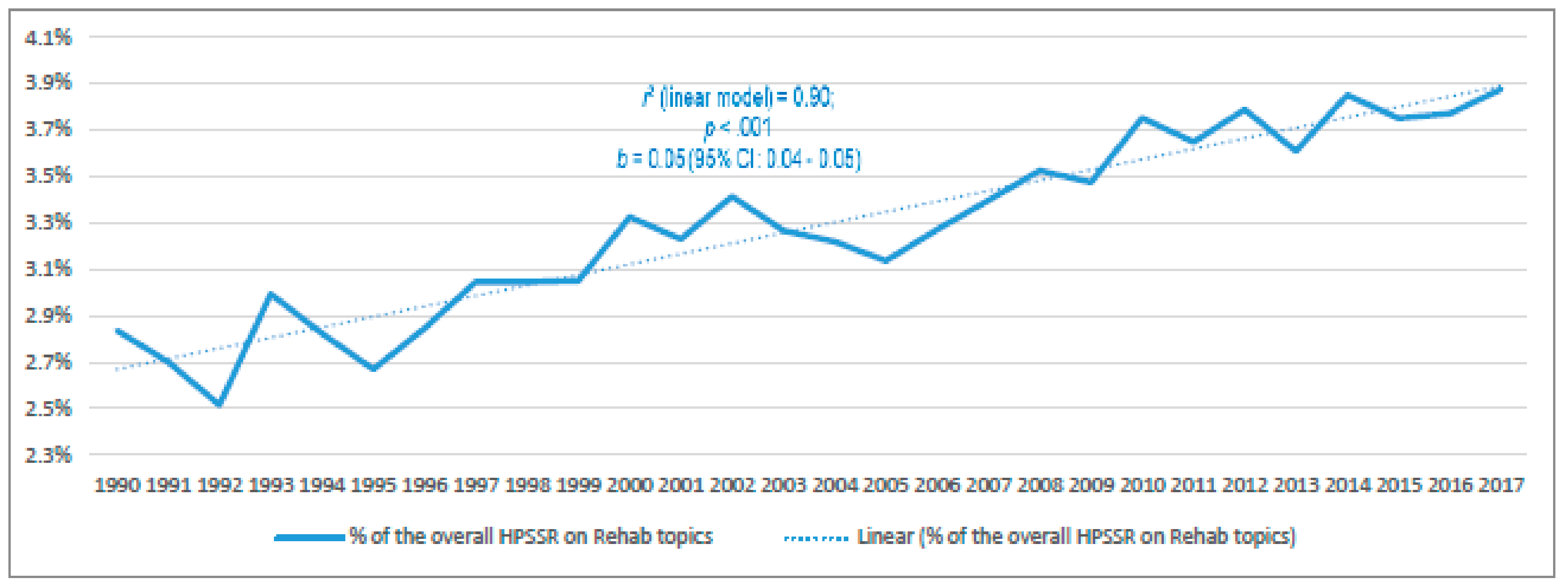
- What is the total amount, absolute growth, and relative growth of Rehabilitation HPSSR publications (i.e., as the percentage of all rehabilitation research publications, and as the percentage of all HPSSR publications)?
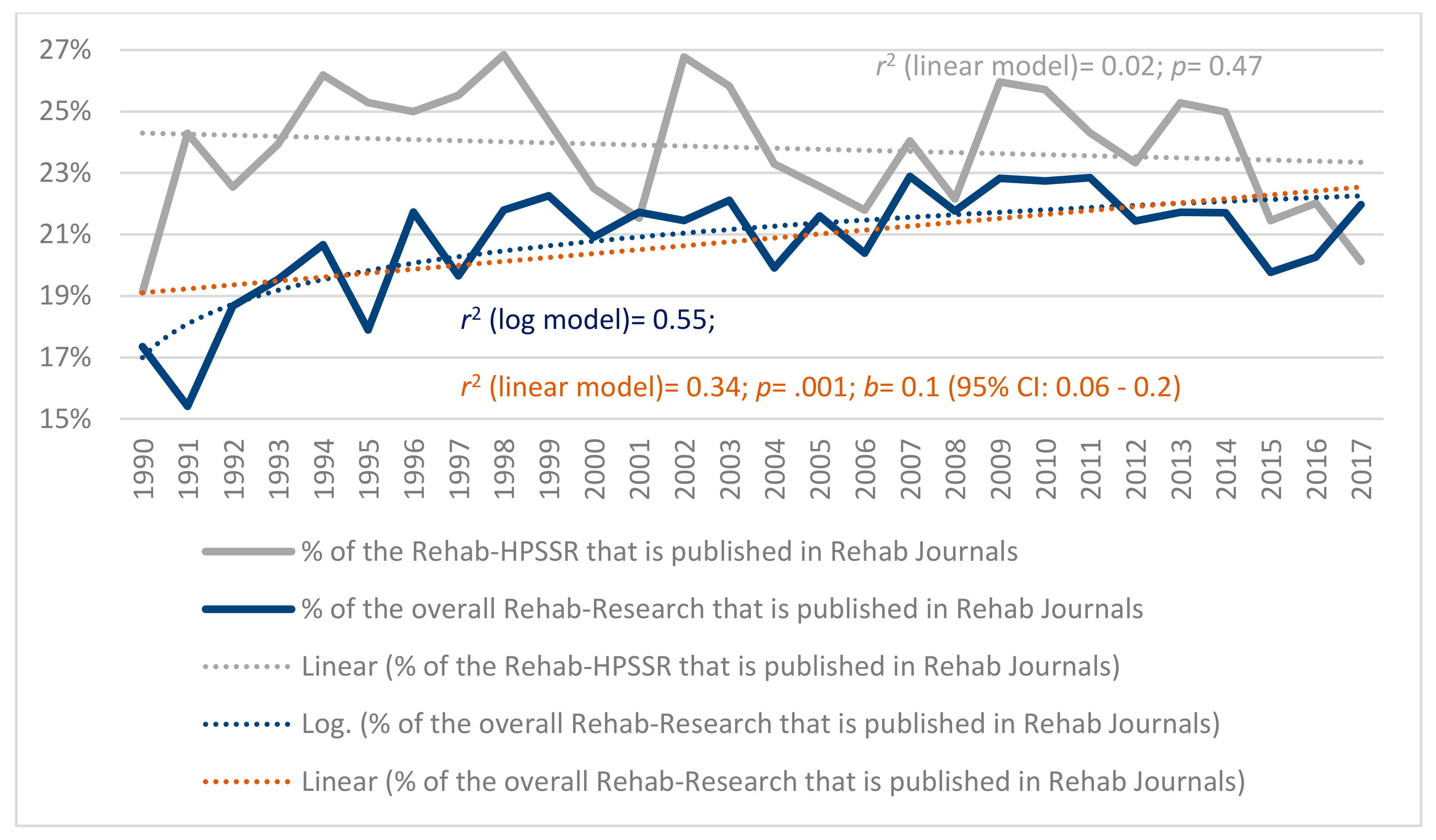
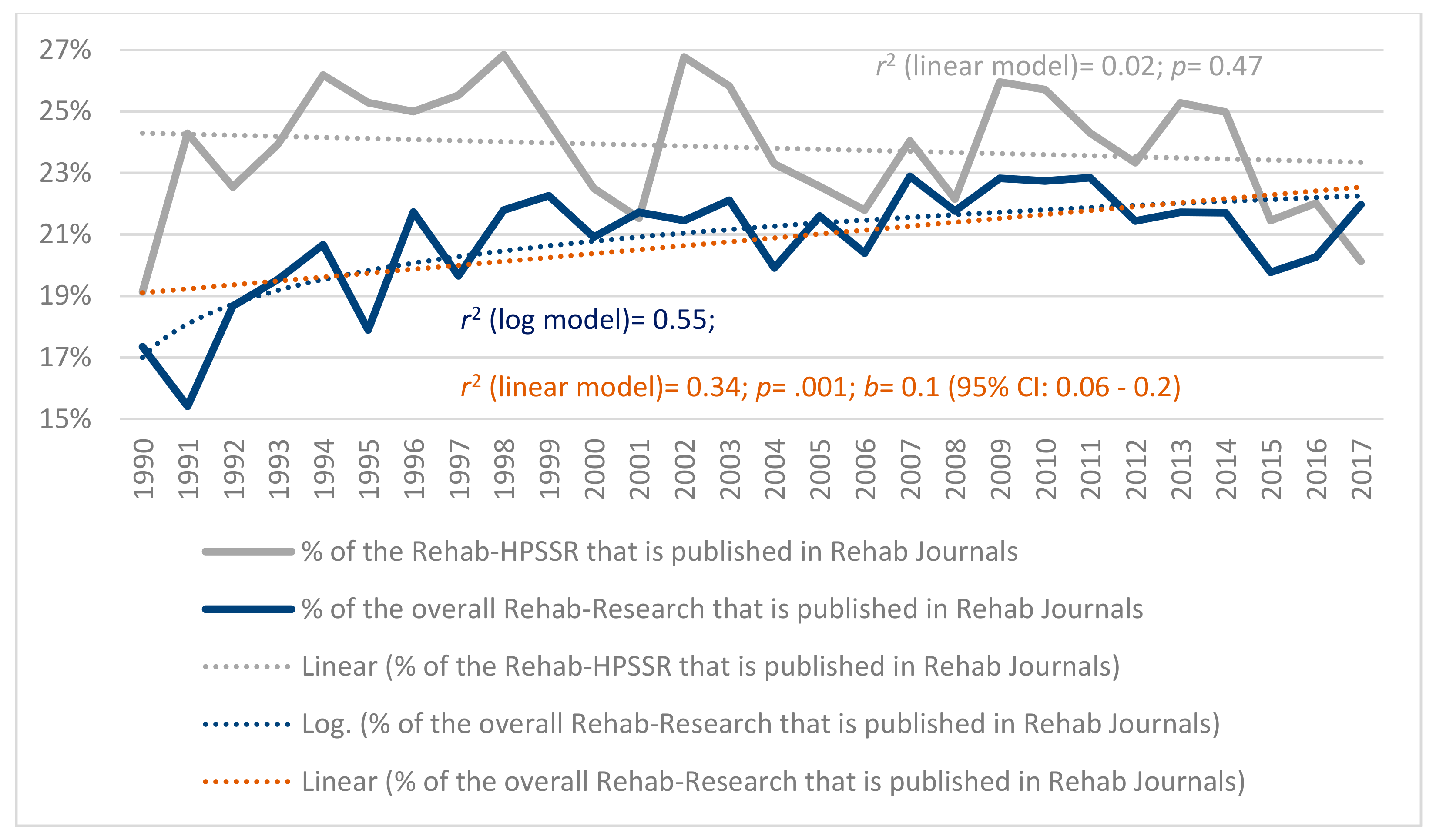
- Which portion of the Rehabilitation HPSSR has been published in rehabilitation journals, and has that changed over time?
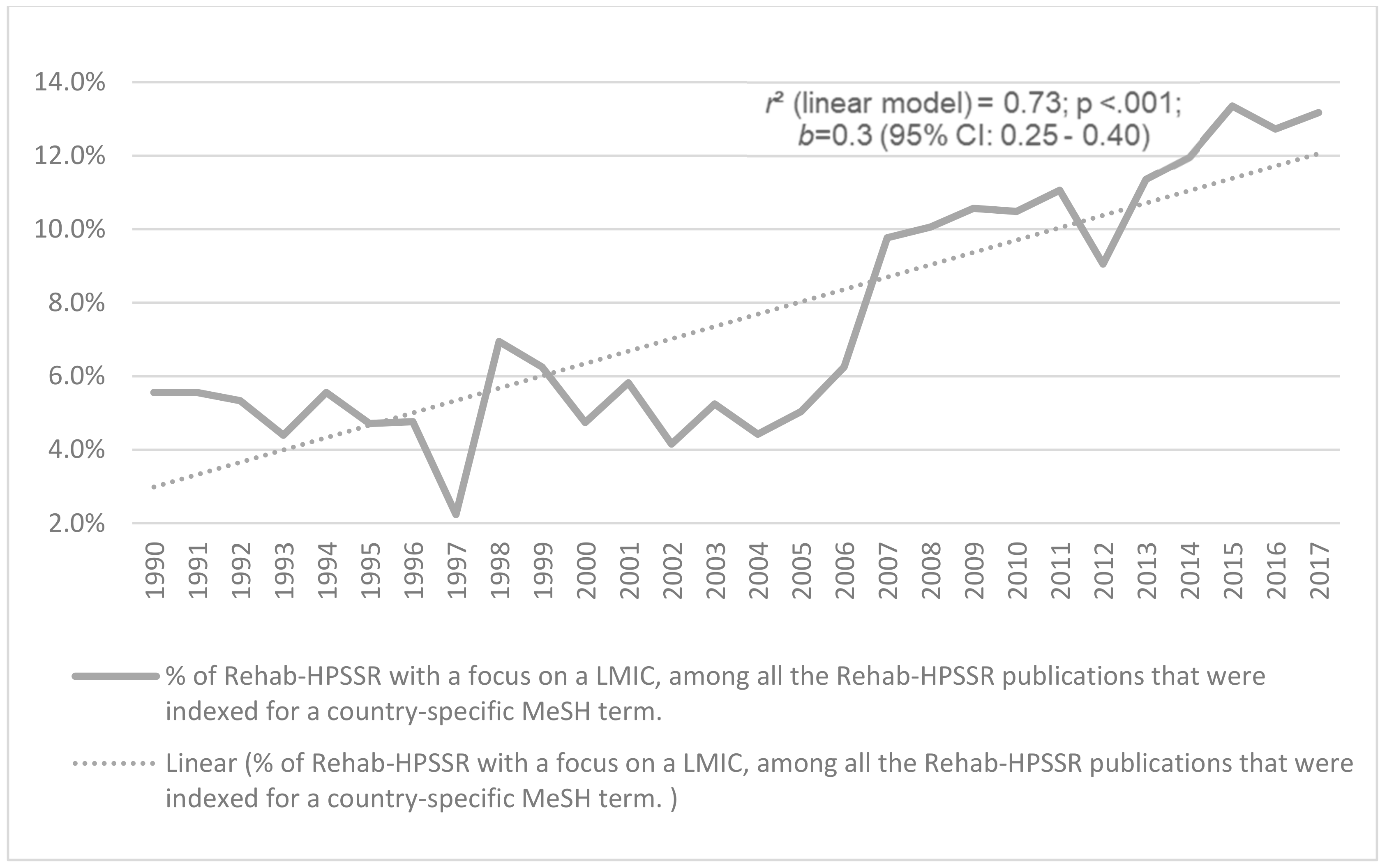
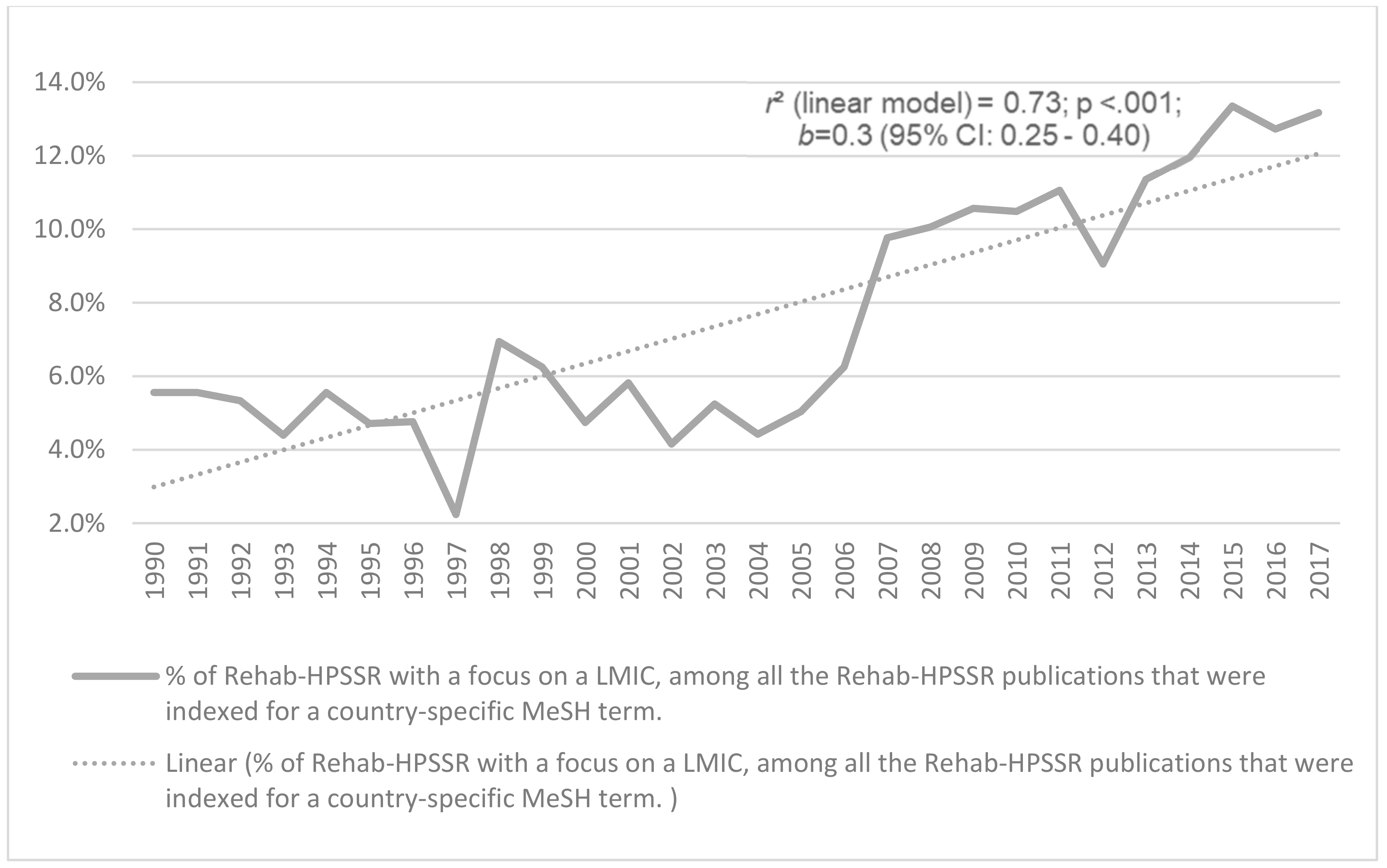
- Which portion of the country-specific rehabilitation HPSSR publications focus on high-income countries (HICs) versus low- and middle-income countries (LMICs)?
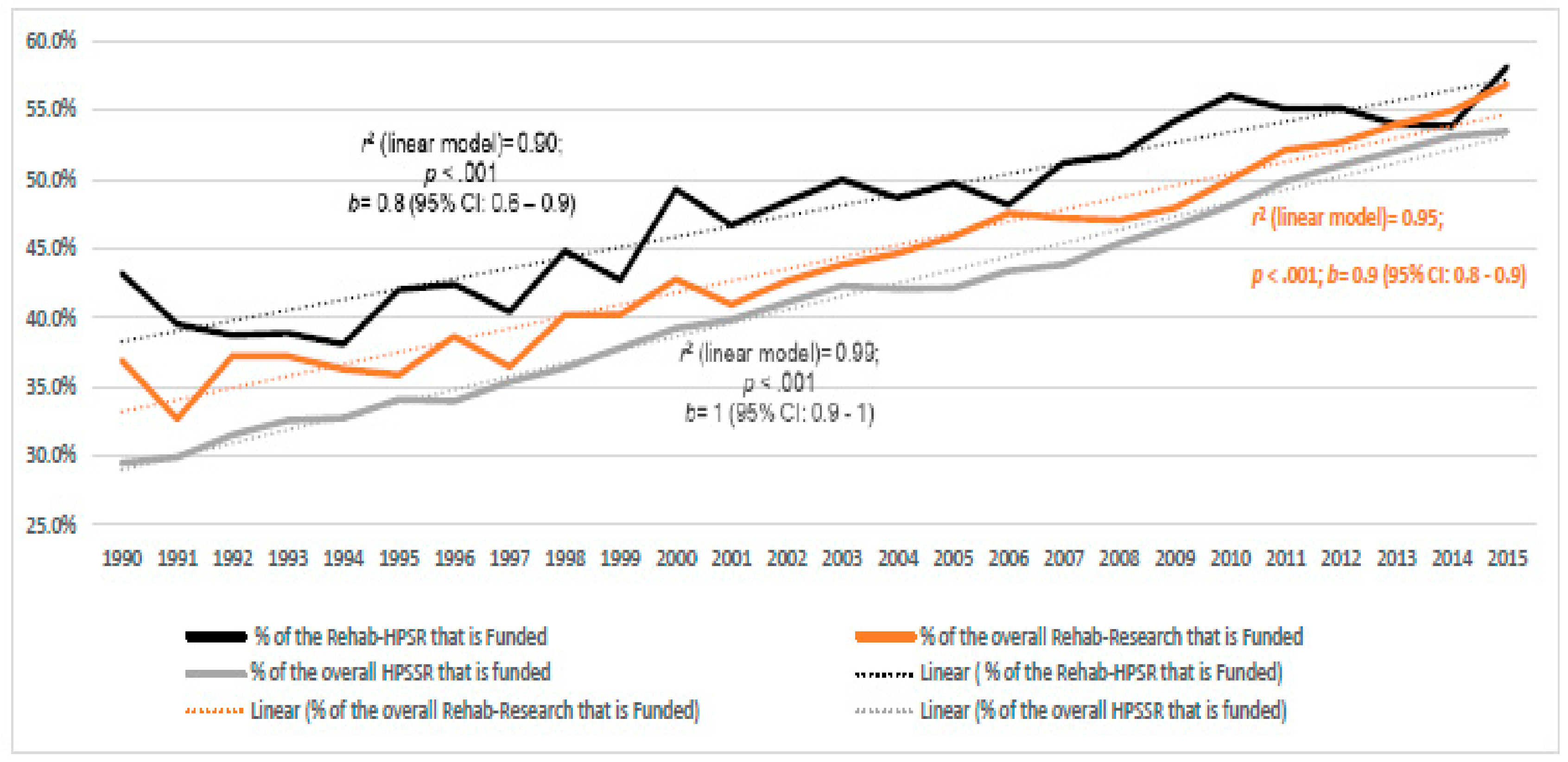
- What are the yearly rates of the Rehabilitation HPSSR publications that declare funding support, and how does that compare to rehabilitation research overall and HPSSR overall.
2. Materials and Methods
2.1. Design
2.2. Data Source
2.3. Search Filters–Construction
2.3.1. HPSSR
2.3.2. Rehabilitation
2.3.3. Research Publications in Humans
2.3.4. Journal Type
2.3.5. Funding Support
2.3.6. Country-Type
2.4. Search Filters–Calibration
2.5. Searches Conduct and Time Span
2.6. Data Extraction, Management and Analysis
3. Results
3.1. Absolute and Relative Growth
3.2. Journal Type
3.3. HICs Versus LMICs
3.4. Funding Support Declared
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A. Search Strategy
- In this Appendix, we present the complete search filters that were used. They enable the reproduction of the searches in PubMed (https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed). Of note, as the indexation process in PubMed is an ongoing endeavor; hence, values retrieved can be slightly higher than those presented in the results, especially for the number of articles published in the more recent years.
- Whenever reproducing the target searches, one needs to combine the relevant search filters below, using the Bolean operator “AND” in between.
- ○
- For example, in the search aimed at locating rehabilitation HPSSR, the following combination of search filters must be employed: the Common Filter (used into all searches) AND the HPSSR filter AND the Rehabilitation Filter.
- Search filters were based essentially on MeSH terms. All lower-level MeSH Terms, i.e., all under those actually written, are included by default, unless otherwise specified (i.e., with the use of the operator “NOT”).
- The hierarchical tree of MeSH terms, their definitions, and which MeSH terms are included under each MeSH term can be consulted at: https://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/mesh.
Note: Even though not written down, relevant MeSH terms such as but not limited to “Health Services Needs and Demand”[Majr] OR “Health Workforce”[Majr] OR “Health Services Accessibility”[Majr] OR “Health Equity” [Majr] are included into the search filter (i.e., fully contained within upper-level MeSH terms included, such as but not limited to “Health Administration”[Majr]). In practice, adding any of the terms exemplified above to the search filter do not change the total number of articles retrieved.
Note: Even though not written down, relevant MeSH terms such as but not limited to “Neurological Rehabilitation”[Majr] and “Cardiac Rehabilitation”[Majr] are included into the search filter (i.e., fully contained within upper-level MeSH terms included, such as “Rehabilitation”[Majr]). In practice, adding any of the illustrated MeSH terms to the search filter above do not change the total number of articles retrieved.
Note: This filter contains all the forms of funding support.
References
- Jesus, T.S.; Landry, M.D.; Hoenig, H. Global Need for Physical Rehabilitation: Systematic Analysis from the Global Burden of Disease Study 2017. Int. J. Environ. Res. Public Health 2019, 16, 980. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krug, E.; Cieza, A. Strengthening health systems to provide rehabilitation services. Bull. World Health Organ. 2017, 95, 167. [Google Scholar] [CrossRef] [PubMed]
- Foster, M.; Allen, S.; Fleming, J. Unmet health and rehabilitation needs of people with long-term neurological conditions in Queensland, Australia. Health Soc. Care Community 2015, 23, 292–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuentes, M.M.; Wang, J.; Haarbauer-Krupa, J.; Yeates, K.O.; Durbin, D.; Zonfrillo, M.R.; Jaffe, K.M.; Temkin, N.; Tulsky, D.; Bertisch, H.; et al. Unmet Rehabilitation Needs after Hospitalization for Traumatic Brain Injury. Pediatrics 2018, 141, e20172859. [Google Scholar] [CrossRef] [Green Version]
- Kamalakannan, S.; Venkata, M.G.; Prost, A.; Natarajan, S.; Pant, H.; Chitalurri, N.; Goenka, S.; Kuper, H. Rehabilitation Needs of Stroke Survivors after Discharge from Hospital in India. Arch. Phys. Med. Rehabil. 2016, 97, 1526–1532. [Google Scholar] [CrossRef] [Green Version]
- Kamenov, K.; Mills, J.A.; Chatterji, S.; Cieza, A. Needs and unmet needs for rehabilitation services: A scoping review. Disabil. Rehabil. 2019, 41, 1227–1237. [Google Scholar] [CrossRef]
- Singh, R.; Sinha, S.; Bill, A.; Turner-Stokes, L. Unmet need for specialised rehabilitation following neurosurgery: Can we maximise the potential cost-benefits? Br. J. Neurosurg. 2017, 31, 249–253. [Google Scholar] [CrossRef]
- Bright, T.; Wallace, S.; Kuper, H. A Systematic Review of Access to Rehabilitation for People with Disabilities in Low- and Middle-Income Countries. Int. J. Environ. Res. Public Health 2018, 15, 2165. [Google Scholar] [CrossRef] [Green Version]
- Magnusson, D.; Sweeney, F.; Landry, M. Provision of rehabilitation services for children with disabilities living in low- and middle-income countries: A scoping review. Disabil. Rehabil. 2019, 41, 861–868. [Google Scholar] [CrossRef]
- Graham, J.E.; Middleton, A.; Roberts, P.; Mallinson, T.; Prvu-Bettger, J. Health Services Research in Rehabilitation and Disability-The Time is Now. Arch. Phys. Med. Rehabil. 2018, 99, 198–203. [Google Scholar] [CrossRef]
- Rundell, S.D.; Goode, A.P.; Friedly, J.L.; Jarvik, J.G.; Sullivan, S.D.; Bresnahan, B.W. Role of Health Services Research in Producing High-Value Rehabilitation Care. Phys. Ther. 2015, 95, 1703–1711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McVeigh, J.; MacLachlan, M.; Gilmore, B.; McClean, C.; Eide, A.H.; Mannan, H.; Geiser, P.; Duttine, A.; Mji, G.; McAuliffe, E.; et al. Promoting good policy for leadership and governance of health-related rehabilitation: A realist synthesis. Glob. Health 2016, 12, 49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Health Policy and Systems Research Agenda for Rehabilitation: Concept Note; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Jesus, T.S.; Hoenig, H. Crossing the global quality chasm: Where does rehabilitation stand? Arch. Phys. Med. Rehabil. 2019, 100, 2215–2217. [Google Scholar] [CrossRef] [PubMed]
- Ghaffar, A.; Tran, N.; Langlois, E.; Shroff, Z.; Javadi, D. Alliance for Health Policy and Systems Research: Aims, achievements and ambitions. Public Health Res. Pract. 2017, 27, 2711703. [Google Scholar] [CrossRef] [Green Version]
- Mills, A. Health policy and systems research: Defining the terrain; identifying the methods. Health Policy Plan. 2012, 27, 1–7. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization & Alliance for Health Policy and Systems Research. Invest in Knowledge for Resilient Health Systems; World Health Organization & Alliance for Health Policy and Systems Research: Geneva, Switzerland, 2016. [Google Scholar]
- Peters, D.H. Health policy and systems research: The future of the field. Health Res. Policy Syst. 2018, 16, 84. [Google Scholar] [CrossRef] [Green Version]
- Bennett, S.; Frenk, J.; Mills, A. The evolution of the field of Health Policy and Systems Research and outstanding challenges. Health Res. Policy Syst. 2018, 16, 43. [Google Scholar] [CrossRef]
- Sheikh, K.; Gilson, L.; Agyepong, I.A.; Hanson, K.; Ssengooba, F.; Bennett, S. Building the field of health policy and systems research: Framing the questions. PLoS Med. 2011, 8, e1001073. [Google Scholar] [CrossRef] [Green Version]
- Adam, T.; Ahmad, S.; Bigdeli, M.; Ghaffar, A.; Rottingen, J.A. Trends in health policy and systems research over the past decade: Still too little capacity in low-income countries. PLoS ONE 2011, 6, e27263. [Google Scholar] [CrossRef]
- Javadi, D.; Tran, N.; Ghaffar, A. Building a Workforce for Future Health Systems: Reflections from Health Policy and Systems Research. Health Serv. Res. 2018, 53, 4024–4033. [Google Scholar] [CrossRef] [Green Version]
- Lohr, K.N.; Steinwachs, D.M. Health services research: An evolving definition of the field. Health Serv. Res. 2002, 37, 7–9. [Google Scholar]
- Agency for Healthcare Research and Quality. Health Services Research: A Definition. Available online: https://www.ahrq.gov/funding/training-grants/hsrguide/hsrguide.html (accessed on 11 October 2019).
- Bettger, J.P.; Nguyen, V.Q.; Thomas, J.G.; Guerrier, T.; Yang, Q.; Hirsch, M.A.; Pugh, T.; Harris, G.; Eller, M.A.; Pereira, C.; et al. Turning Data into Information: Opportunities to Advance Rehabilitation Quality, Research, and Policy. Arch. Phys. Med. Rehabil. 2018, 99, 1226–1231. [Google Scholar] [CrossRef] [PubMed]
- Spyra, K.; Muller-Fahrnow, W. Rehabilitation as a subject of health services research. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2006, 49, 188–197. [Google Scholar] [CrossRef] [PubMed]
- Jette, A.M. Health Services Research in the 21st Century. Phys. Ther. 2019, 99, 255–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skempes, D.; Melvin, J.; von Groote, P.; Stucki, G.; Bickenbach, J. Using concept mapping to develop a human rights based indicator framework to assess country efforts to strengthen rehabilitation provision and policy: The Rehabilitation System Diagnosis and Dialogue framework (RESYST). Glob. Health 2018, 14, 96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jesus, T.S.; Landry, M.D.; Dussault, G.; Fronteira, I. Human resources for health (and rehabilitation): Six Rehab-Workforce Challenges for the century. Hum. Resour. Health 2017, 15, 8. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Rehabilitation in Health Systems: Guide for Action; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Global Rehabilitation Alliance. About Us. Available online: http://global-rehabilitation-alliance.org/about-us-1.html (accessed on 4 October 2019).
- America Congress of Rehabilitation Medicine. Health Services Research Networking Group. Available online: https://acrm.org/acrm-communities/health-services-research/ (accessed on 5 October 2019).
- National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR). 2018–2023 Long-Range Plan 2019. Available online: https://acl.gov/sites/default/files/about-acl/2019-01/NIDILRR%20LRP-2018-2023-Final.pdf (accessed on 20 September 2019).
- Resnik, L.; Freburger, J.K. Health Services Research: Physical Therapy Has Arrived! Phys. Ther. 2015, 95, 1605–1607. [Google Scholar] [CrossRef] [Green Version]
- Jesus, T.S. Systematic Reviews and Clinical Trials in Rehabilitation: Comprehensive Analyses of Publication Trends. Arch. Phys. Med. Rehabil. 2016, 97, 1853–1862. [Google Scholar] [CrossRef]
- Jesus, T.S.; Colquhoun, H.L. Publication trends of study protocols in rehabilitation. Eur. J. Phys. Rehabil. Med. 2018, 54, 785–791. [Google Scholar] [CrossRef]
- Jesus, T.S.G.S.; Castellini, G.; Colquhoun, H.; Brooks, D. Evolving physiotherapy research publications between 2005 and 2015. Physiothe. Can. 2019. [Google Scholar] [CrossRef]
- Kamper, S.J.; Moseley, A.M.; Herbert, R.D.; Maher, C.G.; Elkins, M.R.; Sherrington, C. 15 years of tracking physiotherapy evidence on PEDro, where are we now? Br. J. Sports Med. 2015, 49, 907–909. [Google Scholar] [CrossRef] [Green Version]
- Negrini, S.; Levack, W.; Gimigliano, F.; Arienti, C.; Villafane, J.H.; Kiekens, C. The Struggle for Evidence in Physical and Rehabilitation Medicine: Publication Rate of Randomized Controlled Trials and Systematic Reviews Is Growing More Than in Other Therapeutic Fields. Am. J. Phys. Med. Rehabil. 2019, 98, 258–265. [Google Scholar] [CrossRef] [PubMed]
- English, K.M.; Pourbohloul, B. Increasing health policy and systems research capacity in low- and middle-income countries: Results from a bibliometric analysis. Health Res. Policy Syst. 2017, 15, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macarayan, E.K.; Balabanova, D.; Gotsadze, G. Assessing the field of health policy and systems research using symposium abstract submissions and machine learning techniques. Health Policy Plan. 2019, 34, 721–731. [Google Scholar] [CrossRef] [PubMed]
- English, K.M.; Pourbohloul, B. Health policy and systems research collaboration pathways: Lessons from a network science analysis. Health Res. Policy Syst. 2017, 15, 71. [Google Scholar] [CrossRef] [Green Version]
- Bouchard, L.; Albertini, M.; Batista, R.; de Montigny, J. Research on health inequalities: A bibliometric analysis (1966–2014). Soc. Sci. Med. 1982 2015, 141, 100–108. [Google Scholar] [CrossRef]
- Defor, S.; Kwamie, A.; Agyepong, I.A. Understanding the state of health policy and systems research in West Africa and capacity strengthening needs: Scoping of peer-reviewed publications trends and patterns 1990–2015. Health Res. Policy Syst. 2017, 15, 55. [Google Scholar] [CrossRef] [Green Version]
- Simpson, L.A.; Koechlein, L.; Menachemi, N.; Wolfe, M.J. Show Me the Money! Trends in Funding for Health Services Research. Health Serv. Res. 2018, 53, 3967–3975. [Google Scholar] [CrossRef]
- Halladay, C.W.; Trikalinos, T.A.; Schmid, I.T.; Schmid, C.H.; Dahabreh, I.J. Using data sources beyond PubMed has a modest impact on the results of systematic reviews of therapeutic interventions. J. Clin. Epidemiol. 2015, 68, 1076–1084. [Google Scholar] [CrossRef]
- Booth, A. Over 85% of included studies in systematic reviews are on MEDLINE. J. Clin. Epidemiol. 2016, 79, 165–166. [Google Scholar] [CrossRef] [Green Version]
- Mimouni, M.; Cismariu-Potash, K.; Ratmansky, M.; Shaklai, S.; Amir, H.; Mimouni-Bloch, A. Trends in Physical Medicine and Rehabilitation Publications Over the Past 16 Years. Arch. Phys. Med. Rehabil. 2016, 97, 1030–1033. [Google Scholar] [CrossRef] [PubMed]
- Bastian, H.; Glasziou, P.; Chalmers, I. Seventy-five trials and eleven systematic reviews a day: How will we ever keep up? PLoS Med. 2010, 7, e1000326. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Dong, M.; Zhou, K.; Mita, C.; Liu, J.; Wayne, P.M. Publication Trends in Acupuncture Research: A 20-Year Bibliometric Analysis Based on PubMed. PLoS ONE 2016, 11, e0168123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hung, B.T.; Long, N.P.; Le Phi Hung, N.T.; Anh, N.H.; Nghi, T.D.; Van Hieu, M.; Trang, N.T.; Rafidinarivo, H.F.; Anh, N.K.; Hawkes, D.; et al. Research trends in evidence-based medicine: A joinpoint regression analysis of more than 50 years of publication data. PLoS ONE 2015, 10, e0121054. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richter, R.R.; Austin, T.M. Using MeSH (medical subject headings) to enhance PubMed search strategies for evidence-based practice in physical therapy. Phys. Ther. 2012, 92, 124–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jesus, T.S.; Bright, F.A.; Pinho, C.S.; Papadimitriou, C.; Kayes, N.M.; Cott, C.A. Scoping review of the person-centered literature in adult physical rehabilitation. Disabil. Rehabil. 2019, 1–11. [Google Scholar] [CrossRef]
- Jesus, T.S.; Hoenig, H. Postacute rehabilitation quality of care: Toward a shared conceptual framework. Arch. Phys. Med. Rehabil. 2015, 96, 960–969. [Google Scholar] [CrossRef]
- Meyer, T.; Gutenbrunner, C.; Bickenbach, J.; Cieza, A.; Melvin, J.; Stucki, G. Towards a conceptual description of rehabilitation as a health strategy. J. Rehabil. Med. 2011, 43, 765–769. [Google Scholar] [CrossRef] [Green Version]
- European Physical and Rehabilitation Medicine Bodies Alliance. White Book on Physical and Rehabilitation Medicine (PRM) in Europe. Chapter 1. Definitions and concepts of PRM. Eur. J. Phys. Rehabil. Med. 2018, 54, 156–165. [Google Scholar]
- O’Mara, A.; Rowland, J.H.; Greenwell, T.N.; Wiggs, C.L.; Fleg, J.; Joseph, L.; McGowan, J.; Panagis, J.S.; Washabaugh, C.; Peng, G.C.; et al. National Institutes of Health Research Plan on Rehabilitation: NIH Medical Rehabilitation Coordinating Committee. Phys. Ther. 2017, 97, 104–407. [Google Scholar]
- MacLachlan, M.; McVeigh, J.; Cooke, M.; Ferri, D.; Holloway, C.; Austin, V.; Javadi, D. Intersections Between Systems Thinking and Market Shaping for Assistive Technology: The SMART (Systems-Market for Assistive and Related Technologies) Thinking Matrix. Int. J. Environ. Res. Public Health 2018, 15, 2627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atkins, D.; Kilbourne, A.M.; Shulkin, D. Moving from Discovery to System-Wide Change: The Role of Research in a Learning Health Care System: Experience from Three Decades of Health Systems Research in the Veterans Health Administration. Annu. Rev. Public Health 2017, 38, 467–487. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine. Best Care at Lower Cost: The Path to Continuously Learning Health Care in America; Institute of Medicine: Washington, DC, USA, 2012. [Google Scholar]
- Jesus, T.S.; Landry, M.; Brooks, D.; Hoenig, H. Physical Rehabilitation Needs Per Condition Type: Results from the Global Burden of Disease study 2017. Arch. Phys. Med. Rehabi. 2019. [Google Scholar]
- Louw, Q.; Twizeyemariya, A.; Grimmer, K.; Leibbrandt, D. Estimating the costs and benefits of stroke rehabilitation in South Africa. J. Eval. Clin. Pract. 2019. [Google Scholar] [CrossRef]
- Howard-Wilsher, S.; Irvine, L.; Fan, H.; Shakespeare, T.; Suhrcke, M.; Horton, S.; Poland, F.; Hooper, L.; Song, F. Systematic overview of economic evaluations of health-related rehabilitation. Disabil. Health J. 2016, 9, 11–25. [Google Scholar] [CrossRef] [Green Version]
- Shields, G.E.; Wells, A.; Doherty, P.; Heagerty, A.; Buck, D.; Davies, L.M. Cost-effectiveness of cardiac rehabilitation: A systematic review. Heart Br. Card. Soc. 2018, 104, 1403–1410. [Google Scholar] [CrossRef]
- Burge, E.; Monnin, D.; Berchtold, A.; Allet, L. Cost-Effectiveness of Physical Therapy Only and of Usual Care for Various Health Conditions: Systematic Review. Phys. Ther. 2016, 96, 774–786. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization & the World Bank. World Report on Disability; World Health Organization & the World Bank: Geneva, Switzerland, 2011. [Google Scholar]
- Menachemi, N.; Simpson, L.A.; Wolfe, M.J. Positioning the Health Services Research Workforce for Continued Success: Recommendations from AcademyHealth Stakeholders. Health Serv. Res. 2018, 53, 4041–4050. [Google Scholar] [CrossRef] [Green Version]
- Mor, V.; Wallace, P. Funding the Training of Future Health Services Researchers. Health Serv. Res. 2018, 53, 3976–3984. [Google Scholar] [CrossRef]
- Frogner, B.K. Update on the Stock and Supply of Health Services Researchers in the United States. Health Serv. Res. 2018, 53, 3945–3966. [Google Scholar] [CrossRef] [Green Version]
- Lembani, M.; Teddy, G.; Molosiwa, D.; Hwabamungu, B. Post-doctoral research fellowship as a health policy and systems research capacity development intervention: A case of the CHESAI initiative. Health Res. Policy Syst. 2016, 14, 89. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Izugbara, C.O.; Kabiru, C.W.; Amendah, D.; Dimbuene, Z.T.; Donfouet, H.P.; Atake, E.H.; Ingabire, M.G.; Maluka, S.; Mumah, J.N.; Mwau, M.; et al. “It takes more than a fellowship program”: Reflections on capacity strengthening for health systems research in sub-Saharan Africa. BMC Health Serv. Res. 2017, 17, 696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowsher, G.; Papamichail, A.; El Achi, N.; Ekzayez, A.; Roberts, B.; Sullivan, R.; Patel, P. A narrative review of health research capacity strengthening in low and middle-income countries: Lessons for conflict-affected areas. Glob. Health 2019, 15, 23. [Google Scholar] [CrossRef] [PubMed]
- Moses, H.; Matheson, D.H., III; Cairns-Smith, S.; George, B.P.; Palisch, C.; Dorsey, E.R. The anatomy of medical research: US and international comparisons. JAMA 2015, 313, 174–189. [Google Scholar] [CrossRef] [PubMed]
- Nugraha, B.; Setyono, G.R.; Defi, I.R.; Gutenbrunner, C. Strengthening rehabilitation services in Indonesia: A brief situation analysis. J. Rehabil. Med. 2018, 50, 377–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gutenbrunner, C.; Nugraha, B. Responding to the World Health Organization Global Disability Action Plan in Egypt: A Technical Consultancy to develop a National Disability, Health and Rehabilitation Plan. J. Rehabil. Med. 2018, 50, 333–337. [Google Scholar] [CrossRef] [Green Version]


© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jesus, T.S.; Hoenig, H.; Landry, M.D. Development of the Rehabilitation Health Policy, Systems, and Services Research Field: Quantitative Analyses of Publications over Time (1990–2017) and across Country Type. Int. J. Environ. Res. Public Health 2020, 17, 965. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17030965
Jesus TS, Hoenig H, Landry MD. Development of the Rehabilitation Health Policy, Systems, and Services Research Field: Quantitative Analyses of Publications over Time (1990–2017) and across Country Type. International Journal of Environmental Research and Public Health. 2020; 17(3):965. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17030965
Chicago/Turabian StyleJesus, Tiago S., Helen Hoenig, and Michel D. Landry. 2020. "Development of the Rehabilitation Health Policy, Systems, and Services Research Field: Quantitative Analyses of Publications over Time (1990–2017) and across Country Type" International Journal of Environmental Research and Public Health 17, no. 3: 965. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17030965