Analysis of Network Structure and Doctor Behaviors in E-Health Communities from a Social-Capital Perspective


Abstract
:1. Introduction
2. Materials and Methods
2.1. Description of the Sample
2.2. Instruments Used to Collect Data and Variables
2.3. Definition and Measurement of Social-Capital Theory
3. Results
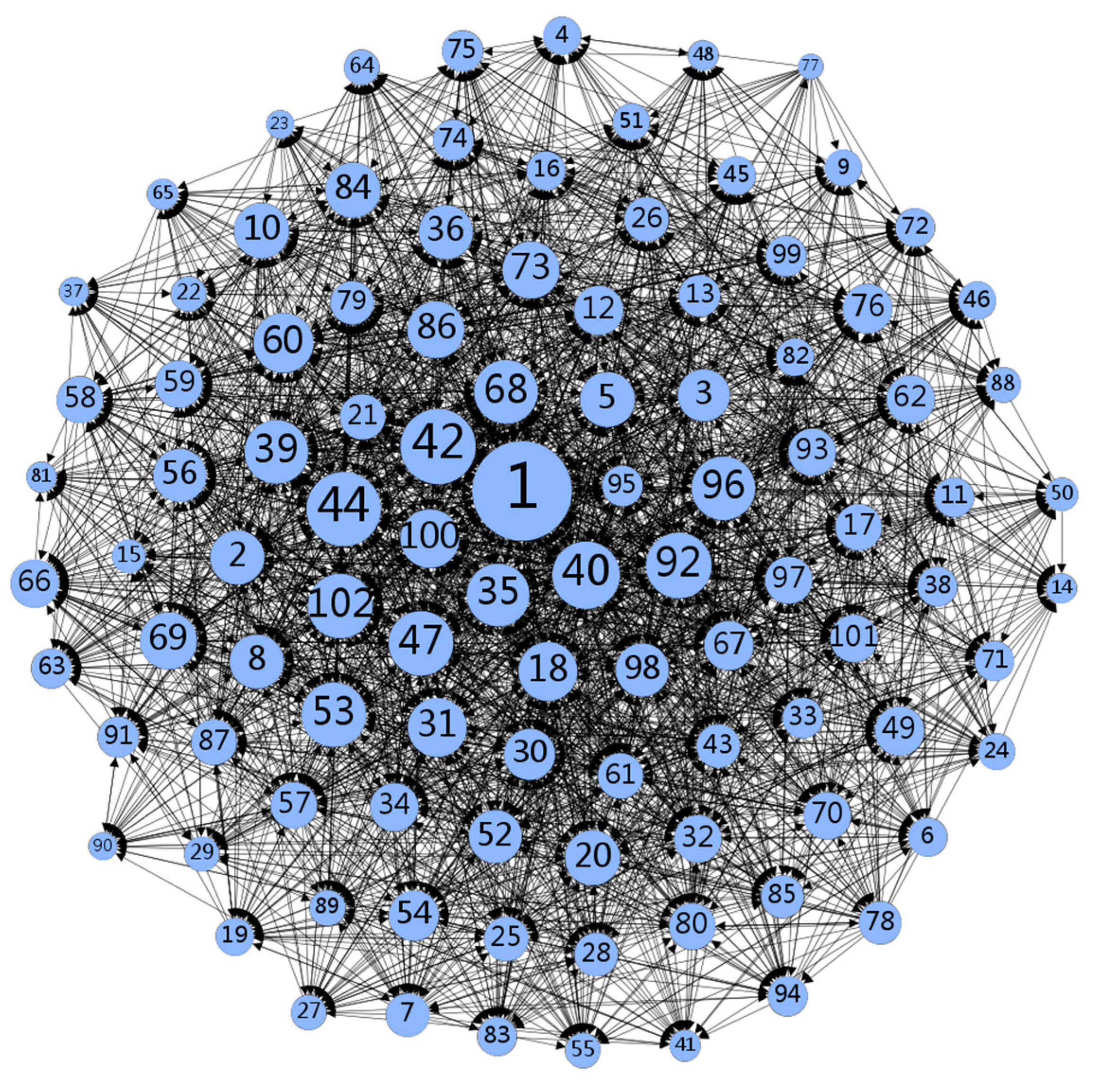
3.1. Network Analysis
3.2. Interaction Frequency
3.3. Emotional Density
3.3.1. Density and Centralization
3.3.2. Geodesic Distance
3.4. Familiarity between Subjects or Mutual Trust
3.4.1. Centrality
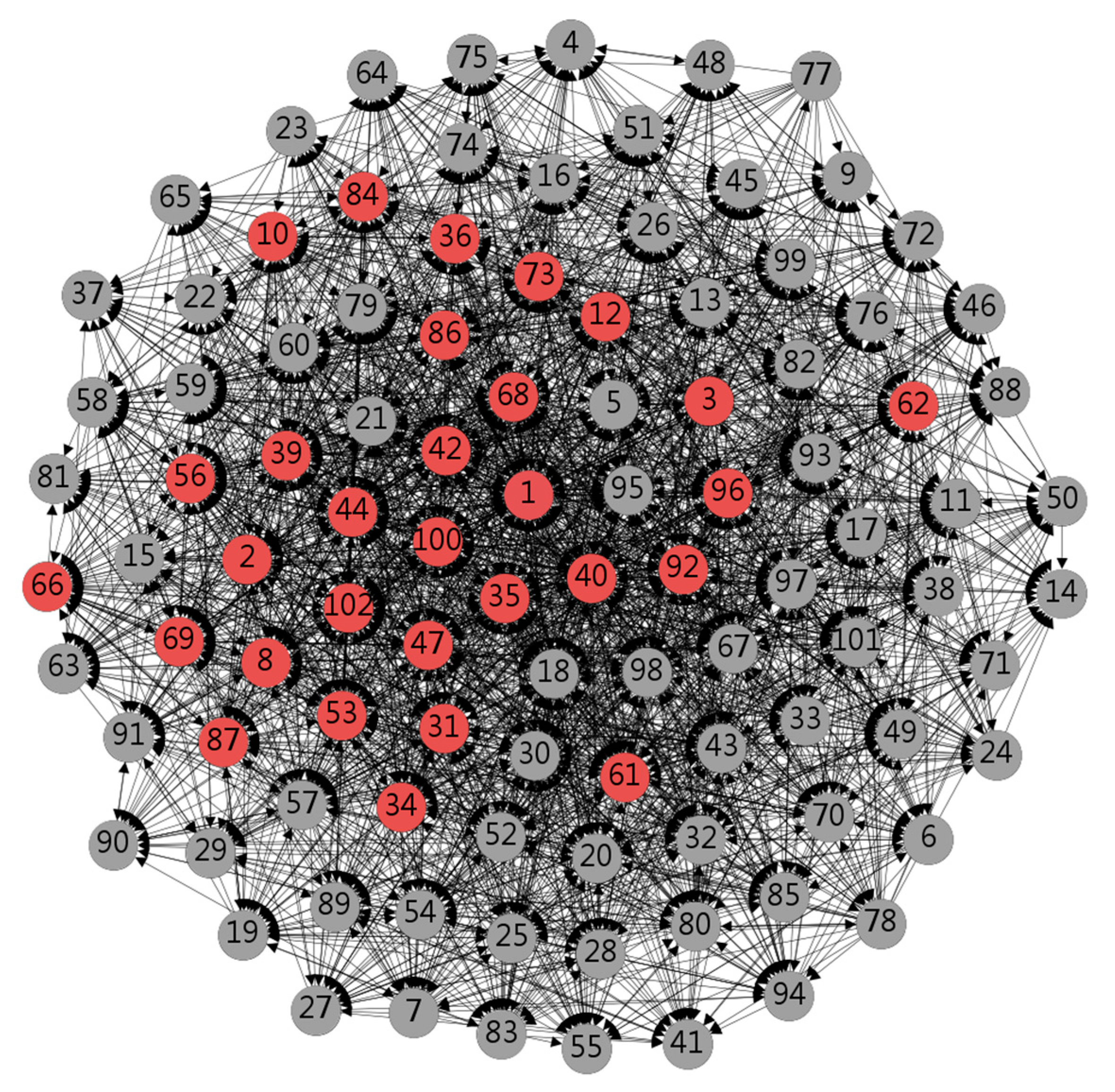
3.4.2. Core–Periphery Model
3.5. Reciprocal Exchange
4. Discussion
4.1. Sense of Identity in the Network is Positively Related to Participation
4.2. Close Communication of Information in the E-Health Community
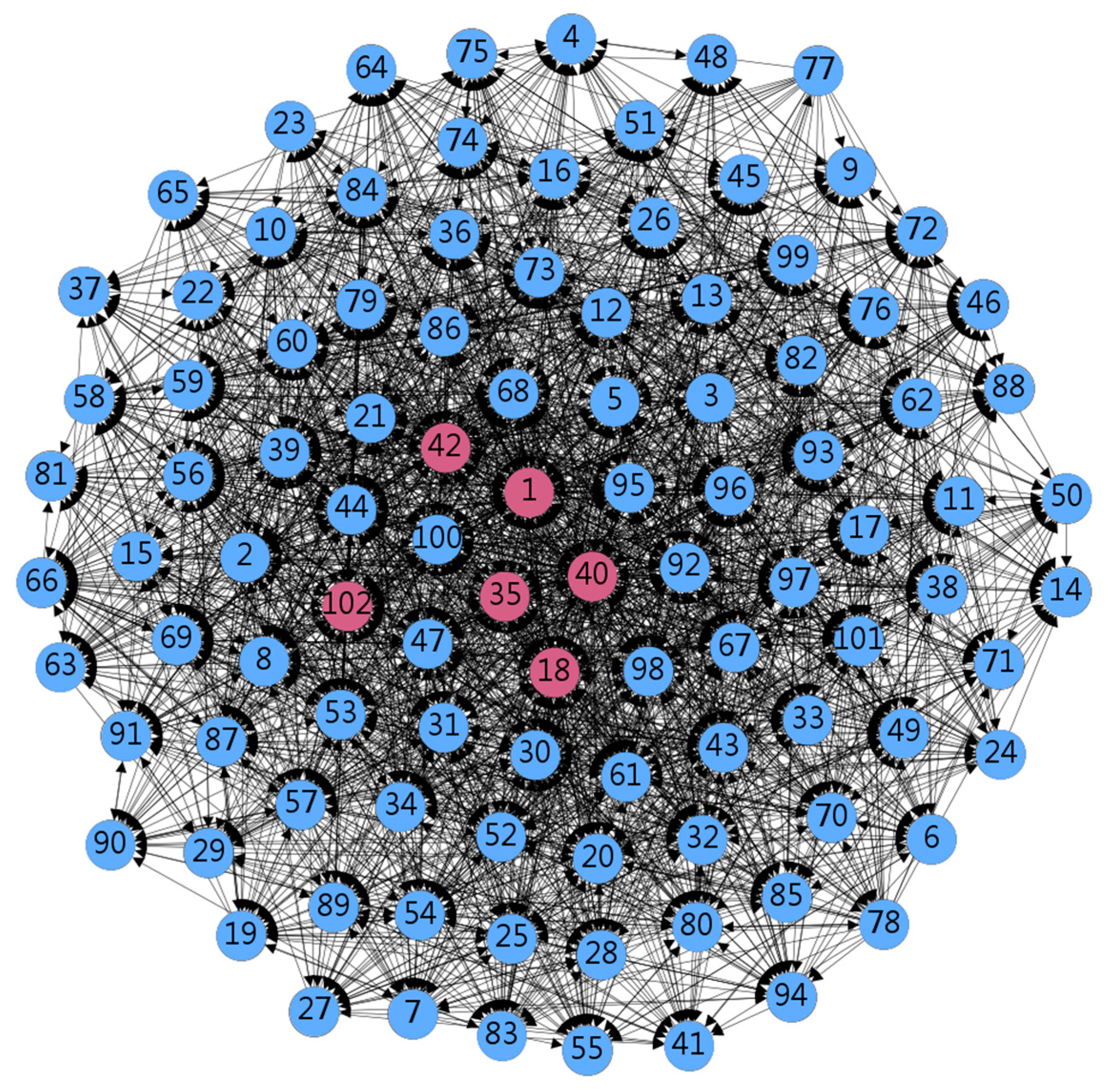
4.3. Significant Positions of Doctors with Higher Professional Titles
4.4. Ethics and Data Privacy
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Tang, Y.; Yang, Y.-T.; Shao, Y.S. Acceptance of Online Medical Websites: An Empirical Study in China. Environ. Res. Public Health 2019, 16, 943. [Google Scholar] [CrossRef] [Green Version]
- Petrasek, D.; Barr, A.; Palem, K.V. The virtual hospital: The emergence of telemedicine. In Proceedings of the International Conference on Compilers, Scottsdale, AZ, USA, 24–29 October 2010. [Google Scholar]
- Pascoe, K.; Lobosco, S.; Bell, D.; Hoskin, B.; Chang, D.J.; Pobiner, B. Ramachandran S Patient- and Physician-Reported Satisfaction with Systemic Lupus Erythematosus Treatment in US Clinical Practice. Clin. Ther. 2017, 399, 1811–1826. [Google Scholar] [CrossRef] [Green Version]
- Hyland, P.; Raymond, E.; Chong, E. A direct-to-patient telemedicine abortion service in Australia: Retrospective analysis of the first 18 months. Contraception 2018, 975, 461–462. [Google Scholar] [CrossRef]
- Gu, Y.; Hsu, H.T.; Zhu, J.; Zheng, X.; Jiang, H.; Fan, H.; Yang, T.A. systematic survey on the diagnosis strategy and patient management of type 1 diabetes by Chinese physicians. Sci. China Life Sci. 2018, 613, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.; Guo, X.; Zhang, X.; Vogel, D. Doctor–patient relationship strength’s impact in an online healthcare community. Inf. Technol. Dev. 2018, 24, 279–300. [Google Scholar] [CrossRef]
- Fang, G.; Su, L.; Wang, Q.; Wang, J. Medical community expert classification based on potential semantic feature transfer learning. In Proceedings of the 2017 29th Chinese Control and Decision Conference (CCDC), Chongqing, China, 28–30 May 2017; IEEE: Piscataway, NJ, USA, 2017. [Google Scholar]
- Chinese Science and Technology Consultation. 2018 Life Service E-commerce User Activity List [EB/OL]. Available online: http://www.100ec.cn/detail--6517757.html (accessed on 5 July 2019).
- Yang, L. Study on Influencing Factors of Doctors’ Contribution Behavior in Online Medical Community. Master’s Thesis, Harbin Institute of Technology, Harbin, China, 2015. [Google Scholar]
- Xuan, L.; Linwei, W.; Jia, L.; Pengzhu, Z. Research on the Impact Mechanism of User Post Behavior in Online Healthy Communities. Manag. Sci. 2017, 301, 62–72. [Google Scholar]
- Dr. Lilac Product Analysis: Refining Existing Functions Based on User Needs [EB/OL]. Available online: http://www.woshipm.com/evaluating/1164830.html (accessed on 15 August 2018).
- Hao, Y. Research on the Theme and Text Sentiment Analysis of Cerebrovascular Disease Medical Forum. Master’s Thesis, Beijing Jiaotong University, Beijing, China, 2016. [Google Scholar]
- Yi, Y.; Haiyan, W. Research on the Dissemination and Control of Low Credibility Information in Question and Answer Community. Libr. Forum 2011, 06, 177–183. [Google Scholar]
- Abrahamson, J.; Rubin, V. Discourse structure differences in lay and professional health communication. J. Doc. 2012, 68, 826–851. [Google Scholar] [CrossRef]
- Gang, K.W.; Ravichandran, T. Exploring the Determinants of Knowledge Exchange in Virtual Communities. IEEE Trans. Eng. Manag. 2015, 621, 89–99. [Google Scholar] [CrossRef]
- Chae, J.; Quick, B.L. An Examination of the Relationship between Health Information Use and Health Orientation in Korean Mothers: Focusing on the Type of Health Information. J. Health Commun. 2015, 203, 275–284. [Google Scholar] [CrossRef]
- Donelle, L.; Hoffman-Goetz, L. Functional health literacy and cancer care conversations in online forums for retired persons. Inform. Health Soc. Care 2009, 341, 59–72. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, R.G.; Das Dores, R.M.; Camilo-Junior, C.G.; Rosa, T.C. SentiHealth-Cancer: A sentiment analysis tool to help detecting mood of patients in online social networks. Int. J. Med. Inform. 2016, 85, 80–95. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, L.G.; Dillingham, L.L. Personal experience as social capital in online investor forums. Libr. Inf. Sci. Res. 2014, 361, 27–35. [Google Scholar] [CrossRef]
- Padmore, A.; Joseph, E.; David, A. Social Networks and Health: Understanding the Nuances of Healthcare Access between Urban and Rural Populations. Int. J. Environ. Res. Public Health 2018, 155, 973–990. [Google Scholar]
- Shi, J.; Salmon, C.T. Identifying Opinion Leaders to Promote Organ Donation on Social Media: Network Study. J. Med. Internet Res. 2018, 20, e7. [Google Scholar] [CrossRef]
- Shi, J.; WanG, X.; Peng, T.Q.; Chen, L. Understanding interactions in virtual HIV communities: A social network analysis approach. Aids Care 2017, 29, 239–243. [Google Scholar] [CrossRef]
- Jun, D.; Xiaojun, M.; Qiang, B. A Comparative Study of Social Network Analysis Tools Ucinet and Gephi. Inf. Theory Pract. 2014, 378, 133–138. [Google Scholar]
- Borg, S. Social Networks and Health: Models, Methods, and Applications. JAMA J. Am. Med. Assoc. 2012, 30711, 488. [Google Scholar] [CrossRef]
- Xiaoming, Z.; Qian, Z.; Song, T. Research on Enterprise Competitiveness in Hybrid Electric Vehicles—Based on Patent Analysis Perspective. Soft Sci. 2014, 28, 1–5. [Google Scholar]
- Poleacovschi, C.; Javernick-Will, A.; Tong, T. The link between knowledge sharing connections and employee time savings: A social network analysis. Constr. Manag. Econ. 2017, 35, 445–467. [Google Scholar] [CrossRef]
- Karen, F.; Thomas, V.; Mary-Louise, M.L. Hygiene and Health: Who Do Mothers in Vanuatu Communicate with about Health? Int. J. Environ. Res. Public Health 2018, 153, 443–457. [Google Scholar]
- Jun, L. Overall Network Analysis Lecture: UCINET Software Practical Guide; Shanghai People’s Publishing House: Shanghai, China, 2009. [Google Scholar]
- Yuan, C.; Xinyu, L. Research on Opinion Leader Recognition Based on Social Network Analysis. Inf. Sci. 2015, 33, 13–19. [Google Scholar]
- Wei, H.L.; Ju, P.H. Dimensions of social capital and supply chain knowledge creation: The mediating role of learning information exchange. In Proceedings of the International Conference on Computers & Indutrial Engineering, Awaji, Japan, 25–28 July 2010; IEEE: Piscataway, NJ, USA, 2010. [Google Scholar]
- Granovetter, M. Economic Action and Social Structure: The Problem of Embeddedness. Am. J. Sociol. 1985, 913, 481–510. [Google Scholar] [CrossRef]
- Jiang, L. Medical aid investment, social capital, and individual health self-evaluation: Analysis based on a multi-level model. China Soc. Work Res. 2017, 1, 19–33 + 208–209. [Google Scholar]
- Jun, C. Research on Organizational Knowledge Sharing Based on Practice Community Platform—From the Perspective of Social Network. Master’s Thesis, Chongqing University, Chongqing, China, 2010. [Google Scholar]
- Sánchez-Franco, M.J.; Roldán, J.L. The influence of familiarity, trust and norms of reciprocity on an experienced sense of community: An empirical analysis based on social online services. Behav. Inf. Technol. 2015, 344, 392–412. [Google Scholar] [CrossRef]
- Paweł, C.; Teresa, K.; Klaudia, J.; Nalepa, D. Differences in the Perception of Social Support among Rural Area Seniors—A Cross-Sectional Survey of Polish Population. Int. J. Environ. Res. Public Health 2018, 156, 1288–1300. [Google Scholar]
- Liébana-Presa, C.; Andina-Díaz, E.; María-Mercedes, R.-G.; Fulgueiras-Carril, I.; Bermejo-Martínez, D.; Fernández-Martínez, E. Social Network Analysis and Resilience in University Students: An Approach from Cohesiveness. Int. J. Environ. Res. Public Health 2018, 15, 2119. [Google Scholar] [CrossRef] [Green Version]
- Eijk, M.V.D.; Faber, M.J.; Aarts, J.W.; Kremer, J.A.; Munneke, M.; Bloem, B.R. Using Online Health Communities to Deliver Patient-Centered Care to People With Chronic Conditions. J. Med. Internet Res. 2013, 156, 190–200. [Google Scholar]
- Xin, Z.; Yang, Z.; Ling, X. Interdependent self-construal matters in the community context: Relationships of self-construal with community identity and participation. J. Community Psychol. 2017, 45, 1050–1064. [Google Scholar] [CrossRef]
- Chin-Siang, A. Internet habit strength and online communication: Exploring gender differences. Comput. Hum. Behav. 2017, 66, 1–6. [Google Scholar]
- Liu, X.; Sun, M.; Li, J. Research on gender differences in online health communities. Int. J. Med. Inform. 2018, 111, 172–181. [Google Scholar] [CrossRef] [PubMed]
- Nath, C.; Huh, J.; Adupa, A.K.; Jonnalagadda, S.R. Website Sharing in Online Health Communities: A Descriptive Analysis. J. Med. Internet Res. 2016, 18, e11. [Google Scholar] [CrossRef] [PubMed]
- Adamson, M.; Choi, K.; Notaro, S.; Cotoc, C. The Doctor-Patient Relationship and Information-Seeking Behavior: Four Orientations to Cancer Communication. J. Palliat. Care 2018, 332, 79. [Google Scholar] [CrossRef] [PubMed]
- Lamont, R.; Fishman, T.; Goodyear-Smith, F. Travelling companions: A story told by a patient and her doctor. Br. J. Gen. Pract. 2018, 68671, 282. [Google Scholar] [CrossRef] [PubMed]
- Franklin, L.; Plaisant, C.; Rahman, K.M.; Shneiderman, B. Treatment Explorer: An Interactive Decision Aid for Medical Risk Communication and Treatment Exploration. Interact. Comput. 2018, 283, 238–252. [Google Scholar]
- Laughey, W.; Grandal, N.S.; Finn, G.M. Medical communication: The views of simulated patients. Med. Educ. 2018. [Google Scholar] [CrossRef]
- Caruana, C.J.; Cunha, J.A.M.; Orton, C.G. Subjects such as strategic planning, extra-disciplinary communication, and management have become crucial to medical physics clinical practice and should become an integral part of the medical physics curriculum. Med. Phys. 2017, 3885–3887. [Google Scholar] [CrossRef] [Green Version]
- Selinger, C.P.; Carbery, I.; Warren, V.; Rehman, A.F.; Williams, C.J.; Mumtaz, S.; Bholah, H.; Sood, R.; Gracie, D.J.; Hamlin, P.J.; et al. The relationship between different information sources and disease-related patient knowledge and anxiety in patients with inflammatory bowel disease. Aliment. Pharmacol. Ther. 2017, 451, 63–74. [Google Scholar] [CrossRef]
- Mboera, L.E.G.; Rumisha, S.F.; Senkoro, K.P.; Mayala, B.K.; Shayo, E.H.; Kisinza, W.N. Knowledge and health information communication in Tanzania. East Afr. J. Public Health 2007, 41, 33–39. [Google Scholar]
- Wu, Y.; Xue, Y.; Xue, Z. The study on the core personality trait words of Chinese medical university students based on social network analysis. Medicine 2017, 9637, 8078–8082. [Google Scholar] [CrossRef]
- Rushmore, J.; Caillaud, D.; Matamba, L.; Stumpf, R.M.; Borgatti, S.P.; Altizer, S. Social network analysis of wild chimpanzees provides insights for predicting infectious disease risk. J. Anim. Ecol. 2013, 82–92. [Google Scholar] [CrossRef]
- Kojaku, S.; Masuda, N. Core-periphery structure requires something else in the network. New J. Phys. 2018, 4, 20. [Google Scholar] [CrossRef]
- Liu, X.; Guo, X.; Wu, H.; Vogel, D. Doctor’s effort influence on online reputation and popularity. In ICSH 2014: Smart Health; Lecture Notes in Computer Science; Springer: Cham, Switzerland, 2014; Volume 8549, pp. 112–126. [Google Scholar]
- Burt, R.S.; Kilduff, M.; Tasselli, S. Social Network Analysis: Foundations and Frontiers on Advantage. Annu. Rev. Psychol. 2013, 641, 527–547. [Google Scholar] [CrossRef]
- Harris, J.K.; Clements, B. Using Social Network Analysis to Understand Missouri’s System of Public Health Emergency Planners. Public Health Rep. 2007, 1224, 488–498. [Google Scholar] [CrossRef] [Green Version]
- Lou, T.; Tang, J. Mining Structural Hole Spanners Through Information Diffusion in Social Networks. In Proceedings of the WWW ’13, 22nd International Conference on World Wide Web, Rio de Janeiro, Brazil, 13–17 May 2013; pp. 825–836. [Google Scholar]
- Haiping, T.; Cheng, L. Expansion of the field of privacy ethics in the era of big data and its basic problems—A case study of the big data health revolution. Ethical Stud. 2018, 3, 67–72. [Google Scholar]
- Xiangning, G.; Hongjiang, Z. Research on Privacy Ethics of Medical Big Data. J. Jinzhou Med. Univ. (Soc. Sci. Ed.) 2019, 1703, 21–24. [Google Scholar]
- Yawei, L.; Jianpeng, Z. Research on Privacy Ethics under the Background of Big Data. J. Mudanjiang Teach. Coll. (Philos. Soc. Sci. Ed.) 2018, 4, 23–27. [Google Scholar]
- Gürsoy, G.; Harmanci, A.; Tang, H.; Ayday, E.; Brenner, S.E. When Biology Gets Personal: Hidden Challenges of Privacy and Ethics in Biological Big Data. Pac. Symp. Biocomput. Pac. Symp. Biocomput. 2019, 24, 386–390. [Google Scholar]
- Ben, L. ‘We are a tight community’: Social groups and social identity in medical undergraduates. Med. Educ. 2015, 4910, 1016–1027. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Job Title | Assigned Number |
|---|---|
| Primary title | 2, 4, 5, 10, 15, 16, 17, 30, 33, 37, 38, 41, 43, 45, 50, 51, 52, 54, 55, 57, 63, 64, 65, 67, 81, 82, 83, 85, 87, 90, 91, 92, 93, 94 |
| Intermediate title | 3, 7, 9, 11, 12, 21, 22, 26, 27, 28, 29, 31, 36, 39, 44, 46, 48, 56, 68, 69, 71, 72, 74, 75, 78, 79, 80, 88, 89, 95, 97, 98, 101 |
| Deputy senior title | 6, 8, 13, 14, 19, 20, 23, 24, 25, 32, 35, 47, 49, 53, 58, 60, 61, 66, 70, 73, 76, 77, 84, 86, 96, 99, 100 |
| Senior professional title | 1, 18, 34, 40, 42, 59, 62, 102 |
| Metric | Conceptual Definition |
|---|---|
| Density | Proportion of possible relationships in the network. Density values vary between 0 and 1, with 1 being when all possible relationships are present [24]. |
| Centralization | The overall integration or consistency of the graph [25]. |
| Geodesic distance | Measures the extent of connection in the network and is the shortest pathway between two people [26]. The shortest distance between two nodes is measured to obtain a geodesic distance matrix. |
| Centrality | Includes the three measures Freeman’s degree, closeness, and Freeman’s betweenness. Centrality measures the most connected people by measuring those who interact with the most people [27]. |
| Core–periphery model | Examines the location characteristics of doctors in information dissemination networks [28]. |
| Structural holes | When a social entity is in a position where two other social entities are directly connected, it is in the structural hole position and plays a key connection role. At the same time, in the process of information transmission, the social entity in the structural hole position can access two kinds-of information and can control the group by transmitting and describing this different information. Structural holes include three metrics: effective size, efficiency, and constraint [29]. |
| Number of Views | Number of Votes | Number of Favorites | |
|---|---|---|---|
| Average | 80,362 | 9677 | 7226 |
| Median | 55,073 | 2864 | 2154 |
| Moderate | No | No | No |
| Standard | 86,956 | 21,331 | 14,212 |
| Kurtosis | 8 | 53 | 23 |
| Skewness | 2 | 6 | 4 |
| Maximum | 541,639 | 192,431 | 104,230 |
| Minimum | 1359 | 9 | 6 |
| Number of Views | Number of Votes | Number of Favorites | |
|---|---|---|---|
| Maximum | individual 40 | individual 1 | individual 62 |
| Minimum | individual 13 | individual 9/ individual 99 | individual 88 |
| Degree Centralization | Betweenness Centralization | Closeness Centralization | ||
|---|---|---|---|---|
| In-Degree | Out-Degree | In-Degree | Out-Degree | |
| 21.95% | 32.95% | 3.96% | 17.17% | 27.19% |
| Node | Freeman’s Degree | Freeman’s Betweenness | Closeness | ||
|---|---|---|---|---|---|
| In-Degree | Out-Degree | In-Degree | Out-Degree | ||
| 1 | 45 | 56 | 476.961 | 64.331 | 69.178 |
| 2 | 15 | 39 | 58.631 | 52.880 | 61.585 |
| 3 | 7 | 45 | 132.778 | 46.119 | 64.331 |
| 8 | 24 | 30 | 97.495 | 56.742 | 58.382 |
| 10 | 20 | 35 | 107.285 | 54.891 | 60.479 |
| 12 | 18 | 31 | 88.459 | 54.595 | 58.721 |
| 31 | 29 | 30 | 163.102 | 58.382 | 58.382 |
| 34 | 20 | 28 | 100.281 | 55.495 | 58.046 |
| 35 | 32 | 31 | 150.781 | 59.412 | 58.721 |
| 36 | 31 | 23 | 94.101 | 59.064 | 56.111 |
| 39 | 26 | 38 | 158.380 | 56.742 | 61.585 |
| 40 | 24 | 44 | 167.231 | 56.425 | 63.522 |
| 42 | 25 | 51 | 196.013 | 56.111 | 66.887 |
| 44 | 38 | 37 | 168.422 | 61.585 | 60.843 |
| 47 | 28 | 37 | 114.957 | 58.046 | 60.843 |
| 53 | 34 | 31 | 118.798 | 60.119 | 58.721 |
| 56 | 36 | 17 | 59.764 | 60.843 | 54.011 |
| 58 | 24 | 22 | 48.690 | 56.425 | 55.495 |
| 59 | 28 | 19 | 56.095 | 58.046 | 54.595 |
| 60 | 29 | 31 | 112.351 | 58.046 | 58.721 |
| 61 | 28 | 17 | 55.600 | 58.046 | 53.723 |
| 62 | 25 | 23 | 69.873 | 57.062 | 56.111 |
| 66 | 27 | 21 | 52.385 | 57.062 | 54.891 |
| 68 | 34 | 30 | 101.925 | 60.119 | 58.382 |
| 69 | 32 | 25 | 101.009 | 59.412 | 56.742 |
| 73 | 25 | 32 | 136.355 | 57.062 | 58.046 |
| 84 | 20 | 35 | 95.423 | 55.495 | 60.119 |
| 86 | 17 | 40 | 118.494 | 54.595 | 61.963 |
| 87 | 25 | 20 | 52.264 | 57.062 | 53.439 |
| 92 | 29 | 37 | 188.107 | 58.382 | 60.843 |
| 96 | 30 | 34 | 146.920 | 58.382 | 59.763 |
| 100 | 28 | 31 | 136.590 | 58.046 | 58.721 |
| 102 | 41 | 24 | 158.262 | 62.733 | 56.425 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Z.; Xu, X. Analysis of Network Structure and Doctor Behaviors in E-Health Communities from a Social-Capital Perspective. Int. J. Environ. Res. Public Health 2020, 17, 1136. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041136
Li Z, Xu X. Analysis of Network Structure and Doctor Behaviors in E-Health Communities from a Social-Capital Perspective. International Journal of Environmental Research and Public Health. 2020; 17(4):1136. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041136
Chicago/Turabian StyleLi, Zhigang, and Xu Xu. 2020. "Analysis of Network Structure and Doctor Behaviors in E-Health Communities from a Social-Capital Perspective" International Journal of Environmental Research and Public Health 17, no. 4: 1136. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17041136