Adaptation of TECCU App Based on Patients´ Perceptions for the Telemonitoring of Inflammatory Bowel Disease: A Qualitative Study Using Focus Groups

 , ,
, ,
Abstract
:1. Introduction
Structure of the Paper
2. Materials and Methods
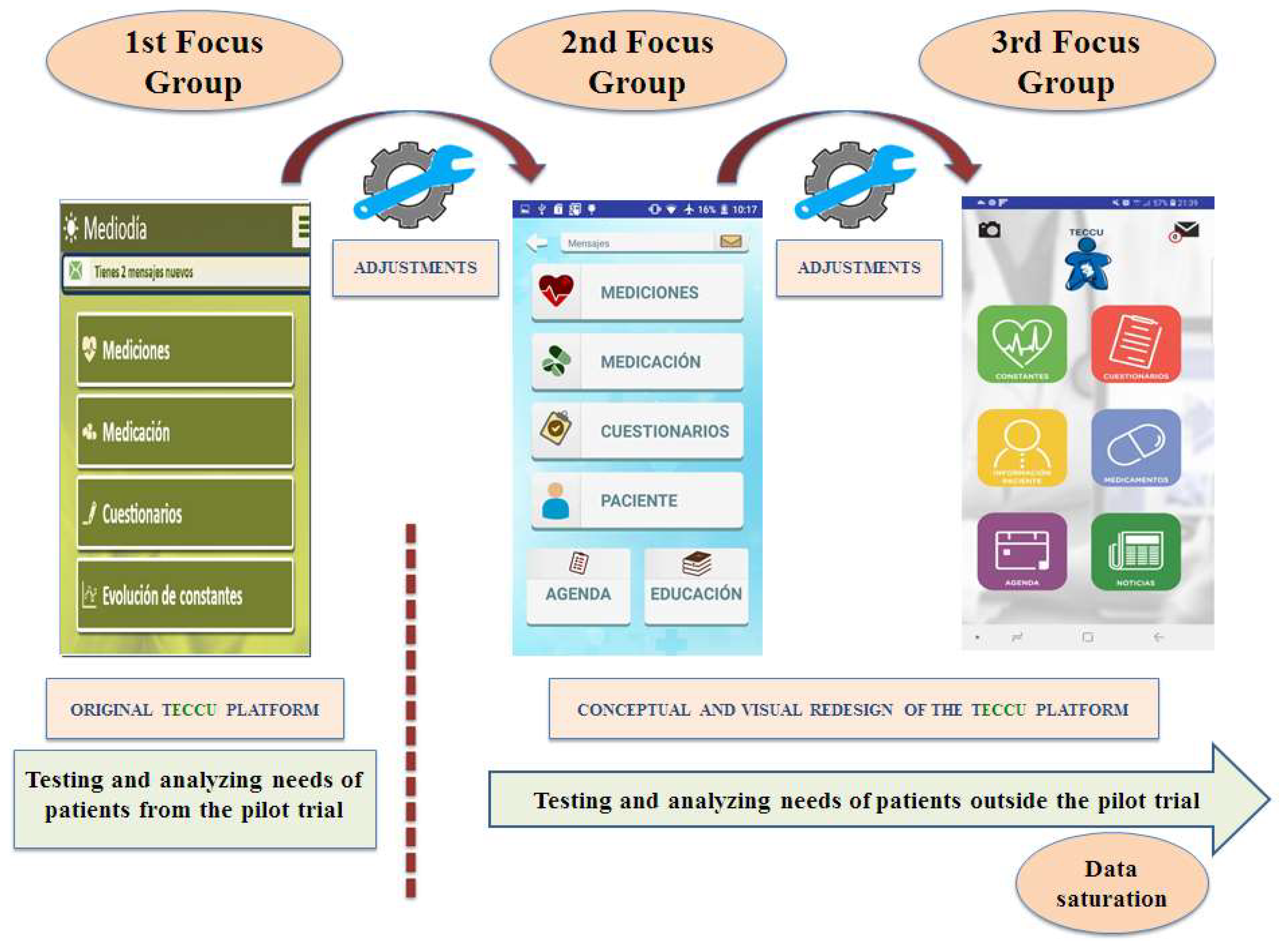
2.1. Study Design
2.2. Working Process and Patient Selection
2.3. First Focus Group with Patients from the Pilot TECCU Trial
2.4. Second and Third Focus Groups with IBD Patients Outside the Pilot Trial
2.5. Data Collection
2.6. Data Coding and Analysis
2.7. Ethical Considerations
3. Results
3.1. Demographics
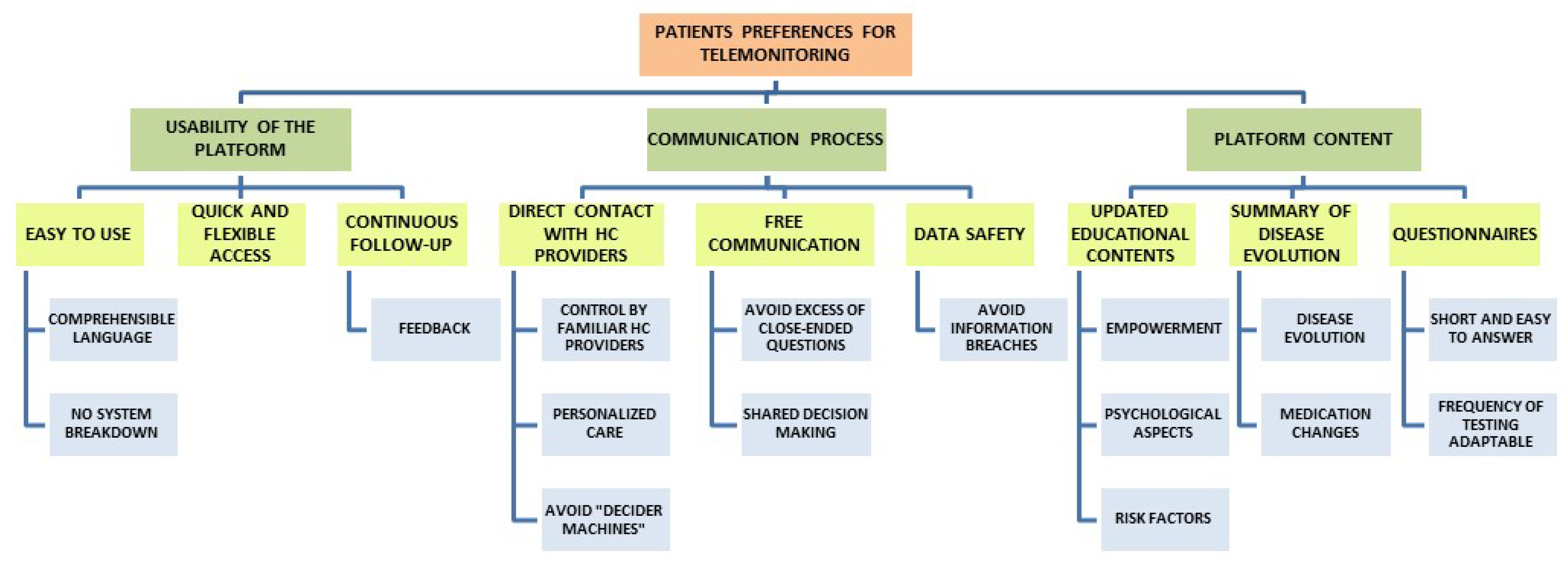
3.2. Emerging Themes
3.3. Usability of the Telemonitoring Platform
3.3.1. Patients’ Perceptions and Needs Regarding Usability
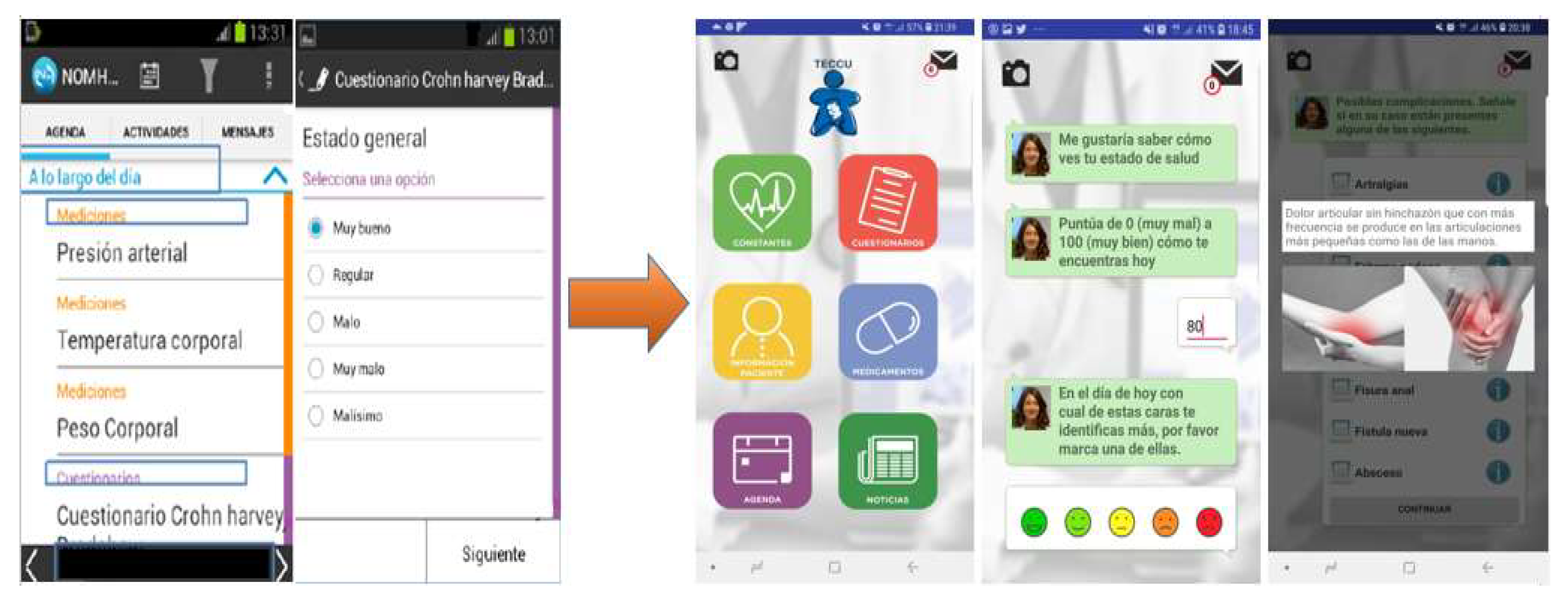
3.3.2. Improvements in the Usability of the TECCU App
3.4. Characteristics of the Communication Process through the Web Platform
3.4.1. Patient Perceptions and their Communication Needs
3.4.2. Improvements in the Communication Process through the TECCU App
3.5. Content that the Platform Should Include
3.5.1. Patient Perceptions and Their Needs in Terms of Platform Content
3.5.2. Updates in the Platform Content
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
References
- Torrent-Sellens, J.; Díaz-Chao, Á.; Soler-Ramos, I.; Saigí-Rubió, F. Modelling and predicting ehealth usage in Europe: A multidimensional approach from an online survey of 13,000 European Union internet users. J. Med. Internet Res. 2016, 18, e188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elbert, N.J.; van Os-Medendorp, H.; van Renselaar, W.; Ekeland, A.G.; Hakkaart-van Roijen, L.; Raat, H.; Pasmans, S.G. Effectiveness and cost-effectiveness of ehealth interventions in somatic diseases: A systematic review of systematic reviews and meta-analyses. J. Med. Internet Res. 2014, 16, e110. [Google Scholar] [CrossRef]
- Aguas Peris, M.; Del Hoyo, J.; Bebia, P.; Faubel, R.; Barrios, A.; Bastida, G.; Valdivieso, B.; Nos, P. Telemedicine in inflammatory bowel disease: Opportunities and approaches. Inflamm. Bowel Dis. 2015, 21, 392–399. [Google Scholar] [CrossRef]
- Høivik, M.L.; Moum, B.; Solberg, I.C.; Henriksen, M.; Cvancarova, M.; Bernklev, T. Work disability in inflammatory bowel disease patients 10 years after disease onset: Results from the IBSEN Study. Gut 2013, 62, 368–375. [Google Scholar] [CrossRef] [PubMed]
- Hoivik, M.L.; Moum, B.; Solberg, I.C.; Cvancarova, M.; Hoie, O.; Vatn, M.H. Health-related quality of life in patients with ulcerative colitis after a 10-year disease course: Results from the IBSEN study. Inflamm. Bowel Dis. 2012, 18, 1540–1549. [Google Scholar] [CrossRef] [PubMed]
- Burisch, J.; Jess, T.; Martinato, M.; Lakatos, P.L. The burden of inflammatory bowel disease in Europe. J. Crohns Colitis. 2013, 7, 322–337. [Google Scholar] [CrossRef] [Green Version]
- Bähler, C.; Vavricka, S.R.; Schoepfer, A.M.; Brüngger, B.; Reich, O. Trends in prevalence, mortality, health care utilization and health care costs of Swiss IBD patients: A claims data based study of the years 2010, 2012 and 2014. BMC Gastroenterol. 2017, 17, 138. [Google Scholar] [CrossRef]
- Peery, A.F.; Crockett, S.D.; Murphy, C.C.; Lund, J.L.; Dellon, E.S.; Williams, J.L.; Kochar, B.; Barnes, E.L.; Fan, Y.C.; Pate, V.; et al. Burden and Cost of Gastrointestinal, Liver and Pancreatic Diseases in the United States: Update 2018. Gastroenterology 2019, 156, 254–272. [Google Scholar] [CrossRef] [Green Version]
- Elkjaer, M.; Shuhaibar, M.; Burisch, J.; Bailey, Y.; Scherfig, H.; Laugesen, B.; Munkholm, P. E-health empowers patients with ulcerative colitis: A randomised controlled trial of the web-guided ‘Constant-care’ approach. Gut 2010, 59, 1652–1661. [Google Scholar] [CrossRef]
- De Jong, M.J.; van der Meulen-de, A.E.; Romberg-Camps, M.J.; Becx, M.C.; Maljaars, J.P.; Cilissen, M.; van Bodegraven, A.A.; Mahmmod, N.; Markus , T.; Hameeteman, W.M.; et al. Telemedicine for management of inflammatory bowel disease (myIBDcoach): A pragmatic, multicentre, randomised controlled trial. Lancet 2017, 390, 959–968. [Google Scholar] [CrossRef]
- Johnson, M.; Lithgo, K.; Price, T. OC-080 IBD-Sshamp (Supported, Self help and Management Programme); UK’s first Internet based Remote Management System for Managing Stable IBD. Gut 2013, 62, A34–A35. [Google Scholar] [CrossRef] [Green Version]
- Sundin, P.; Callan, J.; Mehta, K. Why do entrepreneurial mHealth ventures in the developing world fail to scale? J. Med. Eng Technol. 2016, 40, 444–457. [Google Scholar] [CrossRef] [PubMed]
- Scott Kruse, C.; Karem, P.; Shifflett, K.; Vegi, L.; Ravi, K.; Brooks, M. Evaluating barriers to adopting telemedicine worldwide: A systematic review. J. Telemed. Telecare 2018, 24, 4–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Del Hoyo, J.; Nos, P.; Bastida, G.; Faubel, R.; Muñoz, D.; Garrido-Marín, A.; Valero-Pérez, E.; Bejar-Serrano, S.; Aguas, M. Telemonitoring of Crohn’s Disease and Ulcerative Colitis (TECCU): Cost-effectiveness analysis. J. Med. Internet Res. 2019, 21, e15505. [Google Scholar] [CrossRef] [Green Version]
- Carlsen, K.; Houen, G.; Jakobsen, C.; Kallemose, T.; Paerregaard, A.; Riis, L.B.; Munkholm , P.; Wewer, V. Individualized infliximab treatment guided by patient-managed ehealth in children and adolescents with Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2017, 23, 1473–1482. [Google Scholar] [CrossRef]
- Heida, A.; Dijkstra, A.; Muller Kobold, A.; Rossen, J.W.; Kindermann, A.; Kokke, F.; de Meij, T.; Norbruis, O.; Weersma, R.K.; Wessels, M.; et al. Efficacy of home telemonitoring versus conventional follow-up: A randomized controlled trial among teenagers with inflammatory bowel disease. J. Crohns Colitis 2018, 12, 432–441. [Google Scholar] [CrossRef]
- Cross, R.K.; Cheevers, N.; Rustgi, A.; Langenberg, P.; Finkelstein, J. Randomized, controlled trial of home telemanagement in patients with ulcerative colitis (UC HAT). Inflamm. Bowel Dis. 2012, 18, 1018–1025. [Google Scholar] [CrossRef]
- Cross, R.K.; Langenberg, P.; Regueiro, M.; Schwartz, D.A.; Tracy, J.K.; Collins, J.F.; Katz, J.; Ghazi, J.; Patil, S.A.; Quezada, S.M.; et al. A randomized controlled trial of TELEmedicine for patients with Inflammatory Bowel Disease (TELE-IBD). Am. J. Gastroenterol. 2019, 114, 472–482. [Google Scholar] [CrossRef]
- Del Hoyo, J.; Nos, P.; Faubel, R.; Muñoz, D.; Domínguez, D.; Bastida, G.; Valdivieso, B.; Correcher, M.; Aguas, M. A Web-based telemanagement system for improving disease activity and quality of life in patients with complex inflammatory bowel disease: Pilot randomized controlled trial. J. Med. Internet Res. 2018, 20, e11602. [Google Scholar] [CrossRef]
- Yin, A.L.; Hachuel, D.; Pollak, J.P.; Scherl, E.J.; Estrin, D. Digital health apps in the clinical care of Inflammatory Bowel Disease: Scoping review. J. Med. Internet Res. 2019, 21, e14630. [Google Scholar] [CrossRef]
- Con, D.; De Cruz, P. Mobile phone apps for inflammatory bowel disease self-management: A systematic assessment of content and tools. JMIR Mhealth Uhealth 2016, 4, e13. [Google Scholar] [CrossRef] [PubMed]
- Paré, G.; Trudel, M.C.; Forget, P. Adoption, use, and impact of e-booking in private medical practices: Mixed-methods evaluation of a two-year showcase project in Canada. JMIR Med. Inform. 2014, 2, e24–e34. [Google Scholar]
- Chang, M.Y.; Pang, C.; Tarn, J.M.; Liu, T.S.; Yen, D.C. Exploring user acceptance of an e-hospital service: An empirical study in Taiwan. Comput. Stand. Interfaces 2015, 38, 35–43. [Google Scholar] [CrossRef]
- De Rosis, S.; Barsanti, S. Patient satisfaction, e-health and the evolution of the patient–general practitioner relationship: Evidence from an Italian survey. Health Policy 2016, 120, 1279–1292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Treskes, R.W.; Van der Velde, E.T.; Schoones, J.W.; Schalij, M.J. Implementation of smart technology to improve medication adherence in patients with cardiovascular disease: Is it effective? Expert Rev. Med. Devices 2018, 15, 119–126. [Google Scholar] [CrossRef] [PubMed]
- Kitsios, F.; Stefanakakis, S.; Kamariotou, M.; Dermentzoglou, L. E-service Evaluation: User satisfaction measurement and implications in health sector. Comput. Stand. Interfaces 2019, 63, 16–26. [Google Scholar] [CrossRef]
- Nugraha, D.C.A.; Aknuranda, I. An Overview of e-Health in Indonesia: Past and Present Applications. Int. J. Electr. Comput. Eng. 2017, 7, 2441–2450. [Google Scholar] [CrossRef]
- Ricci, G.; Baldanzi, S.; Seidita, F.; Proietti, C.; Carlini, F.; Peviani, S.; Antonini , G.; Vianello, A.; Siciliano, G.; Italian GSD II group. A mobile app for patients with Pompe disease and its possible clinical applications. Neuromuscul. Disord. 2018, 28, 471–475. [Google Scholar] [CrossRef]
- Con, D.; Jackson, B.; Gray, K.; De Cruz, P. EHealth for inflammatory bowel disease self-management—The patient perspective. Scand. J. Gastroenterol. 2017, 52, 973–980. [Google Scholar] [CrossRef]
- Quinn, C.C.; Chard, S.; Roth, E.G.; Eckert, J.K.; Russman, K.M.; Cross, R.K. The Telemedicine for Patients with Inflammatory Bowel Disease (TELE-IBD) clinical trial: Qualitative assessment of participants’ perceptions. J. Med. Internet Res. 2019, 21, e14165. [Google Scholar] [CrossRef]
- Jackson, B.D.; Con, D.; De Cruz, P. Design considerations for an eHealth decision support tool in inflammatory bowel disease self-management. Intern. Med. J. 2018, 48, 674–681. [Google Scholar] [CrossRef] [PubMed]
- Aguas, M.; del Hoyo, J.; Faubel, R.; Muñoz, D.; Domínguez, D.; Bastida, G.; Navarro, B.; Barrios, A.; Valdivieso, B.; Correcher, M.; et al. A web-based telemanagement system for patients with complex inflammatory bowel disease: Protocol for a randomized controlled clinical trial. JMIR Res. Protoc. 2018, 7, e190. [Google Scholar] [CrossRef] [PubMed]
- Krueger, R.A.; Casey, M.A. Focus Groups: A Practical Guide for Applied Research, 5th ed.; SAGE Publications: Thousand Oaks, CA, USA, 2015. [Google Scholar]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (coreq): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitzinger, J. Qualitative Research: Introducing focus groups. BMJ 1995, 311, 299–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stewart, D.W.; Shamdasani, P.N. Focus Groups. Theory and Practice, 3rd ed.; SAGE Publications: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Donabedian, A. Evaluating the Quality of Medical Care. Milbank Q. 2005, 83, 691–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Saldaña, J. The Coding Manual for Qualitative Researchers; SAGE Publications: London, UK, 2009. [Google Scholar]
- Harvey, R.F.; Bradshaw, J.M. A simple index of Crohn’s-disease activity. Lancet 1980, 1, 514. [Google Scholar] [CrossRef]
- Walmsley, R.S.; Ayres RC, S.; Pounder, R.E.; Allan, R.N. A simple clinical colitis activity index. Gut 1998, 43, 29–32. [Google Scholar] [CrossRef] [Green Version]
- Morisky, D.E.; Green, L.W.; Levine, D.M. Concurrent and predictive validity of a self-reported measure of medication adherence. Med. Care 1986, 24, 67–74. [Google Scholar] [CrossRef]
- Marín-Jiménez, I.; Nos, P.; Domènech, E.; Riestra, S.; Gisbert, J.P.; Calvet, X.; Cortés, X.; Iglesias, E.; Huguet, J.M.; Taxonera, C.; et al. Diagnostic performance of the simple clinical colitis activity index self-administered online at home by patients with ulcerative colitis: CRONICA-UC Study. Am. J. Gastroenterol. 2016, 111, 261–268. [Google Scholar] [CrossRef]
- Barnes, E.L.; Kappelman, M.D.; Long, M.D.; Evon, D.M.; Martin, C.F.; Sandler, R.S. A novel Patient-Reported Outcome-Based Evaluation (PROBE) of quality of life in patients with inflammatory bowel disease. Am. J. Gastroenterol. 2019, 114, 640–647. [Google Scholar] [CrossRef]
- Cross, R.K.; Cheevers, N.; Finkelstein, J. Home telemanagement for patients with ulcerative colitis (UCHAT). Dig. Dis. Sci. 2009, 54, 2463–2472. [Google Scholar] [CrossRef]
- De Jong, M.J.; Roosen, D.; Degens, J.H.; van den Heuvel, T.R.; Romberg-Camps, M.; Hameeteman, W.; Bodelier, A.G.L.; Romanko, I.; Lukas, M.; Winkens, B.; et al. Development and validation of a patient-reported score to screen for mucosal inflammation in inflammatory bowel disease. J. Crohns Colitis 2019, 13, 555–563. [Google Scholar] [CrossRef]
- Zand, A.; Sharma, A.; Stokes, Z.; Reynolds, C.; Hommes, D. The initial development of a Chat-Bot for inflammatory bowel disease (IBD) patients for use in e-health applications. In Poster Presented at: European Crohn’s and Colitis Organisation Congress, Copenhagen, Journal of Crohn’s and Colitis; Oxford University Press: Oxford, UK, 2019. [Google Scholar]
- Available online: https://www.eu-startups.com/2019/05/amsterdam-based-nori-health-raises-e600k-for-its-digital-coach-for-people-living-with-ibd-after-completing-successful-trial/ (accessed on 12 December 2019).
- Kemp, K.; Griffiths, J.; Campbell, S.; Lovell, K. An exploration of the follow-up needs of patients with inflammatory bowel disease. J. Crohns Colitis 2013, 7, e386–e395. [Google Scholar] [CrossRef] [Green Version]
- Chung, A.E.; Vu, M.B.; Myers, K.; Burris, J.; Kappelman, M.D. Crohn’s and Colitis Foundation of America partners patient-powered research network: Patient perspectives on facilitators and barriers to building an impactful patient-powered research network. Med. Care 2018, 56, S33–S40. [Google Scholar] [CrossRef]
- Van der Marel, S.; Duijvestein, M.; Hardwick, J.C.; van den Brink, G.R.; Veenendaal, R.; Hommes, D.W.; Fidder, H.H. Quality of web-based information on inflammatory bowel diseases. Inflamm. Bowel Dis. 2009, 15, 1891–1896. [Google Scholar] [CrossRef] [Green Version]
- Promislow, S.; Walker, J.R.; Taheri, M.; Bernstein, C.N. How well does the internet answer patients’ questions about inflammatory bowel disease? Can. J. Gastroenterol. 2010, 24, 671–677. [Google Scholar] [CrossRef]
- Azer, S.A.; AlOlayan, T.I.; AlGhamdi, M.A.; AlSanea, M.A. Inflammatory bowel disease: An evaluation of health information on the Internet. World J. Gastroenterol. 2017, 23, 1676–1696. [Google Scholar] [CrossRef]
- Available online: https://www.accuesp.com/ (accessed on 5 December 2019).
- Heida, A.; Knol, M.; Kobold, A.M.; Bootsman, J.; Dijkstra, G.; van Rheenen, P.F. Agreement between home-based measurement of stool calprotectin and elisa results for monitoring inflammatory bowel disease activity. Clin. Gastroenterol. Hepatol. 2017, 15, 1742–1749. [Google Scholar] [CrossRef] [Green Version]
- Guest, G. Sampling and selecting participants in field research. In Handbook of Methods in Cultural Anthropology, 2nd ed.; Bernard, H.R., Gravlee, C.C., Eds.; Rowman & Littlefield: Lanham, MD, USA, 2015; pp. 215–250. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex | Age (Years) | Disease Profile | Disease Duration (Years) | Active/ Remission | Education | Internet Use | |
|---|---|---|---|---|---|---|---|
| Patients from the pilot TECCU study | |||||||
| P 01 | Female | 20 | UC (E3) | 3 | Remission | University | Daily |
| P 02 | Male | 60 | CD (L3) | 39 | Active | Secondary | Weekly |
| P 03 | Female | 38 | UC (E3) | 16 | Remission | University | Daily |
| P 04 | Female | 63 | CD (L1) | 24 | Remission | Secondary | Weekly |
| Patients outside the pilot TECCU study | |||||||
| P 05 | Female | 42 | UC (E3) | 28 | Remission | University | Daily |
| P 06 | Male | 43 | UC (E3) | 4 | Active | University | Daily |
| P 07 | Male | 34 | CD (L1) | 3 | Active | Secondary | Daily |
| P 08 | Female | 33 | UC (E2) | 29 | Remission | University | Daily |
| P 09 | Male | 23 | CD (L1) | 4 | Remission | University | Daily |
| P 10 | Male | 37 | UC (E2) | 18 | Active | University | Daily |
| P11 | Female | 62 | CD (L3) | 30 | Remission | Secondary | Weekly |
| P12 | Female | 41 | CD (L2) | 7 | Remission | University | Daily |
| P13 | Male | 22 | UC (E3) | 5 | Remission | University | Daily |
| P14 | Male | 36 | CD (L1) | 18 | Active | University | Daily |
| P15 | Male | 52 | CD (L1) | 25 | Remission | University | Daily |
| P16 | Female | 37 | UC (E2) | 23 | Remission | Secondary | Daily |
| P17 | Male | 42 | CD (L3) | 27 | Remission | University | Daily |
| P18 | Female | 29 | CD (L1) | 10 | Active | University | Daily |
| Theme | Category | Number of Patients who Agree n (%) | Study ID of Patients who Agree |
|---|---|---|---|
| Platform Usability | Easy to use | 18 (100) | 01 to 18 |
| Quick and flexible access | 18 (100) | 01 to 18 | |
| Continuous follow-up | 13 (72.2) | 01, 02, 04, 07, 08, 09, 10, 12, 14, 15, 16, 17, 18 | |
| Communication process | Direct contact with HC providers | 18 (100) | 01 to 18 |
| Fluid communication | 14 (77.8) | 01, 03, 04, 06, 07, 08, 09, 10, 11, 12, 13, 15, 16, 18 | |
| Data safety | 18 (100) | 01 to 18 | |
| Platform Content | Updated educational content | 14 (77.8) | 01, 02, 03, 05, 07, 08, 09, 10, 12, 13, 15, 16, 17, 18 |
| Summary of disease evolution | 12 (66.7) | 01, 03, 05, 06, 07, 09, 10, 12, 13, 16, 17, 18 | |
| Questionnaires | 11 (61.1) | 01, 02, 03, 06, 08, 10, 11, 13, 15, 16, 17 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Del Hoyo, J.; Nos, P.; Faubel, R.; Bastida, G.; Muñoz, D.; Valero-Pérez, E.; Garrido-Marín, A.; Bella, P.; Peña, B.; Savini, C.; et al. Adaptation of TECCU App Based on Patients´ Perceptions for the Telemonitoring of Inflammatory Bowel Disease: A Qualitative Study Using Focus Groups. Int. J. Environ. Res. Public Health 2020, 17, 1871. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17061871
Del Hoyo J, Nos P, Faubel R, Bastida G, Muñoz D, Valero-Pérez E, Garrido-Marín A, Bella P, Peña B, Savini C, et al. Adaptation of TECCU App Based on Patients´ Perceptions for the Telemonitoring of Inflammatory Bowel Disease: A Qualitative Study Using Focus Groups. International Journal of Environmental Research and Public Health. 2020; 17(6):1871. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17061871
Chicago/Turabian StyleDel Hoyo, Javier, Pilar Nos, Raquel Faubel, Guillermo Bastida, Diana Muñoz, Elena Valero-Pérez, Alejandro Garrido-Marín, Pablo Bella, Beatriz Peña, Claudia Savini, and et al. 2020. "Adaptation of TECCU App Based on Patients´ Perceptions for the Telemonitoring of Inflammatory Bowel Disease: A Qualitative Study Using Focus Groups" International Journal of Environmental Research and Public Health 17, no. 6: 1871. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17061871