1.1. The Needs of an Ageing Society and Remote Residents
There is a controversy over the concern of rural health disparities in the practice of a democratic society. Some believe that health disparities should not exist in a democratic society due to equality consideration, while others think the power of influence will determine the focus of health facilities dispense. Undoubtedly, more rural areas do present adverse health conditions than suburban areas [
1]. To tackle rural health disparities and ageing society challenges, connected health (CH) is proposed as a promising solution worldwide. Where CH is practiced, it usually fulfills the pre-conditions of advanced information technology (IT), integrated healthcare, significant geographic isolation and population of ageing or with chronic conditions.
Taiwanese CH, as a case study, is significant and valuable as it demonstrates typical features which may impact and interest the whole of society. Taiwan has become one of the fastest ageing populations in the world due to advancements in medical technology, changes in family structure, and the low birth rate [
2]. Over the past century, there has been a dramatic increase in life expectancy accompanied by a growth in chronic conditions (such as hypertension, diabetes, coronary diseases, and obesity) [
3]. Geographically, Taiwan’s remote areas cover mountain areas, isolated islands, and remote townships [
4]. In these areas, medical and care services are allowed to be practiced remotely according to the law and regulation of the state. There are 48 remote townships that account for 44% of the area in Taiwan, while their residents are only 0.36 million people which accounts for 1.6% of the total population [
5,
6,
7]. These features make Taiwan a typical case to study CH’s challenges and strategies in remote areas accompanied by ageing populations.
Much health-related research is conducted through quantitative method due to its evidence-based nature. Quantitative research is designed for the natural sciences and covers surveys, laboratory experiments, econometrics, statistical analysis and others. On the other hand, qualitative research methods are developed in social sciences for the study of social and cultural phenomena [
8]. It features on seeing the world from the participants’ lenses to discover insights that will contribute to the development of empirical knowledge. Although this study was conducted in a qualitative manner, which differs from a qualitative research that can offer a statistics variation, it may contribute knowledge by offering insights and implications that may inspire areas that encounter similar challenges [
8,
9]. Based on findings of this study, a further discovery of the root causes of the issues in CH can be identified. Their connection with business model innovation can be developed as an innovation driver to sustain CH’s practice.
Studies of Taiwanese universal health insurance (UHI) are of interest for researchers due to the comprehensive coverage of care for residents and the reduction of health disparity in the society [
10]. Particularly, the Taiwanese society has distinct universal health insurance that covers all citizens both in remote and urban areas. However, significant benefits for the insured elderly among remote residents need to be explored and addressed. In the past, challenges in accessing health care associated with transportation, social isolation, poverty, and a lack of health care providers, especially medical specialists confronted the rural residents to facilitate the benefits of UHI, CH is expecting to make contributions to equitable right to access healthcare. What is disputed in the democratic society is the right of equality and the contributions of its participants [
11,
12]. It is seen that citizens pay for the same insurance fees, while not everyone enjoys the same health benefits. Although the implementation of health facilities in remote areas may be costly, it is relevant to concern oneself with the needs of remote residents in a democratic society [
13]. Therefore, the authors aimed to identify key challenges and possible strategies in CH to ensure the quality of care and equality. It is expected that the finding of this research can benefit an ageing society and remote residents. The objective of this study was to discover CH’s influencing factors so as to develop strategies of removing barriers and improving access to health services for remote residents.
1.2. The Selection of Research Target
Several essential features are identified to conduct a meaningful connected health study based on literature review [
14,
15,
16]. These are demographics of population ageing; comprehensive CH ecosystem, Information Communication Technology (ICT) infrastructure; and the region or area with significant geographic features. Taiwan has been selected as a critical case study as it meets the preconditions and essential requirements for the successfully implementation of CH. Taiwan has its importance uniqueness, and revelatory in researching CH due to the following characteristics: Taiwan has become one of the fastest ageing population areas in the world due to the advancement of medical technology, changing family concepts, and a low birth rate as well as its significant geographic features [
17,
18,
19,
20,
21].
Although in Taiwan, different terms, such as remote health, Telecare or Telehealth, in general, are more frequently used rather than the term “connected health” (CH) for describing similar models by healthcare professionals, it is still in the same domain for discussion and comparison (
Figure 1) [
22,
23,
24,
25,
26,
27]. Currently, researchers tend to use Connected Health as a term that applies to the linked systems and people in the application of ICT in healthcare in general [
14,
28,
29].
The literature indicates that CH includes the whole Telemedicine (TM) family: Telemedicine (TM), Telehealth (TH), and Telecare (TC) [
14,
28,
29]. Although Taiwanese Telecare pilot schemes have proven the feasibility of TC, there were not many remarkable results of cost-saving from TH and TM. Moreover, the cases of successful business models (BMs) still remain open issues. The results of Taiwanese pilot schemes were varied. Among these issues of CH, payment models are one of the most important issues as they play an important role in keeping CH businesses sustainable. The CH in Taiwan, like many other areas, have an issue of being sustainable after government funding has finished. Designing comprehensive BMs becomes the key to success.
According to Pare et al. [
30,
31], the results of a systematic review of home telemonitoring, after surveying 65 programs across North America, Europe, and Asia, show the feasibility of telemonitoring healthcare [
32]. However, the results for Taiwanese telemonitoring programs from 2007–2009 have shown that Taiwanese programs are competitive in terms of patient acceptance and satisfaction; a decrease in hospital admissions and a decrease in emergency room visits (shown in
Table 1 and
Table 2).
The reasons, such as “preventing ill health”, “maximizing the potential of technology”, and “supporting workforce” were those which drove the Telehealth (TH) pilot project in Taiwan [
33]. It was initially executed in 2008 and within one year, three different models had a noticeable performance:
In the home care model: the hospital readmission rate had a reduction of around 61%; the hospital visit rate had a decrease of over 1%;
In community care models, the medication non-adherence rate had a decline of over 76%;
In the residential-care model, the readmission rate to the hospital was reduced by over 25%, nosocomial infection decreased by over 38%, and the drug duplication rate declined to 53% [
34].
The concept of this TC monitoring is to allow the long-term management of chronic illnesses as well as providing immediate information, to give an early warning of possible diseases—both of which meet the goal of preventive healthcare.
People in Taiwan tend to share the same feeling of being “Aging-in-Place”, which offers remote health a strong reason to develop [
35,
36,
37,
38]. Pressure on financially constrained healthcare systems is exacerbated by the stress of heavy workloads among healthcare staff. Irrespective of the national effort involved, the wish of the Taiwanese democracy is to maintain and improve its universal healthcare system, but hard work alone cannot maintain it anymore. Therefore, what are the options when putting in more human effort is no longer an option?
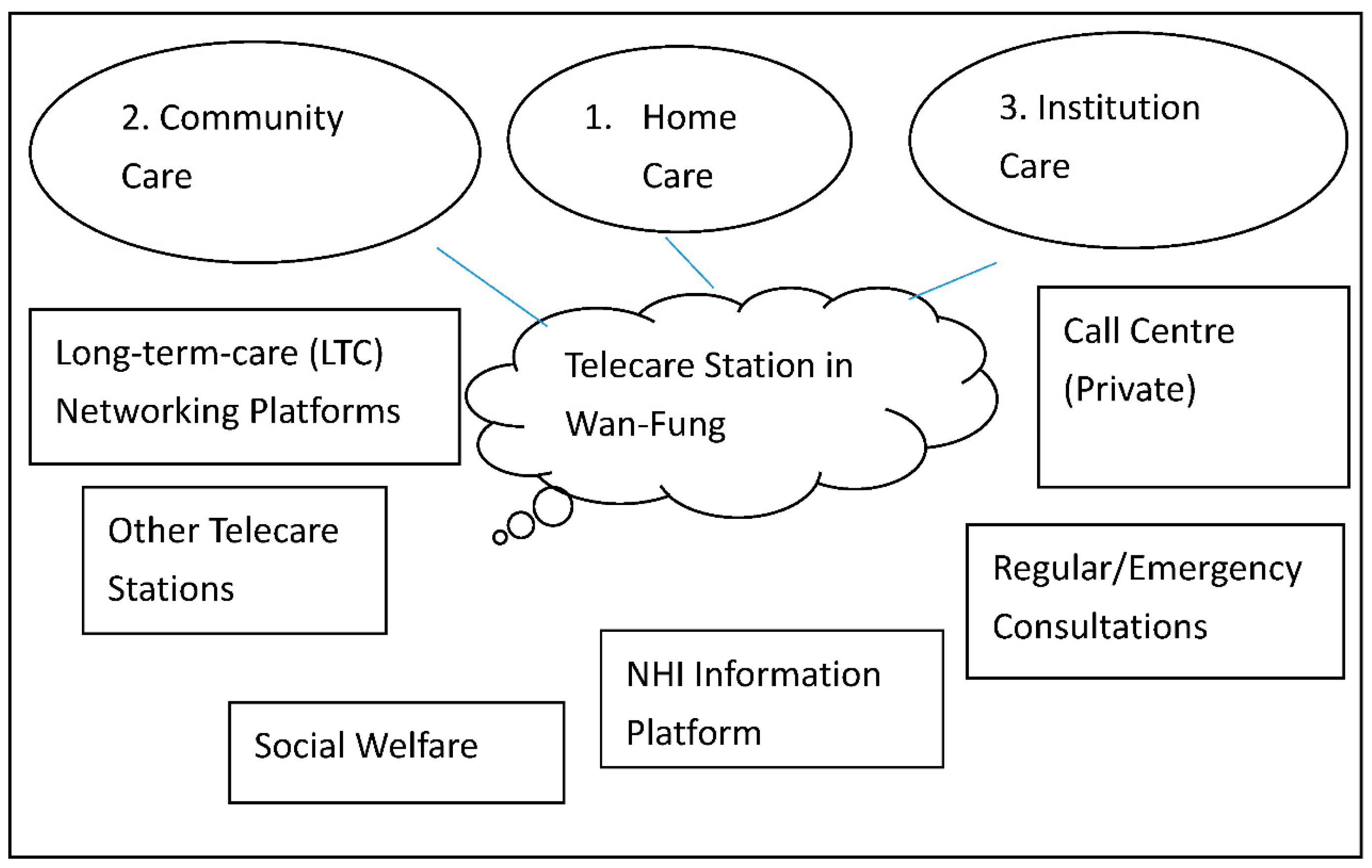
In the TC pilot project, an electronic care records exchange system and an authorized environment were constructed under three service models (home care, community care, and institutional care) in order to offer more integrated care services (shown in
Figure 2). These three models are classified and featured according to where the care is facilitated. The home care is mainly supported full time by the family members of the care receivers while the community model is supported by community facilitators in the daytime and family members after their working hours. As for the institutional model, it is commonly for those who cannot be supported by their family and community members. They will be cared by the institution required in a fulltime base, such as a care home. In general, these three models work independently. However, they will seek help from each other once they are in need. The community care service model aims to establish a community model by connecting various community medical care service resources. The home service model seeks to introduce more than 150 home subjects and connect more than five home care service resources. The institutional care service model cooperates with hospitals and nursing homes to construct two nursing home models. In order to support and monitor quality customer service, 24-hour call centers are established. Long-term care (LTC) networking platforms are built to offer integrated, seamless care by connecting subjects’ information from different care service providers with a referral system to increase resource connecting efficiency. Many educational and promotional events are held to spread the word about these three care service models in order to encourage their potential duplication and expansion.
While some researchers argue that the incorporation of new technologies may not contribute to patient satisfaction, a successful Taiwanese pilot project has proven that this application is beneficial for building up trust and mutual understanding between patients and hospitals and also for reducing criticisms of hospitals [
39,
40]. This project has also proven that TC is effective in maximizing the potential of technology in addition to showing several other immeasurable benefits, such as allocated medical resources and preventive health [
14].
Although this government-sponsored platform can enable tele-monitoring and patients’ self-management to allow remote residents living independently, some issues remained to be addressed. Compared to the institution care model, community care and home care models are more culturally accepted among these three models. As the concept of living with parents and taking care of parents at home are the mainstream in Taiwanese society. To promote the facilities and benefits of institutional care may be an opportunity of action. With the shift of family concept, institutional care may become more and more population in the future. For the other two models, the cost issue may be the most relevant factor influencing people using CH facilities. Most of the users are happy about the services, but only a few people are willing to pay for them. It is suggested that developing a comprehensive business model will be critical for sustaining the CH system of home and community model. What they have in common is that concerns of system integration, information security, and multidisciplinary collaboration need to be resolved among these three models. These challenges will be further communicated in the Result and Discussion Section. The findings of Taiwanese experience imply that users, especially older adults are seeking the care environment that can allow them to live with dignity and comfort. Therefore, it is relevant to understand the key factors of CH’s service models for the benefits of promoting and developing the CH industry.
1.3. Conceptual Framework
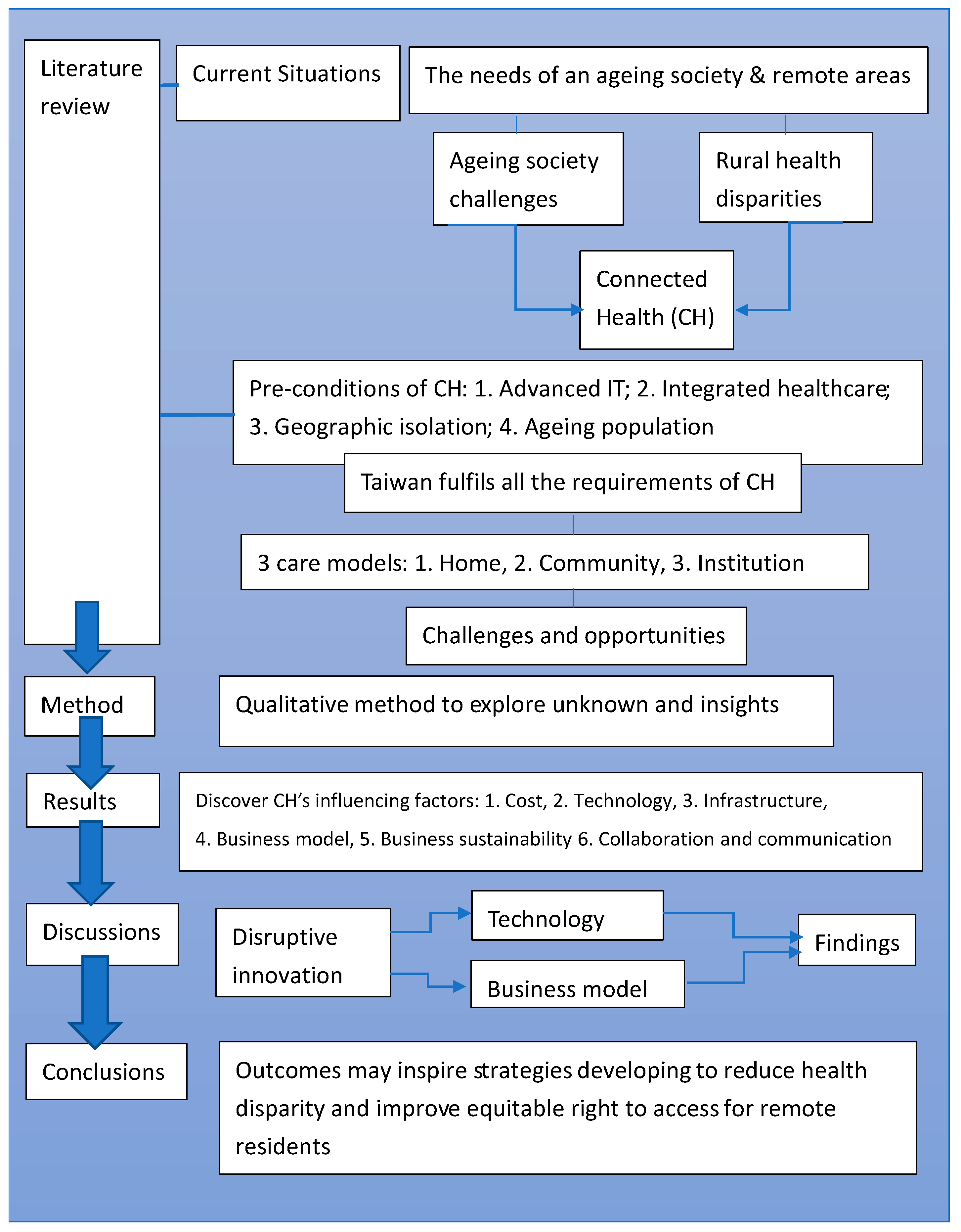
A conceptual framework was developed according to the literature review and will be further developed accordingly after the data analysis, as shown in
Figure 3. The initial issues of CH have been identified in the literature review and further CH challenges have been assessed through data collection and analysis.
According to the three care models mentioned above, they reveal that the institutional care model has potential to be expanded; a sustainable BM needs to be developed to resolve issues of system integration, information security, and multidisciplinary collaboration. Specifically, these issues can be concluded as costs, infrastructure, technology, business model, communication and collaboration, and business sustainability. A further study can be designed based on the characteristics of the factors related to CH in the results section, so that effective investigations of next stage can be developed and followed up.
In the discussion, the disruptive innovation theory and relevant literature are employed to communicate with the findings. Key factors were identified and classified into two groups: generic to health systems and specific to CH inclusion. Generally, it seeks to discover how current health infrastructure can support the implementation of CH. Specifically, it aims to investigate how technology can mediate between geographic isolation and accessibility and how a business model can interact with cost and purchase capability/affordability. Business model and business sustainability are also crucial factors to be discussed, as both direct cost and indirect cost are relevant factors influencing remote residents’ affordability. Therefore, it is relevant to understand the key factors influencing the application of Connected Health in remote areas in Taiwan with a qualitative pilot study for the benefits of promoting and developing the CH industry.
This pilot study aimed to identify future directions and information for conducting the multi-stage interviews for collecting the data more effectively. According to the finding of this study, a comprehensive research for investigating CH’s sustainability and potential strategies that may contribute to academia, industry and government can be designed in the next stage.
Research questions:
- (1)
What are the factors influencing the implementation of connected health in Taiwanese remote areas as perceived by stakeholders?
- (2)
Which factors are perceived by stakeholders as specifically important to the adoption, implementation, and continuation of connected health in remote areas?
- (3)
What are the perceived facilitators and barriers for users in remote areas to access healthcare service through technology?
This research topic is valuable and valid as it influences a human being’s life to such a significant degree. It is particularly important when we are facing global economic and social challenges. It could possibly transfer threats into opportunities. It potentially can generate knowledge that will make contributions to improving efficiency and effectiveness in the healthcare sector.








{kind=link}
{kind=link}
{kind=link}
{kind=link}