A Cohort Study of Korean Radiation Workers: Baseline Characteristics of Participants


Abstract
:1. Introduction
2. Materials and Methods
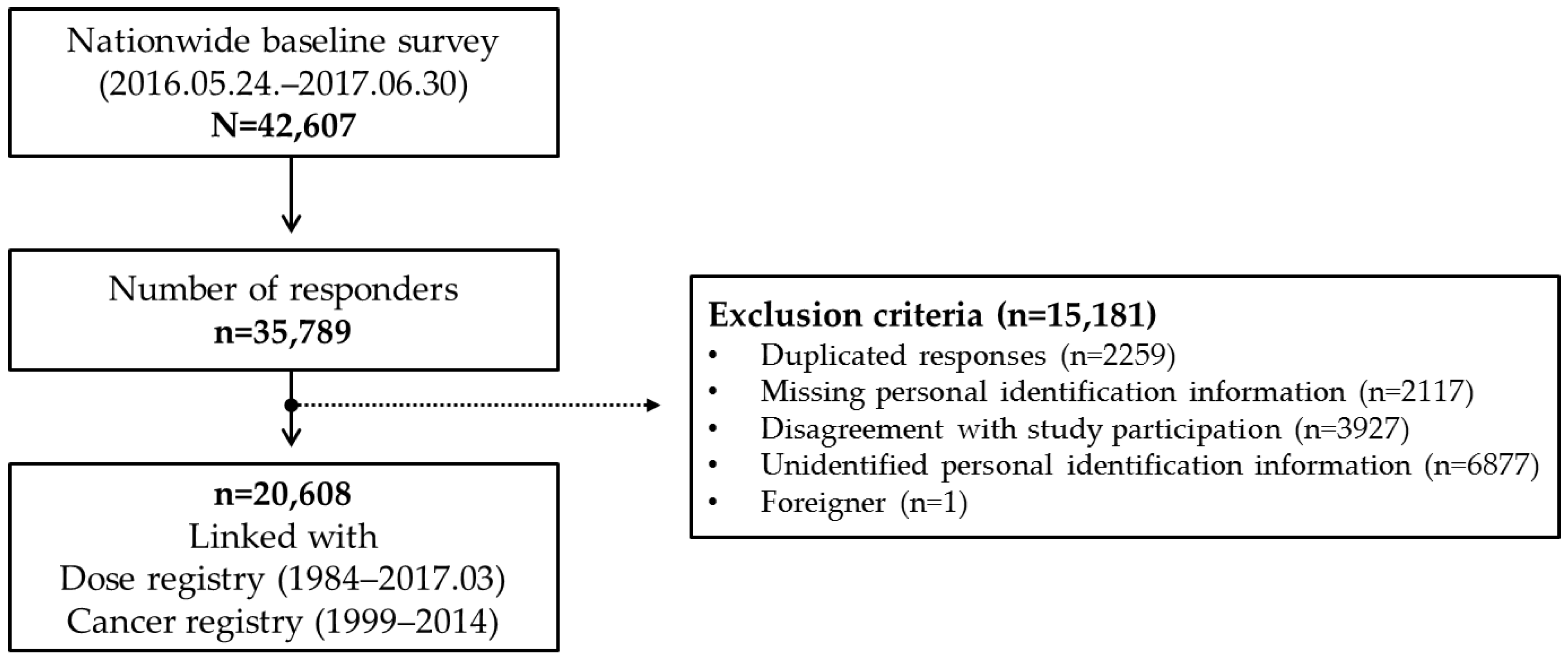
2.1. Study Population and Cohort Enrollment
2.2. Dosimetry and Data for Cancer Incidence
2.3. Data Analysis
2.4. Ethics Approval
3. Results
3.1. Baseline Characteristics of the Cohort
3.2. Distribution of the Radiation Dose of the Cohort
3.3. Cancer Incidence of the Cohort
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Laurier, D.; Richardson, D.B.; Cardis, E.; Daniels, R.D.; Gillies, M.; O’Hagan, J.; Hamra, G.B.; Haylock, R.; Leuraud, K.; Moissonnier, M.; et al. The International Nuclear Workers Study (Inworks): A Collaborative Epidemiological Study to Improve Knowledge About Health Effects of Protracted Low-Dose Exposure. Radiat. Prot. Dosimetry 2017, 173, 21–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leuraud, K.; Richardson, D.B.; Cardis, E.; Daniels, R.D.; Gillies, M.; O’Hagan, J.A.; Hamra, G.B.; Haylock, R.; Laurier, D.; Moissonnier, M.; et al. Ionising radiation and risk of death from leukaemia and lymphoma in radiation-monitored workers (INWORKS): An international cohort study. Lancet Haematol. 2015, 2, e276–e281. [Google Scholar] [CrossRef] [Green Version]
- Richardson, D.B.; Cardis, E.; Daniels, R.D.; Gillies, M.; O’Hagan, J.A.; Hamra, G.B.; Haylock, R.; Laurier, D.; Leuraud, K.; Moissonnier, M.; et al. Risk of cancer from occupational exposure to ionising radiation: Retrospective cohort study of workers in France, the United Kingdom, and the United States (INWORKS). BMJ 2015, 351, h5359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohan, A.K.; Hauptmann, M.; Freedman, D.M.; Ron, E.; Matanoski, G.M.; Lubin, J.H.; Alexander, B.H.; Boice, J.D., Jr.; Doody, M.M.; Linet, M.S. Cancer and other causes of mortality among radiologic technologists in the United States. Int. J. Cancer 2003, 103, 259–267. [Google Scholar] [CrossRef]
- Zielinski, J.M.; Garner, M.J.; Krewski, D.; Ashmore, J.P.; Band, P.R.; Fair, M.E.; Jiang, H.; Letourneau, E.G.; Semenciw, R.; Sont, W.N. Decreases in occupational exposure to ionizing radiation among Canadian dental workers. J. Can. Dent. Assoc. 2005, 71, 29–33. [Google Scholar] [CrossRef]
- Muirhead, C.R.; O’Hagan, J.A.; Haylock, R.G.; Phillipson, M.A.; Willcock, T.; Berridge, G.L.; Zhang, W. Mortality and cancer incidence following occupational radiation exposure: Third analysis of the National Registry for Radiation Workers. Br. J. Cancer 2009, 100, 206–212. [Google Scholar] [CrossRef]
- Ahn, Y.S.; Park, R.M.; Koh, D.H. Cancer admission and mortality in workers exposed to ionizing radiation in Korea. J. Occup. Environ. Med. 2008, 50, 791–803. [Google Scholar] [CrossRef]
- Jeong, M.; Jin, Y.W.; Yang, K.H.; Ahn, Y.O.; Cha, C.Y. Radiation exposure and cancer incidence in a cohort of nuclear power industry workers in the Republic of Korea, 1992–2005. Radiat. Environ. Biophys. 2010, 49, 47–55. [Google Scholar] [CrossRef]
- Personal Information Protection Act. Articles 15 to 22 Section 1. 2014. Available online: http://www.global-regulation.com/law/korea/644669/personal-information-protection-act.html. (accessed on 15 March 2020).
- Seo, S.; Lim, W.Y.; Lee, D.N.; Kim, J.U.; Cha, E.S.; Bang, Y.J.; Lee, W.J.; Park, S.; Jin, Y.W. Assessing the health effects associated with occupational radiation exposure in Korean radiation workers: Protocol for a prospective cohort study. BMJ Open 2018, 8, e017359. [Google Scholar] [CrossRef] [Green Version]
- Cardis, E.; Vrijheid, M.; Blettner, M.; Gilbert, E.; Hakama, M.; Hill, C.; Howe, G.; Kaldor, J.; Muirhead, C.R.; Schubauer-Berigan, M.; et al. Risk of cancer after low doses of ionising radiation: Retrospective cohort study in 15 countries. BMJ 2005, 331, 77. [Google Scholar] [CrossRef] [Green Version]
- Telle-Lamberton, M.; Samson, E.; Caer, S.; Bergot, D.; Bard, D.; Bermann, F.; Gelas, J.M.; Giraud, J.M.; Hubert, P.; Metz-Flamant, C.; et al. External radiation exposure and mortality in a cohort of French nuclear workers. Occup. Environ. Med. 2007, 64, 694–700. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villoing, D.; Yoder, R.C.; Passmore, C.; Bernier, M.O.; Kitahara, C.M. A U.S. Multicenter Study of Recorded Occupational Radiation Badge Doses in Nuclear Medicine. Radiology 2018, 287, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.J.; Ha, M.; Hwang, S.S.; Lee, K.M.; Jin, Y.W.; Jeong, M.; Jun, J.K.; Cha, E.S.; Ko, Y.; Choi, K.H.; et al. The radiologic technologists’ health study in South Korea: Study design and baseline results. Int. Arch. Occup. Environ. Health 2015, 88, 759–768. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.J.; Ko, S.; Bang, Y.J.; Cha, E.S.; Lee, K.M. Mortality among diagnostic medical radiation workers in South Korea, 1996–2015. Occup. Environ. Med. 2018, 75, 739–741. [Google Scholar] [CrossRef] [PubMed]
- Nuclear Safety Yearbook, 2018; Nuclear Safety and Security Commission, Korea Institute of Nuclear Safety, Korea Institute of Nuclear Nonproliferation and Control: Daejeon, Korea, 2019.
- Sources and Effects of Ionizing Radiation; United Nations Scientific Committee on the Effects of Atomic Radiation: UNSCEAR 2008 Report to the General Assembly, with Scientific Annexes; United Nations: New York, NY, USA, 2010.
- Sources, Effects and Risk of Ionizing Radiation UNSCEAR 2017 Report; United Nations Scientific Committee on the Effects of Atomic Radiation; United Nations: New York, NY, USA, 2018.
- 2018 Report Occupational Radiation Exposure in Diagnostic Radiology in Korea; Centers for Diseases Control and Prevent: Cheongju, Korea, 2019.
- Lee, S.Y.; Lim, H.S.; Lee, J.; Kim, H.S. Evaluation of diagnostic medical exposure in Republic of Korea. Radiat. Prot. Dosimetry 2016, 168, 388–395. [Google Scholar] [CrossRef]
- National Helath Insurance System of Korea 2015; National Health Insurance Service: Ilsan, Korea, 2016.
- Occupational Safety And Health Act. Article 72. 2020. Available online: https://www.global-regulation.com/law/korea/644100/occupational-safety-and-health-act.html. (accessed on 27 March 2020).
- Kang, Y.J.; Myong, J.-P.; Eom, H.; Choi, B.; Park, J.H.; Kim, E.-A.L. The current condition of the workers’ general health examination in South Korea: A retrospective study. Ann. Occup. Environ. Med. 2017, 29, 6. [Google Scholar] [CrossRef] [Green Version]
- Chowdhury, R.; Shah, D.; Payal, A.R. Healthy Worker Effect Phenomenon: Revisited with Emphasis on Statistical Methods - A Review. Indian J. Occup Environ. Med. 2017, 21, 2–8. [Google Scholar] [CrossRef]
- Li, C.-Y.; Sung, F.-C. A review of the healthy worker effect in occupational epidemiology. Occup. Med. 1999, 49, 225–229. [Google Scholar] [CrossRef] [Green Version]
- Engels, H.; Swaen, G.M.; Slangen, J.; van Amersvoort, L.; Holmstock, L.; Van Mieghem, E.; Van Regenmortel, I.; Wambersie, A. Radiation exposure and cause specific mortality among nuclear workers in Belgium (1969–1994). Radia.t Prot. Dosimetry 2005, 117, 373–381. [Google Scholar] [CrossRef]
- Guerin, S.; Richard, G.; Biau, A.; Lebre, S.; Crescini, D.; Haddy, N.; Guldner, L.; Paoletti, C.; Hill, C.; de Vathaire, F. Cancer mortality among French nuclear contract workers. Am. J. Ind Med. 2009, 52, 916–925. [Google Scholar] [CrossRef]
- Habib, R.R.; Abdallah, S.M.; Law, M.; Kaldor, J. Cancer incidence among Australian nuclear industry workers. J. Occup. Health 2006, 48, 358–365. [Google Scholar] [CrossRef] [Green Version]
- Howe, G.R.; Zablotska, L.B.; Fix, J.J.; Egel, J.; Buchanan, J. Analysis of the mortality experience amongst U.S. nuclear power industry workers after chronic low-dose exposure to ionizing radiation. Radiat. Res. 2004, 162, 517–526. [Google Scholar] [CrossRef] [PubMed]
- Ivanov, V.K.; Maksioutov, M.A.; Chekin, S.; Kruglova, Z.G.; Petrov, A.V.; Tsyb, A.F. Radiation-epidemiological analysis of incidence of non-cancer diseases among the Chernobyl liquidators. Health Phys. 2000, 78, 495–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schubauer-Berigan, M.K.; Daniels, R.D.; Bertke, S.J.; Tseng, C.Y.; Richardson, D.B. Cancer Mortality through 2005 among a Pooled Cohort of U.S. Nuclear Workers Exposed to External Ionizing Radiation. Radiat. Res. 2015, 183, 620–631. [Google Scholar] [CrossRef] [PubMed]
- Sont, W.N.; Zielinski, J.M.; Ashmore, J.P.; Jiang, H.; Krewski, D.; Fair, M.E.; Band, P.R.; Letourneau, E.G. First analysis of cancer incidence and occupational radiation exposure based on the National Dose Registry of Canada. Am. J. Epidemiol. 2001, 153, 309–318. [Google Scholar] [CrossRef]
- Sigurdson, A.J.; Doody, M.M.; Rao, R.S.; Freedman, D.M.; Alexander, B.H.; Hauptmann, M.; Mohan, A.K.; Yoshinaga, S.; Hill, D.A.; Tarone, R.; et al. Cancer incidence in the US radiologic technologists health study, 1983-1998. Cancer 2003, 97, 3080–3089. [Google Scholar] [CrossRef]
- Park, S.; Oh, C.M.; Cho, H.; Lee, J.Y.; Jung, K.W.; Jun, J.K.; Won, Y.J.; Kong, H.J.; Choi, K.S.; Lee, Y.J.; et al. Association between screening and the thyroid cancer “epidemic” in South Korea: Evidence from a nationwide study. BMJ 2016, 355, i5745. [Google Scholar] [CrossRef] [Green Version]
- Ron, E.; Lubin, J.H.; Schneider, A.B. Thyroid cancer incidence. Nature 1992, 360, 113. [Google Scholar] [CrossRef]
- Ahn, H.S.; Kim, H.J.; Welch, H.G. Korea’s thyroid-cancer “epidemic”—Screening and overdiagnosis. N Engl. J. Med. 2014, 371, 1765–1767. [Google Scholar] [CrossRef]
- Kesminiene, A.; Evrard, A.S.; Ivanov, V.K.; Malakhova, I.V.; Kurtinaitise, J.; Stengrevics, A.; Tekkel, M.; Chekin, S.; Drozdovitch, V.; Gavrilin, Y.; et al. Risk of thyroid cancer among chernobyl liquidators. Radiat. Res. 2012, 178, 425–436. [Google Scholar] [CrossRef] [Green Version]
- Lee, W.J.; Preston, D.L.; Cha, E.S.; Ko, S.; Lim, H. Thyroid cancer risks among medical radiation workers in South Korea, 1996–2015. Environ. Health 2019, 18, 19. [Google Scholar] [CrossRef] [Green Version]
- Zabel, E.W.; Alexander, B.H.; Mongin, S.J.; Doody, M.M.; Sigurdson, A.J.; Linet, M.S.; Freedman, D.M.; Hauptmann, M.; Mabuchi, K.; Ron, E. Thyroid cancer and employment as a radiologic technologist. Int. J. Cancer 2006, 119, 1940–1945. [Google Scholar] [CrossRef]
- Galea, S.; Tracy, M. Participation rates in epidemiologic studies. Annals Epidemiol. 2007, 17, 643–653. [Google Scholar] [CrossRef]
- Nohr, E.A.; Liew, Z. How to investigate and adjust for selection bias in cohort studies. Acta Obstet. Gynecol. Scand. 2018, 97, 407–416. [Google Scholar] [CrossRef] [Green Version]
- Hamra, G.B.; Richardson, D.B.; Cardis, E.; Daniels, R.D.; Gillies, M.; O’Hagan, J.A.; Haylock, R.; Laurier, D.; Leuraud, K.; Moissonnier, M.; et al. Cohort Profile: The International Nuclear Workers Study (INWORKS). Int. J. Epidemiol. 2016, 45, 693–699. [Google Scholar] [CrossRef]
- Boice, J.D., Jr.; Ellis, E.D.; Golden, A.P.; Girardi, D.J.; Cohen, S.S.; Chen, H.; Mumma, M.T.; Shore, R.E.; Leggett, R.W. The Past Informs the Future: An Overview of the Million Worker Study and the Mallinckrodt Chemical Works Cohort. Health Phys. 2018, 114, 381–385. [Google Scholar] [CrossRef] [PubMed]
- Gillies, M.; Haylock, R. The cancer mortality and incidence experience of workers at British Nuclear Fuels plc, 1946-2005. J. Radiol. Prot. 2014, 34, 595–623. [Google Scholar] [CrossRef] [PubMed]
- Leuraud, K.; Fournier, L.; Samson, E.; Caër-Lorho, S.; Laurier, D. Mortality in the French cohort of nuclear workers. Radioprotection 2017, 52, 199–210. [Google Scholar] [CrossRef] [Green Version]
- Zablotska, L.B.; Lane, R.S.; Thompson, P.A. A reanalysis of cancer mortality in Canadian nuclear workers (1956-1994) based on revised exposure and cohort data. Br. J. Cancer 2014, 110, 214–223. [Google Scholar] [CrossRef] [Green Version]
- Jung, K.W.; Won, Y.J.; Kong, H.J.; Oh, C.M.; Cho, H.; Lee, D.H.; Lee, K.H. Cancer statistics in Korea: Incidence, mortality, survival, and prevalence in 2012. Cancer Res. Treat. 2015, 47, 127–141. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | n | (%) |
|---|---|---|
| Sex | ||
| Men | 17,831 | (86.5%) |
| Women | 2777 | (13.5%) |
| Birth year | ||
| ~1960 | 1391 | (6.7%) |
| 1961–1970 | 3449 | (16.7%) |
| 1971–1980 | 5891 | (28.6%) |
| 1981~ | 9877 | (47.9%) |
| Education level | ||
| Less than high school graduation | 159 | (0.8%) |
| High school graduation | 4539 | (22.6%) |
| College graduation and above | 15,402 | (76.6%) |
| Marital status | ||
| Unmarried | 7881 | (39.2%) |
| Married/living together | 11,982 | (59.6%) |
| Other (divorced, widow, separated) | 233 | (1.2%) |
| BMI, kg/m2 | ||
| Underweight (<18.5) | 490 | (2.6%) |
| Normal weight (18.5–24.9) | 11,677 | (61.2%) |
| Overweight (25.0–29.9) | 6012 | (31.5%) |
| Obese (≥30.0) | 913 | (4.8%) |
| Regular exercise | ||
| No | 9061 | (44.3%) |
| Yes | 11,385 | (55.7%) |
| Smoking status | ||
| Never (non-smoker) | 8442 | (41.3%) |
| Ex-smoker | 3615 | (17.7%) |
| Yes (smoker) | 8361 | (40.9%) |
| Alcohol status | ||
| No | 3276 | (16.0%) |
| Yes | 17,239 | (84.0%) |
| Characteristics | n | (%) |
|---|---|---|
| Occupation | ||
| Public institute | 676 | (3.3%) |
| Education institute | 2010 | (9.8%) |
| Military | 165 | (0.8%) |
| Industrial radiography | 3517 | (17.1%) |
| Industry | 3886 | (18.9%) |
| Research institute | 1139 | (5.5%) |
| Nuclear power plant | 6328 | (30.7%) |
| Medical institute | 2887 | (14.0%) |
| Calendar year of hiring | ||
| ~1989 | 1272 | (6.2%) |
| 1990–1999 | 2694 | (13.1%) |
| 2000–2009 | 4569 | (22.2%) |
| 2010~ | 12,073 | (58.6%) |
| Age at the start of radiation work, years | ||
| <20 | 785 | (3.8%) |
| 20–29 | 12,168 | (59.0%) |
| 30–39 | 5449 | (26.4%) |
| 40–49 | 1565 | (7.6%) |
| ≥50 | 641 | (3.1%) |
| Employment status | ||
| Regular employment | 16,450 | (82.6%) |
| Irregular employment (temporary contract) | 2885 | (14.5%) |
| Irregular employment (daily contract) | 589 | (3.0%) |
| Duration of employment, years | ||
| ≤4 | 9265 | (45.0%) |
| 5–9 | 4310 | (20.9%) |
| 10–14 | 2372 | (11.5%) |
| ≥15 years | 4661 | (22.6%) |
| Experience of warning for exceeding 5 mSv per quarter | ||
| No | 17,857 | (90.4%) |
| Yes | 901 | (4.6%) |
| I do not know | 987 | (5.0%) |
| Night shifts | ||
| None | 10,361 | (51.1%) |
| <1 year | 2544 | (12.5%) |
| 1–5 years | 4215 | (20.8%) |
| >5 years | 3152 | (15.5%) |
| Radiation source | ||
| None | 2873 | (14.6%) |
| Sealed isotope | 5309 | (26.9%) |
| Unsealed isotope | 2430 | (12.3%) |
| Radiation-generating device | 5559 | (28.2%) |
| Not sure | 3539 | (18.0%) |
| Distance from radiation source | ||
| <1 m | 3752 | (20.0%) |
| 1–3 m | 4866 | (25.9%) |
| >3 m | 10,149 | (54.1%) |
| While engaged in radiation work, white blood cell counts fell below the normal range | ||
| No | 17,922 | (90.5%) |
| Yes | 498 | (2.5%) |
| Not sure (or had never had a health examination) | 1381 | (7.0%) |
| Report Year | No. of Workers | Annual Collective Dose (man.mSv) | Annual Radiation Dose (mSv [mean ± SD]) | No. of Workers >20 mSv Per Year (%) | |
|---|---|---|---|---|---|
| 1984 | 417 | 1876.55 | 4.5 ± 6.9 | 25 | (6.0) |
| 1985 | 563 | 1831.57 | 3.2 ± 5.5 | 14 | (2.5) |
| 1986 | 683 | 3150.87 | 4.6 ± 7.5 | 46 | (6.7) |
| 1987 | 870 | 2923.13 | 3.4 ± 5.8 | 25 | (2.9) |
| 1988 | 1085 | 4210.68 | 3.9 ± 7.2 | 64 | (5.9) |
| 1989 | 1213 | 3428.80 | 2.8 ± 4.9 | 20 | (1.6) |
| 1990 | 1348 | 4567.53 | 3.4 ± 6.0 | 42 | (3.1) |
| 1991 | 1491 | 3494.45 | 2.3 ± 4.4 | 21 | (1.4) |
| 1992 | 1690 | 4145.30 | 2.5 ± 4.4 | 19 | (1.1) |
| 1993 | 1763 | 4557.83 | 2.6 ± 4.7 | 24 | (1.4) |
| 1994 | 2041 | 4554.59 | 2.2 ± 4.2 | 18 | (0.9) |
| 1995 | 2457 | 6528.34 | 2.7 ± 5.1 | 47 | (1.9) |
| 1996 | 2725 | 6803.13 | 2.5 ± 4.5 | 32 | (1.2) |
| 1997 | 2890 | 5958.99 | 2.1 ± 3.8 | 14 | (0.5) |
| 1998 | 3140 | 6199.69 | 2.0 ± 3.6 | 7 | (0.2) |
| 1999 | 3502 | 6887.96 | 2.0 ± 3.3 | 6 | (0.2) |
| 2000 | 3696 | 7041.37 | 1.9 ± 3.4 | 14 | (0.4) |
| 2001 | 4008 | 7156.33 | 1.8 ± 3.4 | 9 | (0.2) |
| 2002 | 4212 | 6922.35 | 1.6 ± 2.9 | 10 | (0.2) |
| 2003 | 4463 | 6950.28 | 1.6 ± 2.8 | 8 | (0.2) |
| 2004 | 4925 | 8413.59 | 1.7 ± 3.3 | 15 | (0.3) |
| 2005 | 5302 | 8732.94 | 1.6 ± 3.1 | 17 | (0.3) |
| 2006 | 5812 | 9113.73 | 1.6 ± 2.9 | 14 | (0.2) |
| 2007 | 6447 | 10,275.9 | 1.6 ± 2.9 | 10 | (0.2) |
| 2008 | 6986 | 9385.69 | 1.3 ± 3.2 | 31 | (0.4) |
| 2009 | 7605 | 9844.92 | 1.3 ± 3.1 | 27 | (0.4) |
| 2010 | 8350 | 11,133.14 | 1.3 ± 3.3 | 46 | (0.6) |
| 2011 | 9440 | 10,743.07 | 1.1 ± 2.8 | 30 | (0.3) |
| 2012 | 10,803 | 13,282.39 | 1.2 ± 3.4 | 50 | (0.5) |
| 2013 | 11,965 | 15,290.65 | 1.3 ± 3.5 | 72 | (0.6) |
| 2014 | 13,419 | 11,881.34 | 0.9 ± 2.4 | 18 | (0.1) |
| 2015 | 15,568 | 10,974.39 | 0.7 ± 2.2 | 17 | (0.1) |
| 2016 | 18,861 | 11,352.00 | 0.6 ± 1.9 | 15 | (0.1) |
| 2017 a | 18,411 | 2844.70 | 0.2 ± 0.7 | 3 | (0.0) |
| Total | 20,608 | 242,198.04 | 1.3 ± 3.2 | 602 | (2.9) |
| Cancer/Site | Men (n = 16,943) | Women (n = 2584) | ||||
|---|---|---|---|---|---|---|
| Obs | SIR (95% CI) | Obs | SIR (95% CI) | |||
| All cancers combined (C00–C96) | 189 | 0.76 | (0.66–0.88) | 23 | 0.84 | (0.56–1.26) |
| Oral cavity (C03–C06) | 1 | 1.15 | (0.16–8.13) | 0 | 0 | (0–99.86) |
| Salivary gland (C07–C08) | 3 | 2.98 | (0.96–9.25) | 0 | 0 | (0–42.80) |
| Stomach (C16) | 44 | 0.95 | (0.70–1.27) | 1 | 0.63 | (0.09–4.45) |
| Small intestine (C17) | 1 | 0.84 | (0.12–5.94) | 0 | 0 | (0–74.90) |
| Colon (C18) | 15 | 0.93 | (0.56–1.54) | 0 | 0 | (0–4.68) |
| Rectum (C19) | 10 | 0.56 | (0.30–1.04) | 0 | 0 | (0–5.08) |
| Liver (C22) | 7 | 0.20 | (0.10–0.43) | 0 | 0 | (0–8.81) |
| Nose, sinuses, etc. (C30–C31) | 2 | 2.98 | (0.74–11.91) | 0 | 0 | (0–99.86) |
| Lung (C33–C34) | 4 | 0.23 | (0.09–0.61) | 0 | 0 | (0–5.76) |
| Bone (C40–C41) | 1 | 0.89 | (0.13–6.31) | 0 | 0 | (0–33.29) |
| Melanoma of skin (C43) | 1 | 1.41 | (0.20–9.98) | 0 | 0 | (0–74.90) |
| Other skin (C44) | 1 | 0.30 | (0.04–2.11) | 0 | 0 | (0–18.72) |
| Breast (C50) | 0 | 0 | (0–14.97) | 9 | 1.51 | (0.79–2.90) |
| Cervix uteri (C53) | - | - | - | 1 | 0.65 | (0.09–4.60) |
| Uterus, part unspecified (C55) | - | - | - | 1 | 25.86 | (3.64–183.60) |
| Prostate (C61) | 5 | 0.88 | (0.37–2.12) | - | - | - |
| Testis (C62) | 2 | 0.98 | (0.24–3.91) | - | - | - |
| Kidney (C64) | 10 | 1.07 | (0.57–1.98) | 0 | 0 | (0–13.02) |
| Bladder (C67) | 2 | 0.46 | (0.11–1.82) | 0 | 0 | (0–59.91) |
| Brain, nervous system (C70–C72) | 1 | 0.25 | (0.04–1.79) | 0 | 0 | (0–11.98) |
| Thyroid (C73) | 72 | 1.94 | (1.54–2.44) | 11 | 0.92 | (0.51–1.66) |
| Adrenal grand (C74) | 1 | 4.29 | (0.60–30.43) | 0 | 0 | (0–149.79) |
| Hodgkin lymphoma (C81) | 1 | 1.36 | (0.19–9.66) | 0 | 0 | (0–42.80) |
| Non-Hodgkin lymphoma (C82–C86) | 2 | 0.28 | (0.07–1.13) | 0 | 0 | (0–8.32) |
| Multiple myeloma (C90) | 1 | 0.86 | (0.12–6.10) | 0 | 0 | (0–74.90) |
| Leukemia (C91–C95) | 2 | 0.33 | (0.08–1.32) | 0 | 0 | (0–7.88) |
| Characteristics | n | All Cancers Combined | All Cancers Combined Excluding Thyroid Cancer | Thyroid Cancer | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Obs | SIR (95% CI) | Obs | SIR (95% CI) | Obs | SIR (95% CI) | |||||
| Occupation | ||||||||||
| Public institute | 644 | 10 | 1.03 | (0.55–1.91) | 8 | 0.98 | (0.49–1.96) | 2 | 1.29 | (0.32–5.14) |
| Education institute | 1805 | 10 | 0.70 | (0.38–1.30) | 8 | 0.77 | (0.38–1.53) | 2 | 0.51 | (0.13–2.05) |
| Military | 164 | 2 | 2.25 | (0.56–8.99) | 0 | 0 | (0–4.68) | 2 | 8.26 | (2.07–33.04) |
| Industrial radiography | 3415 | 12 | 0.36 | (0.20–0.63) | 10 | 0.38 | (0.20–0.70) | 2 | 0.28 | (0.07–1.13) |
| Industry | 3645 | 42 | 0.96 | (0.71–1.30) | 26 | 0.75 | (0.49–1.05) | 16 | 2.15 | (1.32–3.50) |
| Research institute | 1071 | 17 | 0.63 | (0.39–1.02) | 11 | 0.47 | (0.26–0.85) | 6 | 1.75 | (0.78–3.89) |
| Nuclear power plant | 6037 | 93 | 0.88 | (0.72–1.08) | 53 | 0.59 | (0.45–0.77) | 40 | 2.68 | (1.97–3.65) |
| Medical institute | 2746 | 26 | 0.63 | (0.43–0.93) | 13 | 0.43 | (0.25–0.73) | 13 | 1.23 | (0.72–2.12) |
| Birth year | ||||||||||
| ~1950 | 103 | 8 | 0.45 | (0.23–0.91) | 8 | 0.46 | (0.23–0.93) | 0 | 0 | (0–8.32) |
| 1951–1960 | 1241 | 52 | 0.62 | (0.47–0.81) | 41 | 0.52 | (0.39–0.71) | 11 | 2.01 | (1.11–3.63) |
| 1961–1970 | 3350 | 71 | 0.76 | (0.60–0.96) | 49 | 0.62 | (0.47–0.83) | 22 | 1.46 | (0.96–2.22) |
| 1971–1980 | 5719 | 61 | 1.04 | (0.81–1.34) | 23 | 0.58 | (0.39–0.88) | 38 | 1.97 | (1.44–2.71) |
| 1981–1990 | 7314 | 18 | 0.88 | (0.55–1.40) | 7 | 0.59 | (0.28–1.24) | 11 | 1.27 | (0.71–2.30) |
| 1991~ | 1800 | 2 | 1.85 | (0.46–7.40) | 1 | 1.43 | (0.20–10.17) | 1 | 2.61 | (0.37–18.56) |
| Cancer | Exposed Workers (n = 12,065) | Non-Exposed Workers (n = 7462) | Crude RR (95% CI) | Adj† RR (95% CI) | ||||
|---|---|---|---|---|---|---|---|---|
| Obs | SIR (95% CI) | Obs | SIR (95% CI) | |||||
| All cancers combined | 151 | 0.69 | (0.59–0.81) | 61 | 1.05 | (0.82–1.36) | 0.64 (0.47–0.86) | 0.82 (0.60–1.12) |
| All cancers combined excluding thyroid cancer | 92 | 0.51 | (0.42–0.63) | 37 | 0.79 | (0.58–1.10) | 0.64 (0.44–0.94) | 0.83 (0.56–1.24) |
| Thyroid cancer | 59 | 1.55 | (1.20–2.00) | 24 | 2.17 | (1.46–3.24) | 0.63 (0.39–1.01) | 0.83 (0.49–1.38) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, S.; Seo, S.; Lee, D.; Park, S.; Jin, Y.W. A Cohort Study of Korean Radiation Workers: Baseline Characteristics of Participants. Int. J. Environ. Res. Public Health 2020, 17, 2328. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072328
Park S, Seo S, Lee D, Park S, Jin YW. A Cohort Study of Korean Radiation Workers: Baseline Characteristics of Participants. International Journal of Environmental Research and Public Health. 2020; 17(7):2328. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072328
Chicago/Turabian StylePark, Soojin, Songwon Seo, Dalnim Lee, Sunhoo Park, and Young Woo Jin. 2020. "A Cohort Study of Korean Radiation Workers: Baseline Characteristics of Participants" International Journal of Environmental Research and Public Health 17, no. 7: 2328. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072328