Group Outdoor Health Walks Using Activity Trackers: Measurement and Implementation Insight from a Mixed Methods Feasibility Study


Abstract
:1. Introduction
1.1. Rationale for Group Walks in Nature
1.2. Activity Tracker—Motivator and Intermediate Measure
1.3. Measuring Downstream Health and Wellbeing
1.4. Feasibility Studies
recruitment capability and resulting sample characteristics, data collection procedures and outcome measures, acceptability and suitability of the intervention, the ability to manage and implement the intervention, and preliminary evaluation of participant responses to intervention.[58] (p. 1)
1.5. Study Focus
- Explore the contribution of activity trackers for the recruitment and retention of participants;
- Understand the impact of activity tracker technology on programme implementation;
- Field-test the use of step counts as a measure of physical activity and the SAC scale as a measure of biopsychosocial–spiritual health in studies of nature-based health promotion programmes.
2. Methods
2.1. Nature-based Health Intervention—Activity Tracker GOHW
2.2. Recruitment
2.3. Data Collection and Study Procedures
2.4. Data Collection Instruments
2.4.1. Study Questionnaire
Background Information
Recruitment
Self-report Motivators and Benefits
Self-report Physical Activity
Holistic Health and Wellbeing
2.4.2. Physical Activity Tracker
2.4.3. Walk Attendance, Distance, Duration, Natural Environs
2.4.4. Qualitative Data
3. Results
3.1. Participants
3.2. Recruitment-Retention-Motivation
3.2.1. Recruitment to Walks and Motivation for being Involved
3.2.2. Retention and Motivation for Staying Involved
3.3. Programme Implementation
3.3.1. Walk Leader Characteristics
3.3.2. Activity Tracker System
I found that walkers who wanted a target set were much more engaged throughout the 12 weeks and wanted to see their target on the computer. Those who did not want a target set were less / not interested in the weekly results by about week 5.
3.3.3. Integration of Technology into the GOHW
Activity Tracker Processes
All unassigned trackers at the start of the 12 weeks needed to be charged ready for each walker—but this meant they were all picked up by the iPhone and there was no way to tell which tracker you were assigning [to which walker]. So [you] have to make sure that all but the one you physically have in your hand are out of range of the iPhone when assigning it to a walker.
I found that some days it could be a bit overwhelming at the start of the walk with everyone turning up and immediately asking if they’d been synced! As we had 2 groups (slow and fast) I felt under pressure to get the slower walkers synced first as I was stopping them from going out. I walked with the faster group so was able to sync them as we walked which was much easier! Also had to keep track that I had got everyone synced and quickly check each person’s data and comment on how they had done that week and having the walk register to do!
Impact on the Walk Experience
It is a great incentive. It makes you go out and see how far you can go in a day. I’m not doing as much now as the morning and nights are darker but I did get up to 10,000 steps a day. Now I am doing between 5000–6000 steps. I did 8000 steps yesterday.
The tracker was helpful. It makes you more aware and think ‘I must go out today’, especially when it is a nice day and it makes me walk a bit further. It certainly gives me an incentive to go further.
[The activity tracker GOHW] gave the group a boost and a focus from the “normal” Health Walk… there was more conversations amongst the group about how much they had walked in the week, health and fitness in general...lots of excuses/reasons given by walkers as to why certain days their step count was low! But shows they are thinking about their activity.
3.4. Physical Activity and Health and Wellbeing Measures
3.4.1. Walk Attendance, Distance, Duration, Natural Environs
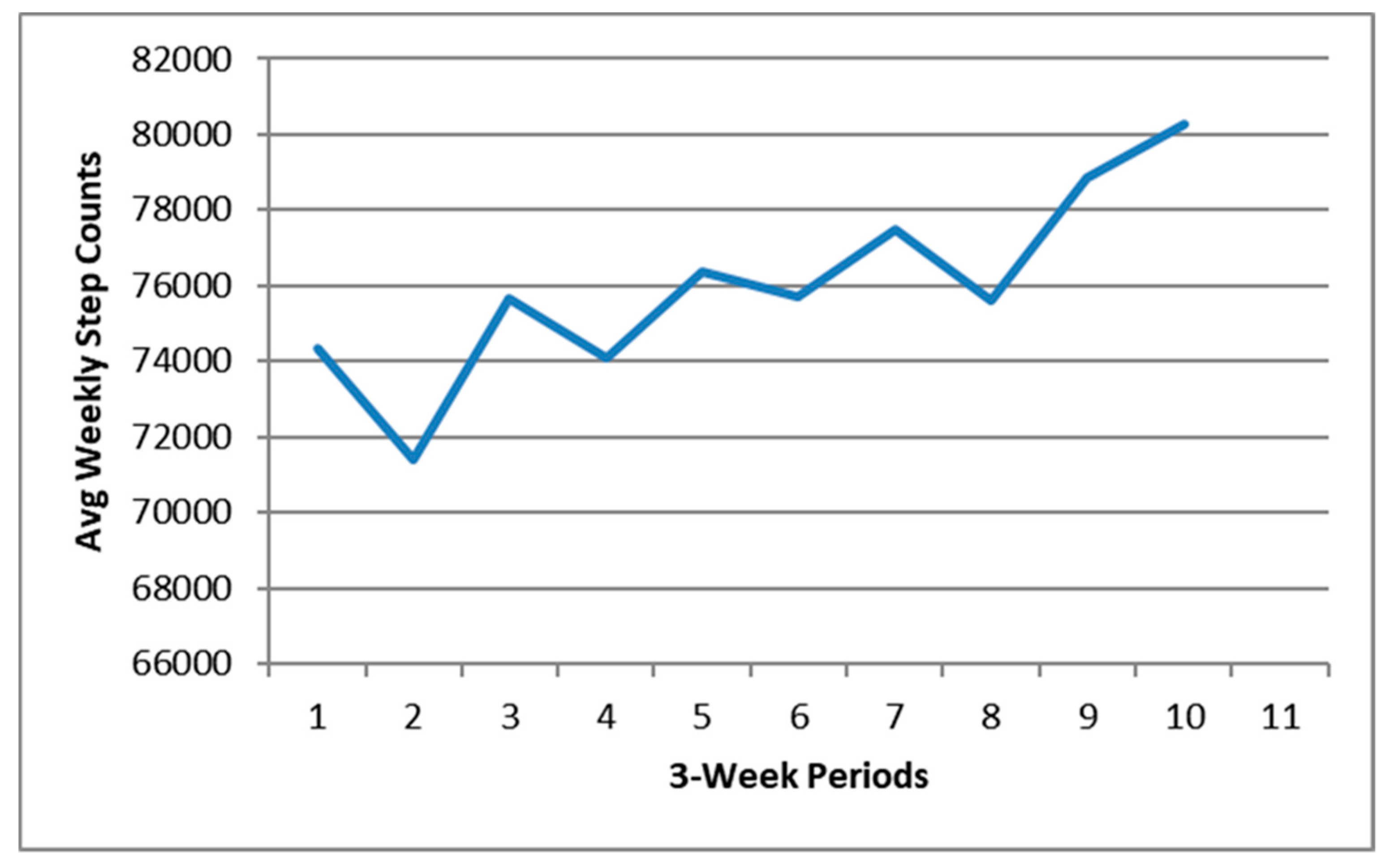
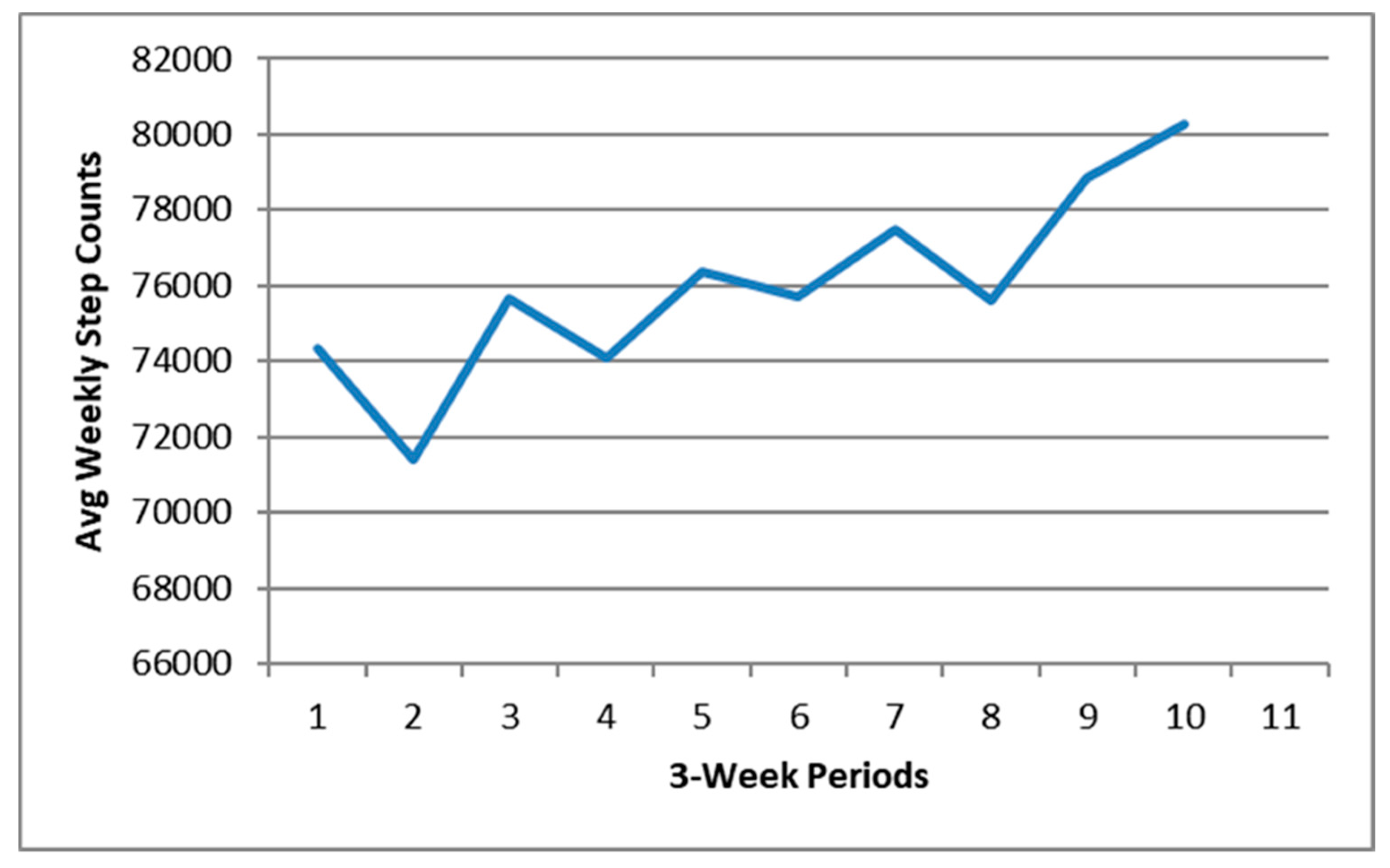
3.4.2. Physical Activity Type and Levels
3.4.3. Health and Wellbeing
4. Discussion
4.1. Motivation for Joining and Maintaining Engagement
4.2. Added Value for Programme Implementation
4.3. Measurement
4.3.1. Intermediate Measure: Physical Activity
4.3.2. Downstream Health and Wellbeing Outcome: Holistic Health and Wellbeing
4.4. Activity Tracker Group Outdoor Health Walks
4.5. Study Limitations
4.6. Future Research
4.7. Implications
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization Noncommunicable Diseases Fact Sheet. Available online: https://www.who.int/en/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 11 October 2019).
- Office for National Statistics Healthcare Expenditure, UK Health Accounts: 2017. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/healthcaresystem/bulletins/ukhealthaccounts/2017 (accessed on 11 October 2019).
- Sisko, A.M.; Keehan, S.P.; Poisal, J.A.; Cuckler, G.A.; Smith, S.D.; Madison, A.J.; Rennie, K.E.; Hardesty, J.C. National health expenditure projections, 2018–2027: Economic and demographic trends drive spending and enrollment growth. Health Aff. 2019, 38, 491–501. [Google Scholar] [CrossRef]
- The Scottish Government Policy: Physical Activity and Sport. Available online: https://beta.gov.scot/policies/physical-activity-sport/ (accessed on 11 October 2019).
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World. Available online: https://www.who.int/ncds/prevention/physical-activity/global-action-plan-2018-2030/en/ (accessed on 11 October 2019).
- Mitchell, J.; Kearney, N.; Teuton, J. What Research Matters for Mental Health Policy in Scotland. Available online: http://www.gov.scot/Resource/0049/00494776.pdf (accessed on 11 October 2019).
- World Health Organization. Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020. Available online: http://www.who.int/nmh/publications/ncd-action-plan/en/ (accessed on 11 October 2019).
- Campbell, A.; Calderwood, C.; Hunter, G.; Murray, A. Physical activity investments that work—Get Scotland walking: A National Walking Strategy for Scotland. Br. J. Sports Med. 2018, 52, 759–760. [Google Scholar] [CrossRef] [Green Version]
- Boone-Heinonen, J.; Evenson, K.R.; Taber, D.R.; Gordon-Larsen, P. Walking for prevention of cardiovascular disease in men and women: A systematic review of observational studies. Obes. Rev. 2009, 10, 204–217. [Google Scholar] [CrossRef] [Green Version]
- Morabia, A.; Costanza, M.C. Does walking 15 minutes a day keep the obesity epidemic away? Simulation of the efficacy of a population wide campaign. Am. J. Public Health 2004, 94, 434–440. [Google Scholar] [CrossRef]
- Pucher, J.; Buehler, R.; Bassett, D.R.; Dannenberg, A.L. Walking and cycling to health: A comparative analysis of city, state, and international data. Am. J. Public Health 2010, 100, 1986–1992. [Google Scholar] [CrossRef]
- Kelly, P.; Williamson, C.; Niven, A.G.; Hunter, R.; Mutrie, N.; Richards, J. Walking on sunshine: Scoping review of the evidence for walking and mental health. Br. J. Sports Med. 2018, 52, 800–806. [Google Scholar] [CrossRef] [Green Version]
- CDC. More People Walk to Better Health. Available online: https://www.cdc.gov/vitalsigns/walking/index.html (accessed on 11 October 2019).
- National Institute for Clinical Excellence. Physical Activity: Walking and Cycling. Available online: https://www.nice.org.uk/guidance/ph41 (accessed on 11 October 2019).
- CDC. FastStats: Exercise or Physical Activity. Available online: https://www.cdc.gov/nchs/fastats/exercise.htm (accessed on 11 October 2019).
- NHS Digital. Statistics on Obesity, Physical Activity and Diet, England, 2019. Part 5: Physical Activity. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/statistics-on-obesity-physical-activity-and-diet/statistics-on-obesity-physical-activity-and-diet-england-2019/part-5-adult-physical-activity (accessed on 10 October 2019).
- Hunter, R.; Ball, K.; Sarmiento, O.L. Socially awkward: How can we better promote walking as a social behaviour? Br. J. Sports Med. 2018, 52, 757–758. [Google Scholar] [CrossRef]
- Ball, K.; Bauman, A.; Leslie, E.; Owen, N. Perceived environmental aesthetics and convenience and company are associated with walking for exercise among Australian adults. Prev. Med. (Baltim). 2001, 33, 434. [Google Scholar] [CrossRef]
- Kassavou, A.; Turner, A.; French, D.P. Do interventions to promote walking in groups increase physical activity? A meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 18. [Google Scholar] [CrossRef] [Green Version]
- Gusi, N.; Reyes, M.C.; Gonzalez-Guerrero, J.L.; Herrera, E.; Garcia, J.M. Cost-utility of a walking programme for moderately depressed, obese, or overweight elderly women in primary care: A randomised controlled trial. BMC Public Health 2008, 8, 231. [Google Scholar] [CrossRef] [Green Version]
- Foster, C.; Kelly, P.; Reid, H.A.B.; Roberts, N.; Murtagh, E.M.; Humphreys, D.K.; Panter, J.; Milton, K. What works to promote walking at the population level? A systematic review. Br. J. Sports Med. 2018, 52, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Shanahan, D.F.; Astell–Burt, T.; Barber, E.A.; Brymer, E.; Cox, D.T.C.; Dean, J.; Depledge, M.; Fuller, R.A.; Hartig, T.; Irvine, K.N.; et al. Nature–Based Interventions for Improving Health and Wellbeing: The Purpose, the People and the Outcomes. Sports 2019, 7, 141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartig, T.; Mitchell, R.; de Vries, S.; Frumkin, H. Nature and health. Annu. Rev. Public Health 2014, 35, 207–228. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frumkin, H.; Bratman, G.N.; Breslow, S.J.; Cochran, B.; Kahn, P.H.J.; Lawler, J.J.; Levin, P.S.; Tandon, P.S.; Varanasi, U.; Wolf, K.L.; et al. Nature contact and human health: A research agenda. Environ. Health Perspect. 2017, 125, 075001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Urban Green Space Interventions and Health: A Review of Impacts and effectiveness. Available online: http://www.euro.who.int/__data/assets/pdf_file/0010/337690/FULL-REPORT-for-LLP.pdf?ua=1 (accessed on 11 October 2019).
- Bowler, D.E.; Buyung-Ali, L.; Knight, T.; Pullin, A.S. A systematic review of evidence for the added benefits to health of exposure to natural environments. BMC Public Health 2010, 10, 456. [Google Scholar] [CrossRef] [Green Version]
- Coon, J.T.; Boddy, K.; Stein, K.; Whear, R.; Barton, J.; Depledge, M.H. Does participating in physical activity in outdoor natural environments have a greater effect on physical and mental wellbeing than physical activity indoors? A systematic review. Environ. Sci. Technol. 2011, 45, 1761–1772. [Google Scholar] [CrossRef]
- Hanson, S.; Jones, A. Is there evidence that walking groups have health benefits? A systematic review and meta-analysis. Br. J. Sports Med. 2015, 49, 710–715. [Google Scholar] [CrossRef] [Green Version]
- France, J.; Sennett, J.; Jones, A.; Fordham, R.; Williams, J.; Burke, A.; Meierkord, A.; Khioe, R.F.S.; Suhrcke, M. Evaluation of Walking for Health. Final report to Macmillan and the Ramblers. Available online: https://www.walkingforhealth.org.uk/sites/default/files/Final Report_0.pdf (accessed on 11 October 2019).
- Roe, J.; Aspinall, P. The restorative benefits of walking in urban and rural settings in adults with good and poor mental health. Health Place 2011, 17, 103–113. [Google Scholar] [CrossRef]
- Mayer, F.S.; Frantz, C.M.; Bruehlman-Senecal, E.; Dolliver, K. Why Is Nature Beneficial? The Role of Connectedness to Nature. Environ. Behav. 2009, 41, 607. [Google Scholar] [CrossRef]
- Nisbet, E.K.; Zelenski, J.M. Underestimating nearby nature: Affective forecasting errors obscure the happy path to sustainability. Psychol. Sci. 2011, 22, 1101–1106. [Google Scholar] [CrossRef]
- Marselle, M.R.; Irvine, K.N.; Warber, S.L. Examining Group Walks in Nature and Multiple Aspects of Well-Being: A Large-Scale Study. Ecopsychology 2014, 6, 134–147. [Google Scholar]
- Peacock, J.; Hine, R.; Pretty, J. Got the Blues, Then Find Some Greenspace: The Mental Health Benefits of Green Exercise Activities and Green Care; MIND: London, UK, 2007. [Google Scholar]
- Marselle, M.R.; Irvine, K.N.; Warber, S.L. Walking for Well-Being: Are Group Walks in Certain Types of Natural Environments Better for Well-Being than Group Walks in Urban Environments? Int. J. Environ. Res. Public Health 2013, 10, 5603–5628. [Google Scholar] [CrossRef] [Green Version]
- Marselle, M.R.; Irvine, K.N.; Lorenzo-Arribas, A.; Warber, S.L. Moving beyond Green: Exploring the Relationship of Environment Type and Indicators of Perceived Environmental Quality on Emotional Well-Being following Group Walks. Int. J. Environ. Res. Public Health 2015, 12, 106. [Google Scholar] [CrossRef]
- Marselle, M.R.; Irvine, K.N.; Lorenzo-Arribas, A.; Warber, S.L. Does perceived restorativeness mediate the effects of perceived biodiversity and perceived naturalness on emotional well-being following group walks in nature? J. Environ. Psychol. 2016, 46, 217–232. [Google Scholar] [CrossRef]
- Paths for All. Walk Leader Training Manual; Paths for All: Stirling, UK, 2015. [Google Scholar]
- South, J.; Giuntoli, G.; Kinsella, K. An Evaluation of the Walking for Wellness Project and the Befriender Role. Available online: http://publications.naturalengland.org.uk/publication/4853061788893184 (accessed on 11 October 2019).
- Wensley, R.; Slade, A. Walking as a meaningful leisure occupation: The implications for occupational therapy. Br. J. Occup. Ther. 2012, 75, 85–92. [Google Scholar] [CrossRef] [Green Version]
- Irvine, K.N.; Warber, S.L.; Devine-Wright, P.; Gaston, K.J. Understanding urban green space as a health resource: A qualitative comparison of visit motivation and derived effects among park users in Sheffield, UK. Int. J. Environ. Res. Public Health 2013, 10, 417–442. [Google Scholar] [CrossRef]
- Duffy, J.; Colon, A. Best Fitness Trackers of 2019. Available online: http://in.pcmag.com/activity-trackers/39350/guide/the-best-fitness-trackers-of-2017 (accessed on 11 October 2019).
- Abedtash, H.; Holden, R.J. Systematic review of the effectiveness of health-related behavioral interventions using portable activity sensing devices (PASDs). J. Am. Med. Inform. Assoc. 2017, 24, 1002–1013. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Definition of Health. Available online: http://www.who.int/suggestions/faq/en/ (accessed on 11 October 2019).
- Linton, M.-J.; Dieppe, P.; Medina-Lara, A. Review of 99 self-report measures for assessing wellbeing in adults: Exploring dimensions of well-being and developments over time. BMJ Open 2016, 6, e010641. [Google Scholar] [CrossRef]
- Irvine, K.N.; Warber, S.L. Greening healthcare: Practicing as if the natural environment really mattered. Altern. Ther. Health Med. 2002, 8, 76–83. [Google Scholar]
- Engel, G.L. The need for a new medical model: A challenge for biomedicine. Science (80-) 1977, 196, 129–136. [Google Scholar] [CrossRef]
- Fava, G.A.; Sonino, N. The biopsychosocial model thirty years later. Psychother. Psychosom. 2008, 77, 1–2. [Google Scholar] [CrossRef]
- McKee, D.D.; Chappel, J.N. Spirituality and medical practice. J. Fam. Pract. 1992, 35, 205–208. [Google Scholar]
- Andrews, F.; McKennell, A. Measures of self-reported wellbeing: Their affective, cognitive, and other components. Soc. Indic. Res. 1980, 8, 127–155. [Google Scholar] [CrossRef]
- Bann, C.M.; Kobau, R.; Lewis, M.A.; Zack, M.M.; Luncheon, C.; Thompson, W.W. Development and psychometric evaluation of the public health surveillance well-being scale. Qual. Life Res. 2012, 21, 1031–1043. [Google Scholar] [CrossRef]
- Mezzich, J.E.; Cohen, N.L.; Ruiperez, M.A.; Banzato, C.E.; Zapata-Vega, M.I. The Multicultural Quality of Life Index: Presentation and validation. J. Eval. Clin. Pract. 2011, 17, 357–364. [Google Scholar] [CrossRef]
- Ventegodt, S.; Merrick, J.; Andersen, N.J. Measurement of quality of life III. From the IQOL theory to the global, generic SEQOL questionnaire. Sci. World J. 2003, 3, 972–991. [Google Scholar] [CrossRef]
- Ritenbaugh, C.; Nichter, M.; Nichter, M.A.; Kelly, K.L.; Sims, C.M.; Bell, I.R.; Castañeda, H.M.; Elder, C.R.; Koithan, M.S.; Sutherland, E.G.; et al. Developing a patient-centered outcome measure for complementary and alternative medicine therapies I: Defining content and format. BMC Complement. Altern. Med. 2011, 11, 135. [Google Scholar] [CrossRef] [Green Version]
- Thompson, J.J.; Kelly, K.L.; Ritenbaugh, C.; Hopkins, A.L.; Sims, C.M.; Coons, S.J. Developing a patient-centered outcome measure for complementary and alternative medicine therapies II: Refining content validity through cognitive interviews. BMC Complement. Altern. Med. 2011, 11, 136. [Google Scholar] [CrossRef] [Green Version]
- Lillehei, A.S.; Halcón, L.; Gross, C.R.; Savik, K.; Reis, R. Well-Being and Self-Assessment of Change: Secondary Analysis of an RCT That Demonstrated Benefit of Inhaled Lavender and Sleep Hygiene in College Students with Sleep Problems. Explore 2016, 12, 427–435. [Google Scholar] [CrossRef]
- Williams, M. Feasibility and Pilot Studies: A Guide for NIHR Research Design Service Advisors. 2016. Available online: https://www.rds-eastmidlands.nihr.ac.uk/resources/Guide%20to%20Supporting%20Feasibility%20and%20Pilot%20Studies%20MAY%202016%20FIANAL.pdf (accessed on 21 February 2020).
- Orsmond, G.I.; Cohn, E.S. The distinctive features of a feasibility study: Objectives and guiding questions. OTJR: Occup. Particip. Health 2015, 35, 169–177. [Google Scholar] [CrossRef]
- Tickle-Degnen, L. Nuts and bolts of conducting feasibility studies. Amer. J. Occup. Ther. 2013, 67, 171–176. [Google Scholar] [CrossRef] [Green Version]
- Cresswell, J.W.; Plano Clark, V. Designing and Conducting Mixed Methods Research, 3rd ed.; Sage Publications: Thousand Oaks, CA, USA, 2018. [Google Scholar]
- Yuan, S.; Humphris, G.; Ross, A.; MacPherson, L.; Zhou, Y.; Freeman, R. A mixed-methods feasibility study protocol to assess the communication behaviours within the dental health professional-parent-child triad in a general dental practice setting. Pilot Feasibility Stud. 2018, 4, 136. [Google Scholar] [CrossRef]
- O’Driscoll, M.; Byrne, S.; Bryne, H.; Lambert, S.; Sahm, L.J. An online mindfulness-based intervention for undergraduate pharmacy students: Results of a mixed-methods feasibility study. Curr. Pharm. Teach. Learn. 2019, 11, 858–875. [Google Scholar] [CrossRef]
- Salkind, N.J. (Ed.) Encyclopedia of Research Design; Sage Publications: Thousand Oaks, CA, USA, 2010; Volume 1. [Google Scholar]
- Colley, K.; Currie, M.; Hopkins, J.; Melo, P. Access to Outdoor Recreation by older People in SCOTLAND. Available online: https://www.gov.scot/publications/access-outdoor-recreation-older-people-scotland/pages/1/ (accessed on 11 October 2019).
- Cairngorms National Park Authority. Management Plans: Cairngorms National Park Partnership Plan 2017–2022; Cairngorms National Park Authority: Grantown-on-Spey, UK, 2017; ISBN 978-1-906071-87-5. [Google Scholar]
- Mutrie, N.; Fitzsimons, C.; Jackson, F.; Scobie, G. Validation of a Physical Activity Validation Report (Scot-PASQ). Available online: http://www.paha.org.uk/Resource/scottish-physcial-activity-screening-validation-report-scot-pasq (accessed on 11 October 2019).
- Department of Health and Social Care. UK Chief Medical Officers’ Physical Activity Guidelines. Available online: https://www.gov.uk/government/publications/physical-activity-guidelines-uk-chief-medical-officers-report (accessed on 11 October 2019).
- Husk, K.; Blockley, K.; Lovell, R.; Bethel, A.; Bloomfield, D.; Warber, S.; Pearson, M.; Lang, I.; Byng, R.; Garside, R. What approaches to social prescribing work, for whom, and in what circumstances? A protocol for a realist review. Syst. Rev. 2016, 5, 93. [Google Scholar] [CrossRef] [Green Version]
- Husk, K.; Blockley, K.; Lovell, R.; Bethel, A.; Lang, I.; Byng, R.; Garside, R. What approaches to social prescribing work, for whom, and in what circumstances? A realist review. Health Soc. Care Community 2019, 28, 309–324. [Google Scholar] [CrossRef] [Green Version]
- Tocci, F.L.; Morey, M.C.; Caves, K.M.; Deberry, J.; Leahy, G.D.; Hall, K. Are Older Adults Ready for Wireless Physical Activity Tracking Devices? A Comparison of Commonly Used Tracking Devices. J. Am. Geriatr. Soc. 2016, 64, 226–228. [Google Scholar] [CrossRef]
- Duvall, J. Enhancing the benefits of outdoor walking with cognitive engagement strategies. J. Environ. Psychol. 2010, 31, 27–35. [Google Scholar] [CrossRef]
- Prince, S.; Adamo, K.; Hamel, M.; Hardt, J.; Gorber, S.; Tremblay, M. A comparison of direct versus self-report measures for assessing physical activity in adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 56. [Google Scholar] [CrossRef] [Green Version]
- Harris, T.J.; Owen, C.G.; Victor, C.R.; Adams, R.; Ekelund, U.; Cook, D.G. A Comparison of Questionnaire, Accelerometer, and Pedometer: Measures in Older People. Med. Sci. Sport Exerc. 2009, 41, 1392–1402. [Google Scholar] [CrossRef]
- An, H.S.; Jones, G.C.; Kang, S.K.; Welk, G.J.; Lee, J.M. How valid are wearable physical activity trackers for measuring steps? Eur. J. Sport Sci. 2017, 17, 360–368. [Google Scholar] [CrossRef]
- Diaz, K.M.; Krupka, D.J.; Chang, M.J.; Shaffer, J.A.; Ma, Y.; Goldsmith, J.; Schwartz, J.E.; Davidson, K.W. Validation of the Fitbit One® for physical activity measurement at an upper torso attachment site. BMC Res. Notes 2016, 9, 213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alley, S.; Schoeppe, S.; Guertler, D.; Jennings, C.; Duncan, M.J.; Vandelanotte, C. Interest and preferences for using advanced physical activity tracking devices: Results of a national cross-sectional survey. BMJ Open 2016, 6, e011243. [Google Scholar] [CrossRef] [Green Version]
- Warber, S.L.; DeHudy, A.A.; Bialko, M.F.; Marselle, M.R.; Irvine, K.N. Addressing “Nature-Deficit Disorder”: A Mixed Methods Pilot Study of Young Adults Attending a Wilderness Camp. Evidence-Based Complement. Altern. Med. 2015, 2015, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ. 2008, 337, a1655. [Google Scholar] [CrossRef] [Green Version]
- Paradies, Y.; Stevens, M. Conceptual diagrams in public health research. J. Epidemiol. Community Health. 2005, 59, 1012–1013. [Google Scholar] [CrossRef] [Green Version]
- Kaplan, S. The restorative benefits of nature: Toward an integrative framework. J. Environ. Psychol. 1995, 15, 169–182. [Google Scholar] [CrossRef]
- Ulrich, R.S.; Simons, R.F.; Losito, B.D.; Fiorito, E.; Miles, M.A.; Zelson, M. Stress recovery during exposure to natural and urban environments. J. Environ. Psychol. 1991, 11, 201–230. [Google Scholar] [CrossRef]
- Yeh, H.-P.; Stone, J.A.; Churchill, S.M.; Wheat, J.S.; Brymer, E.; David, K. Physical, Psychological and Emotional Benefits of Green Physical Activity: An Ecological Dynamics Perspective. Sport. Med. 2015, 46, 947–953. [Google Scholar] [CrossRef] [Green Version]
- Shanahan, D.F.; Bush, R.; Gaston, K.J.; Lin, B.B.; Dean, J.; Barber, E.; Fuller, R.A. Health benefits of nature experiences depend on dose. Sci. Rep. 2016, 6, 28551. [Google Scholar] [CrossRef] [Green Version]
- Irvine, K.N.; Hoesly, D.; Bell-Williams, R.; Warber, S.L. Spiritual wellbeing and biodiversity. In Biodiversity and Health in the Face of Climate Change; Marselle, M.R., Stadler, J., Korn, H., Irvine, K.N., Bonn, A., Eds.; Springer: Berlin/Heidelberg, Germany, 2019. [Google Scholar]
- Local Government Association. Just What the Doctor Ordered. Social Prescribing–A Guide for Local Authorities. Available online: https://www.local.gov.uk/sites/default/files/documents/just-what-doctor-ordered--5c4.pdf (accessed on 11 October 2019).




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Health and Wellbeing VAS Anchoring Word Pairs | Before Mean (SD) | Now Mean (SD) | |
|---|---|---|---|
| Not sleeping well | Sleeping well | 55.25 (30.82) | 68.08 (30.21) 1 |
| Exhausted | Energised | 54.50 (25.00) | 71.67 (27.13) 1 |
| Dull senses | Vibrant senses | 61.45 (23.26) | 73.82 (21.96) 1 |
| Body does not recover quickly | Body recovers quickly | 76.00 (23.23) | 80.00 (22.85) |
| Scattered | Focused | 63.17 (30.35) | 74.17 (27.13) 1 |
| Stuck | Letting go | 64.58 (28.19) | 68.83 (29.39) |
| Defined by my illness or problems | Not defined by my illness or problems | 65.25 (29.46) | 69.50 (31.04) |
| Hopeless | Hopeful | 70.67 (23.62) | 79.08 (15.84) |
| Depressed | Joyful | 68.25 (26.34) | 78.50 (21.85) 1 |
| Anxious | Calm | 62.25 (30.51) | 72.58 (26.53) 1 |
| Closed to others | Open to others | 77.50 (17.26) | 81.17 (16.35) |
| Isolated | Connected | 68.92 (27.21) | 77.58 (22.35) |
| Blaming | Forgiving | 70.75 (18.90) | 74.08 (19.15) |
| Overwhelmed | Empowered | 64.25 (24.80) | 72.67 (19.96) |
| Broken | Whole | 70.50 (26.88) | 81.25 (18.90) 1 |
| Unbalanced | Balanced | 71.92 (24.96) | 79.58 (19.34) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Irvine, K.N.; Marselle, M.R.; Melrose, A.; Warber, S.L. Group Outdoor Health Walks Using Activity Trackers: Measurement and Implementation Insight from a Mixed Methods Feasibility Study. Int. J. Environ. Res. Public Health 2020, 17, 2515. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072515
Irvine KN, Marselle MR, Melrose A, Warber SL. Group Outdoor Health Walks Using Activity Trackers: Measurement and Implementation Insight from a Mixed Methods Feasibility Study. International Journal of Environmental Research and Public Health. 2020; 17(7):2515. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072515
Chicago/Turabian StyleIrvine, Katherine N., Melissa R. Marselle, Alan Melrose, and Sara L. Warber. 2020. "Group Outdoor Health Walks Using Activity Trackers: Measurement and Implementation Insight from a Mixed Methods Feasibility Study" International Journal of Environmental Research and Public Health 17, no. 7: 2515. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17072515