Measures to Promote Rural Healthcare Tourism with a Scientific Evidence-Based Approach

 ,
,  , , and
, , and 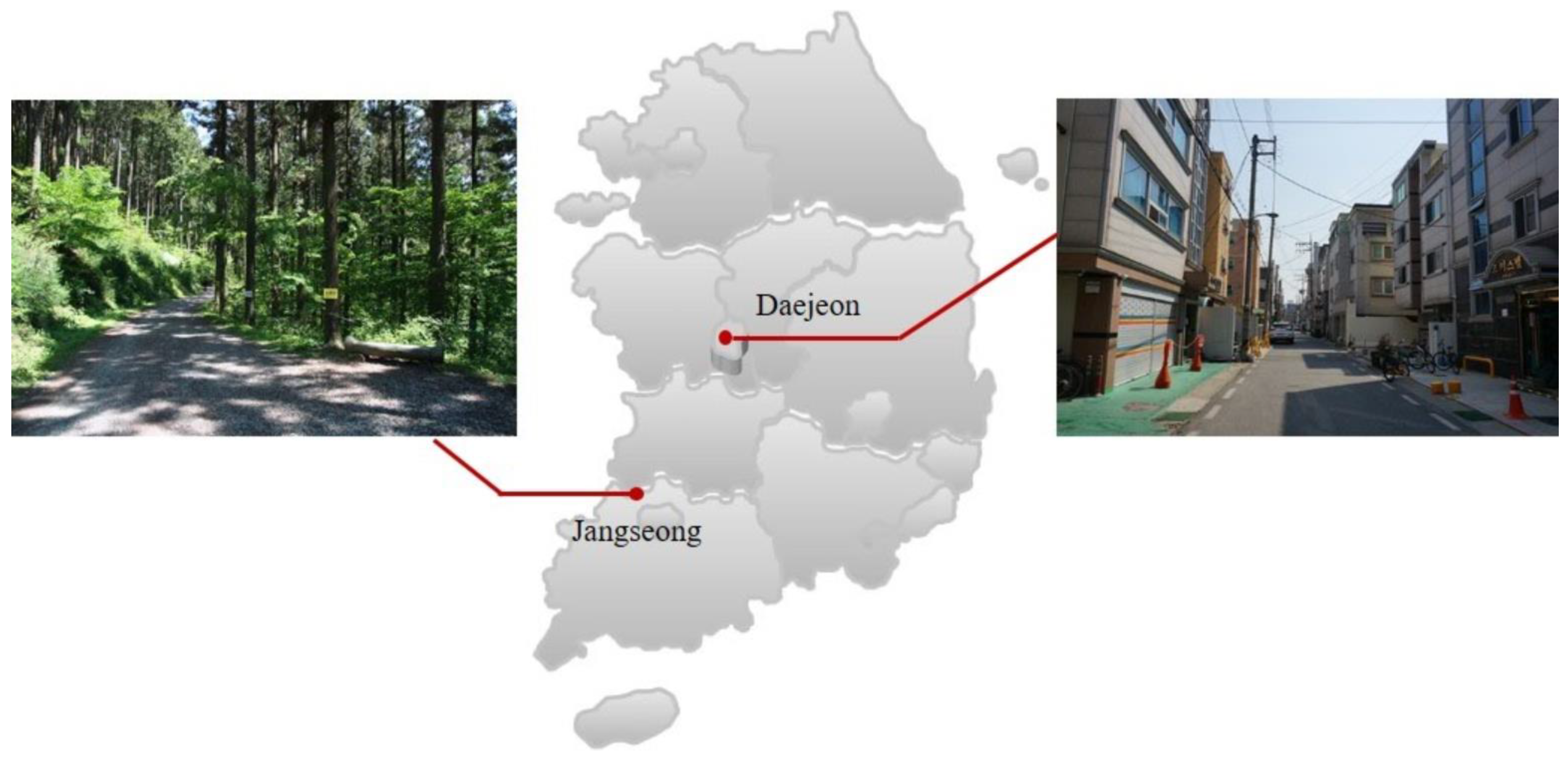{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
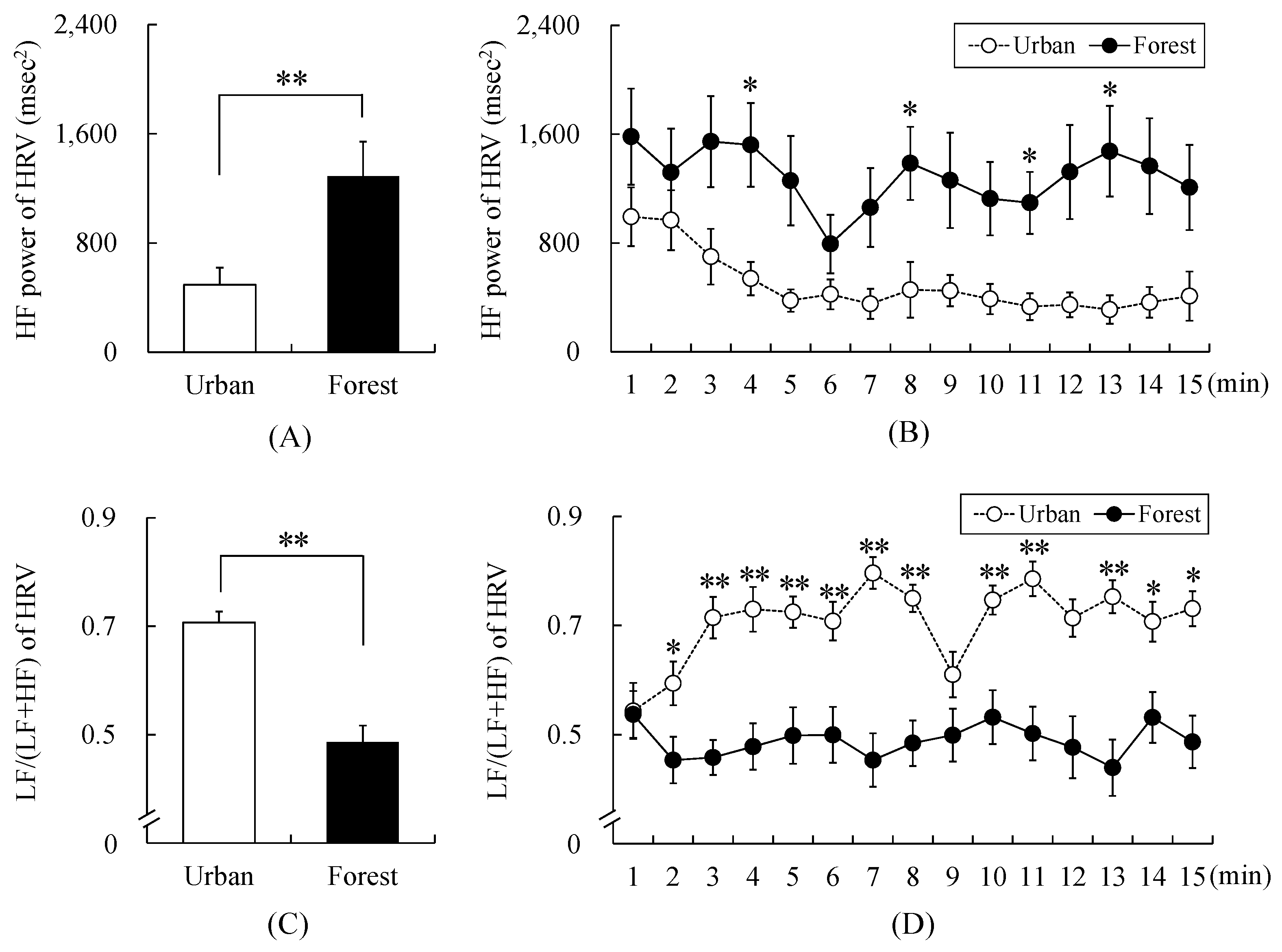
- Short-term walking in the forest in rural areas will increase parasympathetic nervous activity.
- Short-term walking in the forest in rural areas will decrease sympathetic nervous activity.
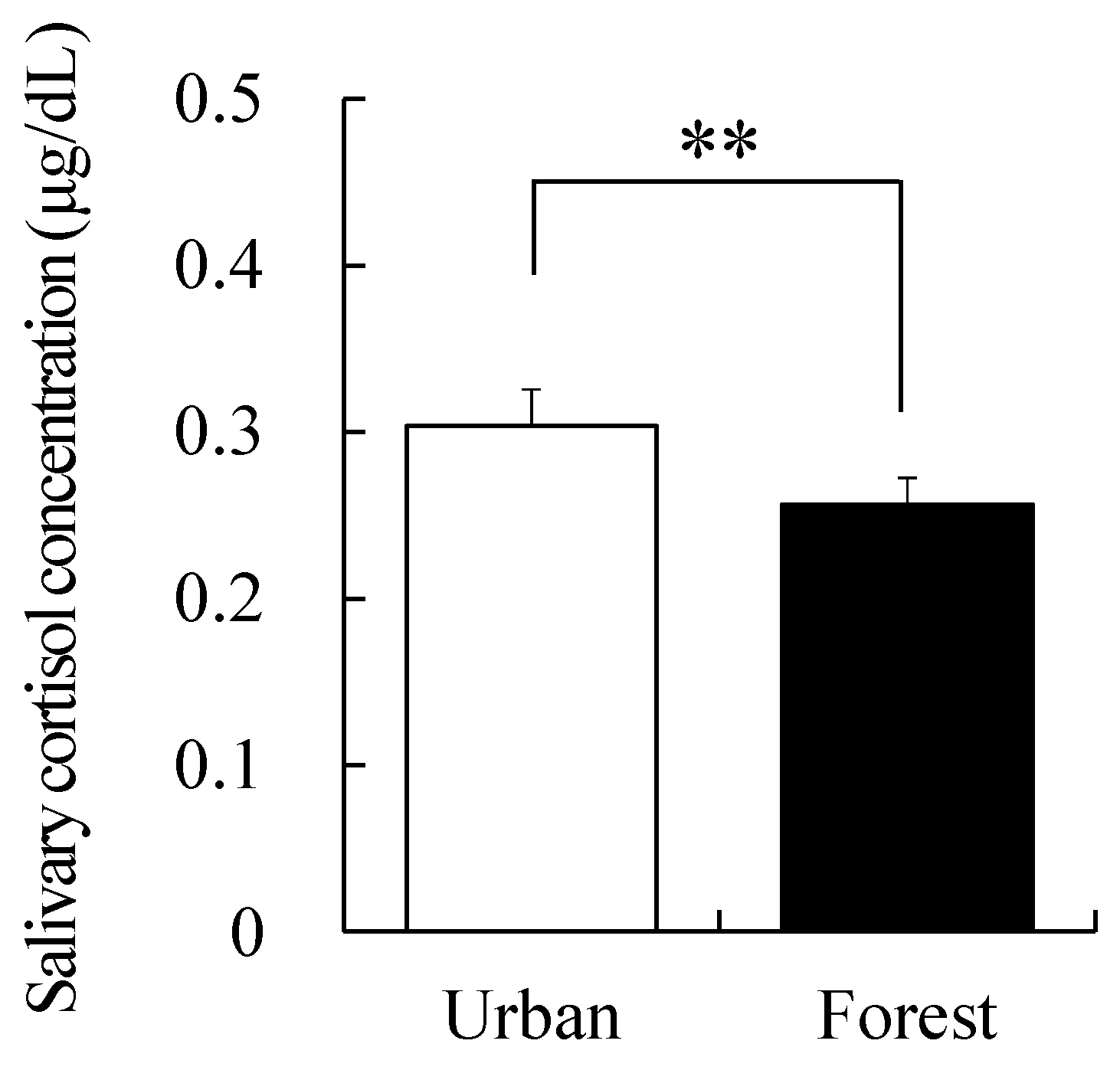
- Short-term walking in the forest in rural areas will reduce salivary cortisol levels.
- Short-term walking in the forest in rural areas will reduce negative emotions (i.e., anxiety, depression, anger, fatigue, and confusion).
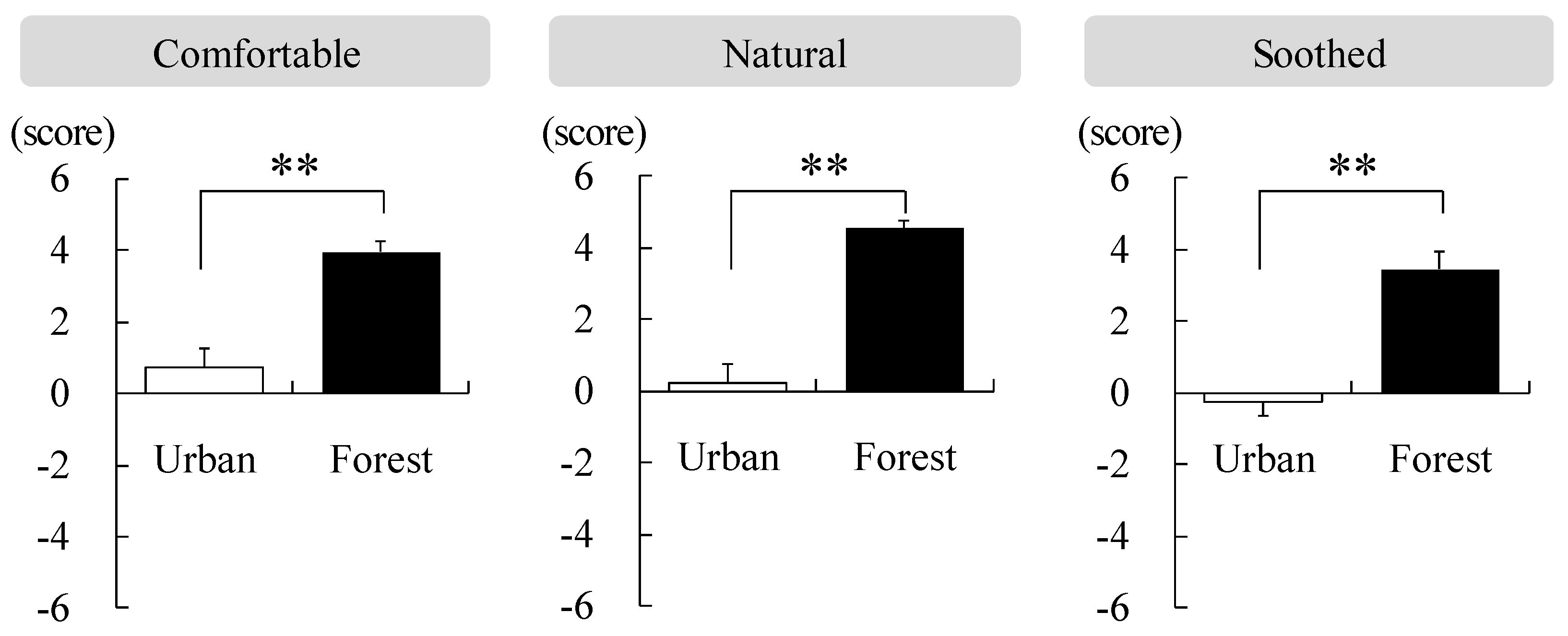
- Short-term walking in the forest in rural areas will make one feel more comfortable, natural, and relaxed.
2. Materials and Methods
2.1. Participants
2.2. Study Area
2.3. Physiological Markers
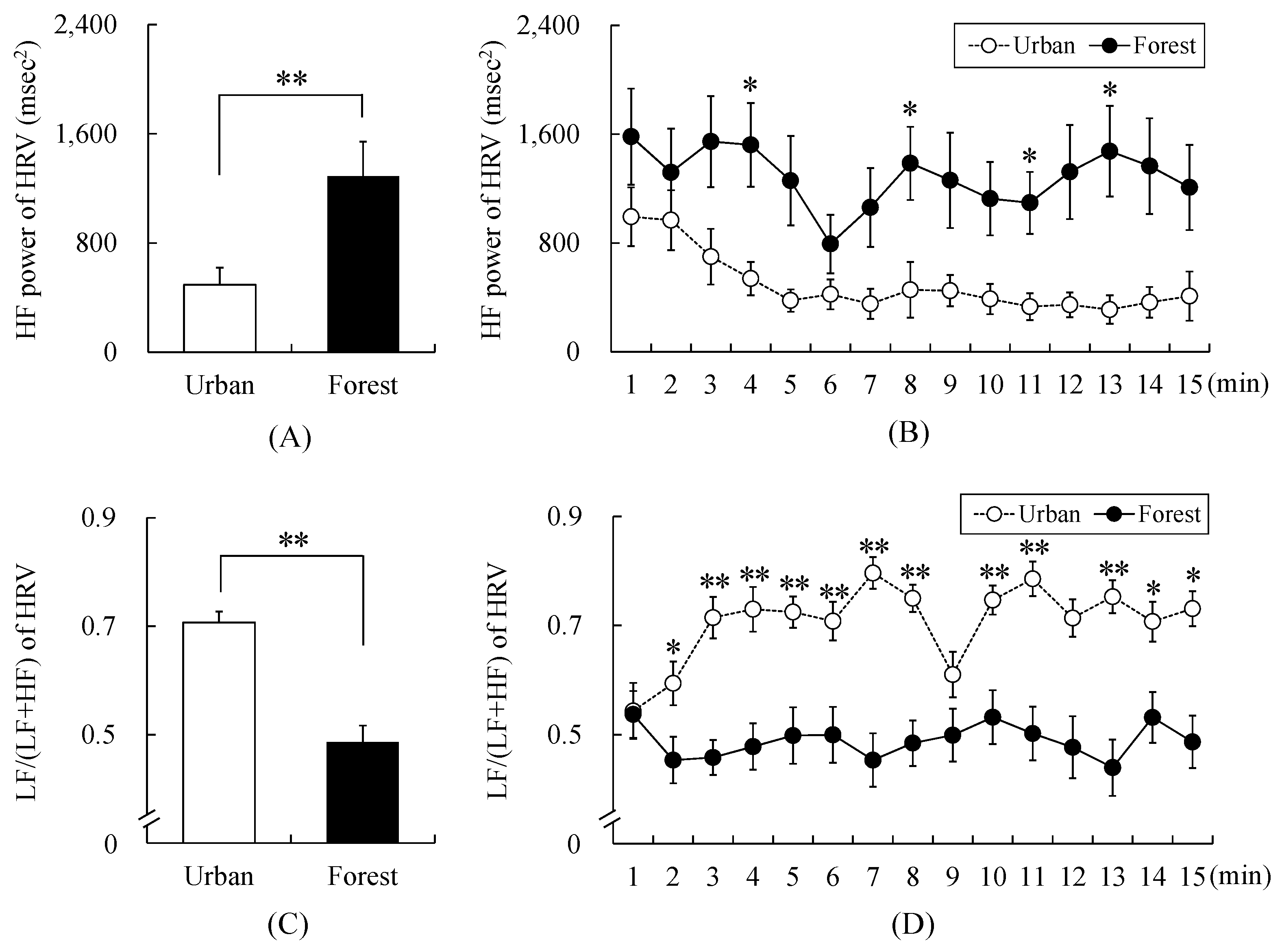
2.3.1. Heart Rate Variability (HRV)
2.3.2. Salivary Cortisol Concentration
2.4. Questionnaires
2.4.1. Semantic Differential (SD) Method
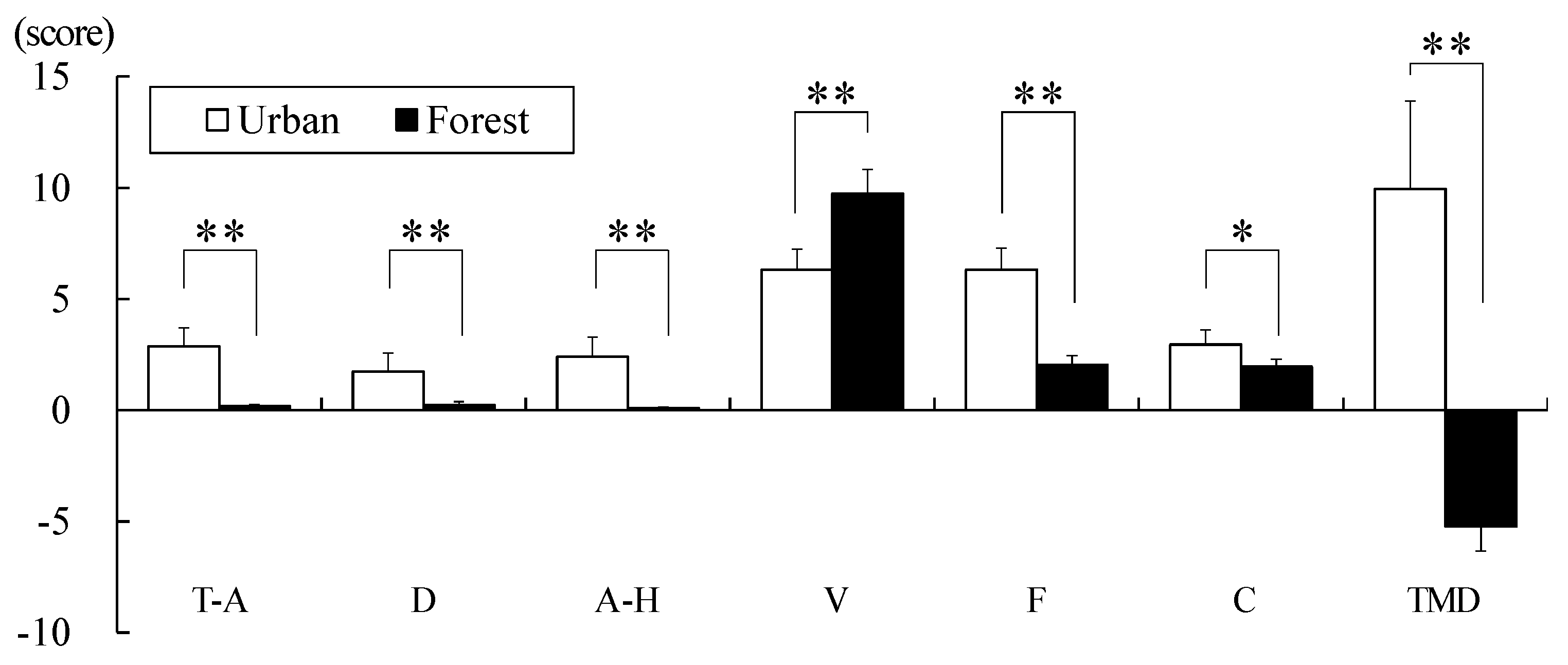
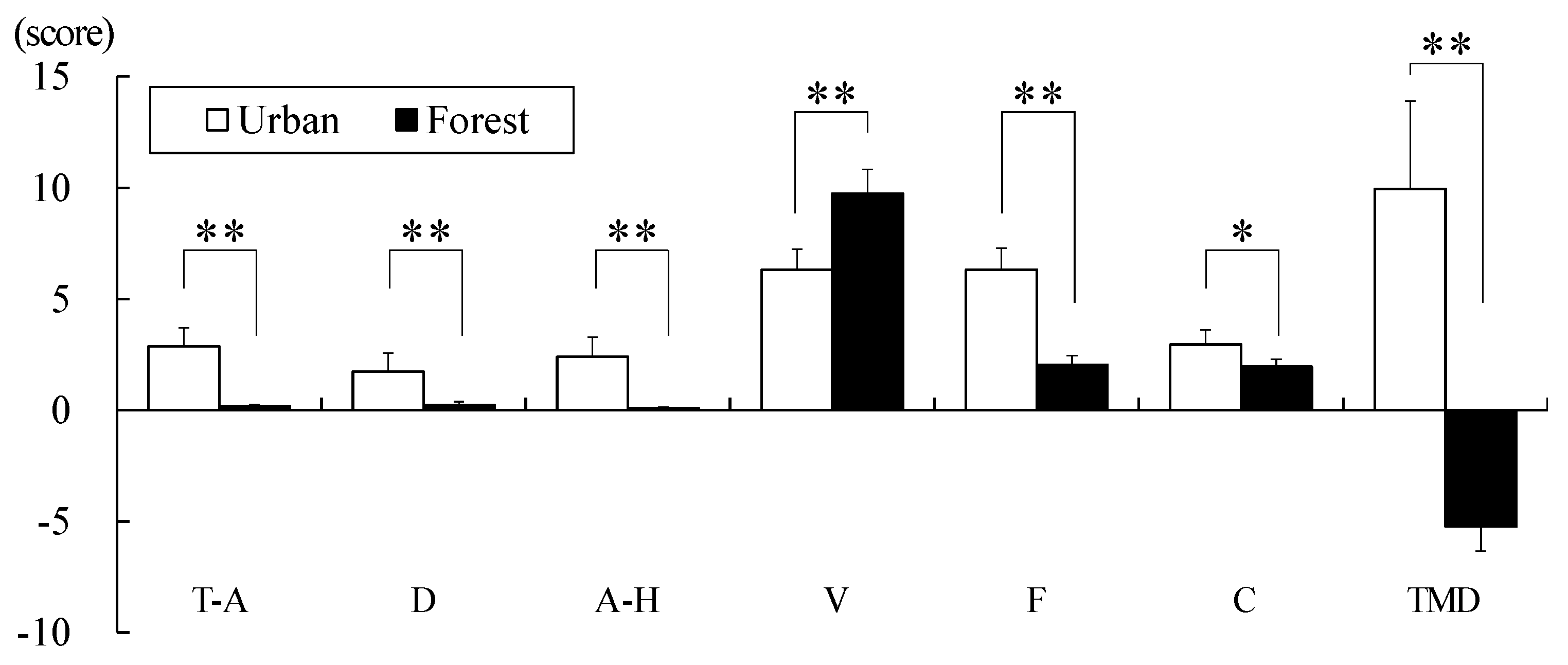
2.4.2. Profile of Mood State
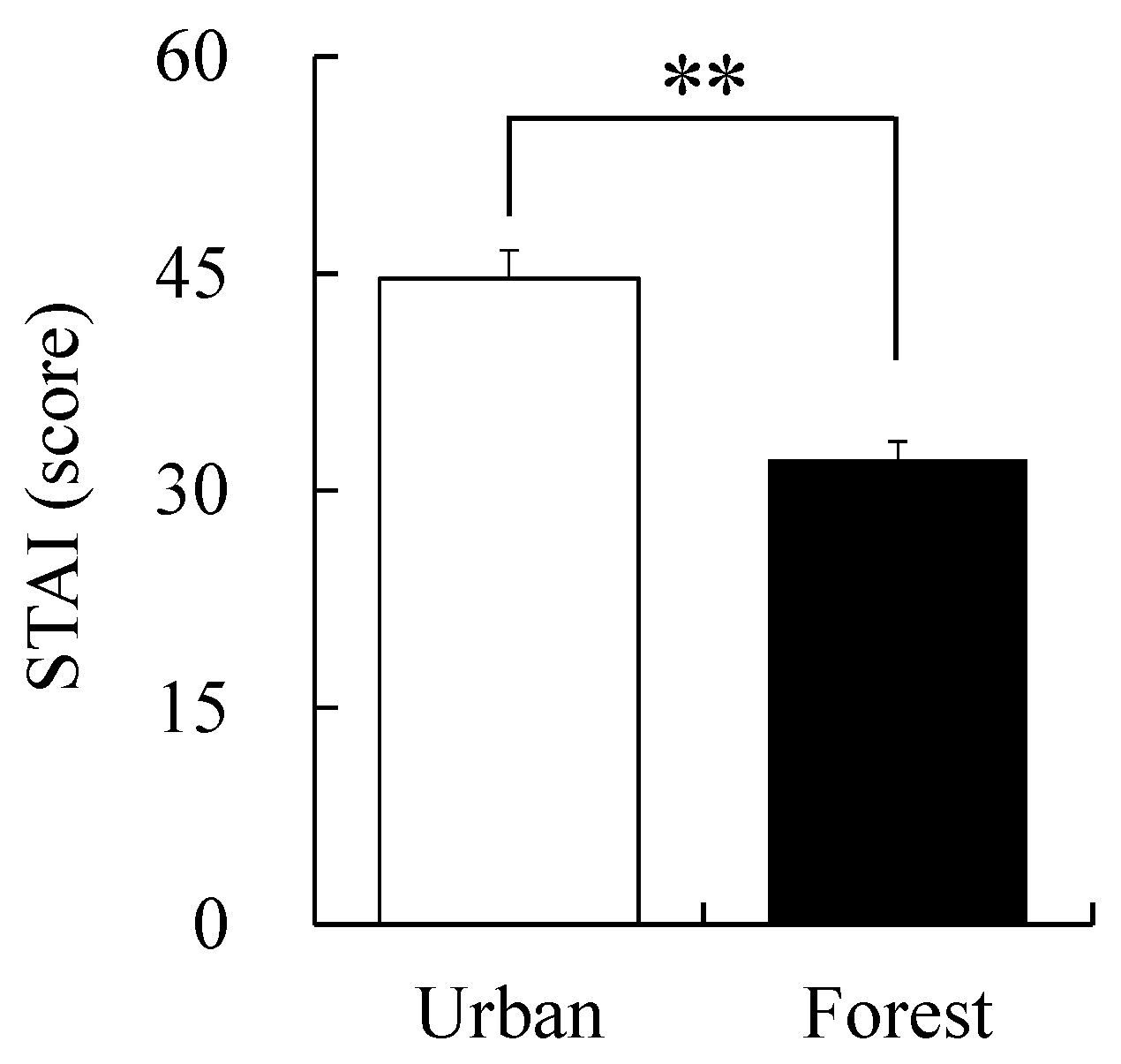
2.4.3. State-Trait Anxiety Inventory (STAI-X)
2.5. Procedure
2.6. Data Analysis
3. Results
3.1. Physiological Markers
3.2. Questionnaires
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Khan, M.H. Governance, Economic Growth and Development since the 1960s; UN DESA Working Paper No. 54; DESA: New York, NY, USA, 2007. [Google Scholar]
- Kim, I.K.; Liang, J.; Rhee, K.O.; Kim, C.S. Population aging in Korea: Changes since the 1960s. J. Cross Cult. Gerontol. 1996, 11, 369–388. [Google Scholar] [CrossRef] [PubMed]
- Statistics Korea. 2015 Agriculture, Forestry & Fishery Census Report Rural Community; No. 1; Statistics Korea: Daejeon, Korea, 2016; Volume 3, pp. 1–872. [Google Scholar]
- Park, S. Analysis of Saemaul Undong: A Korean rural development programme in the 1970s. Asia-Pac. Dev. J. 2012, 16, 113–140. [Google Scholar] [CrossRef]
- Morredu, C. Review of Agricultural Policies in Korea; OECD: Paris, France, 1999; pp. 29–42. [Google Scholar]
- Fleischer, A.; Felsenstein, D. Support for rural tourism: Does it make a difference? Ann. Touris. Res. 2000, 27, 1007–1024. [Google Scholar] [CrossRef]
- Sharpley, R.; Sharpley, J. Rural Tourism: An Introduction; International Thomson Business Press: London, UK, 1997; pp. 1–165. [Google Scholar]
- MacDonald, R.; Jolliffe, L. Cultural rural tourism: Evidence from Canada. Ann. Touris. Res. 2003, 30, 307–322. [Google Scholar] [CrossRef]
- Kang, H.M.; Kim, H.; Lee, C.H.; Lee, C.K.; Im Choi, S. Changes and development plan in the mountain villages of South Korea: Comparison of the first and second national survey. J. Mt. Sci. 2017, 14, 1473–1489. [Google Scholar] [CrossRef]
- Korea Legislation Research Institute. Available online: https://elaw.klri.re.kr/kor_service/lawView.do?hseq=46871&lang=ENG (accessed on 12 April 2020).
- Shin, W.S.; Kim, J.J.; Lim, S.S.; Yoo, R.H.; Jeong, M.A.; Lee, J.; Park, S. Paradigm shift on forest utilization: Forest service for health promotion in the Republic of Korea. Net. J. Agric. Sci. 2017, 5, 53–57. [Google Scholar] [CrossRef] [Green Version]
- Park, B.J.; Tsunetsugu, Y.; Kasetani, T.; Kagawa, T.; Miyazaki, Y. The physiological effects of Shinrin-yoku (taking in the forest atmosphere or forest bathing): Evidence from field experiments in 24 forests across Japan. Environ. Health Prev. Med. 2010, 15, 18–26. [Google Scholar] [CrossRef] [Green Version]
- Song, C.; Ikei, H.; Kagawa, T.; Miyazaki, Y. Effects of walking in a forest on young women. Int. J. Environ. Res. Public Health 2019, 16, 229. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Tsunetsugu, Y.; Takayama, N.; Park, B.J.; Li, Q.; Song, C.; Komatsu, M.; Ikei, H.; Tyrväinen, L.; Kagawa, T.; et al. Influence of forest therapy on cardiovascular relaxation in young adults. Evid. Based Complement. Alternat. Med. 2014, 2014, 834360. [Google Scholar] [CrossRef]
- Park, B.J.; Tsunetsugu, Y.; Kasetani, T.; Hirano, H.; Kagawa, T.; Sato, M.; Miyazaki, Y. Physiological effects of Shinrin-Yoku (taking in the atmosphere of the forest)–using salivary cortisol and cerebral activity as indicators. J. Physiol. Anthropol. 2007, 26, 123–128. [Google Scholar] [CrossRef] [Green Version]
- Joung, D.; Kim, G.; Choi, Y.; Lim, H.; Park, S.; Woo, J.M.; Park, B.J. The prefrontal cortex activity and psychological effects of viewing forest landscapes in autumn season. Int. J. Environ. Res. Public Health 2015, 12, 7235–7243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sung, J.; Woo, J.M.; Kim, W.; Lim, S.K.; Chung, E.J. The effect of cognitive behavior therapy-based “forest therapy” program on blood pressure, salivary cortisol level, and quality of life in elderly hypertensive patients. Clin. Exp. Hypertens. 2012, 34, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Tsao, T.M.; Tsai, M.J.; Hwang, J.S.; Cheng, W.F.; Wu, C.F.; Chou, C.C.; Su, T.C. Health effects of a forest environment on natural killer cells in humans: An observational pilot study. Oncotarget 2018, 9, 16501–16511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Q.; Morimoto, K.; Nakadai, A.; Inagaki, H.; Katsumata, M.; Shimizu, T.; Hirata, Y.; Hirata, K.; Suzuki, H.; Miyazaki, Y.; et al. Forest bathing enhances human natural killer activity and expression of anti-cancer proteins. Int. J. Immunopathol. Pharmacol. 2007, 20, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Morimoto, K.; Kobayashi, M.; Inagaki, H.; Katsumata, M.; Hirata, Y.; Hirata, K.; Suzuki, H.; Li, Y.J.; Wakayama, Y.; et al. Visiting a forest, but not a city, increases human natural killer activity and expression of anti-cancer proteins. Int. J. Immunopathol. Pharmacol. 2008, 21, 117–127. [Google Scholar] [CrossRef] [PubMed]
- Li, Q. Effect of forest bathing trips on human immune function. Environ. Health Prev. Med. 2010, 15, 9–17. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.T.; Yu, C.P.; Lee, H.Y. The effects of forest bathing on stress recovery: Evidence from middle-aged females of taiwan. Forests 2018, 9, 403. [Google Scholar] [CrossRef] [Green Version]
- Song, C.; Ikei, H.; Park, B.J.; Lee, J.; Kagawa, T.; Miyazaki, Y. Psychological benefits of walking through forest areas. Int. J. Environ. Res. Public Health 2018, 15, 2804. [Google Scholar] [CrossRef] [Green Version]
- Bielinis, E.; Takayama, N.; Boiko, S.; Omelan, A.; Bielinis, L. The effect of winter forest bathing on psychological relaxation of young Polish adults. Urban For. Urban Green. 2018, 29, 276–283. [Google Scholar] [CrossRef]
- Li, Q. What is forest medicine? In Forest Medicine; Li, Q., Ed.; Nova Science Publishers: New York, NY, USA, 2012; pp. 1–8. [Google Scholar]
- Tsunetsugu, Y.; Park, B.J.; Miyazaki, Y. Trends in research related to “Shinrin-yoku” (taking in the forest atmosphere or forest bathing) in Japan. Environ. Health Prev. 2010, 15, 27. [Google Scholar] [CrossRef] [Green Version]
- Sumitomo, K.; Akutsu, H.; Fukuyama, S.; Minoshima, A.; Kukita, S.; Yamamura, Y.; Sato, Y.; Hayasaka, T.; Osanai, S.; Funakoshi, H.; et al. Conifer-derived monoterpenes and forest walking. Mass Spectrom. 2015, 4, A0042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ikei, H.; Song, C.; Miyazaki, Y. Effects of olfactory stimulation by α-pinene on autonomic nervous activity. J. Wood Sci. 2016, 62, 568–572. [Google Scholar] [CrossRef]
- Joung, D.; Song, C.; Ikei, H.; Okuda, T.; Igarashi, M.; Koizumi, H.; Park, B.J.; Yamaguchi, T.; Takagaki, M.; Miyazaki, Y. Physiological and psychological effects of olfactory stimulation with D-limonene. Adv. Hort. Sci. 2014, 28, 90–94. [Google Scholar]
- Ohira, T.; Matsui, N. Phytoncides in forest atmosphere. In Forest Medicine; Li, Q., Ed.; Nova Science Publishers: New York, NY, USA, 2012; pp. 25–34. [Google Scholar]
- Ikei, H.; Song, C.; Miyazaki, Y. Physiological effect of olfactory stimulation by Hinoki cypress (Chamaecyparis obtusa) leaf oil. J. Physiol. Anthropol. 2015, 34, 44. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Kobayashi, M.; Wakayama, Y.; Inagaki, H.; Katsumata, M.; Hirata, Y.; Hirata, K.; Shimizu, T.; Kawada, T.; Park, B.J. Effect of phytoncide from trees on human natural killer cell function. Int. J. Immunopathol. Pharmacol. 2009, 22, 951–959. [Google Scholar] [CrossRef]
- Hong, E.J.; Na, K.J.; Choi, I.G.; Choi, K.C.; Jeung, E.B. Antibacterial and antifungal effects of essential oils from coniferous trees. Biol. Pharm. Bull. 2004, 27, 863–866. [Google Scholar] [CrossRef] [Green Version]
- Korea Forest Service. 2018 Statistical Yearbook of Forestry; Korea Forest Service: Daejeon, Korea, 2018; p. 444. [Google Scholar]
- Bramwell, B.; Lane, B. Sustainable tourism: An evolving global approach. J. Sustain. Tour. 1993, 1, 1–5. [Google Scholar] [CrossRef]
- Simpson, M.E.; Serdula, M.; Galuska, D.A.; Gillespie, C.; Donehoo, R.; Macera, C.; Mack, K. Walking trends among US adults: The behavioral risk factor surveillance system, 1987–2000. Am. J. Prev. Med. 2003, 25, 95–100. [Google Scholar] [CrossRef]
- Hillsdon, M.; Thorogood, M.; Anstiss, T.; Morris, J. Randomised controlled trials of physical activity promotion in free living populations: A review. J. Epidemiol. Commun. Health 1995, 49, 448–453. [Google Scholar] [CrossRef] [Green Version]
- Pons-Villanueva, J.; Seguí-Gómez, M.; Martínez-González, M.A. Risk of injury according to participation in specific physical activities: A 6-year follow-up of 14 356 participants of the SUN cohort. Int. J. Epidemiol. 2010, 39, 580–587. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Global Recommendations on Physical Activity for Health; WHO Press: Geneva, Switzerland, 2010; pp. 1–58. [Google Scholar]
- Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, H.; Ishibashi, K.; Noguchi, H. Heart rate variability; an index for monitoring and analyzing human autonomic activities. Appl. Hum. Sci. 1999, 18, 53–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, M.L.; Clark, K.G.; Shi, X. Manual medicine and the autonomic nervous system: Assessing autonomic function in humans. In The Science and Clinical Application of Manual Therapy, 1st ed.; King, H.H., Jänig, W., Patterson, M.M., Eds.; Churchill Livingstone Elsevier: Edinburgh, UK, 2010; pp. 85–92. [Google Scholar]
- Burr, R.L. Interpretation of normalized spectral heart rate variability indices in sleep research: A critical review. SLEEP 2007, 30, 913–919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirschbaum, C.; Hellhammer, D.H. Salivary cortisol in psychoneuroendocrine research: Recent developments and applications. Psychoneuroendocrinology 1994, 19, 313–333. [Google Scholar] [CrossRef]
- Ranjit, N.; Young, E.A.; Kaplan, G.A. Material hardship alters the diurnal rhythm of salivary cortisol. Int. J. Epidemiol. 2005, 34, 1138–1143. [Google Scholar] [CrossRef]
- Osgood, C.E.; Suci, G.J.; Tannenbaum, P. The Measurement of Meaning; University of Illinois Press: Urbana, IL, USA, 1957. [Google Scholar]
- McNair, D.; Lorr, M. An analysis of mood in neurotics. J. Abnorm. Soc. Psychol. 1964, 69, 620–627. [Google Scholar] [CrossRef]
- McNari, D.; Lorr, M.; Droppleman, L. Manual for the Profile of Mood States; Educational and Industrial Testing Services: San Diego, CA, USA, 1971. [Google Scholar]
- Kim, E.J.; Lee, S.I.; Jeong, D.U.; Shin, M.S.; Yoon, I.Y. Standardization and reliability and validity of the Korean edition of profile of mood states (K-POMS). Sleep Med. Psychophysiol. 2003, 10, 39–51. [Google Scholar]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.E. Manual for the State–Trait Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1970. [Google Scholar]
- Kim, J.T.; Shin, D.K. A study based on the standardization of the STAI for Korea. New Med. J. 1978, 21, 69–75. (In Korean) [Google Scholar]
- Bausell, R.B. The Design and Conduct of Meaningful Experiments Involving Human Participants; Oxford University Press: New York, NY, USA, 2015. [Google Scholar]
- Wilson, E.O. Biophillia: The Human Bond with Other Species, 12th ed.; Harvard University Press: Cambridge, MA, USA, 1984; pp. 1–168. [Google Scholar]
- Ulrich, R.S. Aesthetic and affective response to natural environment. In Behavior and the Natural Environment, 1st ed.; Altman, I., Wohlwill, J.F., Eds.; Springer: Boston, MA, USA, 1983; Volume 6, pp. 85–125. [Google Scholar]
- Kaplan, R.; Kaplan, S. The Experience of Nature: A Psychological Perspective, 1st ed.; Cambridge University Press: New York, NY, USA, 1989; pp. 1–352. [Google Scholar]
- Kaplan, S. The restorative benefits of nature: Toward an integrative framework. J. Environ. Psychol. 1995, 15, 169–182. [Google Scholar] [CrossRef]
- Staats, H.; Kieviet, A.; Hartig, T. Where to recover from attentional fatigue: An expectancy-value analysis of environmental preference. J. Environ. Psychol. 2003, 23, 147–157. [Google Scholar] [CrossRef]
- Korpela, K.; Hartig, T. Restorative qualities of favorite places. J. Environ. Psychol. 1996, 16, 221–233. [Google Scholar] [CrossRef] [Green Version]
- Elsadek, M.; Liu, B.; Lian, Z. Green façades: Their contribution to stress recovery and well-being in high-density cities. Urban For. Urban Green. 2019, 46, 126446. [Google Scholar] [CrossRef]
- Elsadek, M.; Liu, B.; Lian, Z.; Xie, J. The influence of urban roadside trees and their physical environment on stress relief measures: A field experiment in Shanghai. Urban For. Urban Green. 2019, 42, 51–60. [Google Scholar] [CrossRef]
- Mitchell, R.; Popham, F. Greenspace, urbanity and health: Relationships in England. J. Epidemiol. Commun. Health 2007, 61, 681–683. [Google Scholar] [CrossRef] [Green Version]
- Carrus, G.; Scopelliti, M.; Lafortezza, R.; Colangelo, G.; Ferrini, F.; Salbitano, F.; Agrimi, M.; Portoghesi, L.; Semenzato, P.; Sanesi, G. Go greener, feel better? The positive effects of biodiversity on the well-being of individuals visiting urban and peri-urban green areas. Landsc. Urban Plan. 2015, 134, 221–228. [Google Scholar] [CrossRef]
- Loreto, F.; Bagnoli, F.; Fineschi, S. One species, many terpenes: Matching chemical and biological diversity. Trends Plant Sci. 2009, 14, 416–420. [Google Scholar] [CrossRef]
- Calfapietra, C.; Fares, S.; Manes, F.; Morani, A.; Sgrigna, G.; Loreto, F. Role of Biogenic Volatile Organic Compounds (BVOC) emitted by urban trees on ozone concentration in cities: A review. Environ. Pollut. 2013, 183, 71–80. [Google Scholar] [CrossRef]
- Strosnider, H.; Kennedy, C.; Monti, M.; Yip, F. Rural and urban differences in air quality, 2008–2012, and community drinking water quality, 2010–2015—United States. MMWR Surveill. Summ. 2017, 66, 1. [Google Scholar] [CrossRef]
- Guo, Y.; Zeng, H.; Zheng, R.; Li, S.; Barnett, A.G.; Zhang, S.; Zou, X.; Huxley, R.; Chen, W.; Williams, G. The association between lung cancer incidence and ambient air pollution in China: A spatiotemporal analysis. Environ. Res. 2016, 144, 60–65. [Google Scholar] [CrossRef]
- Nowak, D.J.; Hirabayashi, S.; Bodine, A.; Greenfield, E. Tree and forest effects on air quality and human health in the United States. Environ. Pollut. 2014, 193, 119–129. [Google Scholar] [CrossRef] [Green Version]
- Gopalakrishnan, V.; Hirabayashi, S.; Ziv, G.; Bakshi, B.R. Air quality and human health impacts of grasslands and shrublands in the United States. Atmos. Environ. 2018, 182, 193–199. [Google Scholar] [CrossRef] [Green Version]
- Schipke, J.D.; Arnold, G.; Pelzer, M. Effect of respiration rate on short-term heart rate variability. J. Clin. Basic Cardio. 1999, 2, 92–95. [Google Scholar]
- Meneguzzo, F.; Albanese, L.; Bartolini, G.; Zabini, F. Temporal and Spatial Variability of Volatile Organic Compounds in the Forest Atmosphere. Int. J. Environ. Res. Public Health 2019, 16, 4915. [Google Scholar] [CrossRef] [PubMed] [Green Version]





© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Joung, D.; Lee, B.; Lee, J.; Lee, C.; Koo, S.; Park, C.; Kim, S.; Kagawa, T.; Park, B.-J. Measures to Promote Rural Healthcare Tourism with a Scientific Evidence-Based Approach. Int. J. Environ. Res. Public Health 2020, 17, 3266. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093266
Joung D, Lee B, Lee J, Lee C, Koo S, Park C, Kim S, Kagawa T, Park B-J. Measures to Promote Rural Healthcare Tourism with a Scientific Evidence-Based Approach. International Journal of Environmental Research and Public Health. 2020; 17(9):3266. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093266
Chicago/Turabian StyleJoung, Dawou, Bohwi Lee, Jeongdo Lee, Changjun Lee, Seungmo Koo, Changwon Park, Sebin Kim, Takahide Kagawa, and Bum-Jin Park. 2020. "Measures to Promote Rural Healthcare Tourism with a Scientific Evidence-Based Approach" International Journal of Environmental Research and Public Health 17, no. 9: 3266. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093266