Flexibility in Spanish Elite Inline Hockey Players: Profile, Sex, Tightness and Asymmetry

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
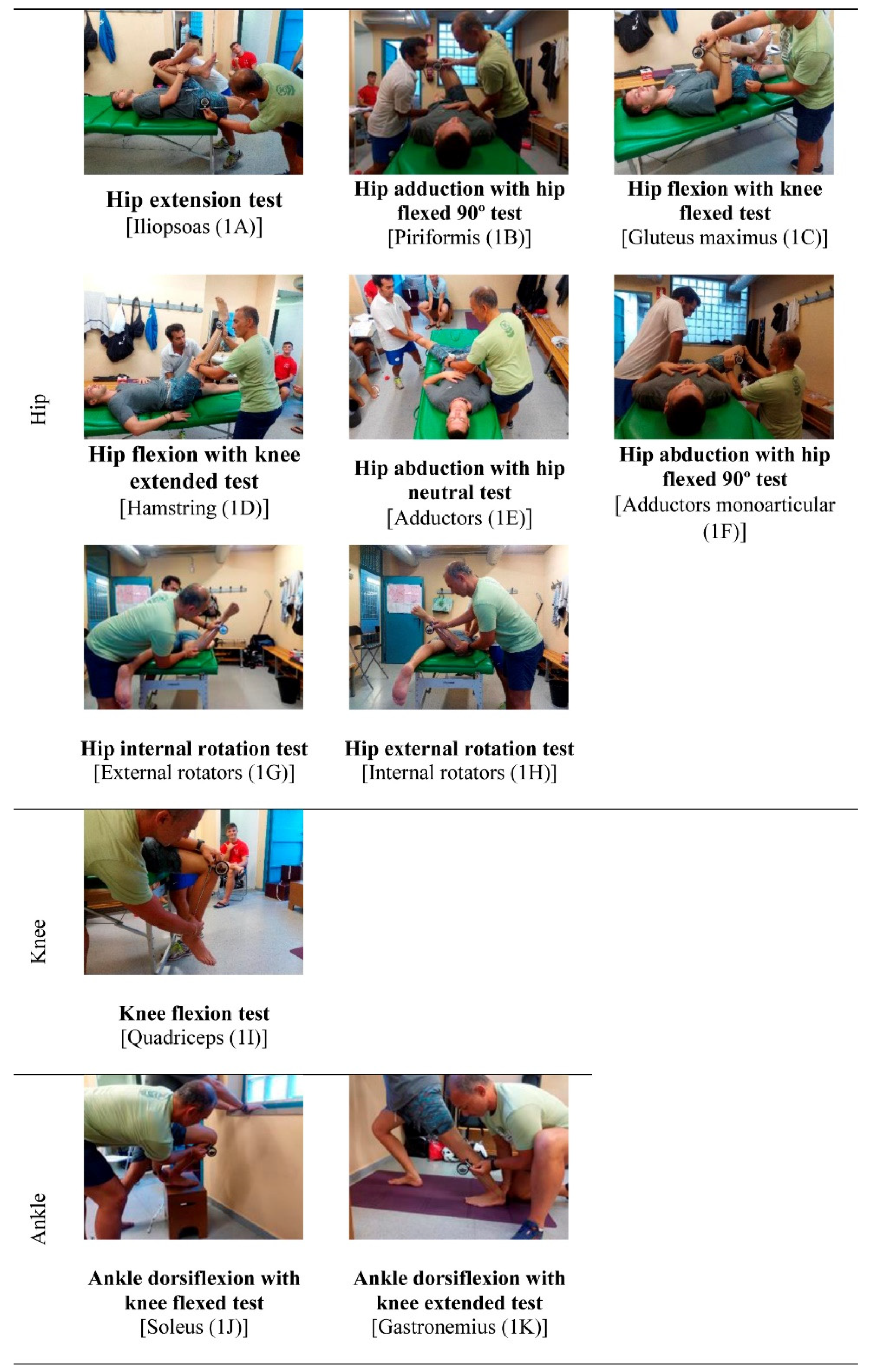
2.2. Testing Procedure
2.3. Statistical Analysis
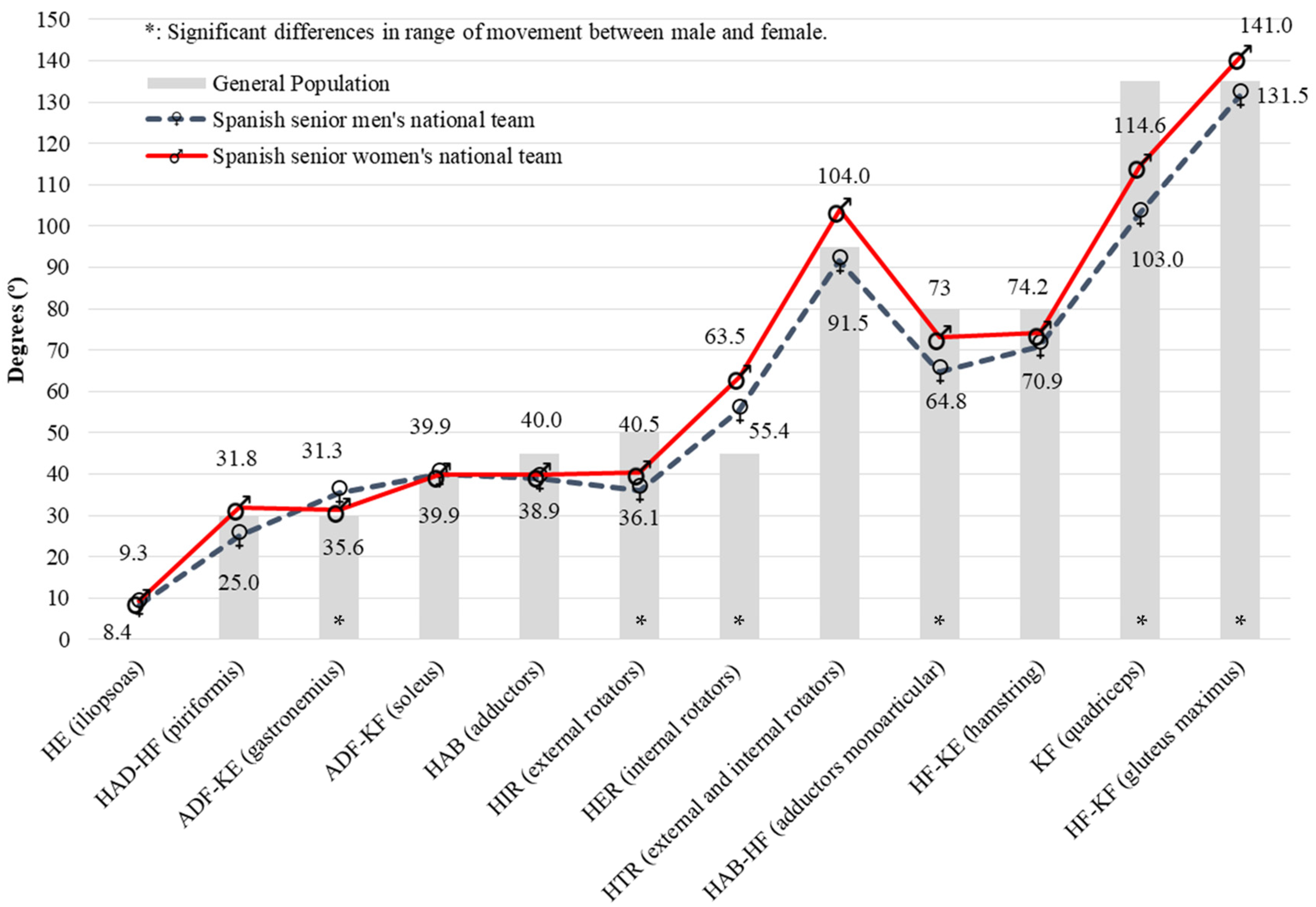
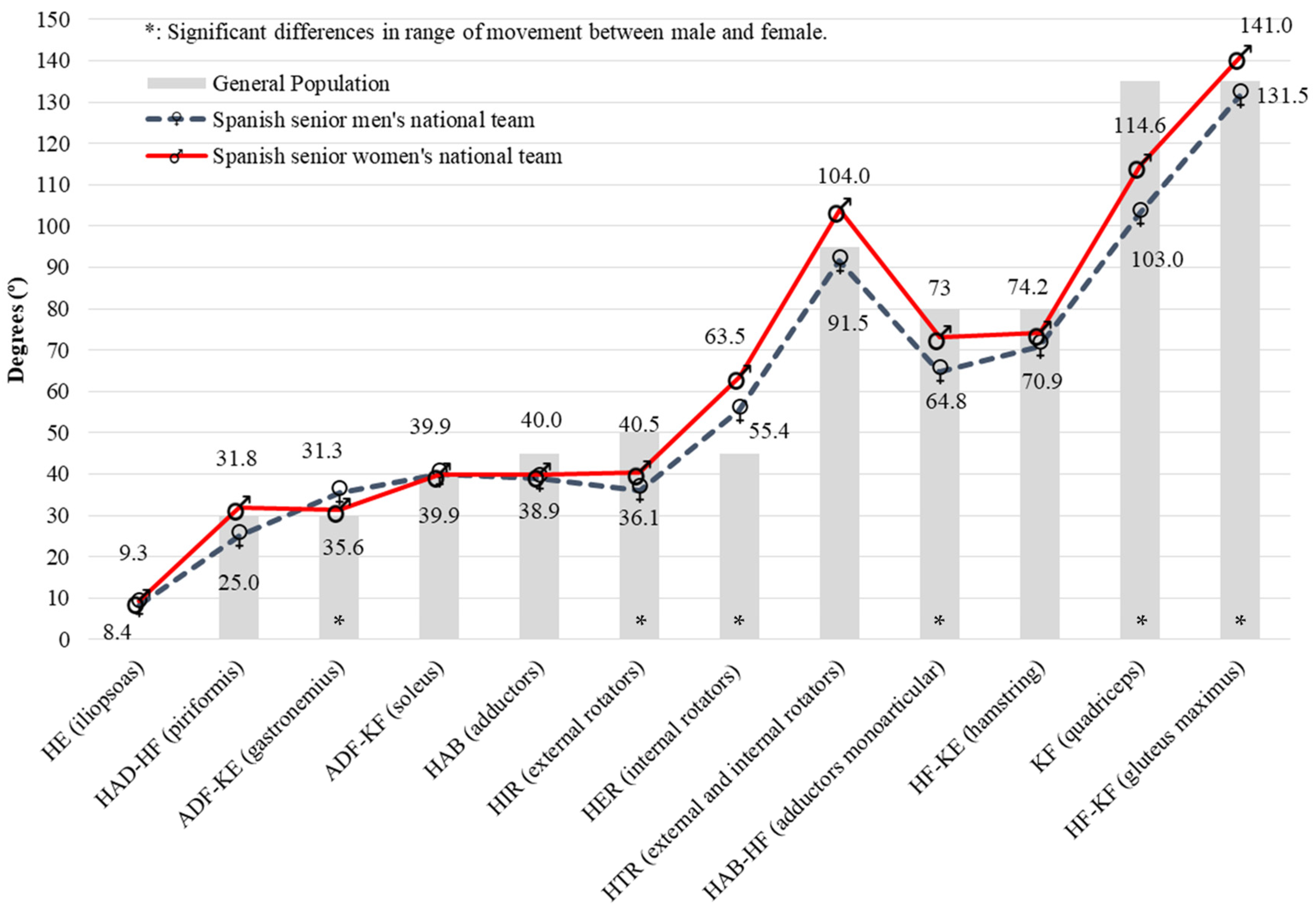
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

References
- Moromizato, K.; Kimura, R.; Fukase, H.; Yamaguchi, K.; Ishida, H. Whole-Body Patterns of the Range of Joint Motion in Young Adults: Masculine Type and Feminine Type. J. Physiol. Anthropol. 2016, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Surgeons American Academy of Orthopaedic. Joint Motion: Method of Measuring and Recording; Churchill, L., Ed.; Churchill Livingstone: Chicago, IL, USA, 1965. [Google Scholar]
- Gerhardt, J.; Cocchiarella, L.; Lea, R. The Practical Guide to Range of Motion Assessment; American Medical Association: Chicago, IL, USA, 2002. [Google Scholar]
- Magee, D. Orthopedic Physical Assessment; Elsevier Health Sciences: Philadelphia, PA, USA, 2013. [Google Scholar]
- Palmer, M.; Epler, M. Fundamentos de Las Técnicas de Evaluación Musculoesquelética; Paidotribo: Barcelona, Spain, 2002. [Google Scholar]
- Clarkson, H. Proceso Evaluativo Musculoesquelético: Amplitud Del Movimiento Articular y Test Manual de Fuerza Muscular; Paidotribo: Barcelona, Spain, 2003. [Google Scholar]
- Norkin, C.; White, D. Measurement Of Joint Motion: A Guide To Goniometry; FA Davis: Philadelphia, 2016. [Google Scholar]
- Peterson, F.; Kendall, E.; Geise, P. Kendall’s Músculos. Pruebas, Funciones y Dolor Postural; Marbán: Madrid, Spain, 2005. [Google Scholar]
- Hogg, J.; Schmitz, R.; Nguyen, A.-D.; Shultz, S.J. Lumbo-Pelvic-Hip Complex Passive Hip Range-of-Motion Values Across Sex and Sport. J. Athl. Train. 2018, 53, 560–567. [Google Scholar] [CrossRef]
- Cejudo, A.; Robles-Palazón, F.; Sainz De Baranda, P. Fútbol Sala de Élite: Diferencias de Flexibilidad Según Sexo. E-Balonmano.Com Rev. Cienc. Del Deport. 2019, 15, 37–48. [Google Scholar]
- Cejudo, A.; Robles-Palazón, F.; Ayala, F.; De Ste Croix, M.; Ortega-Toro, E.; Santonja-Medina, F.; Sainz de Baranda, P. Age-Related Differences in Flexibility in Soccer Players 8–19 Years Old. PeerJ 2019, 2019, e6236. [Google Scholar] [CrossRef] [PubMed]
- De la Fuente, A.; Gómez-Landero, L. Motor Differences in Cadet Taekwondo Athletes According to Competition Level. Rev. Int. Med. Y Cienc. La Act. Fis. Y Del Deport. 2019, 19, 63–75. [Google Scholar] [CrossRef]
- Battista, R.; Pivarnik, J.; Dummer, G.; Sauer, N.; Malina, R. Comparisons of Physical Characteristics and Performances among Female Collegiate Rowers. J. Sports Sci. 2007, 25, 651–657. [Google Scholar] [CrossRef]
- Cejudo, A.; Robles-Palazón, F.; Sainz de Baranda, P. Asimetrías de Flexibilidad En Jugadores de Fútbol Sala. Rev. Pedagógica Adal 2017, 34, 31–38. [Google Scholar]
- Oberg, B.; Ekstrand, J.; Moller, M.; Gillquist, J. Muscle Strength and Flexibility in Different Positions of Soccer Players. Int. J. Sports Med. 1984, 5, 213–216. [Google Scholar] [CrossRef]
- Cejudo, A.; Sainz De Baranda, P.; Ayala, F.; Santonja, F. Normative Data of Lower-Limb Muscle Flexibility in Futsal Players. Rev. Int. Med. Y Cienc. La Act. Fis. Y Del Deport. 2014, 14, 509–525. [Google Scholar]
- Dill, K.; Begalle, R.; Frank, B.; Zinder, S.; Padua, D. Altered Knee and Ankle Kinematics during Squatting in Those with Limited Weight-Bearing-Lunge Ankle-Dorsiflexion Range of Motion. J. Athl. Train. 2014, 49, 723–732. [Google Scholar] [CrossRef] [Green Version]
- Gonzalo-Skok, O.; Serna, J.; Rhea, M.; Marín, P. Relationships between Functional Movement Tests and Performance Tests in Young Elite Male Basketball Players. Int. J. Sports Phys. Ther. 2015, 10, 628–638. [Google Scholar] [PubMed]
- García-Pinillos, F.; Ruiz-Ariza, A.; Moreno del Castillo, R.; Latorre-Román, P. Impact of Limited Hamstring Flexibility on Vertical Jump, Kicking Speed, Sprint, and Agility in Young Football Players. J. Sports Sci. 2015, 33, 1293–1297. [Google Scholar] [CrossRef] [PubMed]
- Moeller, J.; Rifat, S. Winter Sports Medicine Handbook; McGraw Hill Professional: New York, NY, USA, 2004. [Google Scholar]
- Ekstrand, J.; Gillquist, J. The Frequency of Muscle Tightness and Injuries in Soccer Players. Am. J. Sports Med. 1982, 10, 75–78. [Google Scholar] [CrossRef] [PubMed]
- Young, S.; Harris, A.; Safran, M. Hip Range of Motion and Association With Injury in Female Professional Tennis Players Hip Systematic Review View Project New Zealand Rotator Cuff Registry View Project. Artic. Am. J. Sport. Med. 2014, 42, 2654–2658. [Google Scholar] [CrossRef]
- Malliaras, P.; Cook, J.; Kent, P. Reduced Ankle Dorsiflexion Range May Increase the Risk of Patellar Tendon Injury among Volleyball Players. J. Sci. Med. Sport 2006, 9, 304–309. [Google Scholar] [CrossRef]
- Backman, L.; Danielson, P. Low Range of Ankle Dorsiflexion Predisposes for Patellar Tendinopathy in Junior Elite Basketball Players: A 1-Year Prospective Study. Am. J. Sports Med. 2011, 39, 2626–2633. [Google Scholar] [CrossRef]
- Emery, C.; Meeuwisse, W. Risk Factors for Groin Injuries in Hockey. Med. Sci. Sports Exerc. 2001, 33, 1423–1433. [Google Scholar] [CrossRef]
- Sainz de Baranda, P.; Cejudo, A.; Ayala, F.; Santonja, F. Perfil Óptimo de Flexibilidad Del Miembro Inferior En Jugadoras de Fútbol Sala. Rev. Int. Med. Y Cienc. La Act. Fis. Y Del Deport. 2015, 15, 647–662. [Google Scholar] [CrossRef] [Green Version]
- Mölsä, J.; Kujala, U.; Myllynen, P.; Torstila, I.; Airaksinen, O. Injuries to the Upper Extremity in Ice Hockey: Analysis of a Series of 760 Injuries. Am. J. Sports Med. 2003, 31, 751–757. [Google Scholar] [CrossRef]
- Flik, K.; Lyman, S.; Marx, R. American Collegiate Men’s Ice Hockey: An Analysis of Injuries. Am. J. Sports Med. 2005, 33, 183–187. [Google Scholar] [CrossRef]
- Licencias|CSD—Consejo Superior de Deportes. Available online: https://www.csd.gob.es/es/federaciones-y-asociaciones/federaciones-deportivas-espanolas/licencias (accessed on 4 April 2020).
- Twist, P.; Rhodes, T. Exercise Physiology: The Bioenergetic and Physiological Demands of Ice Hockey. Natl. Strength Cond. Assoc. J. 1993, 15, 68–70. [Google Scholar] [CrossRef]
- Upjohn, T.; Turcotte, R.; Pearsall, D.; Loh, J. Three-Dimensional Kinematics of the Lower Limbs during Forward Ice Hockey Skating. Sport. Biomech. 2008, 7, 206–221. [Google Scholar] [CrossRef]
- Pearsall, D.; Turcotte, R.; Murphy, S. Biomechanics of Ice Hockey. Exerc. Sport Sci. 2000, 43, 675–692. [Google Scholar]
- Perrey, S.; Millet, G.; Candau, R.; Rouillon, J. Stretch-Shortening Cycle in Roller Ski Skating: Effects of Technique. Int. J. Sports Med. 1998, 19, 513–520. [Google Scholar] [CrossRef]
- López-Valenciano, A.; Ayala, F.; Vera-García, F.; De Ste Croix, M.; Hernández-Sánchez, S.; Ruiz-Pérez, I.; Cejudo, A.; Santonja, F. Comprehensive Profile of Hip, Knee and Ankle Ranges of Motion in Professional Football Players. J. Sports Med. Phys. Fit. 2019, 59, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Cejudo, A.; Sainz De Baranda, P.; Ayala, F.; Santonja, F. Perfil de Flexibilidad de La Extremidad Inferior En Jugadores Senior de Balonmano. Cuad. Psicol. del Deport. 2014, 14, 111–120. [Google Scholar] [CrossRef] [Green Version]
- Tyler, T.; Nicholas, S.; Campbell, R.; Mchugh, M. The Association of Hip Strength and Flexibility With the Incidence of Adductor Muscle Strains in Professional Ice Hockey Players. Am. J. Sports Med. 2001, 29, 124–128. [Google Scholar] [CrossRef]
- Wilcox, C.; Osgood, C.; White, H.; Vince, R. Investigating Strength and Range of Motion of the Hip Complex in Ice Hockey. J. Sport Rehabil. 2015, 24, 300–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hutchinson, M.; Milhouse, C.; Gapski, M. Comparison of Injury Patterns in Elite Hockey Players Using Ice versus In-Line Skates. Med. Sci. Sport. Exerc. 1988, 30, 1371–1373. [Google Scholar] [CrossRef]
- Mohajan, H. Two Criteria for Good Measurements in Research: Validity and Reliability. Ann. Spiru Haret Univ. Econ. Ser. 2017, 17, 59–82. [Google Scholar] [CrossRef] [Green Version]
- Cejudo, A.; Ayala, F.; Sainz de Baranda, P.; Santonja, F. Reliability of Two Methods of Clinical Examination of the Flexibility of the Hip Adductor Muscles. Int. J. Sports Phys. Ther. 2015, 10, 976–983. [Google Scholar] [PubMed]
- Cejudo, A.; Sainz de Baranda, P.; Ayala, F.; Santonja, F. Test-Retest Reliability of Seven Common Clinical Tests for Assessing Lower Extremity Muscle Flexibility in Futsal and Handball Players. Phys. Ther. Sport 2015, 16, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Taylor, K.L.; Sheppard, J.M.; Lee, H.; Plummer, N. Negative Effect of Static Stretching Restored When Combined with a Sport Specific Warm-up Component. J. Sci. Med. Sport 2009. [Google Scholar] [CrossRef] [PubMed]
- Ayala, F.; Sainz de Baranda, P.; De Ste Croix, M.; Santonja, F. Reproducibility and Criterion-Related Validity of the Sit and Reach Test and Toe Touch Test for Estimating Hamstring Flexibility in Recreationally Active Young Adults. Phys. Ther. Sport 2012, 13, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Santonja, F.; Ferrer, V.; Martínez, I. Exploración Clínica Del Síndrome de Isquiosurales Cortos. Selección 1995, 4, 81–91. [Google Scholar]
- Hopkins, W.; Marshall, S.; Batterham, A.; Hanin, J. Progressive Statistics for Studies in Sports Medicine and Exercise Science. Med. Sci. Sport. Exerc. 2009, 41, 3–12. [Google Scholar] [CrossRef] [Green Version]
- Ellenbecker, T.; Ellenbecker, G.; Roetert, E.; Silva, R.; Keuter, G.; Sperling, F. Descriptive Profile of Hip Rotation Range of Motion in Elite Tennis Players and Professional Baseball Pitchers. Am. J. Sports Med. 2007, 35, 1371–1376. [Google Scholar] [CrossRef]
- Norris, C. Guía Completa de Los Estiramientos, 2a; Paidotribo: Barcelona, Spain, 2007. [Google Scholar]
- Alter, M. Los Estiramientos; Paidotribo: Barcelona, Spain, 2004. [Google Scholar]
- Witvrouw, E.; Danneels, L.; Asselman, P.; D’Have, T.; Cambier, D. Muscle Flexibility as a Risk Factor for Developing Muscle Injuries in Male Professional Soccer Players: A Prospective Study. Am. J. Sports Med. 2003, 31, 41–46. [Google Scholar] [CrossRef]
- Kibler, W.; McQueen, C. Fitness Evaluations and Fitness Findings in Competitive Junior Tennis Players. Clin. Sports Med. 1988, 7, 403–416. [Google Scholar]
- Pallant, J. SPSS Survival Manual: A Step by Step Guide to Data Analysis Using SPSS, 3rd ed.; Open University Press: Philadelphia, PA, USA, 2007. [Google Scholar]
- Castro-Pinero, J.; Chillon, P.; Ortega, F.; Montesinos, J.; Sjostrom, M.; Ruiz, J. Criterion-Related Validity of Sit-and-Reach and Modified Sit-and-Reach Test for Estimating Hamstring Flexibility in Children and Adolescents Aged 617 Years. Int. J. Sports Med. 2009, 30, 658–662. [Google Scholar] [CrossRef]
- Dixon, J.; Keating, J. Variability in Straight Leg Raise Measurements. Physiotherapy 2000, 86, 361–370. [Google Scholar] [CrossRef]
- Fridén, J.; Lieber, R. Eccentric Exercise-Induced Injuries to Contractile and Cytoskeletal Muscle Fibre Components. Acta Physiol. Scand. 2001, 171, 321–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Behara, B.; Jacobson, B. Acute Effects of Deep Tissue Foam Rolling and Dynamic Stretching on Muscular Strength, Power, and Flexibility in Division I Linemen. J. Strength Cond. Res. 2017, 31, 888–892. [Google Scholar] [CrossRef] [PubMed]
- Su, H.; Chang, N.; Wu, W.; Guo, L.; Chu, I. Acute Effects of Foam Rolling, Static Stretching, and Dynamic Stretching during Warm-Ups on Muscular Flexibility and Strength in Young Adults. J. Sport Rehabil. 2017, 26, 469–477. [Google Scholar] [CrossRef]
- Cox, M.; Miles, D.; Verde, T.; Rhodes, E. Applied Physiology of Ice Hockey. Sport. Med. 1995, 19, 184–201. [Google Scholar] [CrossRef]
- Kawałek, K.; Garsztka, T. An Analysys of Muscle Balance in Professional Fi Eld Hockey Players. Trends Sport Sci. 2013, 4, 181–187. [Google Scholar]
- Shell, J.; Robbins, S.; Dixon, P.; Renaud, P.; Turcotte, R.; Wu, T.; Pearsall, D. Skating Start Propulsion: Three-Dimensional Kinematic Analysis of Elite Male and Female Ice Hockey Players. Sport. Biomech. 2017, 16, 313–324. [Google Scholar] [CrossRef]
- Budarick, A.R.; Shell, J.R.; Robbins, S.M.K.; Wu, T.; Renaud, P.J.; Pearsall, D.J. Ice Hockey Skating Sprints: Run to Glide Mechanics of High Calibre Male and Female Athletes. Sport. Biomech. 2018, 1–17. [Google Scholar] [CrossRef]
- Varlotta, G.; Lager, S.; Nicholas, S.; Browne, M.; Schlifstein, T. Professional Roller Hockey Injuries. Clin. J. Sport Med. 2000, 10, 29–33. [Google Scholar] [CrossRef]
- Moreno-Alcaraz, V.; Cejudo, A.; Sainz de Baranda, P. Injury Types and Frequency in Spanish Inline Hockey Players. Phys. Ther. Sport 2020, 42, 91–99. [Google Scholar] [CrossRef]
- Fousekis, K.; Tsepis, E.; Poulmedis, P.; Athanasopoulos, S.; Vagenas, G. Intrinsic Risk Factors of Non-Contact Quadriceps and Hamstring Strains in Soccer: A Prospective Study of 100 Professional Players. Br. J. Sports Med. 2011, 45, 709–714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kersting, U.; Oliveira, A.; Hansen, J.; Thimm, M.; Lysdal, F.; Mortensen, K.; Haase, J. A Testing Battery on Balance and Performance Symmetry for Team Sports—An Example from Ice Hockey. Isbs Proc. Arch. 2017, 35. [Google Scholar]

{kind=link}
{kind=link}
| Variable | Male (n = 10) | Female (n = 10) | Total (n = 20) |
|---|---|---|---|
| Age (years) | 22.30 ± 2.54 | 22.70 ± 3.33 | 22.50 ± 2.89 |
| Body mass (kg) | 71.87 ± 9.64 | 66.83 ± 9.20 | 69.35 ± 9.53 |
| Height (m) * | 1.73 ± 0.05 | 1.66 ± 0.05 | 1.69 ± 0.06 |
| BMI (kg/m2) | 23.96 ± 2.77 | 24.32 ± 2.88 | 24.14 ± 2.76 |
| Years of experience | 14.20 ± 2.97 | 12.90 ± 3.98 | 13.55 ± 3.49 |
| Training months/year * | 11.20 ± 0.92 | 10.00 ± 0.00 | 10.60 ± 0.88 |
| Training days/week | 2.80 ± 0.42 | 2.80 ± 1.03 | 2.80 ± 0.77 |
| Training hours per week | 5.40 ± 2.27 | 5.00 ± 1.83 | 5.20 ± 2.02 |
| ROM | HE [21] | HAD-HF [3,8] | ADF-KE [6,47] | ADF-KF [23] | HAB [2] | HIR [6,48] |
| Value | 13° | 30° | 30° | 45° | 28° | 45° |
| ROM | HER [3] | HAB-HF [2] | HF-KE [49] | KF [50] | HF-KF [3] | |
| Value | 50° | 80° | 88° | 132° | 135° |
| ROM | Dominant | Non-Dominant | Players with Asymmetries | p-Value | Cohen’s d |
|---|---|---|---|---|---|
| HE (iliopsoas) | 7.0 ± 5.8° | 9.80 ± 7.8° | 3 | 0.132 | −0.3288 Small |
| HAD-HF (piriformis) | 25.0 ± 3.3° | 27.60 ± 5.8° | 5 | 0.128 | −0.4851 Small |
| ADF-KE (gastronemius) | 36.2 ± 5.5° | 35.0 ± 6.4° | 1 | 0.279 | 0.1811 No effect |
| ADF-KF (soleus) | 39.6 ± 4.9° | 40.2 ± 5.7° | 0 | 0.591 | −0.2209 Small |
| HAB (adductors) | 39.2 ± 3.2° | 38.60 ± 3.5° | 1 | 0.560 | 0.3333 Small |
| HIR (external rotators) | 35.0 ± 6.6° | 37.2 ± 4.6° | 1 | 0.146 | −0.3922 Small |
| HER (internal rotators) | 57.6 ± 10.9° | 53.2 ± 8.1° | 4 | 0.068 | 0.4417 Small |
| HAB-HF (monoarticular adductors) | 64.0 ± 7.2° | 65.6 ± 6.1° | 1 | 0.387 | −0.1534 Small |
| HF-KE (hamstrings) | 71.4 ± 4.2° | 70.4 ± 4.1° | 0 | 0.322 | 0.25 Small |
| KF (quadriceps) | 102.0 ± 9.6° | 104.0 ± 14.4° | 2 | 0.430 | −0.1699 Small |
| HF-KF (gluteus maximus) | 133.2 ± 6.3° | 129.8 ± 5.5° | 1 | 0.042 | 0.7243 Moderate |
| ROM | Dominant | Non-Dominant | Players with Asymmetries | p-Value | Cohen’s d |
|---|---|---|---|---|---|
| HE (iliopsoas) | 8.2 ± 5.9° | 10.4 ± 4.4° | 3 | 0.178 | −0.4417 Small |
| HAD-HF (piriformis) | 31.2 ± 5.6° | 32.4 ± 4.7° | 1 | 0.279 | −0.2209 Small |
| ADF-KE (gastronemius) | 31.0 ± 5.4° | 31.6 ± 6.8° | 1 | 0.685 | 0 No effect |
| ADF-KF (soleus) | 38.8 ± 5.6° | 41.0 ± 5.3° | 0 | 0.083 | −0.56 Small |
| HAB (adductors) | 41.2 ± 2.9° | 38.8 ± 3.2° | 1 | 0.005 | 1.1767 Moderate |
| HIR (external rotators) | 41.8 ± 6.3° | 39.2 ± 4.8° | 1 | 0.090 | 0.3922 Small |
| HER (internal rotators) | 64.8 ± 5.3° | 62.2 ± 6.9° | 4 | 0.057 | 0.3621 Small |
| HAB-HF9 (monoarticular adductors) | 73.4 ± 5.8° | 72.6 ± 4.8° | 1 | 0.555 | 0.2209 Small |
| HF-KE (hamstrings) | 74.0 ± 6.7° | 74.4 ± 6.9° | 0 | 0.716 | 0 No effect |
| KF (quadriceps) | 115.4 ± 9.4° | 113.8 ± 10.7° | 2 | 0.428 | 0.2102 Small |
| HF-KF (gluteus maximus) | 141.8 ± 6.2° | 140.2 ± 4.9° | 1 | 0.366 | 0.1961 No effect |
| ROM | Tightness | Normal | R | p-Value | ||
|---|---|---|---|---|---|---|
| n | Values | n | Values | |||
| HE (iliopsoas) | 18 | 6.2 ± 4.1° | 2 | 20.0 ± 0.0° | −0.737 | 0.000 |
| HAD-HF (piriformis) | 11 | 24.7 ± 2.7° | 9 | 32.2 ± 5.2° | −0.697 | 0.001 |
| ADF-KE (gastronemius) | 5 | 27.6 ± 3.8° | 15 | 35.6 ± 5.2° | −0.595 | 0.006 |
| ADF-KF (soleus) | 16 | 37.2 ± 3.6° | 4 | 47.0 ± 1.15° | −0.781 | 0.000 |
| HAB (adductors) | 0 | 20 | 40.2 ± 3.1° | |||
| HIR (external rotators) | 19 | 37.5 ± 6.0° | 1 | 56.0° | −0.577 | 0.008 |
| HER (internal rotators) | 2 | 44.0 ± 5.7° | 18 | 63.1 ± 7.3° | −0.642 | 0.002 |
| HAB-HF (monoarticular adductors) | 19 | 68.1 ± 7.8° | 1 | 80.0° | −0.332 | 0.152 |
| HF-KE (hamstrings) | 20 | 72.4 ± 5.9° | 0 | |||
| KF (quadriceps) | 20 | 108.7 ± 11.5° | 0 | |||
| HF-KF (gluteus maximus) | 7 | 129.4 ± 4.4° | 13 | 141.8 ± 4.6° | −0.809 | 0.000 |
| ROM | Tightness | Normal | R | p-Value | ||
|---|---|---|---|---|---|---|
| n | Value | n | Value | |||
| HE (iliopsoas) | 18 | 8.5 ± 3.9° | 2 | 24.0 ± 5.7° | −0.770 | 0.000 |
| HAD-HF (piriformis) | 11 | 26.5 ± 4.9° | 9 | 34.22 ± 3.2° | −0.688 | 0.001 |
| ADF-KE (gastronemius) | 5 | 25.2 ± 2.3° | 15 | 36.0 ± 5.2° | −0.721 | 0.000 |
| ADF-KF (soleus) | 16 | 38.5 ± 3.5° | 4 | 49.0 ± 2.0° | −0.805 | 0.000 |
| HAB (adductors) | 0 | 20 | 38.7 ± 3.3° | |||
| HIR (internal rotators) | 19 | 37.7 ± 4.2° | 1 | 48.0° | −0.489 | 0.029 |
| HER (external rotators) | 2 | 41.0 ± 4.2° | 18 | 59.6 ± 6.8° | −0.659 | 0.002 |
| HAB-HF (monoarticular adductors) | 19 | 68.5 ± 6.1° | 1 | 80.0° | −0.398 | 0.082 |
| HF-KE (hamstrings) | 20 | 72.5 ± 5.5° | 0 | |||
| KF (quadriceps) | 20 | 108.9 ± 13.3° | 0 | |||
| HF-KF (gluteus maximus) | 7 | 128.0 ± 5.2° | 13 | 138.8 ± 5.4° | −0.714 | 0.000 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cejudo, A.; Moreno-Alcaraz, V.J.; Izzo, R.; Robles-Palazón, F.J.; Sainz de Baranda, P.; Santonja-Medina, F. Flexibility in Spanish Elite Inline Hockey Players: Profile, Sex, Tightness and Asymmetry. Int. J. Environ. Res. Public Health 2020, 17, 3295. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093295
Cejudo A, Moreno-Alcaraz VJ, Izzo R, Robles-Palazón FJ, Sainz de Baranda P, Santonja-Medina F. Flexibility in Spanish Elite Inline Hockey Players: Profile, Sex, Tightness and Asymmetry. International Journal of Environmental Research and Public Health. 2020; 17(9):3295. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093295
Chicago/Turabian StyleCejudo, Antonio, Víctor Jesús Moreno-Alcaraz, Riccardo Izzo, Francisco Javier Robles-Palazón, Pilar Sainz de Baranda, and Fernando Santonja-Medina. 2020. "Flexibility in Spanish Elite Inline Hockey Players: Profile, Sex, Tightness and Asymmetry" International Journal of Environmental Research and Public Health 17, no. 9: 3295. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093295