Relationship between the Condylion–Gonion–Menton Angle and Dentoalveolar Heights


 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
- Caucasian race,
- age ≥ 8, and
- a good quality lateral X-ray.
- patients with systemic diseases,
- patients with genetic syndromes,
- previous orthodontic treatment, and
- a history of obstructed nose breathing.
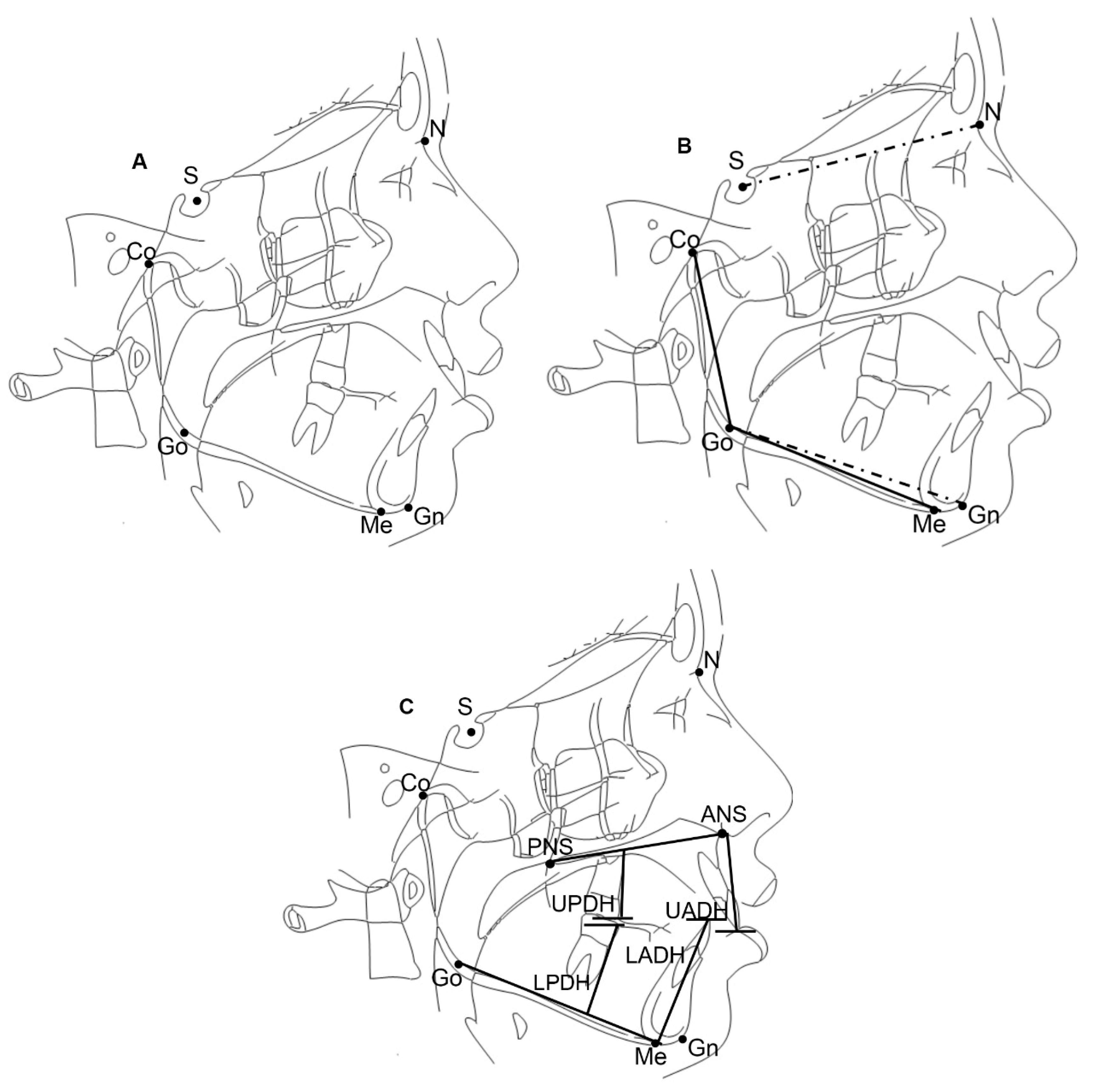
2.2. Cephalometric Evaluation
- UADH: upper anterior dental height measured as the perpendicular distance from the maxillary incisor edge to the palatal plane (mm),
- LADH: lower anterior dental height measured as the perpendicular distance from the mandibular central incisor edge to the mandibular plane (mm),
- UPDH: upper posterior dental height measured as the perpendicular distance from the mesiobuccal cusp tip of the maxillary first molar to the palatal plane (mm), and
- LPDH: lower posterior dental height measured as the perpendicular distance from the mesiobuccal cusp tip of the mandibular first molar to the mandibular plane (mm).
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Rasool, G.; Bibi, T. Comparison of Dentoalveolar Heights in Relation to Vertical Facial Pattern. J. Khyber College Dent. 2016, 7, 16–20. [Google Scholar]
- Schudy, F. The rotation of the mandible resulting from growth: Its implications in orthodontic treatment. Angle Orthod. 1965, 35, 36–50. [Google Scholar] [PubMed]
- Björk, A. Prediction of mandibular growth rotation. Am. J. Orthod. 1969, 55, 585–599. [Google Scholar] [CrossRef]
- Björk, A.; Skieller, V. Facial development and tooth eruption. An implant study at the age of puberty. Am. J. Orthod. 1972, 62, 339–383. [Google Scholar] [CrossRef]
- Von Bremen, J.; Pancherz, H. Association between Björk’s structural signs of mandibular growth rotation and skeletofacial morphology. Angle Orthod. 2005, 75, 506–509. [Google Scholar] [PubMed]
- Tanner, A.C.R.; Sonis, A.L.; Lif Holgerson, P.; Starr, J.R.; Nunez, Y.; Kressirer, C.A.; Paster, B.J.; Johansson, I. White-spot lesions and gingivitis microbiotas in orthodontic patients. J. Dent. Res. 2012, 91, 853–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riedel, R.A. The relation of maxillary structures to cranium in malocclusion and in normal occlusion. Angle Orthod. 1952, 22, 142–145. [Google Scholar]
- Valletta, R.; Pango, A.; Tortora, G.; Rongo, R.; Simeon, V.; Spagnuolo, G.; D’Antò, V. Association between Gingival Biotype and Facial Typology through Cephalometric Evaluation and Three-Dimensional Facial Scanning. Appl. Sci. 2019, 9, 5057. [Google Scholar] [CrossRef] [Green Version]
- Arat, Z.M.; Rübendüz, M. Changes in dentoalveolar and facial heights during early and late growth periods: A longitudinal study. Angle Orthod. 2005, 75, 69–74. [Google Scholar]
- Zafar-Ul-Islam, S.A.; Fida, M. Dentoalveolar heights in skeletal class I normodivergent facial patterns. J. Coll. Physicians Surg. Pak. 2012, 22, 5–9. [Google Scholar]
- Sarnäs, K.V.; Solow, B. Early adult changes in the skeletal and soft-tissue profile. Eur. J. Orthod. 1980, 2, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Tallgren, A.; Solow, B. Age differences in adult dentoalveolar heights. Eur. J. Orthod. 1991, 13, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, H.; Nakamura, S.; Iwasaki, H.; Kitazawa, S.; Tsukada, H.; Sato, Y. Dentoalveolar compensation related to variations in sagittal jaw relationships. Angle Orthod. 1999, 69, 534–538. [Google Scholar] [PubMed]
- Rongo, R.; Bucci, R.; Adaimo, R.; Amato, M.; Martina, S.; Valletta, R.; D’anto, V. Two-dimensional versus three-dimensional Fränkel Manoeuvre: A reproducibility study. Eur. J. Orthod. 2020, 42, 157–162. [Google Scholar] [CrossRef]
- Anwar, N.; Fida, M. Compensation for vertical dysplasia and its clinical application. Eur. J. Orthod. 2009, 31, 516–522. [Google Scholar] [CrossRef]
- Mangla, R.; Singh, N.; Dua, V.; Padmanabhan, P.; Khanna, M. Evaluation of mandibular morphology in different facial types. Contemp. Clin. Dent. 2011, 2, 200–206. [Google Scholar] [CrossRef]
- Isaacson, J.R.; Isaacson, R.J.; Speidel, T.M.; Worms, F.W. Extreme Variation in Vertical Facial Growth and Associated Variation in Skeletal and Dental Relations. Angle Orthod. 1971, 41, 219–229. [Google Scholar]
- Janson, G.R.; Metaxas, A.; Woodside, D.G. Variation in maxillary and mandibular molar and incisor vertical dimension in 12-year-old subjects with excess, normal, and short lower anterior face height. Am. J. Orthod. Dentofac. Orthop. 1994, 106, 409–418. [Google Scholar] [CrossRef]
- Betzenberger, D.; Ruf, S.; Pancherz, H. The compensatory mechanism in high-angle malocclusions: A comparison of subjects in the mixed and permanent dentition. Angle Orthod. 1999, 69, 27–32. [Google Scholar]
- Enoki, C.; Telles, C.D.S. Dental-Skeletal Dimensions in Growing Individuals with Variations in the Lower Facial Height. Braz. Dent. J. 2004, 15, 68–74. [Google Scholar] [CrossRef]
- Martina, R.; Farella, M.; Tagliaferri, R.; Michelotti, A.; Quaremba, G.; van Eijden, T.M.G.J. The Relationship between molar dentoalveolar and craniofacial heights. Angle Orthod. 2005, 75, 974–979. [Google Scholar] [PubMed]
- Islam, Z.U.; Shaikh, A.J.; Fida, M. Dentoalveolar Heights in Vertical and Sagittal Facial Patterns. J. Coll. Physicians Surg. Pak. 2016, 26, 753–757. [Google Scholar] [PubMed]
- Opdebeeck, H.; Bell, W. The short face syndrome. Am. J. Orthod. 1978, 73, 499–511. [Google Scholar] [CrossRef]
- Opdebeeck, H.; Bell, W.H.; Eisenfeld, J.; Mishelevich, D. Comparative study between the SFS and LFS rotation as a possible morphogenic mechanism. Am. J. Orthod. 1978, 74, 509–521. [Google Scholar] [CrossRef]
- Bell, W.H.; Creekmore, T.D.; Alexander, R.G. Surgical correction of the long face syndrome. Am. J. Orthod. 1977, 71, 40–67. [Google Scholar] [CrossRef]
- Schendel, S.A.; Eisenfeld, J.; Bell, W.H.; Epker, B.N.; Mishelevich, D.J. The long face syndrome: Vertical maxillary excess. Am. J. Orthod. 1976, 70, 398–408. [Google Scholar] [CrossRef]
- Kucera, J.; Marek, I.; Tycova, H.; Baccetti, T. Molar height and dentoalveolar compensation in adult subjects with skeletal open bite. Angle Orthod. 2011, 81, 564–569. [Google Scholar] [CrossRef]
- Xiao, D.; Gao, H.; Ren, Y. Craniofacial morphological characteristics of Chinese adults with normal occlusion and different skeletal divergence. Eur. J. Orthod. 2010, 33, 198–204. [Google Scholar] [CrossRef] [Green Version]
- Rongo, R.; Martina, S.; Bucci, R.; Valletta, R.; D’Antò, V.; Martina, R. Differences in craniofacial growth of Class II individuals from different decades: A retrospective study. Orthod. Craniofacial Res. 2019, 22, 304–311. [Google Scholar] [CrossRef]
- Petrovic, A.; Stutzmann, J.; Lavergne, J.; Shaye, R. Is it possible to modulate the growth of the human mandible with a functional appliance? Int. J. Orthod. 1991, 29, 3–8. [Google Scholar]
- Franchi, L.; Baccetti, T. Prediction of Individual Mandibular Changes Induced by Functional Jaw Orthopedics Followed by Fixed Appliances in Class II Patients. Angle Orthod. 2006, 76, 950–954. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Antò, V.; Pango Madariaga, A.C.; Rongo, R.; Bucci, R.; Simeon, V.; Franchi, L.; Valletta, R. Distribution of the condylion-gonion-menton (cogome^) angle in a population of patients from southern Italy. Dent. J. 2019, 7, 104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molhave, A. Sitting & standing posture in man. Ugeskr. Laeger. 1958, 120, 1516–1518. [Google Scholar] [PubMed]
- Solow, B.; Tallgren, A. Natural head position in standing subjects. Acta Odontol. Scand. 1971, 29, 591–607. [Google Scholar] [CrossRef] [PubMed]
- Siersbæk-Nielsen, S.; Solow, B. Intra- and interexaminer variability in head posture recorded by dental auxiliaries. Am. J. Orthod. 1982, 82, 50–57. [Google Scholar] [CrossRef]
- Kuitert, R.; Beckmann, S.; van Loenen, M.; Tuinzing, B.; Zentner, A. Dentoalveolar compensation in subjects with vertical skeletal dysplasia. Am. J. Orthod. Dentofac. Orthop. 2006, 129, 649–657. [Google Scholar] [CrossRef]
- Arriola-Guillén, L.E.; Flores-Mir, C. Anterior maxillary dentoalveolar and skeletal cephalometric factors involved in upper incisor crown exposure in subjects with Class II and III skeletal open bite. Angle Orthod. 2015, 85, 72–79. [Google Scholar] [CrossRef] [Green Version]
- Choi, Y.J.; Kim, D.J.; Nam, J.; Chung, C.J.; Kim, K.-H. Cephalometric configuration of the occlusal plane in patients with anterior open bite. Am. J. Orthod. Dentofac. Orthop. 2016, 149, 391–400. [Google Scholar] [CrossRef]
- Arriola-Guillén, L.E.; Flores-Mir, C. Molar heights and incisor inclinations in adults with Class II and Class III skeletal open-bite malocclusions. Am. J. Orthod. Dentofac. Orthop. 2014, 145, 325–332. [Google Scholar] [CrossRef]
- Kim, S.-J.; Kim, K.-H.; Yu, H.-S.; Baik, H.-S. Dentoalveolar compensation according to skeletal discrepancy and overjet in skeletal Class III patients. Am. J. Orthod. Dentofac. Orthop. 2014, 145, 317–324. [Google Scholar] [CrossRef]
- Angelieri, F.; Franchi, L.; Cevidanes, L.H.S.; Bueno-Silva, B.; McNamara, J.A. Prediction of rapid maxillary expansion by assessing the maturation of the midpalatal suture on cone beam CT. Dent. Press J. Orthod. 2016, 21, 115–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Enlow, D.H.; Moyers, R. Handbook of Facial Growth; WB Saunders Company: Philadelphia, PA, USA, 1982. [Google Scholar]
- DeVincenzo, J.P. Changes in mandibular length before, during, and after successful orthopedic correction of Class II malocclusions, using a functional appliance. Am. J. Orthod. Dentofac. Orthop. 1991, 99, 241–257. [Google Scholar] [CrossRef]
- Subtelny, J.D.; Sakuda, M. Open-bite: Diagnosis and treatment. Am. J. Orthod. 1964, 50, 337–358. [Google Scholar] [CrossRef]
- Rohit, K. Open bite malocclusion: An overview. J. Oral Health Craniofac. Sci. 2018, 3, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Scheffler, N.R.; Proffit, W.R.; Phillips, C. Outcomes and stability in patients with anterior open bite and long anterior face height treated with temporary anchorage devices and a maxillary intrusion splint. Am. J. Orthod. Dentofac. Orthop. 2014, 146, 594–602. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Variables | N | Mean ± SD | 95% CI |
|---|---|---|---|
| Age | 270 | 15.6 ± 5.9 | 14.9–16.3 |
| Gender | N | Percentage % | |
| Male | 115 | 15.5 ±5.2 | 14.5–16.5 |
| Female | 155 | 15.7 ± 6.4 | 14.7–16.7 |
| Variables | Mean ± SD | 95% CI |
|---|---|---|
| CoGoMe^ | 127.1 ± 7.7 | 126.2, 128.0 |
| SN^GoGn | 31.9 ± 6.8 | 31.1, 32.7 |
| UADH | 28.6 ± 3.7 | 28.1, 29.0 |
| LADH | 39.3 ± 4.7 | 38.7, 39.8 |
| UPDH | 22.4 ± 3.6 | 22.0, 22.8 |
| LPDH | 29.0 ± 4.1 | 28.5, 29.5 |
| Number of Subjects | CoGoMe^ | UADH | LADH | UPDH | LPDH | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| t | p-Value | t | p-Value | t | p-Value | t | p-Value | t | p-Value | ||
| Total (270) | SN^GoGn | 0.656 | <0.001 | 0.145 | 0.017 | 0.006 | 0.928 | −0.015 | 0.807 | −0.078 | 0.201 |
| CoGoMe^ | −0.021 | 0.733 | −0.118 | 0.053 | −0.102 | 0.095 | −0.183 | 0.003 | |||
| UADH | 0.774 | <0.001 | 0.779 | <0.001 | 0.659 | <0.001 | |||||
| LADH | 0.771 | <0.001 | 0.873 | <0.001 | |||||||
| UPDH | 0.708 | <0.001 | |||||||||
| Growing ≤16 years old (194) | SN^GoGn | 0.540 | <0.001 | 0.202 | 0.005 | 0.102 | 0.159 | 0.050 | 0.489 | 0.032 | 0.654 |
| CoGoMe^ | −0.008 | 0.912 | −0.092 | 0.200 | −0.092 | 0.201 | −0.143 | 0.007 | |||
| UADH | 0.774 | <0.001 | 0.761 | <0.001 | 0.629 | <0.001 | |||||
| LADH | 0.754 | <0.001 | 0.867 | <0.001 | |||||||
| UPDH | 0.650 | <0.001 | |||||||||
| Not Growing >16 years old (76) | SN^GoGn | 0.770 | <0.001 | 0.187 | 0.034 | 0.008 | 0.944 | 0.089 | 0.444 | −0.089 | 0.443 |
| CoGoMe^ | 0.083 | 0.477 | −0.008 | 0.947 | 0.087 | 0.457 | −0.148 | 0.006 | |||
| UADH | 0.730 | <0.001 | 0.801 | <0.001 | 0.654 | <0.001 | |||||
| LADH | 0.724 | <0.001 | 0.840 | <0.001 | |||||||
| UPDH | 0.682 | <0.001 | |||||||||
| Total (270) | Growing ≤16 years old (194) | Not Growing >16 years old (76) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Outcome | Model | Beta | 95% CI | p-Value | Beta | 95% CI | p-Value | Beta | 95% CI | p-Value |
| UADH | 1 (CoGoMeˆ) | −0.01 | −0.07–0.05 | 0.733 | −0.04 | −0.08–0.07 | 0.912 | 0.03 | −0.06–0.13 | 0.477 |
| 2 (CoGoMeˆ Age Sex) | 0.01 | −0.04–0.07 | 0.550 | |||||||
| LADH | 1 (CoGoMe^) | −0.07 | −0.15–0.00 | 0.053 | −0.06 | −0.15–0.03 | 0.200 | −0.04 | −0.12–0.11 | 0.947 |
| 2 (CoGoMeˆ Age Sex) | −0.02 | −0.09–0.04 | 0.453 | |||||||
| UPDH | 1 (CoGoMeˆ) | −0.04 | −0.10–0.01 | 0.095 | −0.04 | −0.11–0.02 | 0.201 | 0.34 | −0.06–0.12 | 0.457 |
| 2 (CoGoMeˆ Age Sex) | −0.01 | −0.05–0.05 | 0.842 | |||||||
| LPDH | 1 (CoGoMeˆ) | −0.09 | −0.16–−0.04 | 0.003 | −0.08 | −0.16–−0.01 | 0.007 | −0.07 | −0.14–−0.00 | 0.006 |
| 2 (CoGoMeˆ Age Sex) | −0.07 | −0.11–−0.02 | 0.004 | |||||||
| Total (270) | Growing ≤16 years old (194) | Not Growing >16 years old (76) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Outcome | Model | Beta | 95% CI | p-Value | Beta | 95% CI | p-Value | Beta | 95% CI | p-Value |
| UADH | 1 (SN^GoGn) | 0.08 | 0.01–0.14 | 0.017 | 0.12 | 0.04, 0.21 | 0.005 | 0.08 | 0.01–0.17 | 0.034 |
| 2 (SN^GoGn Age Sex) | 0.11 | 0.05–0.17 | 0.001 | |||||||
| LADH | 1 (SN^GoGn) | −0.01 | −0.08–0.08 | 0.928 | 0.08 | −0.03–0.19 | 0.159 | 0.00 | −0.12–0.13 | 0.944 |
| 2 (SN^GoGn Age Sex) | 0.05 | −0.02–0.13 | 0.170 | |||||||
| UPDH | 1 (SN^GoGn) | −0.01 | −0.07–0.06 | 0.807 | 0.03 | −0.05–0.10 | 0.489 | 0.04 | −0.06–0.13 | 0.444 |
| 2 (SN^GoGn Age Sex) | 0.04 | −0.02–0.09 | 0.205 | |||||||
| LPDH | 1 (SN^GoGn) | −0.05 | −0.12–0.03 | 0.201 | 0.02 | −0.07–0.11 | 0.654 | −0.04 | −0.15–0.07 | 0.443 |
| 2 (SN^GoGn Age Sex) | −0.00 | −0.07–0.06 | 0.925 | |||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valletta, R.; Rongo, R.; Pango Madariaga, A.C.; Baiano, R.; Spagnuolo, G.; D’Antò, V. Relationship between the Condylion–Gonion–Menton Angle and Dentoalveolar Heights. Int. J. Environ. Res. Public Health 2020, 17, 3309. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093309
Valletta R, Rongo R, Pango Madariaga AC, Baiano R, Spagnuolo G, D’Antò V. Relationship between the Condylion–Gonion–Menton Angle and Dentoalveolar Heights. International Journal of Environmental Research and Public Health. 2020; 17(9):3309. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093309
Chicago/Turabian StyleValletta, Rosa, Roberto Rongo, Ada Carolina Pango Madariaga, Roberta Baiano, Gianrico Spagnuolo, and Vincenzo D’Antò. 2020. "Relationship between the Condylion–Gonion–Menton Angle and Dentoalveolar Heights" International Journal of Environmental Research and Public Health 17, no. 9: 3309. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph17093309