Technology Used to Recognize Activities of Daily Living in Community-Dwelling Older Adults

 ,
,  ,
,  and
and 
Abstract
:1. Introduction
- (1)
- Which ADL are recognised by technology?
- (2)
- What types of technology are currently used to recognise ADL in free-living older adults?
- (3)
- How are ADL recognised by technology (inferred/direct measurement)?
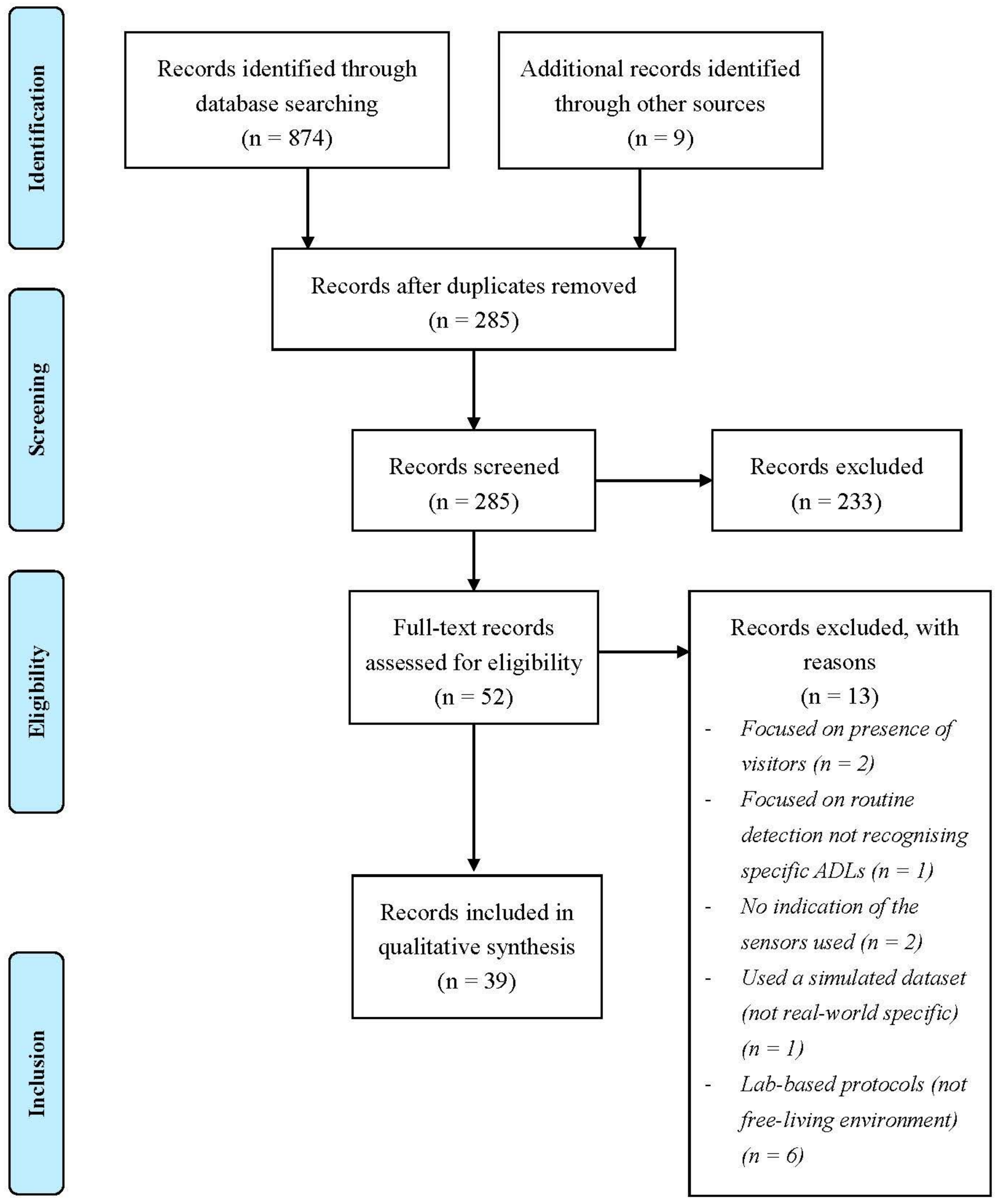
2. Materials and Methods
3. Results
- Environmental + wearable (n = 1): systems using a combination of body-worn and environmentally based technology [39].

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| System Category | Technology Combination | Reference | Year | Total Number of ADL Recognised | Bed Usage | Dressing | Feeding | Grooming | Household | Medicine | Mobility | Recreation | Sleep | Social Interaction | Stair Usage | Toileting | Transferring | TV Usage |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Environmental Only | Depth camera | [53,54] | 5 | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||
| [53] | 2014 | 3 | ✓ | ✓ | ✓ | |||||||||||||
| [54] | 2015 | 4 | ✓ | ✓ | ✓ | ✓ | ||||||||||||
| RFID Tag | [24] | 2012 | 8 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||
| Motion | [10,55,56,57,58] | 11 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||
| [55] | 2008 | 6 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||
| [56] | 2008 | 5 | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||||
| [57] | 2010 | 6 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||
| [58] | 2014 | 2 | ✓ | ✓ | ||||||||||||||
| [10] | 2018 | 7 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||
| Power consumption | [51] | 2011 | 4 | ✓ | ✓ | ✓ | ✓ | |||||||||||
| Video Camera | [23] | 2016 | 8 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||
| Door + Motion | [41,43,45,48,61,64] | 11 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||
| [45] | 2004 | 3 | ✓ | ✓ | ✓ | |||||||||||||
| [61] | 2015 | 9 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||
| [48] | 2017 | 3 | ✓ | ✓ | ✓ | |||||||||||||
| [64] | 2017 | 4 | ✓ | ✓ | ✓ | ✓ | ||||||||||||
| [43] | 2018 | 4 | ✓ | ✓ | ✓ | ✓ | ||||||||||||
| [41] | 2019 | 6 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||
| Force/pressure + Power consumption | [52] | 2013 | 6 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||
| Hydro + Motion | [28] | 2016 | 4 | ✓ | ✓ | ✓ | ✓ | |||||||||||
| Motion + Power Consumption | [37,66] | 7 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||
| [37] | 2012 | 4 | ✓ | ✓ | ✓ | ✓ | ||||||||||||
| [66] | 2019 | 6 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||
| Door + Motion + Power consumption | [47,50,67] | 5 | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||||
| [47] a | 2015 | 5 | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||||
| [50] a | 2019 | 5 | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||||
| [67] | 2020 | 5 | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||||
| Door + Motion + Video Camera | [44] | Unknown | 4 | ✓ | ✓ | ✓ | ✓ | |||||||||||
| Door + Light + Motion + Temperature | [46,63] | 7 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||
| [46] | 2013 | 3 | ✓ | ✓ | ✓ | |||||||||||||
| [63] | 2016 | 6 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||
| Door + Motion + Power consumption + Temperature | [25] | 2014 | 3 | ✓ | ✓ | ✓ | ||||||||||||
| Force / Pressure + Motion + Power consumption + Temperature | [59,65] | 6 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||
| [59] | 2014 | 5 | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||||
| [65] | 2018 | 6 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||
| Accelerometer + Door + Humidity + Light + Motion | [26] | 2011 | 8 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||
| Accelerometer + Humidity + Light + Motion + Temperature | [20,40] | 2014/15 | 7 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||
| Door + Light + Motion + Sound + Temperature | [49] | 2018 | 4 | ✓ | ✓ | ✓ | ✓ | |||||||||||
| Accelerometer + Door + Humidity + Motion + Power consumption + Temperature | [62] | 2015 | 6 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||||
| Door + Grid-eye + Light + Motion + Power consumption + Temperature | [19] | 2019 | 5 | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||
| Accelerometer + Door + Humidity + Motion + Power consumption + Sound + Temperature | [60] | 2014 | 5 | ✓ | ✓ | ✓ | ✓ | ✓ | ||||||||||
| Barometer + Door + Humidity + Light + Motion + Sound + Temperature | [68] | 2020 | 4 | ✓ | ✓ | ✓ | ✓ | |||||||||||
| Wearable Only | Accelerator + Gyroscope | [69] | 2019 | 1 | ✓ | |||||||||||||
| Accelerometer + Altimeter + Barometer + Gyroscope + Light + Temperature | [42] | 2015 | 8 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |||||||
| Environmental and Wearable | Accelerometer + Motion | [39] | 2012 | 6 | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
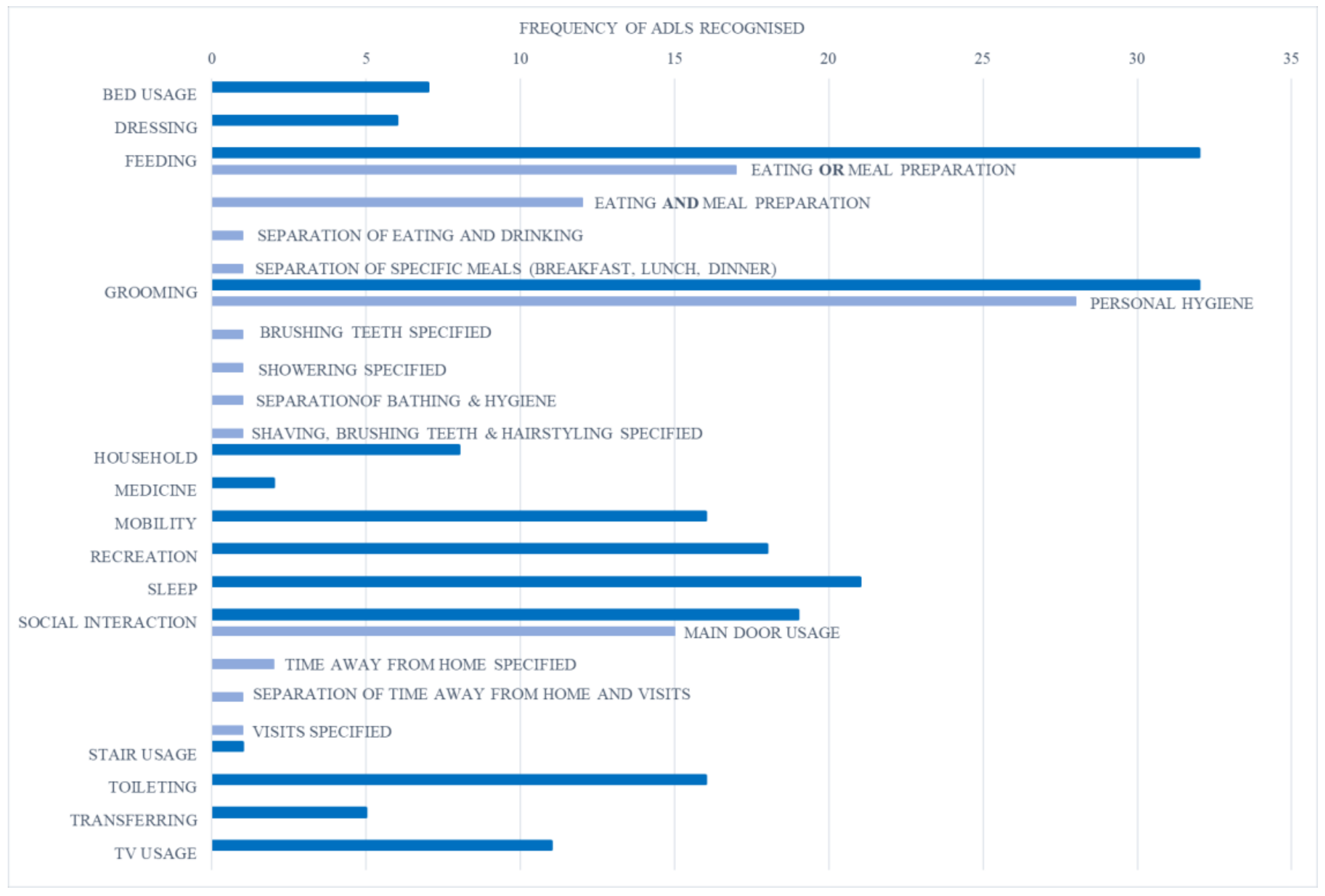
3.1. Recognised ADL
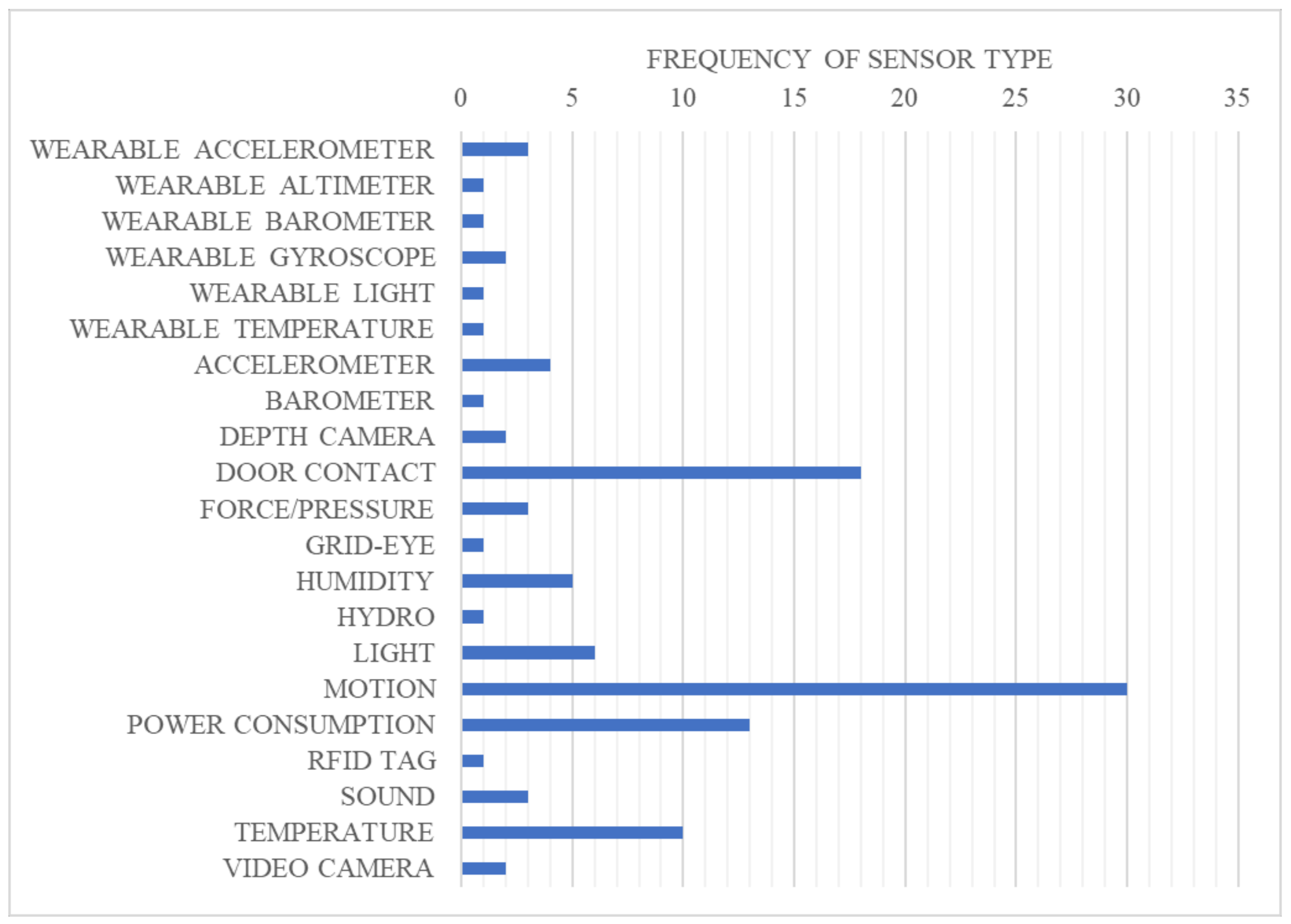
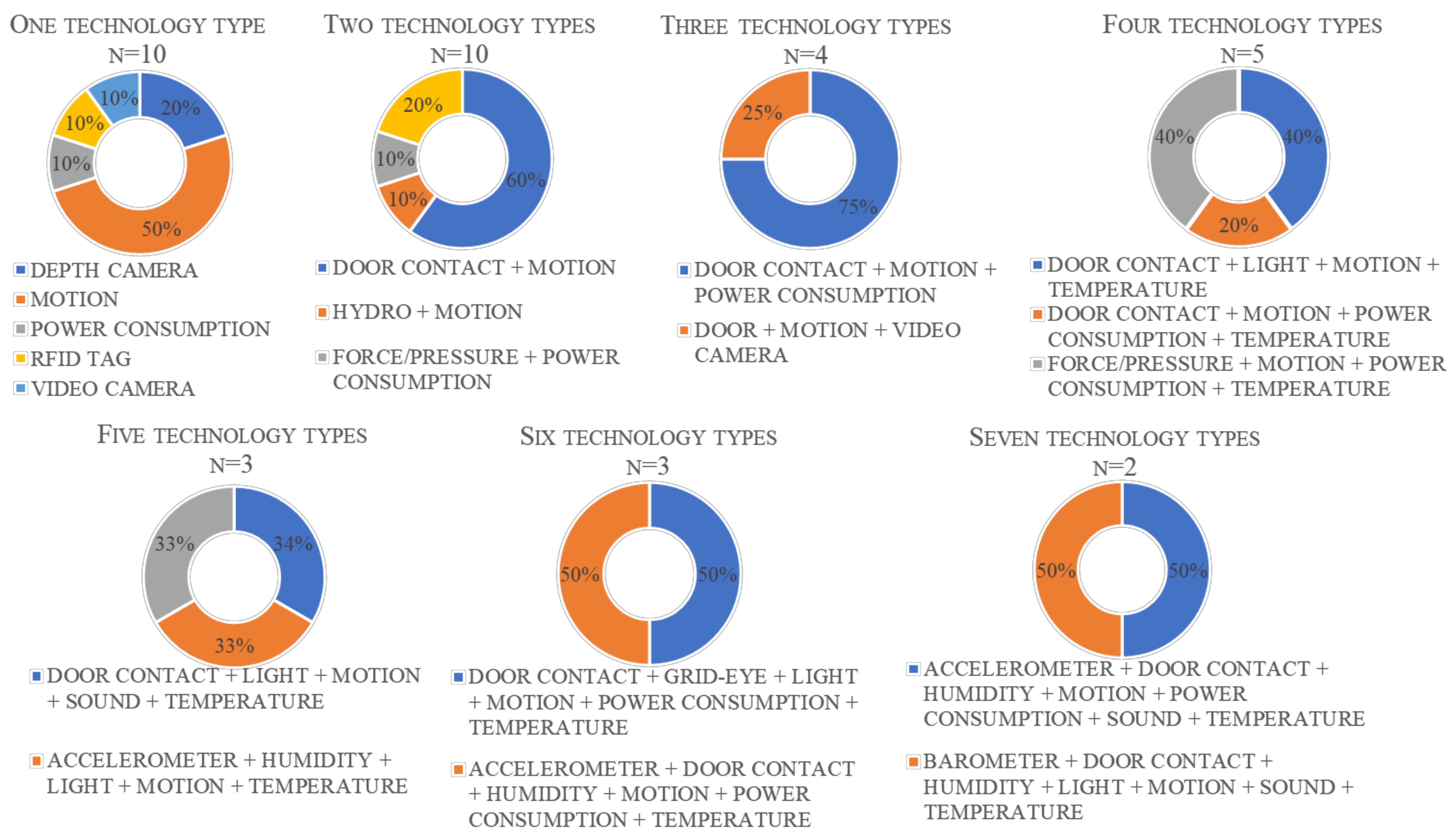
3.2. Identified Technology Types and Recognition Systems
3.3. ADL Recognition Method (Direct/Indirect)
4. Discussion
4.1. ADL Recognised and Compared to Usual Scales
4.2. Sensor Types and Combinations
4.3. ADL Recognition Method
4.4. Limitations and Future Directions
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Coombs, N.; Storey, A.; Giddings, R. Living Longer: Is Age 70 the New Age 65?—Office for National Statistics. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/ageing/articles/livinglongerisage70thenewage65/2019-11-19 (accessed on 20 June 2020).
- Morgan, E. Living Longer and Old-Age Dependency—What Does the Future Hold?—Office for National Statistics. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/ageing/articles/livinglongerandoldagedependencywhatdoesthefuturehold/2019-06-24 (accessed on 20 June 2020).
- Prince, M.J.; Wu, F.; Guo, Y.; Gutierrez Robledo, L.M.; O’Donnell, M.; Sullivan, R.; Yusuf, S. The Burden of Disease in Older People and Implications for Health Policy and Practice. Lancet 2015, 385, 549–562. [Google Scholar] [CrossRef]
- Bloom, D.E.; Chatterji, S.; Kowal, P.; Lloyd-Sherlock, P.; McKee, M.; Rechel, B.; Rosenberg, L.; Smith, J.P. Macroeconomic Implications of Population Ageing and Selected Policy Responses. Lancet 2015, 385, 649–657. [Google Scholar] [CrossRef] [Green Version]
- Sixsmith, A.; Sixsmith, J. Ageing in Place in the United Kingdom. Ageing Int. 2008, 32, 219–235. [Google Scholar] [CrossRef]
- Zhou, W.; Oyegoke, A.S.; Sun, M. Service Planning and Delivery Outcomes of Home Adaptations for Ageing in the UK. J. Hous. Built Environ. 2019, 34, 365–383. [Google Scholar] [CrossRef] [Green Version]
- Van Rensbergen, G.; Pacolet, J. Instrumental Activities of Daily Living (I-ADL) Trigger an Urgent Request for Nursing Home Admission. Arch. Public Health 2012, 70, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vermeulen, J.; Neyens, J.C.; van Rossum, E.; Spreeuwenberg, M.D.; de Witte, L.P. Predicting ADL Disability in Community-Dwelling Elderly People Using Physical Frailty Indicators: A Systematic Review. BMC Geriatr. 2011, 11, 33. [Google Scholar] [CrossRef] [Green Version]
- Katz, S.; Downs, T.D.; Cash, H.R.; Grotz, R.C. Progress in Development of the Index of ADL. Gerontologist 1970, 10, 20–30. [Google Scholar] [CrossRef]
- Aramendi, A.A.; Weakley, A.; Aztiria Goenaga, A.; Schmitter-Edgecombe, M.; Cook, D.J. Automatic Assessment of Functional Health Decline in Older Adults Based on Smart Home Data. J. Biomed. Inform. 2018, 81, 119–130. [Google Scholar] [CrossRef]
- Lawton, M.P.; Brody, E.M. Assessment of Older People: Self-Maintaining and Instrumental Activities of Daily Living. Gerontologist 1969, 8, 179–186. [Google Scholar] [CrossRef]
- Romero-Ayuso, D.; Castillero-Perea, Á.; González, P.; Navarro, E.; Molina-Massó, J.P.; Funes, M.J.; Triviño-Juárez, J.M. Assessment of cognitive instrumental activities of daily living: A systematic review. Disabil. Rehabil. 2020, 1–17. [Google Scholar] [CrossRef]
- Ho, H.K.; Matsubayashi, K.; Wada, T.; Kimura, M.; Kita, T.; Saijoh, K. Factors Associated with ADL Dependence: A Comparative Study of Residential Care Home and Community-Dwelling Elderly in Japan—Ho—2002—Geriatrics & Gerontology International—Wiley Online Library. Available online: https://0-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/abs/10.1046/j.1444-1586.2002.00026.x (accessed on 20 June 2020).
- Rosso, A.L.; Taylor, J.A.; Tabb, L.P.; Michael, Y.L. Mobility, Disability, and Social Engagement in Older Adults. J. Aging Health 2013, 25, 617–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hopman-Rock, M.; van Hirtum, H.; de Vreede, P.; Freiberger, E. Activities of Daily Living in Older Community-Dwelling Persons: A Systematic Review of Psychometric Properties of Instruments. Aging Clin. Exp. Res. 2019, 31, 917–925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartigan, I. A Comparative Review of the Katz ADL and the Barthel Index in Assessing the Activities of Daily Living of Older People. Int. J. Older People Nurs. 2007, 2, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, N.; Metter, E.J.; Lauretani, F.; Bandinelli, S.; Guralnik, J.; Ferrucci, L. Activity Restriction Induced by Fear of Falling and Objective and Subjective Measures of Physical Function: A Prospective Cohort Study. J. Am. Geriatr. Soc. 2008, 56, 615–620. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Bailón, M.; Montoro-Membila, N.; Garcia-Morán, T.; Arnedo-Montoro, M.L.; Funes Molina, M.J. Preliminary cognitive scale of basic and instrumental activities of daily living for dementia and mild cognitive impairment. J. Clin. Exp. Neuropsychol. 2015, 37, 339–353. [Google Scholar] [CrossRef] [PubMed]
- Konios, A.; Jing, Y.; Eastwood, M.; Tan, B. Unifying and Analysing Activities of Daily Living in Extra Care Homes. In Proceedings of the 2018 IEEE 16th Intl Conf on Dependable, Autonomic and Secure Computing, 16th Intl Conf on Pervasive Intelligence and Computing, 4th Intl Conf on Big Data Intelligence and Computing and Cyber Science and Technology Congress(DASC/PiCom/DataCom/CyberSciTech), Athens, Greece, 12–15 August 2018; pp. 474–479. [Google Scholar] [CrossRef]
- Stucki, R.; Urwyler, P.; Rampa, L.; Müri, R.; Mosimann, U.; Nef, T. JMIR—A Web-Based Non-Intrusive Ambient System to Measure and Classify Activities of Daily Living | Stucki | Journal of Medical Internet Research. Available online: https://www.jmir.org/2014/7/e175/?newDesign (accessed on 20 June 2020).
- Van Kasteren, Y.; Bradford, D.; Zhang, Q.; Karunanithi, M.; Ding, H. Understanding Smart Home Sensor Data for Ageing in Place Through Everyday Household Routines: A Mixed Method Case Study. JMIR mHealth uHealth 2017, 5, e52. [Google Scholar] [CrossRef] [PubMed]
- Mlinac, M.E.; Feng, M.C. Assessment of Activities of Daily Living, Self-Care, and Independence. Arch. Clin. Neuropsychol. 2016, 31, 506–516. [Google Scholar] [CrossRef] [Green Version]
- Eldib, M.; Deboeverie, F.; Philips, W.; Aghajan, H. Behavior Analysis for Elderly Care Using a Network of Low-Resolution Visual Sensors. Available online: https://www.spiedigitallibrary.org/journals/Journal-of-Electronic-Imaging/volume-25/issue-4/041003/Behavior-analysis-for-elderly-care-using-a-network-of-low/10.1117/1.JEI.25.4.041003.full (accessed on 20 June 2020).
- Neuhaeuser, J.; Proebstl, D.; D’Angelo, L.T.; Lueth, T.C. First Application of Behavoir Recognition through the Recording of ADL by Radio Modules in a Home—IEEE Conference Publication. Available online: https://0-ieeexplore-ieee-org.brum.beds.ac.uk/abstract/document/6347322 (accessed on 20 June 2020).
- Caroux, L.; Consel, C.; Dupuy, L.; Sauzéon, H. Verification of Daily Activities of Older Adults: A Simple, Non-Intrusive, Low-Cost Approach. In Proceedings of the 16th International ACM SIGACCESS Conference on Computers & accessibility—ASSETS ’14, Rochester, NY, USA, 20–22 October 2014; pp. 43–50. [Google Scholar] [CrossRef] [Green Version]
- Rashidi, P.; Cook, D.J. COM: A Method for Mining and Monitoring Human Activity Patterns in Home-Based Health Monitoring Systems. ACM Trans. Intell. Syst. Technol. 2013, 4, 1–20. [Google Scholar] [CrossRef]
- Rycroft, S.S.; Giovannetti, T.; Divers, R.; Hulswit, J. Sensitive performance-based assessment of everyday action in older and younger adults. Aging Neuropsychol. Cogn. 2018, 25, 259–276. [Google Scholar] [CrossRef]
- Chung, J.; Demiris, G.; Thompson, H.; Chen, K.-Y.; Burr, R.; Patel, S.; Fogarty, J. Feasibility Testing of a Home-Based Sensor System to Monitor Mobility and Daily Activities in Korean American Older Adults—Chung—2017—International Journal of Older People Nursing—Wiley Online Library. Available online: https://0-onlinelibrary-wiley-com.brum.beds.ac.uk/doi/abs/10.1111/opn.12127 (accessed on 20 June 2020).
- Suzman, R.; Beard, J.; Boerma, T.; Chatterji, S. Health in an Ageing World—What Do We Know?—The Lancet. Available online: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(14)61597-X/fulltext (accessed on 20 June 2020).
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping Studies: Advancing the Methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Demiris, G.; Hensel, B.K. Technologies for an Aging Society: A Systematic Review of “Smart Home” Applications. Yearb. Med. Inf. 2008, 17, 33–40. [Google Scholar] [CrossRef] [Green Version]
- Blackman, S.; Matlo, C.; Bobrovitskiy, C.; Waldoch, A.; Fang, M.L.; Jackson, P.; Mihailidis, A.; Nygård, L.; Astell, A.; Sixsmith, A. Ambient Assisted Living Technologies for Aging Well: A Scoping Review. J. Intell. Syst. 2016, 25, 55–69. [Google Scholar] [CrossRef]
- Dasenbrock, L.; Heinks, A.; Schwenk, M.; Bauer, J.M. Technology-Based Measurements for Screening, Monitoring and Preventing Frailty. Z. Gerontol. Geriat. 2016, 49, 581–595. [Google Scholar] [CrossRef]
- De Bruin, E.D.; Hartmann, A.; Uebelhart, D.; Murer, K.; Zijlstra, W. Wearable Systems for Monitoring Mobility-Related Activities in Older People: A Systematic Review—Eling D de Bruin, Antonia Hartmann, Daniel Uebelhart, Kurt Murer, Wiebren Zijlstra. Available online: 2008journals.sagepub.com/doi/abs/10.1177/0269215508090675 (accessed on 20 June 2020).
- Yang, C.-C.; Hsu, Y.-L. Remote Monitoring and Assessment of Daily Activities in the Home Environment. J. Clin. Gerontol. Geriatr. 2012, 3, 97–104. [Google Scholar] [CrossRef] [Green Version]
- Colquhoun, H.L.; Levac, D.; O’Brien, K.K.; Straus, S.; Tricco, A.C.; Perrier, L.; Kastner, M.; Moher, D. Scoping Reviews: Time for Clarity in Definition, Methods, and Reporting. J. Clin. Epidemiol. 2014, 67, 1291–1294. [Google Scholar] [CrossRef]
- Noury, N.; Barralon, P.; Vuillerme, N.; Fleury, A. Fusion of Multiple Sensors Sources in a Smart Home to Detect Scenarios of Activities in Ambient Assisted Living. Int. J. E Health Med. Commun. 2012, 3, 29–44. [Google Scholar] [CrossRef]
- Urwyler, P.; Rampa, L.; Stucki, R.; Büchler, M.; Müri, R.; Mosimann, U.P.; Nef, T. Recognition of Activities of Daily Living in Healthy Subjects Using Two Ad-Hoc Classifiers. Biomed. Eng. Online 2015, 14, 54. [Google Scholar] [CrossRef] [Green Version]
- Son, H.; Kim, H. A Pilot Study to Test the Feasibility of a Home Mobility Monitoring System in Community-Dwelling Older Adults. Int. J. Environ. Res. Public Health 2019, 16, 1512. [Google Scholar] [CrossRef] [Green Version]
- Chernbumroong, S.; Cang, S.; Yu, H. Genetic Algorithm-Based Classifiers Fusion for Multisensor Activity Recognition of Elderly People. IEEE J. Biomed. Health Inf. 2015, 19, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Kaddachi, F. Technological Approach for Early and Unobtrusive Detection of Possible Health Changes toward Better Adaptation of Services for Elderly People; Springer: Berlin/Heidelberg, Germany, 2018; Volume 183, pp. 47–59. [Google Scholar] [CrossRef]
- Mimonitor. Available online: https://www.mimonitor.co.uk/ (accessed on 20 June 2020).
- Just Checking. Available online: https://justchecking.co.uk (accessed on 20 June 2020).
- Canary Care. Available online: https://www.canarycare.co.uk/ (accessed on 20 June 2020).
- MemoHub. Available online: https://memohub.co.uk/ (accessed on 20 June 2020).
- Tec-Angel. Available online: https://www.tec-angel.co.uk/ (accessed on 20 June 2020).
- TextCare. Available online: https://www.textcare.co.uk/ (accessed on 20 June 2020).
- Howz. Available online: https://howz.com/ (accessed on 20 June 2020).
- Noury, N.; Berenguer, M.; Teyssier, H.; Bouzid, M.-J.; Giordani, M. Building an Index of Activity of Inhabitants From Their Activity on the Residential Electrical Power Line. IEEE Trans. Inf. Technol. Biomed. 2011, 15, 758–766. [Google Scholar] [CrossRef] [PubMed]
- Suryadevara, N.K.; Mukhopadhyay, S.C.; Wang, R.; Rayudu, R.K. Forecasting the Behavior of an Elderly Using Wireless Sensors Data in a Smart Home. Eng. Appl. Artif. Intell. 2013, 26, 2641–2652. [Google Scholar] [CrossRef]
- Jalal, A.; Kamal, S.; Kim, D. A Depth Video Sensor-Based Life-Logging Human Activity Recognition System for Elderly Care in Smart Indoor Environments. Sensors 2014, 14, 11735–11759. [Google Scholar] [CrossRef]
- Banerjee, T.; Keller, J.M.; Popescu, M.; Skubic, M. Recognizing Complex Instrumental Activities of Daily Living Using Scene Information and Fuzzy Logic. Comput. Vis. Image Underst. 2015, 140, 68–82. [Google Scholar] [CrossRef]
- Le, X.H.B.; Di Mascolo, M.; Gouin, A.; Noury, N. Health Smart Home for Elders—A Tool for Automatic Recognition of Activities of Daily Living—IEEE Conference Publication. Available online: https://0-ieeexplore-ieee-org.brum.beds.ac.uk/abstract/document/4649914 (accessed on 20 June 2020).
- Virone, G.; Alwan, M.; Dalal, S.; Kell, S.W.; Turner, B.; Stankovic, J.A.; Felder, R. Behavioral Patterns of Older Adults in Assisted Living. IEEE Trans. Inf. Technol. Biomed. 2008, 12, 387–398. [Google Scholar] [CrossRef]
- Franco, C.; Demongeot, J.; Villemazet, C.; Vuillerme, N. Behavioral Telemonitoring of the Elderly at Home: Detection of Nycthemeral Rhythms Drifts from Location Data. In Proceedings of the 2010 IEEE 24th International Conference on Advanced Information Networking and Applications Workshops, Perth, WA, Australia, 20–23 April 2010; pp. 759–766. [Google Scholar] [CrossRef]
- Hajihashemi, Z.; Yefimova, M.; Popescu, M. Detecting Daily Routines of Older Adults Using Sensor Time Series Clustering. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 5912–5915. [Google Scholar] [CrossRef]
- Suryadevara, N.K.; Mukhopadhyay, S.C. Determining Wellness through an Ambient Assisted Living Environment. IEEE Intell. Syst. 2014, 29, 30–37. [Google Scholar] [CrossRef]
- Zhang, Q.; Karunanithi, M.; Bradford, D.; van Kasteren, Y. Activity of Daily Living Assessment through Wireless Sensor Data. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; pp. 1752–1755. [Google Scholar] [CrossRef]
- Nazerfard, E.; Cook, D. CRAFFT: An Activity Prediction Model Based on Bayesian Networks. SpringerLink. Available online: https://0-link-springer-com.brum.beds.ac.uk/article/10.1007/s12652-014-0219-x (accessed on 20 June 2020).
- Yin, J.; Zhang, Q.; Karunanithi, M. Unsupervised Daily Routine and Activity Discovery in Smart Homes. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 5497–5500. [Google Scholar] [CrossRef]
- Dawadi, P.N.; Cook, D.J.; Schmitter-Edgecombe, M. Modeling Patterns of Activities Using Activity Curves. Pervasive Mob. Comput. 2016, 28, 51–68. [Google Scholar] [CrossRef] [Green Version]
- Goonawardene, N.; Toh, X.; Tan, H.-P. Sensor-Driven Detection of Social Isolation in Community-Dwelling Elderly. In Human Aspects of IT for the Aged Population. Applications, Services and Contexts; Zhou, J., Salvendy, G., Eds.; Lecture Notes in Computer Science; Springer International Publishing: Cham, Switzerland, 2017; Volume 10298, pp. 378–392. [Google Scholar] [CrossRef]
- Ghayvat, H.; Mukhopadhyay, S.; Shenjie, B.; Chouhan, A.; Chen, W. Smart Home Based Ambient Assisted Living: Recognition of Anomaly in the Activity of Daily Living for an Elderly Living Alone. In Proceedings of the 2018 IEEE International Instrumentation and Measurement Technology Conference (I2MTC), Houston, TX, USA, 14–17 May 2018; pp. 1–5. [Google Scholar] [CrossRef]
- Honda, Y.; Yamaguchi, H.; Higashino, T. Daily Activity Recognition Based on Markov Logic Network for Elderly Monitoring. In Proceedings of the 2019 16th IEEE Annual Consumer Communications Networking Conference (CCNC), Las Vegas, NV, USA, 11–14 January 2019; pp. 1–6. [Google Scholar] [CrossRef]
- Lussier, M.; Aboujaoudé, A.; Couture, M.; Moreau, M.; Laliberté, C.; Giroux, S.; Pigot, H.; Gaboury, S.; Bouchard, K.; Belchior, P.; et al. Using Ambient Assisted Living to Monitor Older Adults With Alzheimer Disease: Single-Case Study to Validate the Monitoring Report. JMIR Med. Inform. 2020, 8, e20215. [Google Scholar] [CrossRef]
- Matsui, T.; Onishi, K.; Misaki, S.; Fujimoto, M.; Suwa, H.; Yasumoto, K. SALON: Simplified Sensing System for Activity of Daily Living in Ordinary Home. Sensors 2020, 20, 4895. [Google Scholar] [CrossRef]
- Gomes, D.; Mendes-Moreira, J.; Sousa, I.; Silva, J. Eating and Drinking Recognition in Free-Living Conditions for Triggering Smart Reminders. Sensors 2019, 19, 2803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahoney, F.I.; Barthel, D.W. Functional Evaluation: The Barthel Index: A Simple Index of Independence Useful in Scoring Improvement in the Rehabilitation of the Chronically Ill. Md. State Med. J. 1965, 14, 61–65. [Google Scholar] [PubMed]
- Collin, C.; Wade, D.T.; Horne, V. The Barthel ADL Index: A reliability Study: International Disability Studies: Volume 10. Available online: https://0-www-tandfonline-com.brum.beds.ac.uk/doi/abs/10.3109/09638288809164103 (accessed on 20 June 2020).
- Candela, F.; Zucchetti, G.; Magistro, D. Individual Correlates of Autonomy in Activities of Daily Living of Institutionalized Elderly Individuals: An Exploratory Study in a Holistic Perspective. Holist. Nurs. Pract. 2013, 27, 284–291. [Google Scholar] [CrossRef]
- Tural, E.; Lu, D.; Cole, D.A. Factors Predicting Older Adults’ Attitudes toward and Intentions to Use Stair Mobility Assistive Designs at Home. Prev. Med. Rep. 2020, 18, 101082. [Google Scholar] [CrossRef] [PubMed]
- Lindeman, D.A.; Kim, K.K.; Gladstone, C.; Apesoa-Varano, E.C. Technology and Caregiving: Emerging Interventions and Directions for Research. Gerontologist 2020, 60, S41–S49. [Google Scholar] [CrossRef] [PubMed]
- Fischer, B.; Peine, A.; Östlund, B. The Importance of User Involvement: A Systematic Review of Involving Older Users in Technology Design. Gerontologist 2019. [Google Scholar] [CrossRef] [Green Version]
- Merkel, S.; Kucharski, A. Participatory Design in Gerontechnology: A Systematic Literature Review. Gerontologist 2019, 59, e16–e25. [Google Scholar] [CrossRef]
- Sumner, J.; Chong, L.S.; Bundele, A.; Lim, Y.W. Co-Designing Technology for Ageing in Place: A Systematic Review. Gerontologist 2020. [Google Scholar] [CrossRef]




| Inclusion | Exclusion |
|---|---|
|
|
| Property Name | Keywords |
|---|---|
| Population | ag* OR elder* OR older |
| AND | |
| “free living” OR “community dwelling” OR home | |
| Activity | “activities of daily living” OR ADL |
| AND | |
| Measurement | monitor OR assess* OR detect OR measur* OR recogni* |
| AND | |
| Technology | techn* OR wearable OR sens* OR device OR app OR smartphone OR “smart home” OR “human activity recognition” OR HAR |
| Activity | Definition |
|---|---|
| Bed Usage | Time spent in bed, including movements while in bed which can infer sleep quality [26] |
| Dressing | Activity performed in standing posture, in the bedroom or bathroom immediately following getting out of bed or following a visit to the toilet [39] |
| Feeding | Succession of movements performed in a kitchen environment during a reasonable duration and at selected moments in the day, including eating and meal preparation activity [39] |
| Grooming | Activity relating to maintaining personal hygiene (showering, shaving, brushing teeth & styling) [20,40] |
| Household | Any activity relating to household chores, for example laundry or washing up [11] |
| Medicine | Able to manage medication [11] |
| Mobility | Number of activated sensors and total distance covered walking inside the apartment per day [10] |
| Recreation | Sitting at a table or easy chair [20,40] |
| Sleep | Resting at night or napping either in bed or on the couch [40] |
| Social Interaction | Time spent away from the property [41], or the detection of visitors within the home [19] |
| Stair Usage | Walking up or down stairs without falling/tripping [42] |
| Toileting | Spending less than 5 min in a bathroom [23] |
| Transferring | The ability to move oneself from/to a bed or a chair [39] |
| TV Usage | Television is on, usually with a main focus on the TV but can include doing other activities while the television is on [40] |
| Activity | Direct/Indirect/Both | Outcome Measure |
|---|---|---|
| Bed Usage | Direct | Pressure sensors or accelerometers attached to the bed |
| Dressing | Indirect | Room activity and door sensors attached to specific drawers/wardrobes |
| Feeding | Both | Room activity, appliance use, or door sensors attached to cupboards within the kitchen area (inferred activity) Wearable sensor data (direct measure) |
| Grooming | Indirect | Room activity, changes in temperature/humidity, water usage or specific door usage |
| Household | Indirect | Water usage, room activity or appliance usage |
| Medicine | Indirect | Door sensors attached to medicine cabinets |
| Mobility | Both | Room activity (inferred activity) Wearable sensors (direct measure) |
| Recreation | Indirect | Room activity or power consumption |
| Sleep | Indirect | Room presence (but inactivity), typically the living room & bedroom |
| Social Interaction | Indirect | Door sensors attached to the main property entrance |
| Stair Usage | Indirect | Combined wearable sensors |
| Toileting | Indirect | Room activity, specific door usage, water usage or accelerometers attached to the flush mechanism |
| Transferring | Both | Room activity or pressure sensors (indirect) Wearable sensors (direct measure) |
| TV Usage | Direct | Power consumption/smart switch |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Camp, N.; Lewis, M.; Hunter, K.; Johnston, J.; Zecca, M.; Di Nuovo, A.; Magistro, D. Technology Used to Recognize Activities of Daily Living in Community-Dwelling Older Adults. Int. J. Environ. Res. Public Health 2021, 18, 163. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010163
Camp N, Lewis M, Hunter K, Johnston J, Zecca M, Di Nuovo A, Magistro D. Technology Used to Recognize Activities of Daily Living in Community-Dwelling Older Adults. International Journal of Environmental Research and Public Health. 2021; 18(1):163. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010163
Chicago/Turabian StyleCamp, Nicola, Martin Lewis, Kirsty Hunter, Julie Johnston, Massimiliano Zecca, Alessandro Di Nuovo, and Daniele Magistro. 2021. "Technology Used to Recognize Activities of Daily Living in Community-Dwelling Older Adults" International Journal of Environmental Research and Public Health 18, no. 1: 163. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010163