Influence of Public Oral Health Services and Socioeconomic Indicators on the Frequency of Hospitalization and Deaths due to Oral Cancer in Brazil, between 2002–2017


Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miranda-Filho, A.; Bray, F. Global patterns and trends in cancers of the lip, tongue and mouth [published online ahead of print]. Oral Oncol. 2020, 102, 104551. [Google Scholar] [CrossRef] [PubMed]
- INCA. Estimate 2020—Summary of Results and Comments. Available online: https://www.inca.gov.br/estimativa/sintese-de-resultados-e-comentarios (accessed on 24 August 2020).
- Bezerra, N.V.; Leite, K.L.; de Medeiros, M.M.; Martins, M.L.; Cardoso, A.M.; Nonaka, C.F.W.; Padilha, W.W.; Cavalcanti, Y.W. Advanced-stage tongue and mouth floor cancer is related to tobacco and alcohol abuse. J. Public Health 2018, 26, 151–156. [Google Scholar] [CrossRef]
- Conway, D.I.; Purkayastha, M.; Chestnutt, I.G. The changing epidemiology of oral cancer: Definitions, trends, and risk factors. Br. Dent. J. 2018, 225, 867–873. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, I.L.; de Medeiros, J.J.; Rodrigues, L.V.; Valença, A.M.; Lima Neto, E.A. Factors associated with lip and oral cavity cancer. Rev. Bras. Epidemiol. 2015, 18, 618–629. [Google Scholar] [CrossRef] [Green Version]
- Conway, D.I.; Brenner, D.R.; McMahon, A.D.; Macpherson, L.M.; Agudo, A.; Ahrens, W.; Bosetti, C.; Brenner, H.; Castellsague, X.; Chen, C.; et al. Estimating and explaining the effect of education and income on head and neck cancer risk: INHANCE consortium pooled analysis of 31 case-control studies from 27 countries. Int. J. Cancer 2015, 136, 1125–1139. [Google Scholar] [CrossRef] [Green Version]
- da Lins, L.S.S.; Bezerra, N.V.F.; Freire, A.R.; de Almeida, L.D.F.D.; de Lucena, E.H.G.; Cavalcanti, Y.W. Socio-demographic characteristics are related to the advanced clinical stage of oral cancer. Med. Oral Patol Oral y Cir. Bucal. 2019, 24, 759–763. [Google Scholar] [CrossRef]
- Moi, G.P.; Silva, A.M.C.; Galvão, N.D.; de Castro, M.M.; Pereira, A.C. Spatial analysis of the death associated factors due oral cancer in Brazil: An ecological study. BMC Oral Health 2018, 23, 14–22. [Google Scholar] [CrossRef] [Green Version]
- Herrera-Serna, B.Y.; Lara-Carrillo, E.; Toral-Rizo, V.H.; Cristina do, A.R.; Aguilera-Eguía, R.A. Relationship between the Human Development Index and its Components with Oral Cancer in Latin America. J. Epidemiol. Glob. Health 2019, 9, 223–232. [Google Scholar] [CrossRef]
- Chaves, S.C.L.; Almeida, A.M.F.L.; Rossi, T.R.A.; Santana, S.F.; Barros, S.G.; Santos, C.M.L. Oral health policy in Brazil between 2003 and 2014: Scenarios, proposals, actions, and outcomes. Política de Saúde Bucal no Brasil 2003-2014: Cenário, propostas, ações e resultados. Cien Saude Colet. 2017, 22, 1791–1803. [Google Scholar] [CrossRef] [Green Version]
- Department of Primary Care, Department of Health Care, Ministry of Health. National Coordination of Oral Health. National Oral Health Policy Guidelines; Ministério da Saúde: Brasília, Brazil, 2004.
- Cunha, A.R.D.; Prass, T.S.; Hugo, F.N. Mortality from oral and oropharyngeal cancer in Brazil: Impact of the National Oral Health Policy. Cad. Saude Publica 2019, 35, e00014319. [Google Scholar] [CrossRef] [PubMed]
- Campos, G.W.S. Defending the SUS depends on advancing health reform. Interface Commun. Health Educ. 2018, 22, 5–8. [Google Scholar]
- Freire, A.R.; Gomes-Freire, D.E.W.; Pucca, G.A., Jr.; Carrer, F.C.A.; Sousa, S.A.; Lucena, E.H.G.; Cavalcanti, Y.W. Diagnosis of mucosal changes and hospitalized oral cancer patients in Brazil: Influence of socioeconomic factors. Braz Oral Res. 2021, 35, e032. [Google Scholar]
- Raymundo, M.L.; Freire, A.R.; Gomes-Freire, D.E.; Silva, R.O.; Araújo, E.C.; Ishigame, R.T.; Sousa, S.A.; Lucena, E.H.G.; Cavalcanti, Y.W. Trend of hospitalized cases of oral cancer in Brazil and its relationship with oral health coverage in public health system between 2009 and 2017. Med. Oral Patol. Oral Cir. Bucal. 2021, 26, 24009. [Google Scholar]
- Rocha, T.A.H.; Thomaz, E.B.A.F.; da Silva, N.C.; de Sousa Queiroz, R.C.; de Souza, M.R.; Barbosa, A.C.Q.; Thumé, E.; Rocha, J.V.M.; Alvares, V.; de Almeida, D.G.; et al. Oral primary care: An analysis of its impact on the incidence and mortality rates of oral cancer. BMC Cancer 2017, 1, 706–717. [Google Scholar] [CrossRef]
- Medeiros, C.R.G.; Gerhardt, T.E. Avaliação da Rede de Atenção à Saúde de pequenos municípios na ótica das equipes gestoras. Saúde Debate 2015, 39, 160–170. [Google Scholar] [CrossRef] [Green Version]
- Johnson, N.W.; Warnakulasuriya, S.; Gupta, P.C.; Dimba, E.; Chindia, M.; Otoh, E.C.; Sankaranarayanan, R.; Califano, J.; Kowalski, L. Global oral health inequalities in incidence and outcomes for oral cancer: Causes and solutions. Adv. Dent. Res. 2011, 23, 237–246. [Google Scholar] [CrossRef] [Green Version]
- Sakamoto, A.J.; Brizon, V.S.C.; Bulgareli, J.V.; Ambrosano, G.M.B.; Hebling, E. Influence of municipal socioeconomic indices on mortality rates for oral and oropharyngeal cancer in older adults in the State of São Paulo, Brazil. Rev. Bras. Epidemiol. 2019, 21, e190013. [Google Scholar] [CrossRef]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Inter. J. Cancer 2015, 36, E359–E386. [Google Scholar] [CrossRef]
- Antunes, J.L.; Biazevic, M.G.; de Araujo, M.E.; Tomita, N.E.; Chinellato, L.E.; Narvai, P.C. Trends and spatial distribution of oral cancer mortality in São Paulo, Brazil, 1980–1998. Oral Oncol. 2001, 37, 345–350. [Google Scholar] [CrossRef]
- Borges, D.M.L.; Sena, M.F.; Ferreira, M.A.F.; Roncalli, A.G. Mortalidade por câncer de boca e condição sócio-econômica no Brasil. Cad. Saúde Pública 2009, 25, 321–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bezerra, N.V.F.; Leite, K.L.F.; Medeiros, M.M.D.; Martins, M.L.; Cardoso, A.M.R.; Alves, P.N.; Padilha, W.W.; Cavalcanti, Y.W. Impact of the anatomical location, alcoholism and smoking on the prevalence of advanced oral cancer in Brazil. Med. Oral Patol. Oral Cir. Bucal. 2018, 23, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Mattos, G.C.; Ferreira, E.F.; Leite, I.C.; Greco, R.M. A inclusão da equipe de saúde bucal na Estratégia Saúde da Família: Entraves, avanços e desafios [The inclusion of the oral health team in the Brazilian Family Health Strategy: Barriers, advances and challenges]. Cien Saude Colet. 2014, 19, 373–382. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noro, L.R.A.; Landim, J.R.; Martins, M.C.A.; Lima, Y.C.P. The challenge of the approach to oral cancer in primary health care. Ciência Saúde Coletiva 2017, 22, 1579–1587. [Google Scholar] [CrossRef] [Green Version]
- Gómez, I.; Warnakulasuriya, S.; Varela-Centelles, P.I.; López-Jornet, P.; Suárez-Cunqueiro, M.; Diz-Dios, P.; Seoane, J. Is early diagnosis of oral cancer a feasible objective? Who is to blame for diagnostic delay? Oral Dis. 2010, 16, 333–342. [Google Scholar]
- Sousa, F.B.; Freitas e Silva, M.R.; Fernandes, C.P.; Silva, P.G.; Alves, A.P. Oral cancer from a health promotion perspective: Experience of a diagnosis network in Ceará. Braz. Oral Res. 2014, 28, s1–s8. [Google Scholar] [CrossRef] [Green Version]
- Torres-Pereira, C.C.; Angelim-Dias, A.; Melo, N.S.; Lemos, C.A., Jr.; Oliveira, E.M. Abordagem do câncer da boca: Uma estratégia para os níveis primário e secundário de atenção em saúde [Strategies for management of oral cancer in primary and secondary healthcare services]. Cad. Saude Publica 2012, 28, s30–s39. [Google Scholar] [CrossRef] [Green Version]
- Al-Maweri, S.A.; Halboub, E.; Warnakulasuriya, S. Impact of COVID-19 on the early detection of oral cancer: A special emphasis on high risk populations. Oral Oncol. 2020, 106, 104760. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Hospitalized Cases of Oral Cancer | |||||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Median | Max. | Min. | n | % | ||
| Year | 2002 | 0.74 | 7.25 | 0 | 406 | 0 | 4516 | 6.3 |
| 2003 | 0.75 | 6.73 | 0 | 344 | 0 | 4516 | 6.3 | |
| 2004 | 0.86 | 7.49 | 0 | 406 | 0 | 4516 | 6.3 | |
| 2005 | 0.96 | 7.37 | 0 | 398 | 0 | 4516 | 6.3 | |
| 2006 | 0.97 | 6.95 | 0 | 383 | 0 | 4516 | 6.3 | |
| 2007 | 1.06 | 7.07 | 0 | 366 | 0 | 4516 | 6.3 | |
| 2008 | 1.10 | 7.32 | 0 | 408 | 0 | 4516 | 6.3 | |
| 2009 | 1.20 | 8.05 | 0 | 436 | 0 | 4516 | 6.3 | |
| 2010 | 1.27 | 7.33 | 0 | 383 | 0 | 4516 | 6.3 | |
| 2011 | 1.33 | 8.52 | 0 | 477 | 0 | 4516 | 6.3 | |
| 2012 | 1.29 | 8.41 | 0 | 484 | 0 | 4516 | 6.3 | |
| 2013 | 1.35 | 8.27 | 0 | 474 | 0 | 4516 | 6.3 | |
| 2014 | 1.37 | 8.60 | 0 | 478 | 0 | 4516 | 6.3 | |
| 2015 | 1.37 | 7.37 | 0 | 394 | 0 | 4516 | 6.3 | |
| 2016 | 1.16 | 4.62 | 0 | 192 | 0 | 4516 | 6.3 | |
| 2017 | 0.90 | 3.81 | 0 | 149 | 0 | 4516 | 6.3 | |
| Population Size | Up to 30 thousand inhabitants | 0.38 | 0.75 | 0 | 30 | 0 | 57,088 | 79.0 |
| 30 to 50 thousand inhabitants | 1.09 | 1.41 | 1 | 9 | 0 | 6496 | 9.0 | |
| 50 to 100 thousand inhabitants | 1.99 | 2.13 | 1 | 19 | 0 | 4704 | 6.5 | |
| Above 100 thousand inhabitants | 10.54 | 29.31 | 5 | 484 | 0 | 3968 | 5.5 | |
| Municipality’s Human Development Index (MHDI) | Low or very low MHDI (up to 0.59) | 0.33 | 0.67 | 0 | 7 | 0 | 17,520 | 24.2 |
| Average MHDI (between 0.60 and 0.69) | 0.54 | 1.18 | 0 | 30 | 0 | 28,608 | 39.6 | |
| High or very high MHDI (above 0.7) | 2.24 | 12.00 | 0 | 484 | 0 | 26,128 | 36.2 | |
| Gini’s coefficient | Less unequal (<0.4) | 0.48 | 1.04 | 0 | 19 | 0 | 5968 | 8.3 |
| More unequal (>0.4) | 1.16 | 7.62 | 0 | 484 | 0 | 66,288 | 91.7 | |
| Oral Health coverage in primary care | Up to 50% | 1.82 | 10.78 | 0 | 484 | 0 | 32,333 | 44.7 |
| Above 50% | 0.53 | 1.37 | 0 | 50 | 0 | 39,923 | 55.3 | |
| Presence of Dental Specialized Center (DSC) | Without DSC | 0.63 | 2.97 | 0 | 406 | 0 | 64,304 | 89.0 |
| With DSC | 4.96 | 19.94 | 1 | 484 | 0 | 7952 | 11.0 | |
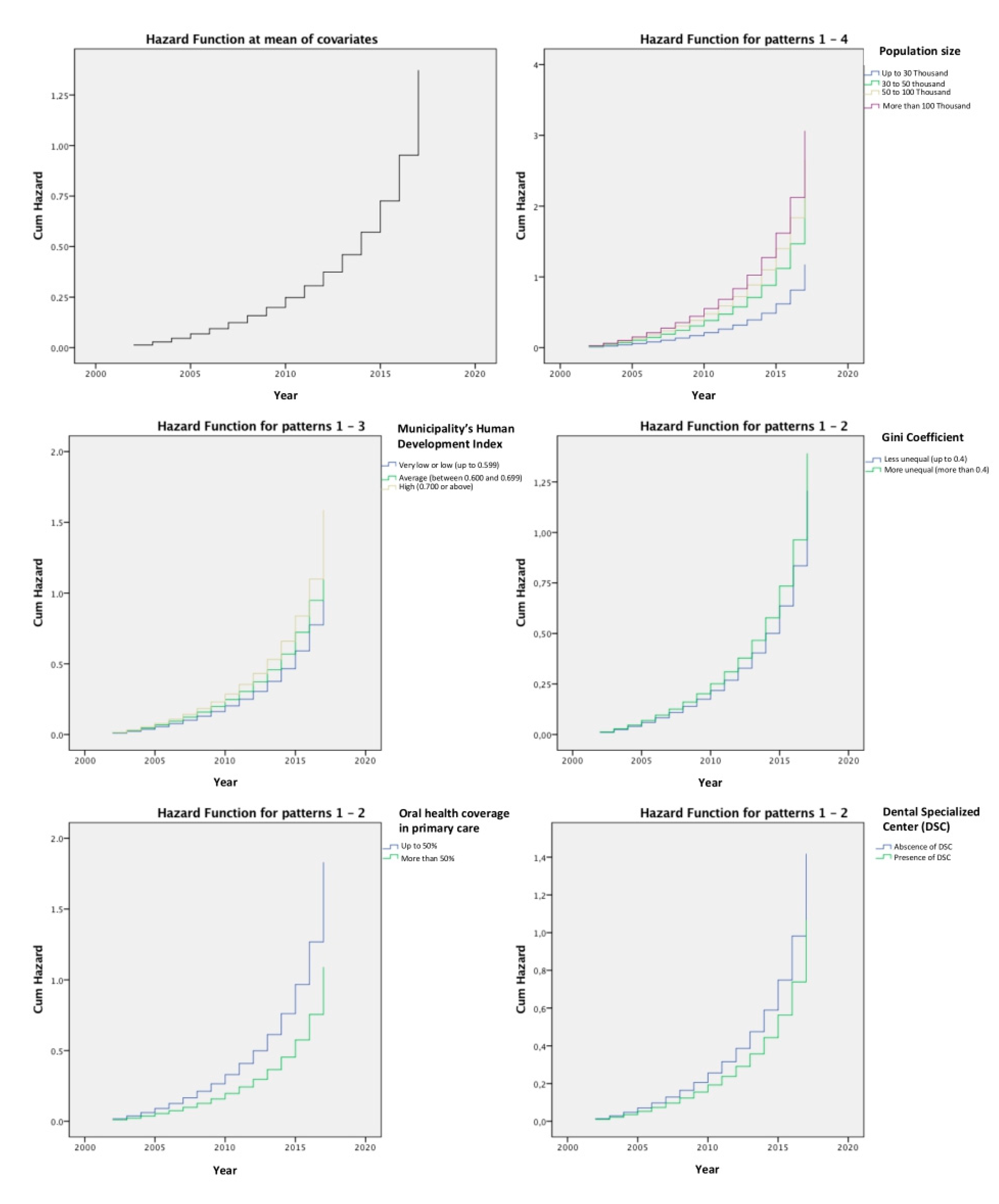
| B | p-Value | HR | 95% CI | ||
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Population size | <0.001 | ||||
| Up to 30 thousand inhabitants | Reference | ||||
| 30 to 50 thousand inhabitants | 0.000 | 0.998 | 1.000 | 0.972 | 1.029 |
| 50 to 100 thousand inhabitants | 0.223 | <0.001 | 1.250 | 1.215 | 1.287 |
| Above 100 thousand inhabitants | 0.369 | <0.001 | 1.446 | 1.400 | 1.492 |
| Municipality’s Human Development Index (MHDI) | <0.001 | ||||
| Low or very low MHDI | Reference | ||||
| Average MHDI | 0.017 | 0.064 | 1.017 | 0.999 | 1.036 |
| High or very high MHDI | 0.166 | <0.001 | 1.180 | 1.158 | 1.203 |
| Gini’s coefficient | <0.001 | ||||
| Less unequal (<0.4) | Reference | ||||
| More unequal (>0.4) | 0.071 | <0.001 | 1.074 | 1.048 | 1.101 |
| Oral Health coverage in primary care | <0.001 | ||||
| Up to 50% | 0.260 | <0.001 | 1.296 | 1.278 | 1.315 |
| Above 50% | Reference | ||||
| Presence of Dental Specialized Center (DSC) | <0.001 | ||||
| Without DSC | 0.142 | <0.001 | 1.153 | 1.132 | 1.174 |
| With DSC | Reference | ||||
| Variables | Number of Deaths due to Oral Cancer | |||||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Median | Max. | Min. | n | % | ||
| Population Size | Up to 30 thousand inhabitants | 0.51 | 1.01 | 0 | 11.00 | 0 | 3563 | 79.0 |
| 30 to 50 thousand inhabitants | 1.35 | 1.95 | 1.00 | 10.00 | 0 | 406 | 9.0 | |
| 50 to 100 thousand inhabitants | 2.41 | 3.23 | 1.00 | 17.00 | 0 | 294 | 6.5 | |
| Above 100 thousand inhabitants | 14.75 | 40.82 | 5.00 | 484.00 | 0 | 248 | 55.0 | |
| Municipality’s Human Development Index (MHDI) | Low or very low MHDI (up to 0.59) | 0.51 | 0.96 | 0 | 11.00 | 0 | 1092 | 24.2 |
| Average MHDI (between 0.60 and 0.69) | 0.88 | 1.95 | 0 | 28.00 | 0 | 1787 | 39.6 | |
| High or very high MHDI (above 0.7) | 2.82 | 16.70 | 0 | 484.00 | 0 | 1632 | 36.2 | |
| Gini’s coefficient | Less unequal (<0.4) | 0.45 | 1.24 | 0 | 13.00 | 0 | 373 | 8.3 |
| More unequal (>0.4) | 1.59 | 10.62 | 0 | 484.00 | 0 | 4138 | 91.7 | |
| Oral Health coverage in primary care | Up to 50% | 1.70 | 11.04 | 0 | 484.00 | 0 | 3821 | 84.7 |
| Above 50% | 0.34 | 0.88 | 0 | 11.00 | 0 | 690 | 15.3 | |
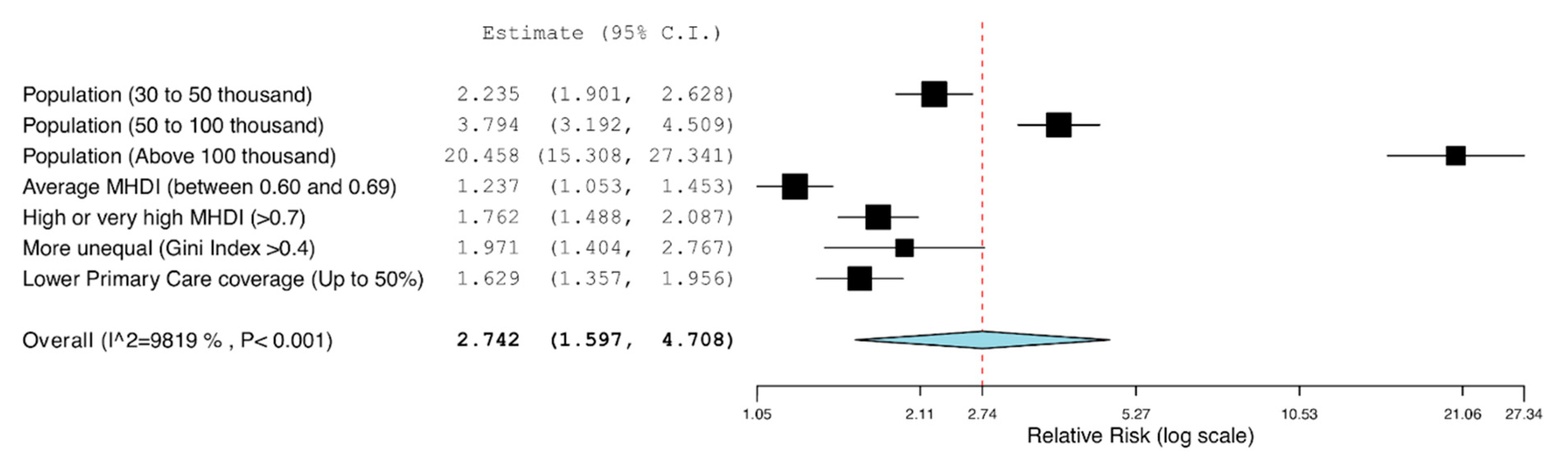
| B | p-Value | IRR | 95% CI | ||
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Population size | <0.001 | ||||
| Up to 30 thousand inhabitants | Reference | ||||
| 30 to 50 thousand inhabitants | 0.804 | <0.001 | 2.235 | 1.900 | 2.628 |
| 50 to 100 thousand inhabitants | 1.333 | <0.001 | 3.794 | 3.192 | 4.509 |
| Above 100 thousand inhabitants | 3.018 | <0.001 | 20.458 | 15.308 | 27.341 |
| Municipality’s Human Development Index (MHDI) | <0.001 | ||||
| Low or very low MHDI | Reference | ||||
| Average MHDI | 0.212 | 0.010 | 1.237 | 1.052 | 1.453 |
| High or very high MHDI | 0.567 | <0.001 | 1.762 | 1.488 | 2.087 |
| Gini’s coefficient | <0.001 | ||||
| Less unequal (<0.4) | Reference | ||||
| More unequal (>0.4) | 0.679 | <0.001 | 1.971 | 1.405 | 2.767 |
| Oral Health coverage in primary care | <0.001 | ||||
| Up to 50% | 0.488 | <0.001 | 1.629 | 1.357 | 1.956 |
| Above 50% | Reference | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Freire, A.R.; Freire, D.E.W.G.; Araújo, E.C.F.d.; de Lucena, E.H.G.; Cavalcanti, Y.W. Influence of Public Oral Health Services and Socioeconomic Indicators on the Frequency of Hospitalization and Deaths due to Oral Cancer in Brazil, between 2002–2017. Int. J. Environ. Res. Public Health 2021, 18, 238. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010238
Freire AR, Freire DEWG, Araújo ECFd, de Lucena EHG, Cavalcanti YW. Influence of Public Oral Health Services and Socioeconomic Indicators on the Frequency of Hospitalization and Deaths due to Oral Cancer in Brazil, between 2002–2017. International Journal of Environmental Research and Public Health. 2021; 18(1):238. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010238
Chicago/Turabian StyleFreire, Aldelany R., Deborah E. W. G. Freire, Elza C. F. de Araújo, Edson H. G. de Lucena, and Yuri W. Cavalcanti. 2021. "Influence of Public Oral Health Services and Socioeconomic Indicators on the Frequency of Hospitalization and Deaths due to Oral Cancer in Brazil, between 2002–2017" International Journal of Environmental Research and Public Health 18, no. 1: 238. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18010238