
The Impact of Health Literacy on Knowledge and Attitudes towards Preventive Strategies against COVID-19: A Cross-Sectional Study



Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Participants’ Characteristics
3.2. Participants’ Knowledge and Attitudes towards Preventive Strategies Related to COVID-19
3.3. Participants’ Knowledge about Symptoms
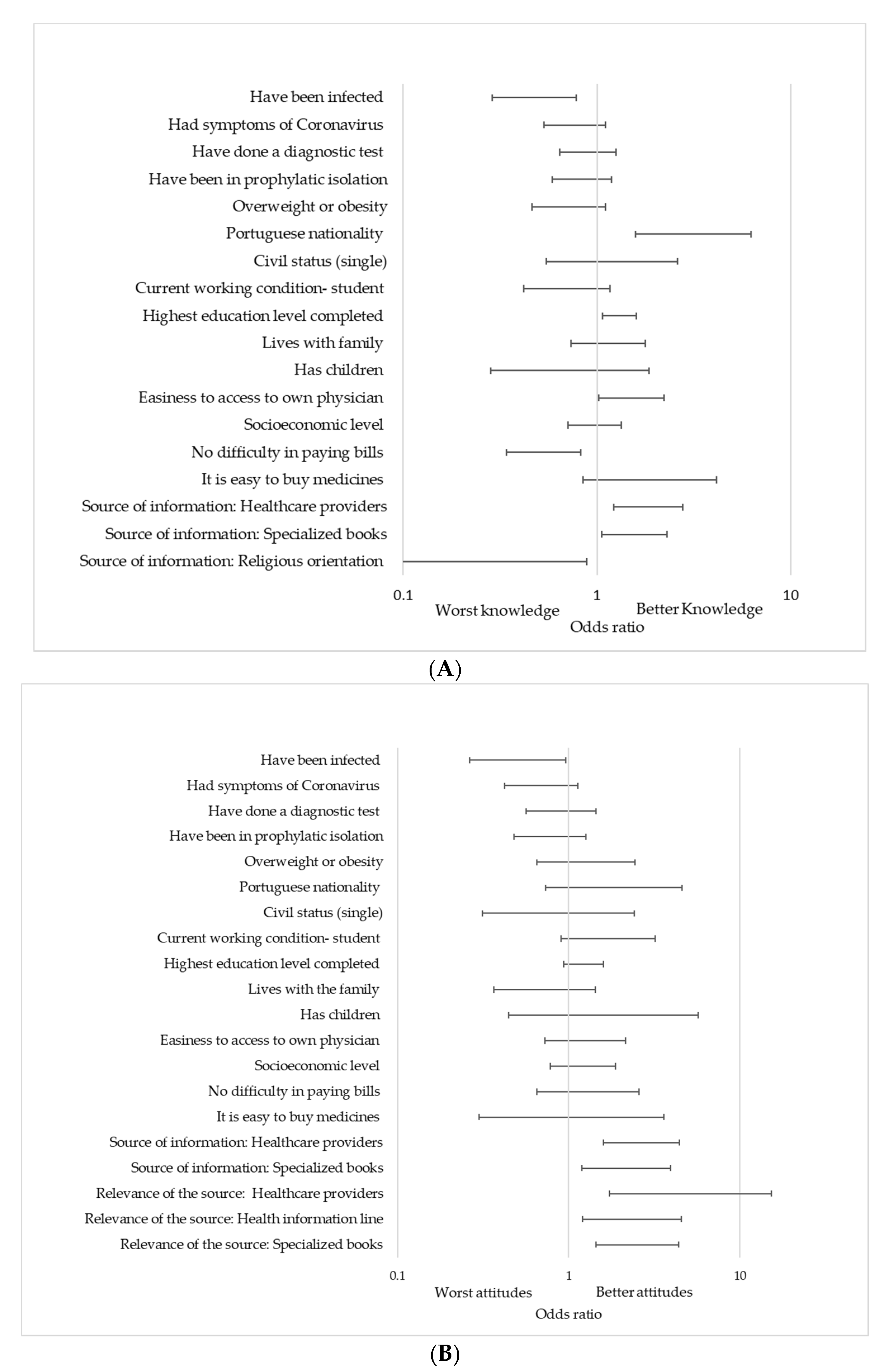
3.4. Logistic Regression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Spring, H. Health literacy and COVID-19. Health Inf. Libr. J. 2020, 37, 171–172. [Google Scholar] [CrossRef]
- Paakkari, L.; Okan, O. COVID-19: Health literacy is an underestimated problem. Lancet Public Health 2020, 5, e249–e250. [Google Scholar] [CrossRef]
- Iezadi, S.; Azami-Aghdash, S.; Ghiasi, A.; Rezapour, A.; Pourasghari, H.; Pashazadeh, F.; Gholipour, K. Effectiveness of the non-pharmaceutical public health interventions against COVID-19; a protocol of a systematic review and realist review. PLoS ONE 2020, 15, e0239554. [Google Scholar] [CrossRef] [PubMed]
- Cowling, B.J.; Ali, S.T.; Ng, T.W.Y.; Tsang, T.K.; Li, J.C.M.; Fong, M.W.; Liao, Q.; Kwan, M.Y.; Lee, S.L.; Chiu, S.S.; et al. Impact assessment of non-pharmaceutical interventions against coronavirus disease 2019 and influenza in Hong Kong: An observational study. Lancet Public Health 2020, 5, e279–e288. [Google Scholar] [CrossRef]
- Zamir, M.; Shah, Z.; Nadeem, F.; Memood, A.; Alrabaiah, H.; Kumam, P. Non Pharmaceutical Interventions for Optimal Control of COVID-19. Comput. Methods Programs Biomed. 2020, 196, 105642. [Google Scholar] [CrossRef] [PubMed]
- Ratzan, S.; Parker, R. Introduction. In National Library of Medicine Current Bibliographies in Medicine: Health Literacy; Selden, C.R., Zorn, M., Ratzan, S., Parker, R.M., Eds.; National Institutes of Health: Bethesda, MD, USA, 2000; pp. v–vii. [Google Scholar]
- Nutbeam, D. Health literacy as a public health goal: A challenge for contemporary health education and communication strategies into the 21st century. Health Promot. Int. 2000, 15, 259–267. [Google Scholar] [CrossRef] [Green Version]
- Berkman, N.D.; Davis, T.C.; McCormack, L. Health Literacy: What Is It? J. Health Commun. 2010, 15, 9–19. [Google Scholar] [CrossRef]
- National Center for Health Statistics (U.S.). Healthy People 2010: Final Review; U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Health Statistics: Hyattsville, MD, USA, 2012.
- Santos, P.; Sá, L.; Couto, L.; Hespanhol, A. Health literacy as a key for effective preventive medicine. Cogent Soc. Sci. 2017, 3, 1407522. [Google Scholar] [CrossRef]
- Hersh, L.; Salzman, B.; Snyderman, D. Health Literacy in Primary Care Practice. Am. Fam. Physician 2015, 92, 118–124. [Google Scholar]
- Sheridan, S.L.; Halpern, D.J.; Viera, A.J.; Berkman, N.D.; Donahue, K.E.; Crotty, K. Interventions for Individuals with Low Health Literacy: A Systematic Review. J. Health Commun. 2011, 16, 30–54. [Google Scholar] [CrossRef]
- Nguyen, H.C.; Nguyen, M.H.; Do, B.N.; Tran, C.Q.; Nguyen, T.T.P.; Pham, K.M.; Pham, L.V.; Tran, K.V.; Duong, T.T.; Tran, T.V.; et al. People with Suspected COVID-19 Symptoms Were More Likely Depressed and Had Lower Health-Related Quality of Life: The Potential Benefit of Health Literacy. J. Clin. Med. 2020, 9, 965. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berkman, N.D.; Sheridan, S.L.; Donahue, K.E.; Halpern, D.J.; Crotty, K. Low health literacy and health outcomes: An updated systematic review. Ann. Intern. Med. 2011, 155, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Bennett, I.M.; Chen, J.; Soroui, J.S.; White, S. The contribution of health literacy to disparities in self-rated health status and preventive health behaviors in older adults. Ann. Fam. Med. 2009, 7, 204–211. [Google Scholar] [CrossRef] [Green Version]
- Abel, T.; McQueen, D. Critical health literacy and the COVID-19 crisis. Health Promot. Int. 2020, 35, 1612–1613. [Google Scholar] [CrossRef]
- Santos, P.; Sá, L.; Couto, L.; Hespanhol, A. Sources of information in health education: A crosssectional study in Portuguese university students. AMJ 2018, 11, 352–360. [Google Scholar] [CrossRef]
- Allcott, H.; Gentzkow, M. Social Media and Fake News in the 2016 Election. J. Econ. Perspect. 2017, 31, 211–236. [Google Scholar] [CrossRef] [Green Version]
- Patil, U.; Kostareva, U.; Hadley, M.; Manganello, J.A.; Okan, O.; Dadaczynski, K.; Massey, P.M.; Agner, J.; Sentell, T. Health Literacy, Digital Health Literacy, and COVID-19 Pandemic Attitudes and Behaviors in U.S. College Students: Implications for Interventions. Int. J. Environ. Res. Public Health 2021, 18, 3301. [Google Scholar] [CrossRef] [PubMed]
- Rosario, R.; Martins, M.R.O.; Augusto, C.; Silva, M.J.; Martins, S.; Duarte, A.; Fronteira, I.; Ramos, N.; Okan, O.; Dadaczynski, K. Associations between COVID-19-Related Digital Health Literacy and Online Information-Seeking Behavior among Portuguese University Students. Int. J. Environ. Res. Public Health 2020, 17, 8987. [Google Scholar] [CrossRef]
- Dadaczynski, K.; Okan, O.; Messer, M.; Leung, A.Y.M.; Rosario, R.; Darlington, E.; Rathmann, K. Digital Health Literacy and Web-Based Information-Seeking Behaviors of University Students in Germany during the COVID-19 Pandemic: Cross-sectional Survey Study. J. Med. Internet Res. 2021, 23, e24097. [Google Scholar] [CrossRef]
- Santos, P.; Hespanhol, A. An ethical view of vaccine refusal. Rev. Port. Med. Geral. Fam. 2013, 29, 328–333. [Google Scholar]
- Santos, P.; Sá, L.; Couto, L.; Hespanhol, A. Literacia em Saúde e Equidade. In Vulnerabilidades & Saúde: Grupos em cena por Visibilidade no Espaço Urbano, 1st ed.; Figueiredo, G.L.A., Martins, C.H.G., Akerman, M., Eds.; HUCITEC: São Paulo, Brazil, 2018; pp. 462–473. [Google Scholar]
- Gautam, V.; Dileepan, S.; Rustagi, N.; Mittal, A.; Patel, M.; Shafi, S.; Thirunavukkarasu, P.; Raghav, P. Health literacy, preventive COVID 19 behaviour and adherence to chronic disease treatment during lockdown among patients registered at primary health facility in urban Jodhpur, Rajasthan. Diabetes Metab. Syndr. 2021, 15, 205–211. [Google Scholar] [CrossRef]
- Weiss, B.D.; Mays, M.Z.; Martz, W.; Castro, K.M.; DeWalt, D.A.; Pignone, M.P.; Mockbee, J.; Hale, F.A. Quick assessment of literacy in primary care: The newest vital sign. Ann. Fam. Med. 2005, 3, 514–522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Correia Martins, A.; Andrade, I.M. Adaptação cultural e validação da versão portuguesa de Newest Vital Sign. Rev. de Enferm. Ref. 2014, IV, 75–84. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Guidelines for the Implementation of Nonpharmaceutical Interventions against COVID-19 in the EU/EEA and the UK. ECDC. Stockholm; 2020; p. 38. Available online: https://www.ecdc.europa.eu/en/publications-data/covid-19-guidelines-non-pharmaceutical-interventions (accessed on 17 May 2021).
- An, L.; Bacon, E.; Hawley, S.; Yang, P.; Russell, D.; Huffman, S.; Resnicow, K. Relationship between Coronavirus-Related eHealth Literacy and COVID-19 Knowledge, Attitudes, and Practices among US Adults: Web-Based Survey Study. J. Med. Internet Res. 2021, 23, e25042. [Google Scholar] [CrossRef] [PubMed]
- Dumitrescu, A.L.; Wagle, M.; Dogaru, B.C.; Manolescu, B. Modeling the theory of planned behavior for intention to improve oral health behaviors: The impact of attitudes, knowledge, and current behavior. J. Oral Sci. 2011, 53, 369–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Liu, Q. Social Media Use, eHealth Literacy, Disease Knowledge, and Preventive Behaviors in the COVID-19 Pandemic: Cross-Sectional Study on Chinese Netizens. J. Med. Internet Res. 2020, 22, e19684. [Google Scholar] [CrossRef]
- Wong, J.Y.H.; Wai, A.K.C.; Zhao, S.; Yip, F.; Lee, J.J.; Wong, C.K.H.; Wang, M.P.; Lam, T.H. Association of Individual Health Literacy with Preventive Behaviours and Family Well-Being during COVID-19 Pandemic: Mediating Role of Family Information Sharing. Int. J. Environ. Res. Public Health 2020, 17, 8838. [Google Scholar] [CrossRef] [PubMed]
- McCaffery, K.J.; Dodd, R.H.; Cvejic, E.; Ayrek, J.; Batcup, C.; Isautier, J.M.; Copp, T.; Bonner, C.; Pickles, K.; Nickel, B.; et al. Health literacy and disparities in COVID-19-related knowledge, attitudes, beliefs and behaviours in Australia. Public Health Res. Pr. 2020, 30. [Google Scholar] [CrossRef]
- Riiser, K.; Helseth, S.; Haraldstad, K.; Torbjørnsen, A.; Richardsen, K.R. Adolescents’ health literacy, health protective measures, and health-related quality of life during the Covid-19 pandemic. PLoS ONE 2020, 15, e0238161. [Google Scholar] [CrossRef]
- Castro-Sánchez, E.; Chang, P.W.S.; Vila-Candel, R.; Escobedo, A.A.; Holmes, A.H. Health literacy and infectious diseases: Why does it matter? Int. J. Infect. Dis. 2016, 43, 103–110. [Google Scholar] [CrossRef] [Green Version]
- Pampel, F.C.; Krueger, P.M.; Denney, J.T. Socioeconomic Disparities in Health Behaviors. Annu. Rev. Sociol. 2010, 36, 349–370. [Google Scholar] [CrossRef] [Green Version]
- Chen, X.; Chen, H. Differences in Preventive Behaviors of COVID-19 between Urban and Rural Residents: Lessons Learned from A Cross-Sectional Study in China. Int. J. Environ. Res. Public Health 2020, 17, 4437. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.J.; Dong, X.; Cao, Y.Y.; Yuan, Y.D.; Yang, Y.B.; Yan, Y.Q.; Akdis, C.A.; Gao, Y.D. Clinical characteristics of 140 patients infected with SARS-CoV-2 in Wuhan, China. Allergy 2020, 75, 1730–1741. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Wu, X.; Zeng, W.; Guo, D.; Fang, Z.; Chen, L.; Huang, H.; Li, C. Chest CT Findings in Patients With Coronavirus Disease 2019 and Its Relationship With Clinical Features. Investig. Radiol. 2020, 55, 257–261. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.-J.; Ni, Z.-Y.; Hu, Y.; Liang, W.-H.; Ou, C.-Q.; He, J.-X.; Liu, L.; Shan, H.; Lei, C.-L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Paiva, D.; Silva, S.; Severo, M.; Moura-Ferreira, P.; Lunet, N.; Azevedo, A. Limited Health Literacy in Portugal Assessed with the Newest Vital Sign. Acta Med. Port. 2017, 30, 861–869. [Google Scholar] [CrossRef] [Green Version]
- Sørensen, K.; Pelikan, J.M.; Röthlin, F.; Ganahl, K.; Slonska, Z.; Doyle, G.; Fullam, J.; Kondilis, B.; Agrafiotis, D.; Uiters, E.; et al. Health literacy in Europe: Comparative results of the European health literacy survey (HLS-EU). Eur. J. Public Health 2015, 25, 1053–1058. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paiva, D.; Azevedo, A.; Lunet, N.; Ferreira, P.M.; Barros, H.; Silva, S. Medição da literacia em saúde individual: O Newest Vital Sign. In A Informação Sobre Saúde dos Portugueses: Fontes, Conhecimentos e Comportamentos; Ferreira, P.M., Lunet, N., Silva, S., Eds.; Associação Para Investigação e Desenvolvimento da Faculdade de Medicina de Lisboa: Lisboa, Portugal, 2017; pp. 73–82. [Google Scholar]
- Dewalt, D.A.; Berkman, N.D.; Sheridan, S.; Lohr, K.N.; Pignone, M.P. Literacy and health outcomes: A systematic review of the literature. J. Gen. Intern. Med. 2004, 19, 1228–1239. [Google Scholar] [CrossRef] [PubMed]
- Brors, G.; Norman, C.D.; Norekval, T.M. Accelerated importance of eHealth literacy in the COVID-19 outbreak and beyond. Eur. J. Cardiovasc. Nurs. J. Work. Group Cardiovasc. Nurs. Eur. Soc. Cardiol. 2020, 19, 458–461. [Google Scholar] [CrossRef] [PubMed]
- Brar Prayaga, R.; Prayaga, R.S. Mobile Fotonovelas within a Text Message Outreach: An Innovative Tool to Build Health Literacy and Influence Behaviors in Response to the COVID-19 Pandemic. JMIR mHealth uHealth 2020, 8, e19529. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | n = 871 (%) |
|---|---|
| Gender | |
| Female | 665 (76.3%) |
| Male | 206 (23.7%) |
| Mean age (SD) | 23.9 (±7.0) |
| Practice or education in health | 253 (29.0%) |
| Overweight/Obesity | 111 (12.7%)/28 (3.2%) |
| Had symptoms of Coronavirus | 225 (25.8%) |
| Have been infected | 83 (9.5%) |
| Have been in prophylactic isolation | 270 (31.0%) |
| Have taken a diagnostic test | 428 (49.1%) |
| Nationality | |
| Portuguese | 827 (94.9%) |
| Other | 43 (4.9%) |
| Do not know/did not answer | 1 (0.1%) |
| Civil status | |
| Single | 781 (89.7%) |
| Married | 78 (9.0%) |
| Other | 7 (0.8%) |
| Do not know/did not answer | 5 (0.6%) |
| Family situation | |
| Lives alone | 28 (3.2%) |
| Lives with the household | 717 (82.3%) |
| Lives away from home | 119 (13.7%) |
| Do not know/did not answer | 7 (0.8%) |
| Highest education level completed | |
| Upper secondary education | 440 (50.5%) |
| Bachelor | 205 (23.5%) |
| Post-graduation | 221 (25.3%) |
| Do not know/did not answer | 5 (0.6%) |
| Current working condition | |
| Student | 663 (76.1%) |
| Student workers (paid or unpaid) | 180 (20.7%) |
| Other | 25 (2.8%) |
| Do not know/did not answer | 3 (0.3%) |
| Difficulty in paying bills at the end of the month (during the past 12 months) | |
| Most times and sometimes | 136 (15.6%) |
| Almost never and never | 619 (71.1%) |
| Do not know/did not answer | 116 (13.3%) |
| Easiness in buying medicines | |
| Very easy and easy | 772 (88.6%) |
| Difficult and very difficult | 33 (3.7%) |
| Do not know/did not answer | 66 (7.6%) |
| Easiness to access to own physician | |
| Very easy and easy | 564 (64.8%) |
| Difficult and very difficult | 216 (24.8%) |
| Do not know/did not answer | 91 (10.4%) |
| Socioeconomic level (self-perception) | |
| Low | 25 (2.9%) |
| Middle | 488 (56%) |
| High | 332 (38.1%) |
| Did not answer | 26 (3%) |
| % | 95%CI | |
|---|---|---|
| (A) Knowledge | ||
| The minimum distance required to ensure a safe contact is 2 m. | 89.4 | 87.4–91.4 |
| The use of a visor replaces the use of a mask. | 81.2 | 78.6–83.8 |
| There is a proven benefit in the use of gloves. | 44.5 | 41.2–47.8 |
| There is a proven benefit in wearing a mask. | 97.5 | 96.5–98.5 |
| Hand washing/disinfection should be a frequent practice in everyday life. | 99.3 | 98.8–99.9 |
| We must avoid contact of the hands with the respiratory tract. | 97.9 | 96.9–98.9 |
| (B) Attitudes | ||
| Do you maintain the recommended social distance? | 91.6 | 89.8–93.4 |
| Do you wear gloves? | 89.8 | 87.8–91.8 |
| Do you wear a mask indoors? | 98.9 | 98.2–99.6 |
| Do you wear a mask outdoors? | 94.9 | 93.4–96.4 |
| Do you wash your hands? | 97.2 | 96.1–98.3 |
| Do you avoid contact of the hands with the respiratory tract? | 81.2 | 78.6–83.8 |
| Do you adopt respiratory hygiene measures? | 94.7 | 93.2–96.2 |
| (A) Knowledge | (B) Attitudes | |||||
|---|---|---|---|---|---|---|
| OR | 95%CI | p | OR | 95%CI | p | |
| Total NVS Score | 1.141 | 0.981–1.326 | 0.086 | 1.212 | 1.002–1.467 | 0.048 |
| Gender | 0.579 | 0.401–0.835 | 0.003 | 0.541 | 0.333–0.879 | 0.013 |
| Practice or formation in health | 1.705 | 1.134–2.562 | 0.010 | 3.974 | 1.873–8.429 | <0.001 |
| Age | 1.009 | 0.984–1.034 | 0.492 | 0.991 | 0.962–1.022 | 0.573 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva, M.J.; Santos, P. The Impact of Health Literacy on Knowledge and Attitudes towards Preventive Strategies against COVID-19: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 5421. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105421
Silva MJ, Santos P. The Impact of Health Literacy on Knowledge and Attitudes towards Preventive Strategies against COVID-19: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(10):5421. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105421
Chicago/Turabian StyleSilva, Maria João, and Paulo Santos. 2021. "The Impact of Health Literacy on Knowledge and Attitudes towards Preventive Strategies against COVID-19: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 10: 5421. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18105421