
The Influence of Kinesio Tape and an Ankle Brace on the Lower Extremity Joint Motion in Fatigued, Unstable Ankles during a Lateral Drop Landing



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
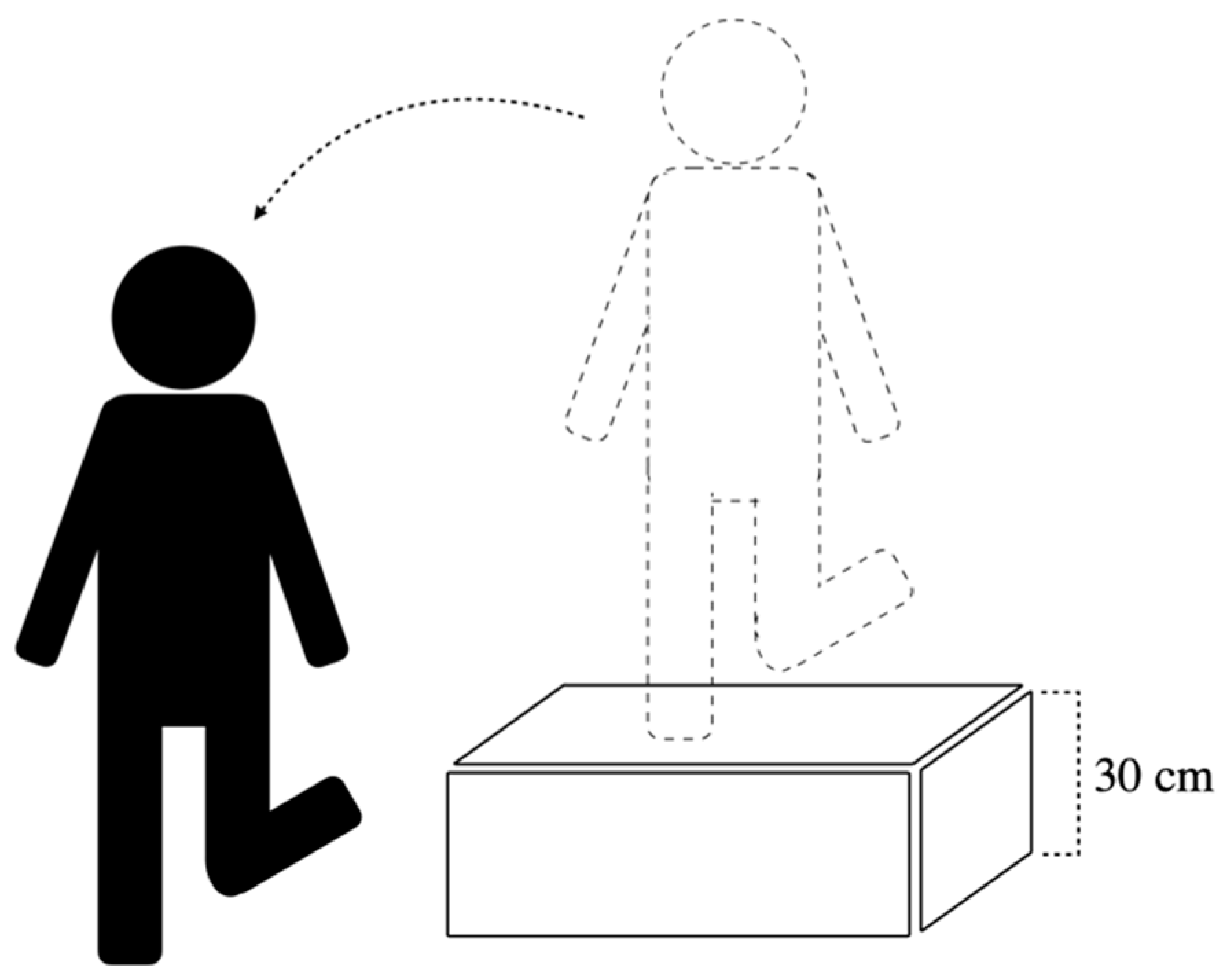
2.2. Experimental Procedure
2.3. Outcome Measures
2.4. Data Analysis
3. Results
3.1. Maximal Joint Angle
3.2. Range of Joint Angle
3.3. The COM Range
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Freeman, M.A.; Dean, M.R.; Hanham, I.W. The etiology and prevention of functional instability of the foot. J. Bone Joint Surg. Br. 1965, 47, 678–685. [Google Scholar] [CrossRef]
- Tropp, H.; Odenrick, P.; Gillquist, J. Stabilometry recordings in functional and mechanical instability of the ankle joint. Int. J. Sports Med. 1985, 6, 180–182. [Google Scholar] [CrossRef]
- Gabbett, T.J. Incidence, site, and nature of injuries in amateur rugby league over three consecutive seasons. Br. J. Sports Med. 2000, 34, 98–103. [Google Scholar] [CrossRef] [Green Version]
- Pinto, M.; Kuhn, J.E.; Greenfield, M.L.; Hawkins, R.J. Prospective Analysis of Ice Hockey Injuries at the Junior A Level over the Course of One Season. Clin. J. Sport Med. 1999, 9, 70–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woods, C.; Hawkins, R.; Hulse, M.; Hodson, A. The Football Association Medical Research Programme: An audit of injuries in professional football: An analysis of ankle sprains. Br. J. Sports Med. 2003, 37, 233–288. [Google Scholar] [CrossRef] [Green Version]
- Neptune, R.R.; Zajac, F.E.; Kautz, S.A. Muscle force redistributes segmental power for body progression during walking. Gait Posture 2004, 19, 194–205. [Google Scholar] [CrossRef] [Green Version]
- Neptune, R.R.; Kautz, S.A.; Zajac, F.E. Contributions of the individual ankle plantar flexors to support, forward progression and swing initiation during walking. J. Biomech. 2001, 34, 1387–1398. [Google Scholar] [CrossRef]
- Neptune, R.R.; Sasaki, K. Ankle plantar flexor force production is an important determinant of the preferred walk-to-run transition speed. J. Exp. Biol. 2005, 208, 799–808. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brazen, D.M.; Todd, M.K.; Ambegaonkar, J.P.; Wunderlich, R.; Peterson, C. The effect of fatigue on landing biomechanics in single-leg drop landings. Clin. J. Sport Med. 2010, 20, 286–292. [Google Scholar] [CrossRef]
- Orishimo, K.F.; Kremenic, I.J. Effect of fatigue on single-leg hop landing biomechanics. J. Appl. Biomech. 2006, 22, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Parijat, P.; Lockhart, T.E. Effects of quadriceps fatigue on the biomechanics of gait and slip propensity. Gait Posture 2008, 28, 568–573. [Google Scholar] [CrossRef] [Green Version]
- Gribble, P.A.; Hertel, J.; Denegar, C.R.; Buckley, W.E. The Effects of Fatigue and Chronic Ankle Instability on Dynamic Postural Control. J. Athl. Train. 2004, 39, 321–329. [Google Scholar]
- Briem, K. Effects of kinesio tape compared with nonelastic sports tape and the untaped ankle during a sudden inversion perturbation in male athletes. J. Orthop. Sports Phys. Ther. 2011, 41, 328. [Google Scholar] [CrossRef] [Green Version]
- Cordova, M.L. Effects of ankle support on lower-extremity functional performance: A meta-analysis. Med. Sci. Sports Exerc. 2005, 37, 635. [Google Scholar] [CrossRef] [PubMed]
- Simon, J.; Garcia, W.; Docherty, C.L. The effect of kinesio tape on force sense in people with functional ankle instability. Clin. J. Sport Med. 2014, 24, 289–294. [Google Scholar] [CrossRef]
- Sitler, M.R.; Horodyski, M. Effectiveness of prophylactic ankle stabilisers for prevention of ankle injuries. Sports Med. 1995, 20, 53–57. [Google Scholar] [CrossRef] [PubMed]
- Cordova, M.; Ingersoll, C.; LeBlanc, M. Influence of ankle support on joint range of motion before and after exercise: A meta-analysis. J. Orthop. Sports Phys. Ther. 2000, 30, 170–177. [Google Scholar] [CrossRef] [Green Version]
- Cordova, M.L.; Ingersoll, C.D. Peroneus longus stretch reflex amplitude increases after ankle brace application. Br. J. Sports Med. 2003, 37, 258–262. [Google Scholar] [CrossRef] [Green Version]
- Babins, E.M. Lace-up ankle braces reduced acute ankle injuries in high school basketball players. Clin. J. Sport Med. 2012, 22, 379–380. [Google Scholar] [CrossRef] [PubMed]
- Hoch, M.C.; Staton, G.S.; McKeon, J.M.M.; Mattacola, C.G.; McKeon, P.O. Dorsiflexion and dynamic postural control deficits are present in those with chronic ankle instability. J. Sci. Med. Sport 2012, 15, 574–579. [Google Scholar] [CrossRef]
- Hoch, M.C.; Farwell, K.E.; Gaven, S.L.; Weinhandl, J.T. Weight-Bearing Dorsiflexion Range of Motion and Landing Biomechanics in Individuals with Chronic Ankle Instability. J. Athl. Train. 2015, 50, 833–839. [Google Scholar] [CrossRef] [Green Version]
- Hiller, C.E.; Refshauge, K.M.; Bundy, A.C.; Herbert, R.D.; Kilbreath, S.L. The Cumberland ankle instability tool: A report of validity and reliability testing. Arch. Phys. Med. Rehabil. 2006, 87, 1235–1241. [Google Scholar] [CrossRef]
- Rodacki, A.F.; Fowler, N.E.; Bennet, S. Multi-segment coordination: Fatigue effects. Med. Sci. Sports Exerc. 2001, 33, 1157–1167. [Google Scholar] [CrossRef]
- Borg, G. Perceived exertion as an indicator of somatic stress. Scand. J. Rehabil. Med. 1970, 2, 92–98. [Google Scholar] [PubMed]
- Thomasson, M.L.; Comfort, P. Occurrence of fatigue during sets of static squat jumps performed at a variety of loads. J. Strength Cond. Res. 2012, 26, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-C.; Chen, S.-J.; Lee, W.-C.; Lin, C.-F. Effects of Different Ankle Supports on the Single-Leg Lateral Drop Landing Following Muscle Fatigue in Athletes with Functional Ankle Instability. Int. J. Environ. Res. Public Health 2020, 17, 3438. [Google Scholar] [CrossRef]
- Rowley, K.M.; Richards, J.G. Increasing plantarflexion angle during landing reduces vertical ground reaction forces, loading rates and the hip’s contribution to support moment within participants. J. Sports Sci. 2015, 33, 1–10. [Google Scholar] [CrossRef]
- Brown, C.; Padua, D.; Marshall, S.W.; Guskiewicz, K. Individuals with mechanical ankle instability exhibit different motion patterns than those with functional ankle instability and ankle sprain copers. Clin. Biomech. 2008, 23, 822–831. [Google Scholar] [CrossRef]
- Fox, J.; Docherty, C.L.; Schrader, J.; Applegate, T. Eccentric Plantar-Flexor Torque Deficits in Participants with Functional Ankle Instability. J. Athl. Train. 2008, 43, 51–54. [Google Scholar] [CrossRef] [Green Version]
- Yamaguchi, G.T.; Sawa, A.G.; Morgan, D.W.; Fessler, M.J.; Winter, J.M. A.G.;Morgan, D.W.; Fessler, M.J.; Winter, J.M. A survey of human musculotendon actuator parameters. In Multiple muscle systems: Biomechanics and movement organization; Springer: New York, NY, USA, 1990; pp. 717–773. [Google Scholar]
- Son, S.J.; Kim, H.; Seeley, M.K.; Hopkins, J.T. Movement Strategies among Groups of Chronic Ankle Instability, Coper, and Control. Med. Sci. Sports Exerc. 2017, 49, 1649. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Son, S.J.; Seeley, M.K.; Hopkins, J.T. Kinetic Compensations due to Chronic Ankle Instability during Landing and Jumping. Med. Sci. Sports Exerc. 2018, 50, 308–317. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Bates, B.; Dufek, J. Contributions of lower extremity joints to energy dissipation during landings. Med. Sci. Sports Exerc. 2000, 32, 812–819. [Google Scholar] [CrossRef]
- Simpson, K.J.; Yom, J.P.; Fu, Y.C.; Arnett, S.W.; O’Rourke, S.; Brown, C.N. Does wearing a prophylactic ankle brace during drop landings affect lower extremity kinematics and ground reaction forces? J. Appl. Biomech. 2013, 29, 205–213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, T.; Tanaka, M.; Shida, M. Intrinsic Risk Factors of Lateral Ankle Sprain: A Systematic Review and Meta-analysis. Sports Health 2016, 8, 190–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panagiotakis, E.; Mok, K.M.; Fong, D.T.; Bull, A.M.J. Biomechanical analysis of ankle ligamentous sprain injury cases from televised basketball games: Understanding when, how and why ligament failure occurs. J. Sci. Med. Sport 2017, 20, 1057–1061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ha, S.C.; Fong, D.T.; Chan, K.M. Review of ankle inversion sprain simulators in the biomechanics laboratory. Asia Pac. J. Sports Med. Arthrosc. Rehabil. Technol. 2015, 2, 114–121. [Google Scholar] [CrossRef] [Green Version]
- Gehring, D.; Wissler, S.; Lohrer, H.; Nauck, T.; Gollhofer, A. Expecting ankle tilts and wearing an ankle brace influence joint control in an imitated ankle sprain mechanism during walking. Gait Posture 2014, 39, 894–898. [Google Scholar] [CrossRef]
- Doherty, C.; Bleakley, C.; Hertel, J.; Caulfield, B.; Ryan, J.; Sweeney, K.; Patterson, M.R.; Delahunt, E. Coordination and Symmetry Patterns During the Drop Vertical Jump in People with Chronic Ankle Instability and Lateral Ankle Sprain Copers. Phys. Ther. 2016, 9, 1152–1161. [Google Scholar] [CrossRef] [Green Version]
- De Ridder, R.; Willems, T.M.; Vanrenterghem, J.; Roosen, P. Effect of Tape on Dynamic Postural Stability in Subjects with Chronic Ankle Instability. Int. J. Sports Med. 2015, 36, 321–326. [Google Scholar] [CrossRef]
- Juchler, I.; Blasimann, A.; Baur, H.; Radlinger, L. The effect of kinesio tape on neuromuscular activity of peroneus longus. Physiother. Theory Pract. 2016, 32, 124–129. [Google Scholar] [CrossRef]
- El-Gazzar, H.; Akl, A.-R. Influence of Kinesio tape on lower limb muscular activity after knee joint rehabilitation program. Preprint 2020. [Google Scholar] [CrossRef]
- Júnior, M.A.D.L.; De Almeida, M.O.; Santos, R.S.; Civile, V.T.; Costa, L.O.P. Effectiveness of kinesio taping in patients with chronic nonspecific low back pain: A systematic review with meta-analysis. Spine 2019, 44, 68–78. [Google Scholar] [CrossRef]
- González-Iglesias, J.; Fernández-de-Las-Peñas, C.; Cleland, J.A.; Huijbregts, P.; Del Rosario Gutiérrez-Vega, M. Short-term effects of cervical kinesio taping on pain and cervical range of motion in patients with acute whiplash injury: A randomized clinical trial. J. Orthop. Sports Phys. Ther. 2009, 39, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.Y.; Chou, K.Y.; Lin, J.J.; Lin, C.F.; Wang, C.H. Immediate effect of forearm Kinesio taping on maximal grip strength and force sense in healthy collegiate athletes. Phys. Ther. Sport 2010, 11, 122–127. [Google Scholar] [CrossRef]
- Mostafavifar, M.; Wertz, J.; Borchers, J. A systematic review of the effectiveness of kinesio taping for musculoskeletal injury. Phys. Sportsmed. 2012, 40, 33–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyas, S.; Hajj, M.; Bilodeau, M. Influence of ankle plantarflexor fatigue on postural sway, lower limb articular angles, and postural strategies during unipedal quiet standing. Gait Posture 2013, 37, 547–551. [Google Scholar] [CrossRef] [PubMed]
- Gribble, P.A.; Hertel, J. Effect of lower-extremity muscle fatigue on postural control. Arch. Phys. Med. Rehabil. 2004, 85, 589–592. [Google Scholar] [CrossRef]
- Yaggie, J.A.; McGregor, S.J. Effects of isokinetic ankle fatigue on the maintenance of balance and postural limits. Arch. Phys. Med. Rehabil. 2002, 83, 224–228. [Google Scholar] [CrossRef]
- Hertel, J. Functional instability following lateral ankle sprain. Sports Med. 2000, 29, 361–371. [Google Scholar] [CrossRef]
- Hertel, J. Functional anatomy, pathomechanics, and pathophysiology of lateral ankle instability. J. Athl. Train. 2002, 37, 364. [Google Scholar]
- Chou, L.-S.; Kaufman, K.R.; Brey, R.H.; Draganich, L.F. Motion of the whole body’s center of mass when stepping over obstacles of different heights. Gait Posture 2001, 13, 17–26. [Google Scholar] [CrossRef]
- Chou, L.-S.; Kaufman, K.R.; Hahn, M.E.; Brey, R.H. Medio-lateral motion of the center of mass during obstacle crossing distinguishes elderly individuals with imbalance. Gait Posture 2003, 18, 125–133. [Google Scholar] [CrossRef]
- Lee, H.-J.; Chou, L.-S. Detection of gait instability using the center of mass and center of pressure inclination angles. Arch. Phys. Med. Rehabil. 2006, 87, 569–575. [Google Scholar] [CrossRef]
- Mason-Mackay, A.R.; Whatman, C.; Reid, D. The effect of reduced ankle dorsiflexion on lower extremity mechanics during landing: A systematic review. J. Sci. Med. Sport 2017, 20, 451–458. [Google Scholar] [CrossRef]
- Tweed, J.; Campbell, J.; Avil, S. Biomechanical Risk Factors in the Development of Medial Tibial Stress Syndrome in Distance Runners. J. Am. Podiatr. Med. Assoc. 2008, 98, 436–444. [Google Scholar] [CrossRef]
- Mauntel, T.C.; Begalle, R.L.; Cram, T.R.; Frank, B.S.; Hirth, C.J.; Blackburn, T.; Padua, D.A. The effects of lower extremity muscle activation and passive range of motion on single leg squat performance. J. Strength Cond. Res. 2013, 27, 1813–1823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macrum, E.; Bell, D.R.; Boling, M.; Lewek, M.; Padua, D. Effect of limiting ankle-dorsiflexion range of motion on lower extremity kinematics and muscle-activation patterns during a squat. J. Sport Rehab. 2012, 21, 144–150. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Cn | AB | KT | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Median | Mean Rank | Mean | Median | Mean Rank | Mean | Median | Mean Rank | K-W Test | |
| Hip | ||||||||||
| Sagittal Flex(+) Ext(-) | 2.79 | 1.25 | 17.27 | 1.58 | 1.60 | 16.64 | 3.97 | 0.46 | 17.09 | 0.987 |
| Frontal ABD(+) ADD(-) | 0.72 | −0.11 | 23.18 | −3.26 | −2.89 a | 12.27 | −2.47 | −1.67 | 15.55 | 0.025 * |
| Transverse ER(+) IR(-) | 0.09 | −0.27 | 18.45 | −1.67 | 0.29 | 17.36 | −1.69 | −1.86 | 15.18 | 0.721 |
| Knee | ||||||||||
| Sagittal Flex(+) Ext(-) | 4.74 | 3.67 | 20.73 | 0.22 | −1.55 | 12.64 | 3.36 | 3.02 | 17.64 | 0.141 |
| Frontal ABD(+) ADD(-) | 0.15 | −0.54 | 19.55 | −0.77 | 0.25 | 18.64 | −4.34 | −4.53 | 12.82 | 0.209 |
| Transverse ER(+) IR(-) | −3.97 | −1.33 | 16.55 | −0.91 | 0.48 | 20.82 | −4.43 | −5.15 | 13.64 | 0.215 |
| Ankle | ||||||||||
| Sagittal DF(+) PF(-) | 2.50 | 1.93 | 22.55 | −1.68 | −3.43 | 16.73 | −6.74 | −5.63 b | 11.73 | 0.032 * |
| Frontal ABD(+) ADD(-) | 3.47 | −2.82 | 17.64 | −2.58 | −3.35 | 12.18 | 2.49 | 1.03 | 21.18 | 0.089 |
| Transverse ER(+) IR(-) | 4.62 | 3.78 | 16.59 | 3.73 | 2.91 | 15.91 | 5.83 | 5.45 | 18.50 | 0.809 |
| Trunk | ||||||||||
| Sagittal Flex(+) Ext(-) | 2.76 | 0.43 | 17.59 | 2.45 | 1.56 | 17.55 | 1.63 | 0.60 | 15.86 | 0.892 |
| Frontal Medial(+) Lateral (-) | −0.53 | −0.07 | 19.55 | −0.94 | −0.55 | 15.73 | −0.66 | −0.71 | 15.73 | 0.565 |
| Cn | AB | KT | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Median | Mean Rank | Mean | Median | Mean Rank | Mean | Median | Mean Rank | K–W Test | |
| Hip | ||||||||||
| Sagittal Flex(+) Ext(-) | 2.28 | 3.00 | 19.73 | −1.46 | −2.45 a | 10.64 | 2.65 | 1.10 | 20.64 | 0.027 * |
| Frontal ABD(+) ADD(-) | 1.37 | 1.94 | 23.55 | −2.23 | −1.98 b | 12.82 | −2.86 | −1.57 c | 14.64 | 0.021 * |
| Transverse ER(+) IR(-) | 1.38 | 1.48 | 19.64 | 0.81 | 0.05 | 17.55 | −1.90 | −1.64 | 13.82 | 0.360 |
| Knee | ||||||||||
| Sagittal Flex(+) Ext(-) | 4.58 | 4.98 | 21.45 | −2.57 | −4.68 d,e | 9.55 | 4.51 | 1.71 | 20.00 | 0.007 * |
| Frontal ABD(+) ADD(-) | 0.65 | 1.00 | 19.86 | −0.23 | −0.03 | 16.64 | −1.43 | −0.52 | 14.50 | 0.424 |
| Transverse ER(+) IR(-) | 0.75 | 1.13 | 17.27 | 0.97 | 1.28 | 17.73 | 0.68 | 0.53 | 16.00 | 0.910 |
| Ankle | ||||||||||
| Sagittal DF(+) PF(-) | 5.01 | 5.37 | 22.55 | −0.85 | 1.94 | 12.82 | 1.47 | 1.76 | 15.64 | 0.052 |
| Frontal ABD(+) ADD(-) | 3.23 | 2.34 | 21.00 | −1.06 | −0.79 | 13.64 | 0.78 | .01 | 16.36 | 0.196 |
| Transverse ER(+) IR(-) | 1.61 | 0.20 | 22.00 | −1.34 | 2.01 | 17.00 | −4.14 | −3.59 | 12.00 | 0.053 |
| Trunk | ||||||||||
| Sagittal Flex(+) Ext(-) | 1.69 | 1.64 | 20.86 | 0.40 | 0.46 | 15.50 | 0.32 | −0.35 | 14.64 | 0.262 |
| Frontal Medial(+) Lateral (-) | 0.85 | 0.82 | 20.86 | 0.20 | 0.23 | 15.50 | 0.16 | −0.17 | 14.64 | 0.262 |
| Cn | AB | KT | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Median | Mean Rank | Mean | Median | Mean Rank | Mean | Median | Mean Rank | K–W Test | |
| Difference of COM range (%BH) | ||||||||||
| ML | 0.00507 | 0.00470 | 23.45 | −0.00332 | −0.00316 a | 11.09 | 0.00014 | −0.00094 | 16.45 | 0.011 * |
| AP | −0.00064 | 0.00059 | 19.36 | −0.00254 | −0.00264 | 14.45 | −0.00067 | −0.00159 | 17.18 | 0.491 |
| Vertical | 0.00788 | 0.00844 | 24.27 | −0.00832 | −0.00892 b | 11.36 | −0.00433 | −0.00160 c | 15.36 | 0.006 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.-C.; Lee, W.-C.; Chen, J.-C.; Chen, S.-J.; Lin, C.-F. The Influence of Kinesio Tape and an Ankle Brace on the Lower Extremity Joint Motion in Fatigued, Unstable Ankles during a Lateral Drop Landing. Int. J. Environ. Res. Public Health 2021, 18, 6081. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116081
Lin C-C, Lee W-C, Chen J-C, Chen S-J, Lin C-F. The Influence of Kinesio Tape and an Ankle Brace on the Lower Extremity Joint Motion in Fatigued, Unstable Ankles during a Lateral Drop Landing. International Journal of Environmental Research and Public Health. 2021; 18(11):6081. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116081
Chicago/Turabian StyleLin, Cheng-Chieh, Wan-Chin Lee, Jih-Ching Chen, Shing-Jye Chen, and Cheng-Feng Lin. 2021. "The Influence of Kinesio Tape and an Ankle Brace on the Lower Extremity Joint Motion in Fatigued, Unstable Ankles during a Lateral Drop Landing" International Journal of Environmental Research and Public Health 18, no. 11: 6081. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18116081