
Lifestyle Interventions to Improve Glycemic Control in Adults with Type 2 Diabetes Living in Low-and-Middle Income Countries: A Systematic Review and Meta-Analysis of Randomized Controlled Trials (RCTs)

 , ,
, ,
Abstract
:1. Introduction
- To explore core components of lifestyle interventions, specifically in relation to strategies and intervention characteristics for the management of T2DM (method, context of delivery, by whom, with what intensity and for how long).
- To complete a quality assessment on included randomized control trials (RCTs).
- To conduct a meta-analysis to establish the effectiveness of these interventions on improving glycemic control and anthropometry.
- To compile recommendations for future research on this topic.
2. Materials and Methods
2.1. Registration
2.2. Search Strategy
2.3. Inclusion Criteria
2.4. Outcome Measures
2.5. Selection Process
2.6. Data Extraction
2.7. Quality Assessment
2.8. Data Synthesis
2.9. Assessment of Publication Bias
2.10. Grading of the Quality of Evidence
3. Results
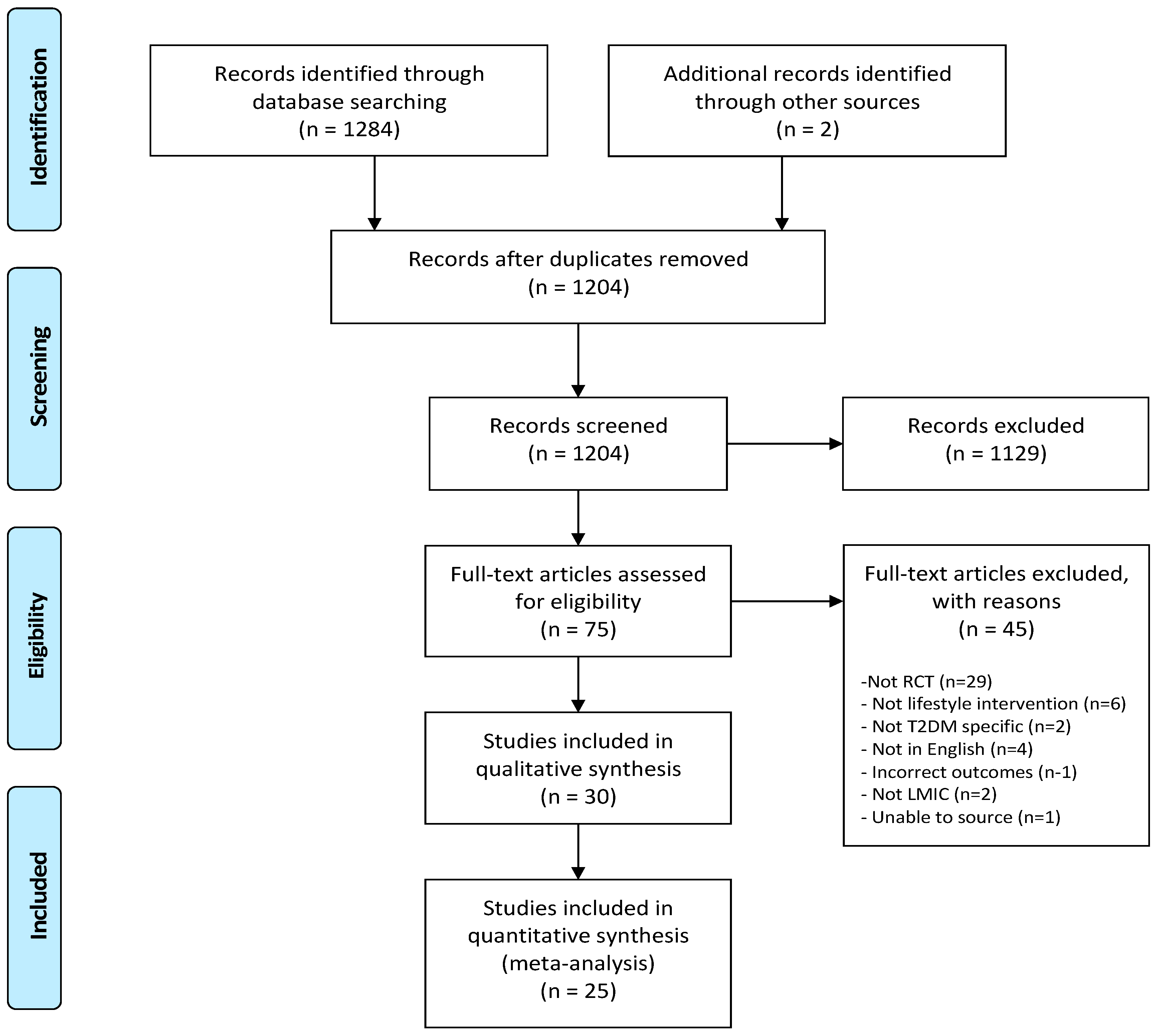
3.1. Literature Selection
3.2. Study Characteristics
3.3. Lifestyle Intervention Characteristics
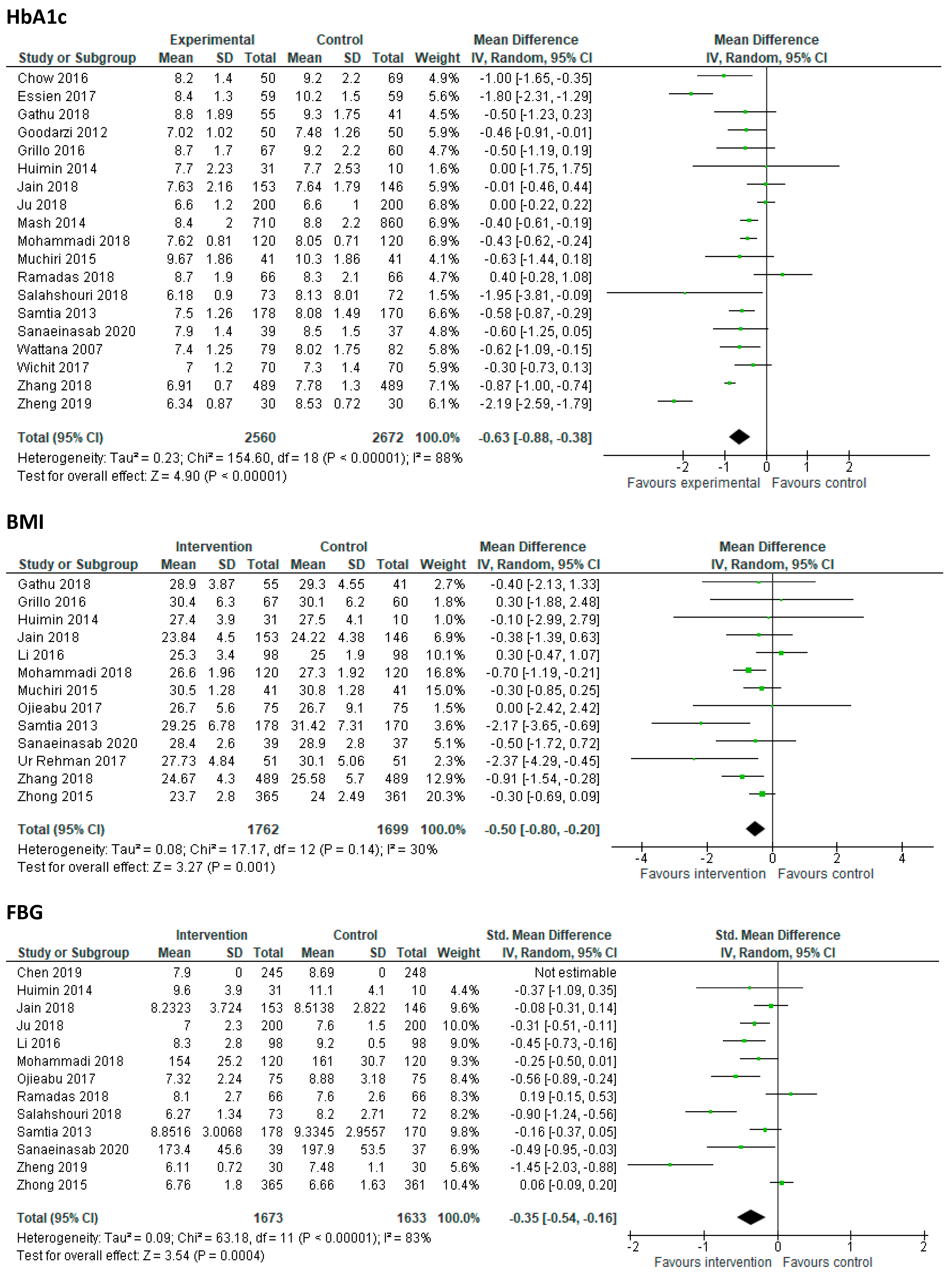
3.4. Effects of Lifestyle Interventions on Clinical Outcome Measures
3.5. Risk of Bias Assessment
3.6. Publication Bias
3.7. Strength of the Evidence
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Unnikrishnan, R.; Mohan, V. Diabetes in the tropics: Prevalent, increasing and a major public health problem. Trans. R. Soc. Trop. Med. Hygeine 2016, 110, 263–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Diabetes Epidemic in Europe 2014. Available online: https://www.who.int/news-room/fact-sheets/detail/diabetes (accessed on 1 October 2020).
- IDF Diabetes Atlas. Federation ofNorth America and Caribbean Diabetes Report 2010–2045. 2019. Available online: https://www.diabetesatlas.org/data/en/region/5/nac.html. (accessed on 1 October 2020).
- Owolabi, M.O.; Yaria, J.O.; Daivadanam, M.; Makanjuola, A.I.; Parker, G.; Oldenburg, B.; Vedanthan, R.; Norris, S.; Oguntoye, A.R.; Osundina, M.A.; et al. Gaps in Guidelines for the Management of Diabetes in Low- and Middle-Income Versus High-Income Countries-A Systematic Review. Diabetes Care 2018, 41, 1097–1105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moucheraud, C.; Lenz, C.; Latkovic, M.; Wirtz, V.J. The costs of diabetes treatment in low- and middle-income countries: A systematic review. Br. Med. J. Glob. Health 2019, 4, e001258. [Google Scholar] [CrossRef]
- Association, A.D. Lifestyle Management: Standards of Medical Care in Diabetes—2018. Diabetes Care 2018, 41, S38–S50. [Google Scholar] [CrossRef] [Green Version]
- Jacobs-van der Bruggen, M.A.; Bos, G.; Bemelmans, W.J.; Hoogenveen, R.T.; Vijgen, S.M.; Baan, C.A. Lifestyle Interventions Are Cost-Effective in People With Different Levels of Diabetes Risk: Results from a modeling study. Diabetes Care 2007, 30, 128–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, Y.; You, W.; Almeida, F.; Estabrooks, P.; Davy, B. The Effectiveness and Cost of Lifestyle Interventions Including Nutrition Education for Diabetes Prevention: A Systematic Review and Meta-Analysis. J. Acad. Nutr. Diet. 2017, 117, 404–421. [Google Scholar] [CrossRef] [Green Version]
- Howells, L.; Musaddaq, B.; McKay, A.J.; Majeed, A. Clinical impact of lifestyle interventions for the prevention of diabetes: An overview of systematic reviews. BMJ Open 2016, 6, e013806. [Google Scholar] [CrossRef]
- Huang, X.L.; Pan, J.H.; Chen, D.; Chen, J.; Chen, F.; Hu, T.T. Efficacy of lifestyle interventions in patients with type 2 diabetes: A systematic review and meta-analysis. Eur. J. Intern. Med. 2016, 27, 37–47. [Google Scholar] [CrossRef]
- Mohamed, A.; Staite, E.; Ismail, K.; Winkley, K. A systematic review of diabetes self-management education interventions for people with type 2 diabetes mellitus in the Asian Western Pacific (AWP) region. Nurs. Open 2019, 6, 1424–1437. [Google Scholar] [CrossRef] [Green Version]
- Wai Htoo, Z.; Hsu, W.-W.; Rosenkranz, R. Syatematic review and meta-anlysis: Is lifestyle modification effectvie for glycemic control among adults with type II daibetes in Southeast Asia? Diabetes Res. Clin. Pract. 2016, 122, 148–153. [Google Scholar] [CrossRef]
- Shirinzadeh, M.; Afshin-Pour, B.; Angeles, R.; Gaber, J.; Agarwal, G. The effect of community-based programs on diabetes prevention in low- and middle-income countries: A systematic review and meta-analysis. Glob. Health 2019, 15, 10–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afable, A.; Karingula, N.S. Evidence based review of type 2 diabetes prevnetion and management in low and middle income countries. World J. Diabetes 2016, 7, 209–229. [Google Scholar] [CrossRef] [PubMed]
- Mohan, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1–9. [Google Scholar]
- Association, A.D. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes—2019. Diabetes Care 2019, 42, S13–S28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bank, T.W. World Bank Country and Lending Groups 2019. Available online: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups (accessed on 1 November 2020).
- Armijo-Olivo, S.; Stiles, C.R.; Hagen, N.A.; Biondo, P.D.; Cummings, G.G. Assessment of study quality for systematic reviews: A comparison of the Cochrane Collaboration Risk of Bias Tool and the Effective Public Health Practice Project Quality Assessment Tool: Methodological research. J. Eval. Clin. Pract. 2012, 18, 12–18. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Cochrane Collaboration 2011. Available online: https://training.cochrane.org/handbook/current (accessed on 10 September 2020).
- Chaveepojnkamjorn, W.; Pichainarong, N.; Schelp, F.P.; Mahaweerawat, U. A randomized controlled trial to improve the quality of life of type 2 diabetic patients using a self-help group program. Southeast Asian J. Trop. Med. Public Health 2009, 40, 169–176. [Google Scholar]
- Chen, S.; Burström, B.; Sparring, V.; Qian, D.; Burström, K. Differential impact of an education-based intervention for patients with type 2 diabetes mellitus in rural China. Int. J. Environ. Res. Public Health 2019, 16, 2676. [Google Scholar] [CrossRef] [Green Version]
- Chow, E.P.; Hassali, M.A.; Saleem, F.; Aljadhey, H. Effects of pharmacist-led patient education on diabetes-related knowledge and medication adherence: A home-based study. Health Educ. J. 2016, 75, 421–433. [Google Scholar] [CrossRef]
- Gagliardino, J.J.; Lapertosa, S.; Pfirter, G.; Villagra, M.; Caporale, J.E.; Gonzalez, C.D.; Elgart, J.; Gonzalez, L.; Cernadas, C.; Rucci, E.; et al. Clinical, metabolic and psychological outcomes and treatment costs of a prospective randomized trial based on different educational strategies to improve diabetes care (PRODIACOR). Diabet. Med. 2013, 30, 1102–1111. [Google Scholar] [CrossRef]
- Goldhaber-Fiebert, J.D.; Goldhaber-Fiebert, S.N.; Tristán, M.L.; Nathan, D.M. Randomized controlled community-based nutrition and exercise intervention improves glycemia and cardiovascular risk factors in type 2 diabetic patients in rural Costa Rica. Diabetes Care 2003, 26, 24–29. [Google Scholar] [CrossRef] [Green Version]
- Goodarzi, M.; Ebrahimzadeh, I.; Rabi, A.; Saedipoor, B.; Jafarabadi, M.A. Impact of distance education via mobile phone text messaging on knowledge, attitude, practice and self efficacy of patients with type 2 diabetes mellitus in Iran. J. Diabetes Metab. Disord. 2012, 11, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ju, C.; Shi, R.; Yao, L.; Ye, X.; Jia, M.; Han, J.; Yang, T.; Lu, Q.; Jin, H.; Cai, X.; et al. Effect of peer support on diabetes distress: A cluster randomized controlled trial. Diabet. Med. 2018, 35, 770–775. [Google Scholar] [CrossRef] [PubMed]
- Sanaeinasab, H.; Saffari, M.; Yazdanparast, D.; Zarchi, A.K.; Al-Zaben, F.; Koenig, H.G.; Pakpour, A.H. Effects of a health education program to promote healthy lifestyle and glycemic control in patients with type 2 diabetes: A randomized controlled trial. Prim. Care Diabetes 2020, 15, 275–282. [Google Scholar] [CrossRef]
- Li, Y.; Xu, M.; Fan, R.; Ma, X.; Gu, J.; Cai, X.; Liu, R.; Chen, Q.; Ren, J.; Mao, R.; et al. The effects of intensive nutrition education on late middle-aged adults with type 2 diabetes. Int. J. Environ. Res. Public Health 2016, 13, 897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohammadi, S.; Karim, N.A.; Talib, R.A.; Amani, R. The impact of self-efficacy education based on the health belief model in Iranian patients with type 2 diabetes: A randomised controlled intervention study. Asia Pac. J. Clin. Nutr. 2018, 27, 546–555. [Google Scholar]
- Muchiri, J.W.; Gericke, G.J.; Rheeder, P. Effect of a nutrition education programme on clinical status and dietary behaviours of adults with type 2 diabetes in a resource-limited setting in South Africa: A randomised controlled trial. Public Health Nutr. 2015, 19, 142055. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramadas, A.; Chan, C.K.Y.; Oldenburg, B.; Hussein, Z.; Quek, K.F. Randomised-controlled trial of a web-based dietary intervention for patients with type 2 diabetes: Changes in health cognitions and glycemic control. BMC Public Health 2018, 18, 716. [Google Scholar] [CrossRef]
- Salahshouri, A.; Alavijeh, F.Z.; Mahaki, B.; Mostafavi, F. Effectiveness of educational intervention based on psychological factors on achieving health outcomes in patients with type 2 diabetes. Diabetol. Metab. Syndr. 2018, 10, 67–79. [Google Scholar] [CrossRef] [Green Version]
- Wichit, N.; Mnatzaganian, G.; Courtney, M.; Schulz, P.; Johnson, M. Randomized controlled trial of a family-oriented self-management program to improve self-efficacy, glycemic control and quality of life among Thai individuals with Type 2 diabetes. Diabetes Res. Clin. Pract. 2017, 123, 37–48. [Google Scholar] [CrossRef] [Green Version]
- Zheng, F.; Liu, S.; Liu, Y.; Deng, L. Effects of an outpatient diabetes self-management education on patients with type 2 diabetes in China: A randomized controlled trial. J. Diabetes Res. 2019, 2019, 1073131. [Google Scholar] [CrossRef]
- Zhang, Y.; Chu, L. Effectiveness of Systematic Health Education Model for Type 2 Diabetes Patients. Int. J. Endocrinol. 2018, 2018, 6530607. [Google Scholar] [CrossRef] [Green Version]
- Mash, R.J.; Rhode, H.; Zwarenstein, M.; Rollnick, S.; Lombard, C.; Steyn, K.; Levitt, N. Effectiveness of a group diabetes education programme in under-served communities in South Africa: A pragmatic cluster randomized controlled trial. Diabet. Med. 2014, 31, 987–993. [Google Scholar] [CrossRef] [PubMed]
- Wattana, C.; Srisuphan, W.; Pothiban, L.; Upchurch, S.L. Effects of a diabetes self-management program on glycemic control, coronary heart disease risk, and quality of life among Thai patients with type 2 diabetes. Nurs. Health Sci. 2007, 9, 135–141. [Google Scholar] [CrossRef]
- Zhong, X.; Wang, Z.; Fisher, E.B.; Tanasugarn, C. Peer Support for Diabetes Management in Primary Care and Community Settings in Anhui Province, China. Ann. Fam. Med. 2015, 13, S50–S58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Essien, O.; Otu, A.; Umoh, V.; Enang, O.; Hicks, J.P.; Walley, J. Intensive patient education improves glycaemic control in diabetes compared to conventional education: A randomised controlled trial in a nigerian tertiary care hospital. PLoS ONE 2017, 12, e0168835. [Google Scholar] [CrossRef]
- Fottrell, E.; Ahmed, N.; Morrison, J.; Kuddus, A.; Shaha, S.K.; King, C.; Jennings, H.; Akter, K.; Nahar, T.; Haghparast-Bidgoli, H.; et al. Community groups or mobile phone messaging to prevent and control type 2 diabetes and intermediate hyperglycaemia in Bangladesh (DMagic): A cluster-randomised controlled trial. Lancet Diabetes Endocrinol. 2019, 7, 200–212. [Google Scholar] [CrossRef] [Green Version]
- Gathu, C.W.; Shabani, J.; Kunyiha, N.; Ratansi, R. Effect of diabetes self-management education on glycaemic control among type 2 diabetic patients at a family medicine clinic in Kenya: A randomised controlled trial. Afr. J. Prim. Health Care Fam. Med. 2018, 10, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Grillo, M.D.F.F.; Neumann, C.R.; Scain, S.F.; Rozeno, R.F.; Beloli, L.; Perinetto, T.; Gross, J.L.; Leitão, C.B. Diabetes education in primary care: A randomized clinical trial. Cad. Saude Publica 2016, 32, e00097115. [Google Scholar] [CrossRef]
- Jain, V.; Joshi, R.; Idiculla, J.; Xavier, D. Community health worker interventions in type 2 diabetes mellitus patients: Assessing the feasibility and effectiveness in Rural Central India. J. Cardiovasc. Dis. Res. 2018, 9, 127–133. [Google Scholar] [CrossRef] [Green Version]
- Malathy, R.; Narmadha, M.P.; Jose, M.A.; Ramesh, S.; Babu, N.D. Effect of a diabetes counseling programme on knowledge, attitude and practice among diabetic patients in Erode district of South India. J. Young Pharm. 2011, 3, 65–72. [Google Scholar] [CrossRef] [Green Version]
- Ojieabu, W.A.; Saka, S.A.; Ojieabu, C.E. Evaluation of pharmacists’ educational and counseling impact on patients’ clinical outcomes in a diabetic setting. J. Diabetol. 2017, 8, 7–11. [Google Scholar] [CrossRef]
- Samtia, A.M.; Rasool, M.F.; Ranjha, N.M.; Usman, F.; Javed, I. A multifactorial intervention to enhance adherence to medications and disease-related knowledge in type 2 diabetic patients in Southern Punjab, Pakistan. Trop. J. Pharm. Res. 2013, 12, 851–858. [Google Scholar] [CrossRef] [Green Version]
- Rehman, S.S.U.; Karimi, H.; Gillani, S.A.; Ahmad, S. Effects of supervised structured aerobic exercise training programme on level of exertion, dyspnoea, VO2 max and body mass index in patients with type 2 diabetes mellitus. J. Pak. Med. Assoc. 2017, 67, 1670–1673. [Google Scholar]
- Debussche, X.; Besançon, S.; Balcou-Debussche, M.; Ferdynus, C.; Delisle, H.; Huiart, L.; Sidibé, A.T. Structured peer-led diabetes self-management and support in a low-income country: The ST2EP randomised controlled trial in Mali. PLoS ONE 2018, 13, e0191262. [Google Scholar] [CrossRef] [Green Version]
- Yan, H.; Prista, A.; Ranadive, S.M.; Damasceno, A.; Caupers, P.; Kanaley, J.A.; Fernhall, B. Effect of Aerobic Training on Glucose Control and Blood Pressure in T2DDM East African Males. ISRN Endocrinology. Int. Sch. Res. Not. 2014, 2014, 864897. [Google Scholar]
- Lenters-Westra, E.; Schindhelm, R.K.; Bilo, H.J.; Groenier, K.H.; Slingerland, R.J. Differences in interpretation of haemoglobin A1c values among diabetes care professionals. Neth. J. Med. 2014, 72, 462–466. [Google Scholar]
- Mannucci, E.; Monami, M.; Lamanna, C.; Gori, F.; Marchionni, N. Prevention of cardiovascular disease through glycemic control in type 2 diabetes: A meta-analysis of randomized clinical trials. Nutr. Metab. Cardiovasc. Dis. 2009, 19, 604–612. [Google Scholar] [CrossRef]
- Siegel, K.R.; Ali, M.K.; Zhou, X.; Ng, B.P.; Jawanda, S.; Proia, K.; Zhang, X.; Gregg, E.W.; Albright, A.L.; Zhang, P. Cost-effectiveness of Interventions to Manage Diabetes: Has the Evidence Changed Since 2008? Diabetes Care 2020, 43, 1557. [Google Scholar] [CrossRef]
- Pan, B.; Ge, L.; Xun, Y.Q.; Chen, Y.J.; Gao, C.Y.; Han, X.; Zuo, L.Q.; Shan, H.Q.; Yang, K.H.; Ding, G.W.; et al. Exercise training modalities in patients with type 2 diabetes mellitus: A systematic review and network meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 72. [Google Scholar] [CrossRef]
- Chen, L.; Pei, J.H.; Kuang, J.; Chen, H.M.; Chen, Z.; Li, Z.W.; Yang, H.Z. Effect of lifestyle intervention in patients with type 2 diabetes: A meta-analysis. Metabolism 2015, 64, 338–347. [Google Scholar] [CrossRef] [PubMed]
- Flood, D.; Hane, J.; Dunn, M.; Brown, S.J.; Wagenaar, B.H.; Rogers, E.A.; Heisler, M.; Rohloff, P.; Chopra, V. Health system interventions for adults with type 2 diabetes in low- and middle-income countries: A systematic review and meta-analysis. PLoS Med. 2020, 17, e1003434. [Google Scholar] [CrossRef]
- Horigan, G.; Davies, M.; Findlay-White, F.; Chaney, D.; Coates, V. Reasons why patients referred to diabetes education programmes choose not to attend: A systematic review. Diabet. Med. 2017, 34, 14–26. [Google Scholar] [CrossRef] [PubMed]
- Graziani, C.; Rosenthal, M.P.; Diamond, J.J. Diabetes education program use and patient-perceived barriers to attendance. Fam. Med. 1999, 31, 358–363. [Google Scholar] [PubMed]
- Werfalli, M.; Raubenheimer, P.J.; Engel, M.; Musekiwa, A.; Bobrow, K.; Peer, N.; Hoegfeldt, C.; Kalula, S.; Kengne, A.P.; Levitt, N.S. The effectiveness of peer and community health worker-led self-management support programs for improving diabetes health-related outcomes in adults in low- and-middle-income countries: A systematic review. Syst. Rev. 2020, 9, 133. [Google Scholar] [CrossRef]
- Checkley, W.; Ghannem, H.; Irazola, V.; Kimaiyo, S.; Levitt, N.S.; Miranda, J.J.; Niessen, L.; Prabhakaran, D.; Rabadán-Diehl, C.; Ramirez-Zea, M.; et al. Management of NCD in low- and middle-income countries. Glob. Heart 2014, 9, 431–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plumb, J.; Weinstein, L.C.; Brawer, R.; Scott, K. Community-based partnerships for improving chronic disease management. Prim. Care 2012, 39, 433–447. [Google Scholar] [CrossRef] [Green Version]
- Harman, N.L.; Wilding, J.P.H.; Curry, D.; Harris, J.; Logue, J.; Pemberton, R.J.; Perreault, L.; Thompson, G.; Tunis, S.; Williamson, P.R. Selecting Core Outcomes for Randomised Effectiveness trials In Type 2 diabetes (SCORE-IT): A patient and healthcare professional consensus on a core outcome set for type 2 diabetes. BMJ Open Diabetes Res. Care 2019, 7, e000700. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Author | Year | Country | Country Classification | Intervention Description | Intervnetion Category | Study Duration (Weeks) | Sample Size (I/C) | Age Mean (SD) | Gender (% Female) | Diabetes Any Diabetes Medication (Insulin) | Outcome Measures |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Chaveepojnkamjorn [20] | 2009 | Thailand | Upper middle | Self-help group program for patients. | SME | 16 | 80/84 | I: 48.9 (6.9) C: 49.1 (7.3) | I: 78 C: 76 | QoL | |
| Chen [21] | 2019 | China | Upper middle | Education-based intervention for patients. | SME | 104 | 245/248 | I: 63.3 (6.8) C: 61.5 (9.1) | I: 79 C: 67 | FBG, QoL | |
| Chow [22] | 2016 | Malaysia | Upper middle | Home based pharmacist led educational intervention for patients. | SME | 12 | 75/75 | 60.31 | I: 64 C: 63 | HbA1c | |
| Debussche [48] | 2018 | Mali | Low | Structured T2DM Self-management Education by peers for patients. | SME | 52 | 76/75 | I: 53.9 (9.8) C: 51.1 (9.6) | I: 75 C: 77 | I: 55 (22) C: 53 (21) | HbA1c, BMI, WC, SBP, DBP |
| Essien [39] | 2017 | Nigeria | Lower middle | Intensive diabetes self-management program for patients. | SME | 26 | 59/59 | I: 52.6 (10.9) C: 52.8 (10.1) | I: 52 C: 67 | HbA1c | |
| Fottrell [40] | 2019 | Bangladesh | Lower middle | 1. MHealth educational voice messages. 2. Participatory learning which engages communities to identify and address their own local problems. | 1. SME * 2. SME | 104 | * 4093/4079/4108 | I 1: 55 I 2: 53 C: 52 | BMI, SBP, DBP, QoL | ||
| Gagliardino [23] | 2013 | Argentina | Upper middle | 1. Education for healthcare professionals. 2. Self-management education for patients. 3. Education for patients and healthcare professionals. | 1. SME ^ 2. SME ^^ 3. SME ^^^ | 182 | 135/135/135/135 | I 1: 62.4 (9.1) I 2: 62.2 (8.4) I 3: 62.2 (9.0) C: 62.1 (8.4) | HbA1c, SBP, TG | ||
| Gathu [41] | 2018 | Kenya | Lower middle | Diabetes self-management education training for patients. | SME | 26 | 70/70 | I: 50.2 (9.9) C: 47.5 (9.5) | I: 41 C: 47 | HbA1c, BMI, SBP, DBP | |
| Goldhaber-Fiebert [24] | 2003 | Costa Rica | Upper middle | Community-based nutrition and exercise intervention for patients. | SDEP | 12 | 40/35 | I: 60 (10) C: 57 (9) | I: 83 C: 75 | HbA1c, FBG, BW, BMI, SBP, DBP, TC, HDLc, LDLc, TG | |
| Goodarzi [25] | 2012 | Iran | Upper middle | Distance education including exercise, diet, diabetic meds, self-monitoring of blood glucose levels, via mobile phone text messaging. | SME | 12 | 50/50 | I: 50.1 (10.3) C: 56.7 (9.7) | I: 79 C: 76 | I: 41 (13) C: 37 (13) | HBA1c, TC, HDLc, LDLc, TG |
| Grillo [42] | 2016 | Brazil | Lower middle | Structured diabetes self-management education course for patients, administered by a generalist nurse trained in diabetes education. | SME | 52 | 69/68 | I: 61.7 (9.9) C: 63.2 (9.7) | I: 71 C: 55 | I: 69 (4) C: 68 (3) | BMI, WC, SBP, DPB, HDLc, LDLc |
| Huimin [49] | 2014 | Mozmbique | Low | Low to vigorous intensity exercise intervention for patients. | SDEP | 12 | 31/10 | I: 53.2 (2.5) C: 55.3 (3) | I: 0 C: 0 | HbA1c, FBG, BW, BMI, WC, SBP, DBP, VO2max | |
| Jain [43] | 2018 | India | Lower middle | Face-to-face interaction by community health workers as well as telephonic reminders. | SME | 24 | 153/146 | I: 55.7 (10.9) C: 57.4 (10.1) | I: 45 C: 41 | HBA1c, FBG, BW, BMI, WC, SBP, DPB, TC, HDLc, LDLc, TG | |
| Ju [26] | 2018 | China | Upper middle | Usual education of 2 h each month of focused diabetes education and peer support. | SME | 52 | 200/200 | I: 67.8 (7.4) C: 68.8 (8) | I: 65 C: 68 | HBA1c, FBG, 2HBG | |
| Li [28] | 2016 | China | Upper middle | Intensive nutrition education classes for patients. | SDEP | 4 | 98/98 | I: 59.1 (4.6) C: 58.3 (4.1) | I: 52 C: 46 | I: 84 (16) C: 82 (17) | HBA1c, FBG, 2HBG, BW, BMI, HDLc, LDLc, TG |
| Malathy [44] | 2011 | India | Lower middle | Pharmacist-led diabetes counseling program for patients. | SME | 12 | 137/70 | I: 52.1 (9.5) C: 51.1 (9.8) | I: 73 C: 35 | TC, HDLc, LDLc, TG | |
| Mash [36] | 2014 | South Africa | Upper middle | Group-based diabetes education program for patients. | SME | 52 | 710/860 | I: 55.8 (11.5) C: 56.4 (11.6) | I: 72 C: 76 | I: 213 (59) C: 228 (73) | HBA1c, WC, BW, SBP, DBP, TC |
| Mohammadi [29] | 2018 | Iran | Upper middle | Self-efficacy education for patients, based on health belief model. | SME | 36 | 120/120 | I: 51.2 (6.2) C: 51.4 (6.1) | HBA1c, FBG, BW, BMI, WC, LDLc, HDLc, QoL | ||
| Muchiri [30] | 2015 | South Africa | Upper middle | Nutrition education program for patients. | SDEP | 52 | 41/41 | I: 59.4 (6.9) C: 58.2 (8) | 85 | HbA1c, BMI, SBP, DBP, TC, LDLc, HDLc | |
| Ojieabu [45] | 2017 | Nigeria | Lower middle | Pharmacist-led education and counseling program for patients. | SME | 20 | 75/75 | I: 64 C: 60 | FBG, BMI, SBP, DBP | ||
| Ramadas [31] | 2018 | Malaysia | Upper middle | Web-based dietry intervention program. | SDEP | 52 | 66/66 | I: 49.6 (10.7) C: 51.5 (10.3) | I: 41 C:40 | I: 56 (7) C: 51 (7) | HbA1c |
| Salahshouri [32] | 2018 | Iran | Upper middle | Educational sessions for patients, based on psychological factors administered by a group of internal specialists, dieticians, diabetes experts, a psychologist and a religious expert. | SME | 20 | 73/72 | I: 55.9 (12.4) C: 54.8 (9.4) | I: 67 C: 69 | HbA1c, FBG | |
| Sanaeinasab [27] | 2020 | Iran | Upper middle | Group face-to-face sessions, 1 × weekly × 6 weeks; health education and promotion program focusing on diabetes self-care. | SME | 6 | 40/40 | 50.7 (5.9) | I: 55 C: 63 | HBA1c, FBG, BMI, SBP, DBP, TC, HDL, LDL, TG | |
| Samtia [46] | 2013 | Pakistan | Lower middle | Pre-defined, pharmacist-led, multifactorial, specialized care for patients. | SME | 20 | 178/170 | I: 46.1 C: 42.3 | I: 47 C: 52 | HBA1c, FBG, BMI, WC | |
| Ur Rehman [47] | 2017 | Pakistan | Lower middle | Supervised structured aerobic exercise training (SSAET) program, routine medication, and dietry planning for patients. | SDEP | 25 | 51/51 | 54.7 (8.2) | 67 | BMI | |
| Wattana [37] | 2007 | Thailand | Upper middle | Diabetes self-management program for patients, based on the theories of self efficacy and self-management. | SME | 24 | 79/82 | 56.8 (4.6) | 76 | HbA1c, QoL | |
| Wichit [33] | 2017 | Thailand | Upper middle | Family oriented self-management intervention program for patients, designed based on the self-efficacy theory. | SME | 13 | 70/70 | I: 61.3 (11.6) C: 55.5 (10.5) | I: 76 C: 70 | HbA1c, QoL | |
| Zhang [35] | 2018 | China | Upper middle | A nine-component systematic education intervention for patients. | SME | 348 | 489/489 | I: 56.8 (14.2) C: 52.6 (13.2) | I: 51 C: 49 | HbA1c, BMI, SBP, DBP, TC, LDLc, HDLc | |
| Zheng [34] | 2019 | China | Upper middle | 2-session diabetes self-management education program for patients with theory and practical elements. | SME | 12 | 30/30 | I: 52.5 (10.5) C: 51.9 (12.3) | I: 47 C: 43 | HBA1c, FBG, 2HBG | |
| Zhong [38] | 2015 | China | Upper middle | Peer leader-support program for patients. | SME | 26 | 365/361 | 55 | FBG, 2HBG, BMI, SBP, DBP |
| Clinical Outcome Measure | |||
|---|---|---|---|
| Glycated Hemoglobin (HbA1c) | Body Mass Index (BMI) | Fasting Blood Glucose (FBG) | |
| Overall | MD −0.63 (−0.86 to −0.40), I2 88% | MD −0.50 (−0.80 to −0.20), I2 30% | SMD −0.35 (−0.54 to −0.16), I2 83% |
| Intervention | |||
| Self-management education | MD −0.69 (−0.96 to −0.43), I2 90% | MD −0.54 (−0.79 to −0.29), I2 0% | SMD −0.42 (−0.69 to −0.16), I2 87% |
| Structured Diet/exercise/combined | MD −0.07 (−0.81 to 0.67), I2 45% | MD −0.06 (−0.64 to 0.51), I2 35% | SMD −0.14 (−0.76 to 0.48), I2 87% |
| Delivery | |||
| Healthcare professional(s)/MDT | MD −0.71 (−1.01 to −0.41), I2 77% | MD −0.48 (−1.11 to 0.15), I2 57% | SMD −0.37 (−0.70 to −0.05), I2 84% |
| Trained peers/lay people | MD −0.24 (−0.47 to 0.00), I2 57% | MD −0.51 (−1.10 to 0.09), I2 30% | SMD −0.11 (−0.33 to 0.12), I2 77% |
| Setting | |||
| Hospital/clinic | MD −0.77 (−1.08 to −0.56), I2 88% | MD −0.61 (−1.07 to −0.15), I2 50% | SMD −0.47 (−0.74 to −0.20), I2 82% |
| Community | MD −0.2 (−0.59 to 0.19), I2 85% | N/A | SMD −0.12 (−0.48 to 0.24), I2 88% |
| Home | MD −0.48 (−1.44 to 0.49), I2 83% | N/A | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
O’Donoghue, G.; O’Sullivan, C.; Corridan, I.; Daly, J.; Finn, R.; Melvin, K.; Peiris, C. Lifestyle Interventions to Improve Glycemic Control in Adults with Type 2 Diabetes Living in Low-and-Middle Income Countries: A Systematic Review and Meta-Analysis of Randomized Controlled Trials (RCTs). Int. J. Environ. Res. Public Health 2021, 18, 6273. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126273
O’Donoghue G, O’Sullivan C, Corridan I, Daly J, Finn R, Melvin K, Peiris C. Lifestyle Interventions to Improve Glycemic Control in Adults with Type 2 Diabetes Living in Low-and-Middle Income Countries: A Systematic Review and Meta-Analysis of Randomized Controlled Trials (RCTs). International Journal of Environmental Research and Public Health. 2021; 18(12):6273. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126273
Chicago/Turabian StyleO’Donoghue, Grainne, Cliona O’Sullivan, Isabelle Corridan, Jennifer Daly, Ronan Finn, Kathryn Melvin, and Casey Peiris. 2021. "Lifestyle Interventions to Improve Glycemic Control in Adults with Type 2 Diabetes Living in Low-and-Middle Income Countries: A Systematic Review and Meta-Analysis of Randomized Controlled Trials (RCTs)" International Journal of Environmental Research and Public Health 18, no. 12: 6273. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18126273