
Physical Activity Level Following Resistance Training in Community-Dwelling Older Adults Receiving Home Care: Results from a Cluster-Randomized Controlled Trial

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
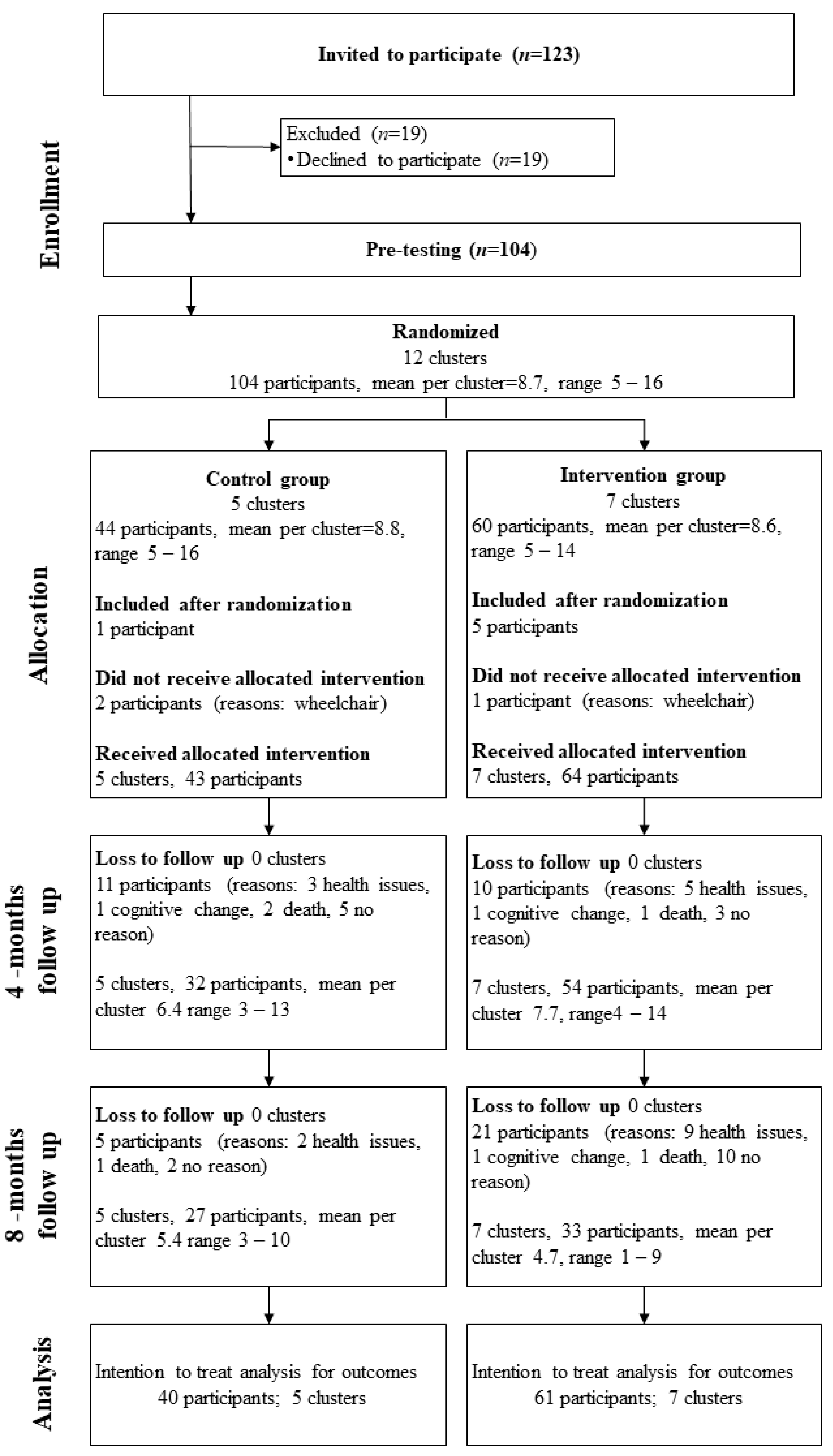
2.1. Trial Design
2.2. Participants
2.3. Intevention
2.4. Physical Activity Outcomes
2.5. Randomization and Blinding
2.6. Statistical Analysis
3. Results
3.1. Participant Characteristics
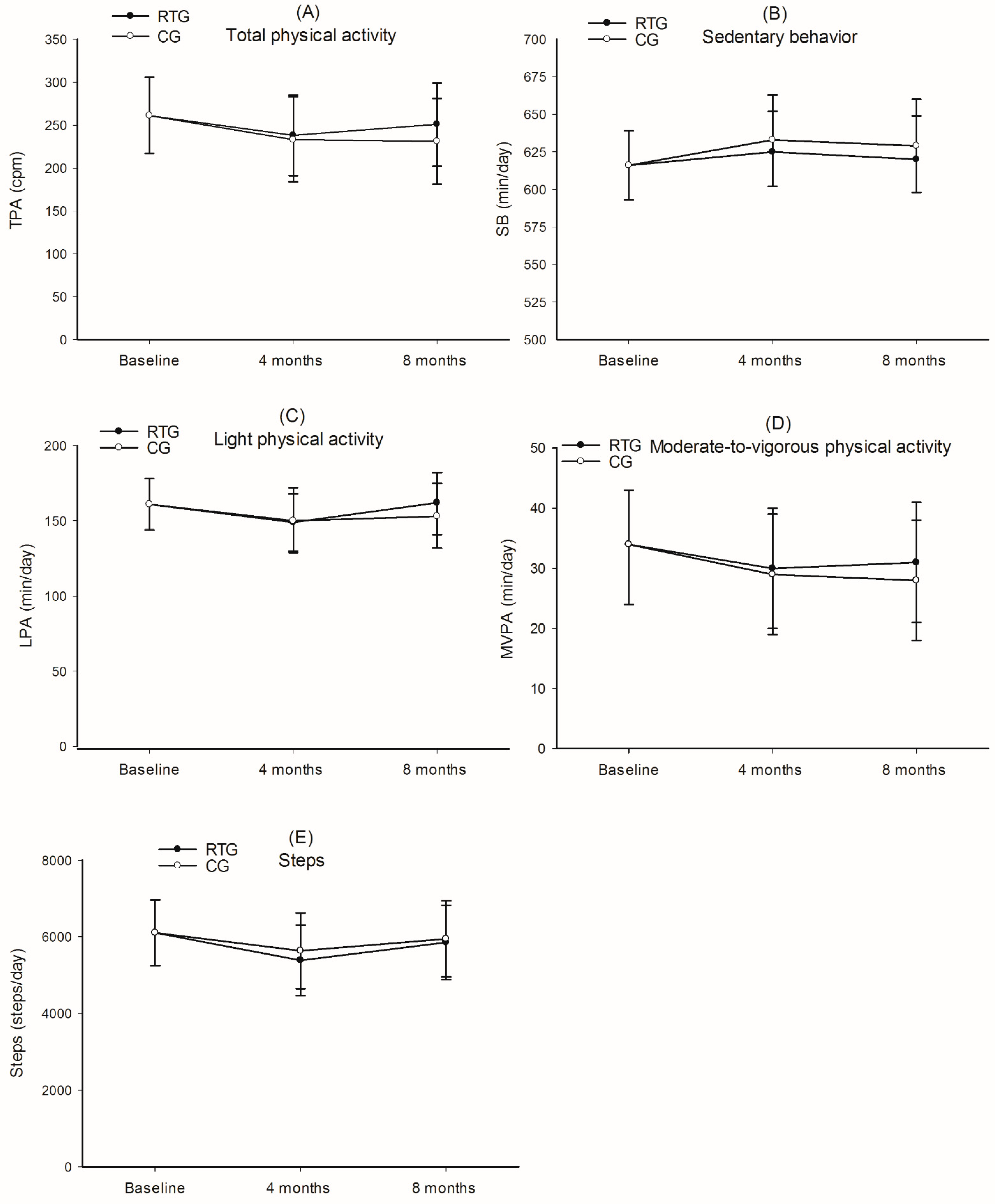
3.2. Physical Activity Level
3.3. Per Protocol Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dogra, S.; Stathokostas, L. Sedentary behavior and physical activity are independent predictors of successful aging in middle-aged and older adults. J. Aging Res. 2012, 2012, 190654. [Google Scholar] [CrossRef] [Green Version]
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet (Lond. UK) 2012, 380, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Chodzko-Zajko, W.J.; Proctor, D.N.; Fiatarone Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S.; American College of Sports Medicine. American College of Sports Medicine position stand. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef]
- Ekelund, U.; Tarp, J.; Steene-Johannessen, J.; Hansen, B.H.; Jefferis, B.; Fagerland, M.W.; Whincup, P.; Diaz, K.M.; Hooker, S.; Chernofsky, A.; et al. Dose-response associations between accelerometry measured physical activity and sedentary time and all cause mortality: Systematic review and harmonised meta-analysis. BMJ (Clin. Res. Ed.) 2019, 366, l4570. [Google Scholar] [CrossRef] [Green Version]
- Hansen, B.H.; Kolle, E.; Steene-Johannessen, J.; Dalene, K.E.; Ekelund, U.; Anderssen, S.A. Monitoring population levels of physical activity and sedentary time in Norway across the lifespan. Scand. J. Med. Sci. Sports 2019, 29, 105–112. [Google Scholar] [CrossRef] [Green Version]
- Lohne-Seiler, H.; Hansen, B.H.; Kolle, E.; Anderssen, S.A. Accelerometer-determined physical activity and self-reported health in a population of older adults (65–85 years): A cross-sectional study. BMC Public Health 2014, 14, 284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edholm, P.; Nilsson, A.; Kadi, F. Physical function in older adults: Impacts of past and present physical activity behaviors. Scand. J. Med. Sci. Sports 2019, 29, 415–421. [Google Scholar] [CrossRef]
- Hayashida, I.; Tanimoto, Y.; Takahashi, Y.; Kusabiraki, T.; Tamaki, J. Correlation between muscle strength and muscle mass, and their association with walking speed, in community-dwelling elderly Japanese individuals. PLoS ONE 2014, 9, e111810. [Google Scholar] [CrossRef] [PubMed]
- Cooper, A.; Lamb, M.; Sharp, S.J.; Simmons, R.K.; Griffin, S.J. Bidirectional association between physical activity and muscular strength in older adults: Results from the UK Biobank study. Int. J. Epidemiol. 2017, 46, 141–148. [Google Scholar] [CrossRef] [Green Version]
- Sardinha, L.B.; Santos, D.A.; Silva, A.M.; Baptista, F.; Owen, N. Breaking-up sedentary time is associated with physical function in older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 119–124. [Google Scholar] [CrossRef] [Green Version]
- Reitlo, L.S.; Sandbakk, S.B.; Viken, H.; Aspvik, N.P.; Ingebrigtsen, J.E.; Tan, X.; Wisløff, U.; Stensvold, D. Exercise patterns in older adults instructed to follow moderate-or high-intensity exercise protocol-the generation 100 study. BMC Geriatr. 2018, 18, 208. [Google Scholar] [CrossRef]
- Valenti, G.; Bonomi, A.G.; Westerterp, K.R. Walking as a contributor to physical activity in healthy older adults: 2 week longitudinal study using accelerometry and the doubly labeled water method. JMIR Mhealth Uhealth 2016, 4, e56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, C.J.; Latham, N.K. Progressive resistance strength training for improving physical function in older adults. Cochrane Database Syst. Rev. 2009, 2009, CD002759. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chin, A.P.M.J.; van Poppel, M.N.; van Mechelen, W. Effects of resistance and functional-skills training on habitual activity and constipation among older adults living in long-term care facilities: A randomized controlled trial. BMC Geriatr. 2006, 6, 9. [Google Scholar]
- Fiatarone, M.A.; O’Neill, E.F.; Ryan, N.D.; Clements, K.M.; Solares, G.R.; Nelson, M.E.; Roberts, S.B.; Kehayias, J.J.; Lipsitz, L.A.; Evans, W.J. Exercise training and nutritional supplementation for physical frailty in very elderly people. N. Engl. J. Med. 1994, 330, 1769–1775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saeterbakken, A.H.; Bardstu, H.B.; Brudeseth, A.; Andersen, V. Effects of strength training on muscle properties, physical function, and physical activity among frail older people: A pilot study. J. Aging Res. 2018, 2018, 8916274. [Google Scholar] [CrossRef]
- Strandberg, E.; Edholm, P.; Ponsot, E.; Wahlin-Larsson, B.; Hellmen, E.; Nilsson, A.; Engfeldt, P.; Cederholm, T.; Riserus, U.; Kadi, F. Influence of combined resistance training and healthy diet on muscle mass in healthy elderly women: A randomized controlled trial. J. Appl. Physiol. (1985) 2015, 119, 918–925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oesen, S.; Halper, B.; Hofmann, M.; Jandrasits, W.; Franzke, B.; Strasser, E.M.; Graf, A.; Tschan, H.; Bachl, N.; Quittan, M.; et al. Effects of elastic band resistance training and nutritional supplementation on physical performance of institutionalised elderly--A randomized controlled trial. Exp. Gerontol. 2015, 72, 99–108. [Google Scholar] [CrossRef]
- Buman, M.P.; Hekler, E.B.; Haskell, W.L.; Pruitt, L.; Conway, T.L.; Cain, K.L.; Sallis, J.F.; Saelens, B.; Frank, L.D.; King, A.C. Objective light-intensity physical activity associations with rated health in older adults. Am. J. Epidemiol. 2010, 172, 1155–1165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Rezende, L.F.; Rey-López, J.P.; Matsudo, V.K.; do Carmo Luiz, O. Sedentary behavior and health outcomes among older adults: A systematic review. BMC Public Health 2014, 14, 333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Global Action Plan on Physical Activity 2018–2030: More Active People for a Healthier World; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Franco, M.R.; Tong, A.; Howard, K.; Sherrington, C.; Ferreira, P.H.; Pinto, R.Z.; Ferreira, M.L. Older people’s perspectives on participation in physical activity: A systematic review and thematic synthesis of qualitative literature. Br. J. Sports Med. 2015, 49, 1268–1276. [Google Scholar] [CrossRef] [PubMed]
- Bårdstu, H.B.; Andersen, V.; Fimland, M.S.; Aasdahl, L.; Raastad, T.; Cumming, K.T.; Sæterbakken, A.H. Effectiveness of a resistance training program on physical function, muscle strength, and body composition in community-dwelling older adults receiving home care: A cluster-randomized controlled trial. Eur. Rev. Aging Phys. Act. 2020, 17, 11. [Google Scholar] [CrossRef] [PubMed]
- Campbell, M.K.; Piaggio, G.; Elbourne, D.R.; Altman, D.G. Consort 2010 statement: Extension to cluster randomised trials. BMJ (Clin. Res. Ed.) 2012, 345, e5661. [Google Scholar] [CrossRef] [Green Version]
- Fragala, M.S.; Cadore, E.L.; Dorgo, S.; Izquierdo, M.; Kraemer, W.J.; Peterson, M.D.; Ryan, E.D. Resistance training for older adults: Position statement from the national strength and conditioning association. J. Strength Cond. Res. 2019, 33, 2019–2052. [Google Scholar] [CrossRef] [PubMed]
- Helsedirektoratet. Anbefalinger om Kosthold, Ernæring og Fysisk Aktivitet; Contract No.: IS-2170; Helsedirektoratet: Oslo, Norway, 2014. [Google Scholar]
- ActiGraph, S. The Low-Frequency Filter Explained. 2012. Available online: https://actigraph.desk.com/customer/en/portal/articles/2515505-low-frequency-extension-explained (accessed on 15 October 2019).
- Choi, L.; Ward, S.C.; Schnelle, J.F.; Buchowski, M.S. Assessment of wear/nonwear time classification algorithms for triaxial accelerometer. Med. Sci. Sports Exerc. 2012, 44, 2009–2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motl, R.W.; McAuley, E.; Dlugonski, D. Reactivity in baseline accelerometer data from a physical activity behavioral intervention. Health Psychol. 2012, 31, 172–175. [Google Scholar] [CrossRef]
- Troiano, R.P.; Berrigan, D.; Dodd, K.W.; Masse, L.C.; Tilert, T.; McDowell, M. Physical activity in the United States measured by accelerometer. Med. Sci. Sports Exerc. 2008, 40, 181–188. [Google Scholar] [CrossRef]
- Aguilar-Farías, N.; Brown, W.J.; Peeters, G.M. ActiGraph GT3X+ cut-points for identifying sedentary behaviour in older adults in free-living environments. J. Sci. Med. Sport 2014, 17, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Barnett, A.; van den Hoek, D.; Barnett, D.; Cerin, E. Measuring moderate-intensity walking in older adults using the ActiGraph accelerometer. BMC Geriatr. 2016, 16, 211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fitzmaurice, G.M.; Laird, N.M.; Ware, J.H. Applied Longitudinal Analysis, 2nd ed.; Wiley: Hoboken, NJ, USA, 2011; p. 752. [Google Scholar]
- Coupland, C.; DiGuiseppi, C. The design and use of cluster randomised controlled trials in evaluating injury prevention interventions: Part 2. Design effect, sample size calculations and methods for analysis. Inj. Prev. 2010, 16, 132–136. [Google Scholar] [CrossRef] [PubMed]
- de Vries, N.M.; van Ravensberg, C.D.; Hobbelen, J.S.; Olde Rikkert, M.G.; Staal, J.B.; Nijhuis-van der Sanden, M.W. Effects of physical exercise therapy on mobility, physical functioning, physical activity and quality of life in community-dwelling older adults with impaired mobility, physical disability and/or multi-morbidity: A meta-analysis. Ageing Res. Rev. 2012, 11, 136–149. [Google Scholar] [CrossRef] [PubMed]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- dos Santos, L.; Ribeiro, A.S.; Nunes, J.P.; Tomeleri, C.M.; Nabuco, H.C.G.; Nascimento, M.A.; Junior, P.S.; Fernandes, R.R.; Campa, F.; Toselli, S.; et al. Effects of pyramid resistance-training system with different repetition zones on cardiovascular risk factors in older women: A randomized controlled trial. Int. J. Environ. Res. Public Health 2020, 17, 6115. [Google Scholar] [CrossRef]
- Toselli, S.; Badicu, G.; Bragonzoni, L.; Spiga, F.; Mazzuca, P.; Campa, F. Comparison of the effect of different resistance training frequencies on phase angle and handgrip strength in obese women: A randomized controlled trial. Int. J. Environ. Res. Public Health 2020, 17, 1163. [Google Scholar] [CrossRef] [Green Version]
- Talbot, L.A.; Gaines, J.M.; Huynh, T.N.; Metter, E.J. A home-based pedometer-driven walking program to increase physical activity in older adults with osteoarthritis of the knee: A preliminary study. J. Am. Geriatr. Soc. 2003, 51, 387–392. [Google Scholar] [CrossRef]
- van der Bij, A.K.; Laurant, M.G.; Wensing, M. Effectiveness of physical activity interventions for older adults: A review. Am. J. Prev. Med. 2002, 22, 120–133. [Google Scholar] [CrossRef]
- Harris, T.; Kerry, S.M.; Limb, E.S.; Victor, C.R.; Iliffe, S.; Ussher, M.; Whincup, P.H.; Ekelund, U.; Fox-Rushby, J.; Furness, C.; et al. Effect of a primary care walking intervention with and without nurse support on physical activity levels in 45- to 75-year-olds: The pedometer and consultation evaluation (PACE-UP) cluster randomised clinical trial. PLoS Med. 2017, 14, e1002210. [Google Scholar] [CrossRef]
- Meijer, E.P.; Westerterp, K.R.; Verstappen, F.T. Effect of exercise training on total daily physical activity in elderly humans. Eur. J. Appl. Physiol. Occup. Physiol. 1999, 80, 16–21. [Google Scholar] [CrossRef]
- Migueles, J.H.; Cadenas-Sanchez, C.; Ekelund, U.; Delisle Nystrom, C.; Mora-Gonzalez, J.; Lof, M.; Labayen, I.; Ruiz, J.R.; Ortega, F.B. Accelerometer data collection and processing criteria to assess physical activity and other outcomes: A systematic review and practical considerations. Sports Med. 2017, 47, 1821–1845. [Google Scholar] [CrossRef]
- Davis, M.G.; Fox, K.R.; Hillsdon, M.; Sharp, D.J.; Coulson, J.C.; Thompson, J.L. Objectively measured physical activity in a diverse sample of older urban UK adults. Med. Sci. Sports Exerc. 2011, 43, 647–654. [Google Scholar] [CrossRef]
- Aspvik, N.P.; Viken, H.; Zisko, N.; Ingebrigtsen, J.E.; Wisloff, U.; Stensvold, D. Are older adults physically active enough-A matter of assessment method? The generation 100 study. PLoS ONE 2016, 11, e0167012. [Google Scholar] [CrossRef]
- Feito, Y.; Hornbuckle, L.M.; Reid, L.A.; Crouter, S.E. Effect of ActiGraph’s low frequency extension for estimating steps and physical activity intensity. PLoS ONE 2017, 12, e0188242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sasaki, J.E.; Júnior, J.H.; Meneguci, J.; Tribess, S.; Júnior, M.M.; Neto, A.S.; Júnior, J.S.V. Number of days required for reliably estimating physical activity and sedentary behaviour from accelerometer data in older adults. J. Sports Sci. 2018, 36, 1572–1577. [Google Scholar] [CrossRef]
- Aspvik, N.P.; Viken, H.; Ingebrigtsen, J.E.; Zisko, N.; Mehus, I.; Wisløff, U.; Stensvold, D. Do weather changes influence physical activity level among older adults? The Generation 100 study. PLoS ONE 2018, 13, e0199463. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | RTG (n = 64) | CG (n = 43) | ICC |
|---|---|---|---|
| Age (years), median (IQR) | 87 (80–90) | 86 (80–90) | |
| Women, n (%) | 42 (66) | 22 (51) | |
| Use of walking devices, n (%) * | 33 (52) | 31 (72) | |
| Height (cm), mean (SD) | 160 (9) | 164 (9) | |
| Weight (kg), median (IQR) | 66.5 (55.5–79.5) a | 70.4 (62.4–80.2) b | |
| Body Mass Index (kg/m2), median (IQR) | 25.1 (23.6–28.1) a | 27.0 (23.7–30.3) b | |
| Wear time (min/day), mean (SD) § | 805 (77) c | 817 (70) d | |
| Number of valid days, median (IQR) § | 13 (12–14) c | 13 (11–14) d | |
| TPA (cpm), mean (SD) | 278 (165) c | 224 (138) d | 0.16 |
| SB (min/day), mean (SD) | 600 (100) c | 643 (85) c | 0.10 |
| LPA (min/day), mean (SD) | 170 (73) c | 145 (64) c | 0.10 |
| MVPA (min/day), mean (SD) | 35 (35) c | 29 (30) d | 0.16 |
| Steps (steps/day), mean (SD) | 6623 (3258) c | 5223 (2623) d | 0.18 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bårdstu, H.B.; Andersen, V.; Fimland, M.S.; Aasdahl, L.; Lohne-Seiler, H.; Saeterbakken, A.H. Physical Activity Level Following Resistance Training in Community-Dwelling Older Adults Receiving Home Care: Results from a Cluster-Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2021, 18, 6682. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136682
Bårdstu HB, Andersen V, Fimland MS, Aasdahl L, Lohne-Seiler H, Saeterbakken AH. Physical Activity Level Following Resistance Training in Community-Dwelling Older Adults Receiving Home Care: Results from a Cluster-Randomized Controlled Trial. International Journal of Environmental Research and Public Health. 2021; 18(13):6682. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136682
Chicago/Turabian StyleBårdstu, Hilde Bremseth, Vidar Andersen, Marius Steiro Fimland, Lene Aasdahl, Hilde Lohne-Seiler, and Atle Hole Saeterbakken. 2021. "Physical Activity Level Following Resistance Training in Community-Dwelling Older Adults Receiving Home Care: Results from a Cluster-Randomized Controlled Trial" International Journal of Environmental Research and Public Health 18, no. 13: 6682. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18136682