
Risk Perception and Coping Behavior of Construction Workers on Occupational Health Risks—A Case Study of Nanjing, China



Abstract
:1. Introduction
2. Literature Review
2.1. Occupational Health Risk
2.2. Risk Perception
2.3. Coping Behavior
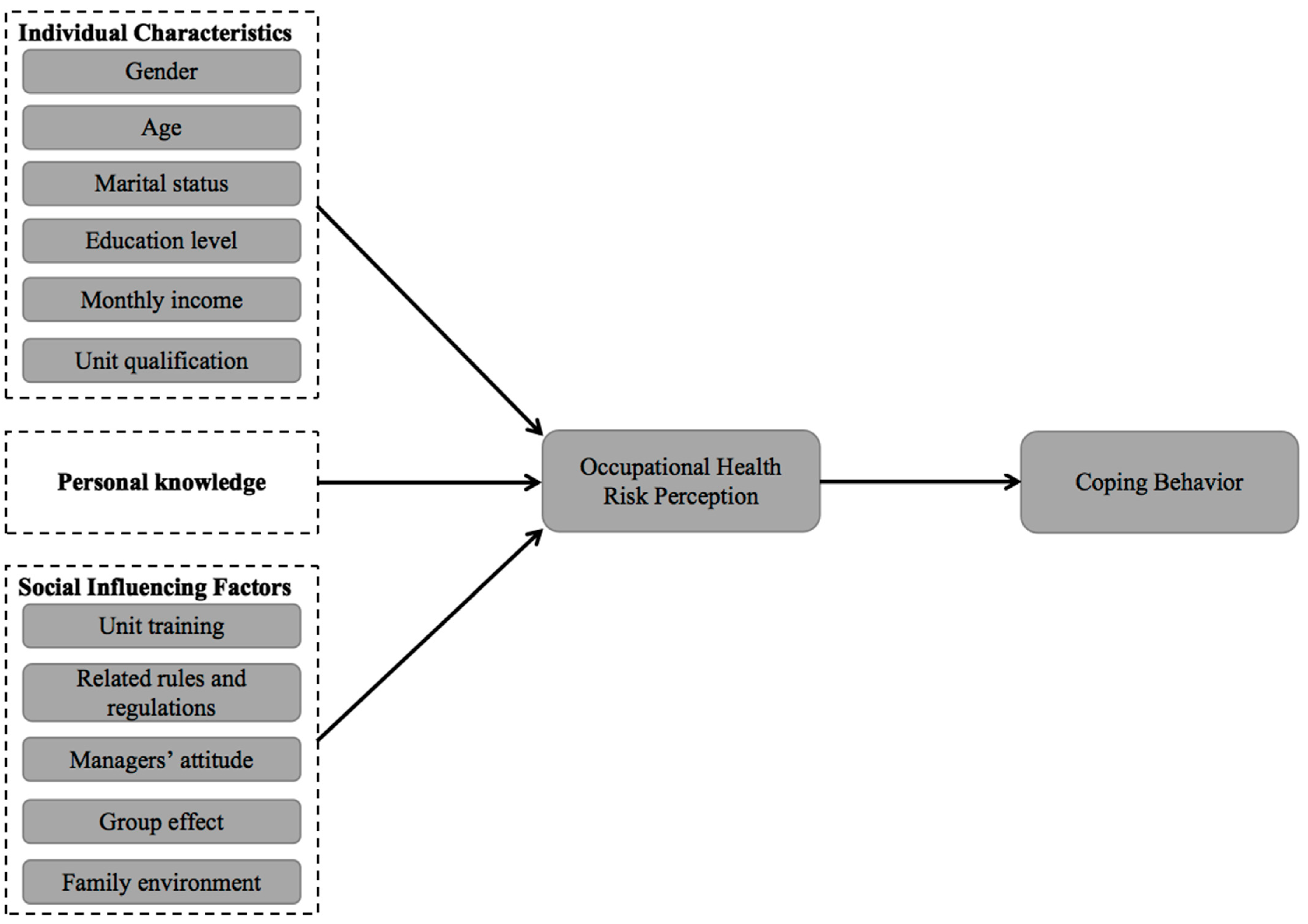
3. Hypothesis Development
4. Methodology
5. Results
5.1. Current Risk Perception Level and Coping Behavior Level of Construction Workers
5.2. Hypothetical Test
5.2.1. Differences Analysis of Individual Characteristics in Occupational Health Risk Perception
5.2.2. The Impact of Personal Knowledge on Risk Perception
5.2.3. The Impact of Social Influencing Factors on Risk Perception
5.2.4. The Impact of Risk Perception on Coping Behavior
5.2.5. Mediating Effect of Risk Perception
6. Discussion
6.1. Risk Perception Level and Coping Behavior Level of Construction Workers
6.2. Differences in Perception of Occupational Health Risk
6.3. Influencing Factors on Occupational Health Risk Perception
6.4. The Mediating Effect of Occupational Health Risk Perception
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Oswald, D.; Sherratt, F.; Smith, S. Problems with safety observation reporting: A construction industry case study. Saf. Sci. 2018, 107, 35–45. [Google Scholar] [CrossRef]
- Loosemore, M.; Malouf, N. Safety training and positive safety attitude formation in the Australian construction industry. Saf. Sci. 2019, 113, 233–243. [Google Scholar] [CrossRef]
- Buniya, M.K.; Othman, I.; Sunindijo, R.Y.; Kineber, A.F.; Mussi, E.; Ahmad, H. Barriers to safety program implementation in the construction industry. Ain Shams Eng. J. 2021, 12, 65–72. [Google Scholar] [CrossRef]
- Li, S.; Xiang, X. The establishment of cause-system of poor construction site safety and priority analysis from different perspectives. World Acad. Sci. Eng. Technol. 2011, 57, 570–574. [Google Scholar]
- Jin, R.; Zou, P.X.; Piroozfar, P.; Wood, H.; Yang, Y.; Yan, L.; Han, Y. A science mapping approach based review of construction safety research. Saf. Sci. 2019, 113, 285–297. [Google Scholar] [CrossRef]
- Cheung, W.F.; Lin, T.H.; Lin, Y.C. A real-time construction safety monitoring system for hazardous gas integrating wireless sensor network and building information modeling technologies. Sensors 2018, 18, 436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teizer, J. Right-time vs. real-time pro-active construction safety and health system architecture. Constr. Innov. 2016, 16, 253–280. [Google Scholar] [CrossRef]
- Wang, J.; Zou, P.X.; Li, P.P. Critical factors and paths influencing construction workers’ safety risk tolerances. Accid. Anal. Prev. 2016, 93, 267–279. [Google Scholar] [CrossRef] [PubMed]
- Harsini, A.Z.; Ghofranipour, F.; Sanaeinasab, H.; Shokravi, F.A.; Bohle, P.; Matthews, L.R. Factors associated with unsafe work behaviours in an Iranian petrochemical company: Perspectives of workers, supervisors, and safety managers. BMC Public Health 2020, 20, 1192–1204. [Google Scholar] [CrossRef]
- Lingard, H. Occupational health and safety in the construction industry. Constr. Manag. Econ. 2013, 31, 505–514. [Google Scholar] [CrossRef]
- Calkins, M. Materials for Sustainable Sites: A Complete Guide to the Evaluation, Selection, and Use of Sustainable Construction Materials; John Wiley & Sons: Hoboken, NJ, USA, 2008. [Google Scholar]
- Sousa, V.; Almeida, N.M.; Dias, L.A. Risk-based management of occupational safety and health in the construction industry-Part 1: Background knowledge. Saf. Sci. 2014, 66, 75–86. [Google Scholar] [CrossRef]
- Fang, W.; Ma, L.; Love, P.E.; Luo, H.; Ding, L.; Zhou, A. Knowledge graph for identifying hazards on construction sites: Integrating computer vision with ontology. Autom. Constr. 2020, 119, 103310. [Google Scholar] [CrossRef]
- Lucas, R.A.; Epstein, Y.; Kjellstrom, T. Excessive occupational heat exposure: A significant ergonomic challenge and health risk for current and future workers. Extrem. Physiol. Med. 2014, 3, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Si, Y. Quality Management of Construction Site of Construction Decoration Engineering. J. Archit. Res. Dev. 2017, 1, 30–32. [Google Scholar] [CrossRef] [Green Version]
- Leijten, F.R.; van den Heuvel, S.G.; Ybema, J.F.; van der Beek, A.J.; Robroek, S.J.; Burdorf, A. The influence of chronic health problems on work ability and productivity at work: A longitudinal study among older employees. Scand. J. Work Environ. Health 2014, 40, 473–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kazaz, A.; Ulubeyli, S.; Tuncbilekli, N.A. Causes of delays in construction projects in Turkey. J. Civ. Eng. Manag. 2012, 18, 426–435. [Google Scholar] [CrossRef] [Green Version]
- Shah, R.K. An exploration of causes for delay and cost overrun in construction projects: A case study of Australia, Malaysia & Ghana. J. Adv. Coll. Eng. Manag. 2016, 2, 41–55. [Google Scholar]
- Dorji, K.; Hadikusumo, B.H. Safety management practices in the Bhutanese construction industry. J. Constr. Dev. Ctries. 2012, 11, 53–75. [Google Scholar]
- Langford, D.; Rowlinson, S.; Sawacha, E. Safety behaviour and safety management: Its influence on the attitudes of workers in the UK construction industry. Eng. Constr. Archit. Manag. 2000, 7, 133–140. [Google Scholar] [CrossRef]
- Varianou-Mikellidou, C.; Boustras, G.; Dimopoulos, C.; Wybo, J.L.; Guldenmund, F.W.; Nicolaidou, O.; Anyfantis, I. Occupational health and safety management in the context of an ageing workforce. Saf. Sci. 2019, 116, 231–244. [Google Scholar] [CrossRef]
- Chen, Y. Prevention and Control of Occupational Hazards in Decoration Work. J. Occup. Health Damage 2016, 31, 50–54. (In Chinese) [Google Scholar]
- Chen, C.; Zhao, B. Review of relationship between indoor and outdoor particles: I/O ratio, infiltration factor and penetration factor. Atmos. Environ. 2011, 45, 275–288. [Google Scholar] [CrossRef]
- Davis, J.M.; Akese, G.; Garb, Y. Beyond the pollution haven hypothesis: Where and why do e-waste hubs emerge and what does this mean for policies and interventions? Geoforum 2019, 98, 36–45. [Google Scholar] [CrossRef]
- Ma, G.; Gong, L. Indoor Air Pollution Caused by Interior Architecture Decoration and Reason of Not Absolutely Forbidden. In Proceedings of the 4th International Conference on Bioinformatics and Biomedical Engineering, Chengdu, China, 18–20 June 2010; IEEE: New York, NY, USA, 2010; pp. 1–3. [Google Scholar]
- Huang, Y.; Liu, C.M.; Li, S.Y.; Zhou, J.S.; Liu, Y.C.; Long, J.B. Study on Influence of Indoor Decoration Risk Factors in Workers. Shiyong Yufang Yixue 2007, 14, 328–330. (In Chinese) [Google Scholar]
- Lu, M.L.; Waters, T.R.; Krieg, E.; Werren, D. Efficacy of the revised NIOSH lifting equation to predict risk of low-back pain associated with manual lifting: A one-year prospective study. Hum. Factors 2014, 56, 73–85. [Google Scholar] [CrossRef]
- Campos-Serna, J.; Ronda-Pérez, E.; Artazcoz, L.; Moen, B.E.; Benavides, F.G. Gender inequalities in occupational health related to the unequal distribution of working and employment conditions: A systematic review. Int. J. Equity Health 2013, 12, 57–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ndejjo, R.; Musinguzi, G.; Yu, X.; Buregyeya, E.; Musoke, D.; Wang, J.S.; Ssempebwa, J. Occupational health hazards among healthcare workers in Kampala, Uganda. J. Environ. Public Health 2015, 2015, 913741. [Google Scholar] [CrossRef] [Green Version]
- Stocks, S.J.; Turner, S.; McNamee, R.; Carder, M.; Hussey, L.; Agius, R.M. Occupation and work-related ill-health in UK construction workers. Occup. Med. 2011, 61, 407–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Song, Z.; Wang, T.; Zheng, Y.; Ning, X. Health impacts of construction noise on workers: A quantitative assessment model based on exposure measurement. J. Clean. Prod. 2016, 135, 721–731. [Google Scholar] [CrossRef] [Green Version]
- Tong, R.; Cheng, M.; Zhang, L.; Liu, M.; Yang, X.; Li, X.; Yin, W. The construction dust-induced occupational health risk using Monte-Carlo simulation. J. Clean. Prod. 2018, 184, 598–608. [Google Scholar] [CrossRef]
- Chen, X.; Guo, C.; Song, J.; Wang, X.; Cheng, J. Occupational health risk assessment based on actual dust exposure in a tunnel construction adopting roadheader in Chongqing, China. Build. Environ. 2019, 165, 106415. [Google Scholar] [CrossRef]
- Sámano-Ríos, M.L.; Ijaz, S.; Ruotsalainen, J.; Breslin, F.C.; Gummesson, K.; Verbeek, J. Occupational safety and health interventions to protect young workers from hazardous work-a scoping review. Saf. Sci. 2019, 113, 389–403. [Google Scholar] [CrossRef]
- Khan, M.W.; Ali, Y.; De Felice, F.; Petrillo, A. Occupational health and safety in construction industry in Pakistan using modified-SIRA method. Saf. Sci. 2019, 118, 109–118. [Google Scholar] [CrossRef]
- Başağa, H.B.; Temel, B.A.; Atasoy, M.; Yıldırım, İ. A study on the effectiveness of occupational health and safety trainings of construction workers in Turkey. Saf. Sci. 2018, 110, 344–354. [Google Scholar] [CrossRef]
- Dingsdag, D.P.; Biggs, H.C.; Sheahan, V.L. Understanding and defining OH&S competency for construction site positions: Worker perceptions. Saf. Sci. 2008, 46, 619–633. [Google Scholar]
- Pinto, A.; Nunes, I.L.; Ribeiro, R.A. Occupational risk assessment in construction industry–Overview and reflection. Saf. Sci. 2011, 49, 616–624. [Google Scholar] [CrossRef]
- Kartam, N.A.; Flood, I.; Koushki, P. Construction safety in Kuwait: Issues, procedures, problems, and recommendations. Saf. Sci. 2000, 36, 163–184. [Google Scholar] [CrossRef]
- Tesfaye, S.; Hamba, N.; Gerbi, A.; Negeri, Z. Occupational formaldehyde exposure linked to increased systemic health impairments and counteracting beneficial effects of selected antioxidants. Alex. J. Med. 2021, 57, 157–167. [Google Scholar]
- Jones, W.; Gibb, A.; Haslam, R.; Dainty, A. Work-related ill-health in construction: The importance of scope, ownership and understanding. Saf. Sci. 2019, 120, 538–550. [Google Scholar] [CrossRef]
- Starr, C. Social benefit versus technological risk. Science 1969, 165, 1232–1238. [Google Scholar] [CrossRef] [PubMed]
- Slovic, P. Perception of risk. Science 1987, 236, 280–285. [Google Scholar] [CrossRef] [PubMed]
- Slovic, P. The Perception of Risk. Risk Soc. Policy 2000, 69, 112. [Google Scholar]
- Desai, S.D.; Sondak, H.; Diekmann, K.A. When fairness neither satisfies nor motivates: The role of risk aversion and uncertainty reduction in attenuating and reversing the fair process effect. Organ. Behav. Hum. Decis. Process 2011, 116, 32–45. [Google Scholar] [CrossRef]
- Scherer, C.W.; Cho, H. A social network contagion theory of risk perception. Risk Anal. Int. J. 2003, 23, 261–267. [Google Scholar] [CrossRef] [PubMed]
- Leiserowitz, A. Climate Change Risk Perception and Policy Preferences: The Role of Affect, Imagery, and Values. Clim. Chang. 2006, 77, 45–72. [Google Scholar] [CrossRef] [Green Version]
- Fyhri, A.; Backer-Grondahl, A. Personality and risk perception in transport. Accid. Anal. Prev. 2012, 49, 470–475. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.K.; Taylor, R.W. Assessing the role of risk perception in ensuring sustainable arsenic mitigation. Groundw. Sustain. Dev. 2019, 9, 100241. [Google Scholar] [CrossRef]
- Fernandez, G.; Tun, A.M.; Okazaki, K.; Zaw, S.H.; Kyaw, K. Factors influencing fire, earthquake, and cyclone risk perception in Yangon, Myanmar. Int. J. Disaster Risk Reduct. 2018, 28, 140–149. [Google Scholar] [CrossRef]
- Jeong, J.H.; Kim, J.S. Health literacy, health risk perception and health behavior of elders. J. Korean Acad. Community Health Nurs. 2014, 25, 65–73. [Google Scholar] [CrossRef]
- Renner, B.; Schupp, H.; Vollmann, M.; Hartung, F.M.; Schmälzle, R.; Panzer, M. Risk perception, risk communication and health behavior change: Health psychology at the University of Konstanz. Zeitschrift für Gesundheitspsychologie 2008, 16, 150–153. [Google Scholar] [CrossRef]
- Orru, K.; Nordin, S.; Harzia, H.; Orru, H. The role of perceived air pollution and health risk perception in health symptoms and disease: A population-based study combined with modelled levels of PM 10. Int. Arch. Occup. Environ. Health 2018, 91, 581–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Motta Zanin, G.; Gentile, E.; Parisi, A.; Spasiano, D. A preliminary evaluation of the public risk perception related to the COVID-19 health emergency in Italy. Int. J. Environ. Res. Public Health 2020, 17, 3024. [Google Scholar] [CrossRef]
- Namian, M.; Albert, A.; Feng, J. Effect of distraction on hazard reperception and safety risk perception. J. Constr. Eng. Manag. 2018, 144, 04018008. [Google Scholar] [CrossRef]
- Xia, N.; Wang, X.; Griffin, M.A.; Wu, C.; Liu, B. Do we see how they perceive risk? An integrated analysis of risk perception and its effect on workplace safety behavior. Accid. Anal. Prev. 2017, 106, 234–242. [Google Scholar] [CrossRef]
- Alomari, K.A.; Gambatese, J.A.; Tymvios, N. Risk perception comparison among construction safety professionals: Delphi perspective. J. Constr. Eng. Manag. 2018, 144, 04018107. [Google Scholar] [CrossRef]
- Chaswa, E.N.; Kosamu, I.B.M.; Kumwenda, S.; Utembe, W. Risk perception and its influencing factors among construction workers in Malawi. Safety 2020, 6, 33. [Google Scholar] [CrossRef]
- Man, S.S.; Ng, J.Y.K.; Chan, A.H.S. A review of the risk perception of construction workers in construction safety. In Proceedings of the International Conference on Human Systems Engineering and Design: Future Trends and Applications, Munich, Germany, 16–18 September 2019; Springer: Berlin/Heidelberg, Germany, 2019; pp. 637–643. [Google Scholar]
- Brewer, N.T.; Chapman, G.B.; Gibbons, F.X.; Gerrard, M.; McCaul, K.D.; Weinstein, N.D. Meta-analysis of the relationship between risk perception and health behavior: The example of vaccination. Health Psychol. 2007, 26, 136–145. [Google Scholar] [CrossRef] [Green Version]
- Strickland, J.R.; Wagan, S.; Dale, A.M.; Evanoff, B.A. Prevalence and perception of risky health behaviors among construction workers. J. Occup. Environ. Med. 2017, 59, 673–678. [Google Scholar] [CrossRef] [PubMed]
- Gürcanlı, G.E.; Baradan, S.; Uzun, M. Risk perception of construction equipment operators on construction sites of Turkey. Int. J. Ind. Ergon. 2015, 46, 59–68. [Google Scholar] [CrossRef]
- Arezes, P.M.; Miguel, A.S. Hearing protection use in industry: The role of risk perception. Saf. Sci. 2005, 43, 253–267. [Google Scholar] [CrossRef]
- Ganster, D.C.; Rosen, C.C. Work stress and employee health: A multidisciplinary review. J. Manag. 2013, 39, 1085–1122. [Google Scholar] [CrossRef]
- Aven, T. Risk assessment and risk management: Review of recent advances on their foundation. Eur. J. Oper. Res. 2016, 253, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Lazarus, R.S.; Folkman, S. Stress, Appraisal, and Coping; Springer Publishing Company: Berlin, Germany, 1984. [Google Scholar]
- Compas, B.E.; Connor-Smith, J.K.; Saltzman, H.; Thomsen, A.H.; Wadsworth, M.E. Coping with stress during childhood and adolescence: Problems, progress, and potential in theory and research. Psychol. Bull. 2001, 127, 87–127. [Google Scholar] [CrossRef] [PubMed]
- Chan, I.Y.; Leung, M.Y.; Yuan, T. Structural relationships between cultural values and coping behaviors of professionals in the stressful construction industry. Eng. Constr. Archit. Manag. 2014, 21, 133–151. [Google Scholar] [CrossRef]
- Lindell, M.K.; Perry, R.W. The protective action decision model: Theoretical modifications and additional evidence. Risk Anal. Int. J. 2012, 32, 616–632. [Google Scholar] [CrossRef]
- Trumbo, C.W. Heuristic-systematic information processing and risk judgment. Risk Anal. 1999, 19, 391–400. [Google Scholar] [CrossRef]
- Leung, M.Y.; Chan, I.Y.S.; Cooper, C. Stress Management in the Construction Industry; John Wiley & Sons: New York, NY, USA, 2014. [Google Scholar]
- Tillmann, J.N.; Beard, M.T. Manager’s healthy lifestyles, coping strategies, job stressors and performance: An occupational stress model. J. Theory Constr. Test. 2001, 5, 7. [Google Scholar]
- Gal-Tzur, A.; Grant-Muller, S.M.; Minkov, E.; Nocera, S. The impact of social media usage on transport policy: Issues, challenges and recommendations. Proc. Soc. Behav. Sci. 2014, 111, 937–946. [Google Scholar] [CrossRef] [Green Version]
- Jackson, S.A.; Kleitman, S. Individual differences in decision-making and confidence: Capturing decision tendencies in a fictitious medical test. Metacogn. Learn. 2014, 9, 25–49. [Google Scholar] [CrossRef]
- Tamres, L.K.; Janicki, D.; Helgeson, V.S. Sex differences in coping behavior: A meta-analytic review and an examination of relative coping. Personal. Soc. Psychol. Rev. 2002, 6, 2–30. [Google Scholar] [CrossRef]
- Martin, P.; Rott, C.; Poon, L.W.; Courtenay, B.; Lehr, U. A molecular view of coping behavior in older adults. J. Aging Health 2001, 13, 72–91. [Google Scholar] [CrossRef] [PubMed]
- Liang, Q.; Leung, M.Y.; Ahmed, K. How adoption of coping behaviors determines construction workers’ safety: A quantitative and qualitative investigation. Saf. Sci. 2021, 133, 105035. [Google Scholar] [CrossRef]
- Ohira, T.; Tanigawa, T.; Iso, H.; Sankai, T.; Imano, H.; Shimamoto, T. Impact of anger expression on blood pressure levels in white-color workers with low-coping behavior. Environ. Health Prev. Med. 2000, 5, 37–42. [Google Scholar] [CrossRef] [PubMed]
- Nwaogu, J.M.; Chan, A.P.; Tetteh, M.O. Staff resilience and coping behavior as protective factors for mental health among construction tradesmen. J. Eng. Des. Technol. 2021. ahead of print. [Google Scholar]
- Park, C.; Kim, Y.; Jeong, M. Influencing factors on risk perception of IoT-based home energy management services. Telemat. Inform. 2018, 35, 2355–2365. [Google Scholar] [CrossRef]
- Park, J.W.; Cho, Y.K.; Khodabandelu, A. Sensor-based safety performance assessment of individual construction workers. Sensors 2018, 18, 3897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanco, N.J.; Love, B.C.; Ramscar, M.; Otto, A.R.; Smayda, K.; Maddox, W.T. Exploratory decision-making as a function of lifelong experience, not cognitive decline. J. Exp. Psychol. Gen. 2016, 145, 284. [Google Scholar] [CrossRef]
- Ren, X.; Che, Y.; Yang, K.; Tao, Y. Risk perception and public acceptance toward a highly protested Waste-to-Energy facility. Waste Manag. 2016, 48, 528–539. [Google Scholar] [CrossRef]
- Visschers, V.H.; Siegrist, M. Differences in risk perception between hazards and between individuals. In Psychological Perspectives on Risk and Risk Analysis; Springer: Berlin/Heidelberg, Germany, 2018; pp. 63–80. [Google Scholar]
- Aluko, O.O.; Adebayo, A.E.; Adebisi, T.F.; Ewegbemi, M.K.; Abidoye, A.T.; Popoola, B.F. Knowledge, attitudes and perceptions of occupational hazards and safety practices in Nigerian healthcare workers. BMC Res. Notes 2016, 9, 71–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Namian, M.; Albert, A.; Zuluaga, C.M.; Behm, M. Role of safety training: Impact on hazard reperception and safety risk perception. J. Constr. Eng. Manag. 2016, 142, 04016073. [Google Scholar] [CrossRef]
- Diaz, Y.F. Predicting Employee Compliance with Safety Regulations, Factoring Risk Perception; FIU Electronic Theses and Dissertations: Miam, FL, USA, 2000. [Google Scholar]
- Zhao, X.; Hwang, B.G.; Low, S.P. Critical success factors for enterprise risk management in Chinese construction companies. Constr. Manag. Econ. 2013, 31, 1199–1214. [Google Scholar] [CrossRef]
- DeHart-Davis, L.; Pandey, S.K. Red tape and public employees: Does perceived rule dysfunction alienate managers? J. Public Adm. Res. Theory 2005, 15, 133–148. [Google Scholar] [CrossRef]
- Liang, H.; Lin, K.Y.; Zhang, S.; Su, Y. The impact of coworkers’ safety violations on an individual worker: A social contagion effect within the construction crew. Int. J. Environ. Res. Public Health 2018, 15, 773. [Google Scholar] [CrossRef] [Green Version]
- Man, S.S.; Chan, A.H.; Wong, H.M. Risk-taking behaviors of Hong Kong construction workers–A thematic study. Saf. Sci. 2017, 98, 25–36. [Google Scholar] [CrossRef]
- De Dominicis, S.; Fornara, F.; Cancellieri, U.G.; Twigger-Ross, C.; Bonaiuto, M. We are at risk, and so what? Place attachment, environmental risk perceptions and preventive coping behaviours. J. Environ. Psychol. 2015, 43, 66–78. [Google Scholar] [CrossRef]
- Nie, R.; Han, Y.; Xu, J.; Huang, Q.; Mao, J. Illness perception, risk perception and health promotion self-care behaviors among Chinese patient with type 2 diabetes: A cross-sectional survey. Appl. Nurs. Res. 2018, 39, 89–96. [Google Scholar] [CrossRef]
- Xu, J.; Tan, H. Differentiated effects of risk perception and causal attribution on public behavioral responses to air pollution: A segmentation analysis. J. Environ. Psychol. 2019, 65, 101335. [Google Scholar]
- Joffre, O.M.; Poortvliet, P.M.; Klerkx, L. Are shrimp farmers actual gamblers? An analysis of risk perception and risk management behaviors among shrimp farmers in the Mekong Delta. Aquaculture 2018, 495, 528–537. [Google Scholar] [CrossRef]
- Lim, T.S.; Mail, R.; Karim, M.R.A.; Ulum, Z.K.A.B.; Jaidi, J.; Noordin, R. A serial mediation model of financial knowledge on the intention to invest: The central role of risk perception and attitude. J. Behav. Exp. Financ. 2018, 20, 74–79. [Google Scholar] [CrossRef]
- Boo, S.; Froelicher, E.S. Cardiovascular risk factors and 10-year risk for coronary heart disease in Korean women. Asian Nurs. Res. 2012, 6, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hong, Y.; Kim, J.; Xiong, L. Media exposure and individuals’ emergency preparedness behaviors for coping with natural and human-made disasters. J. Environ. Psychol. 2019, 63, 82–91. [Google Scholar] [CrossRef]
- Li, C.Z.; Zhao, Y.; Xu, X. Investigation of dust exposure and control practices in the construction industry: Implications for cleaner production. J. Clean. Prod. 2019, 227, 810–824. [Google Scholar] [CrossRef]
- Shim, H.; Choi, G. Study of construction convergence technology for performance improvement in functional building materials. J. Build. Eng. 2017, 11, 108–114. [Google Scholar] [CrossRef]
- Wu, Z.; Zhang, X.; Wu, M. Mitigating construction dust pollution: State of the art and the way forward. J. Clean. Prod. 2016, 112, 1658–1666. [Google Scholar] [CrossRef]
- Zhuo, J. Research on Prevention of Indoor Air Environment Pollution by Building Decoration Materials. In Proceedings of the 2018 International Conference on Air Pollution and Environmental Engineering (APEE 2018), Hong Kong, China, 26–28 October 2018; pp. 26–28. [Google Scholar]
- Xia, C.F. Discussion on indoor formaldehyde treatment. Appl. Mech. Mater. 2012, 178–181, 280–283. [Google Scholar] [CrossRef]
- Chong, D.; Wang, Y.; Zhao, K.; Wang, D.; Oeser, M. Asphalt fume exposures by pavement construction workers: Current status and project cases. J. Constr. Eng. Manag. 2018, 144, 05018002. [Google Scholar] [CrossRef]
- Cui, P.; Schito, G.; Cui, Q. VOC emissions from asphalt pavement and health risks to construction workers. J. Clean. Prod. 2020, 244, 118757. [Google Scholar] [CrossRef]
- Cincinelli, A.; Martellini, T. Indoor air quality and health. Int. J. Environ. Res. Public Health 2017, 14, 1286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, L. Analysis of Indoor Air Pollution of Decoration and Control Measures. In Proceedings of the 3rd International Conference on Advances in Environment Research, Beijing, China, 23–25 May 2017; pp. 23–25. [Google Scholar]
- Li, H.; Li, X.; Luo, X.; Siebert, J. Investigation of the causality patterns of non-helmet use behavior of construction workers. Autom. Constr. 2017, 80, 95–103. [Google Scholar] [CrossRef]
- Lette, A.; Ambelu, A.; Getahun, T.; Mekonen, S. A survey of work-related injuries among building construction workers in southwestern Ethiopia. Int. J. Ind. Ergon. 2018, 68, 57–64. [Google Scholar] [CrossRef]
- Tadesse, S.; Israel, D. Occupational injuries among building construction workers in Addis Ababa, Ethiopia. J. Occup. Med. Toxicol. 2016, 11, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Weidman, J.; Dickerson, D.E.; Koebel, C.T. Effective intervention strategy to improve worker readiness to adopt ventilated tools. J. Constr. Eng. Manag. 2016, 142, 04016028. [Google Scholar] [CrossRef]
- Chen, F.; Zhang, H.; Chen, X.; Ren, J. Design method for interior decoration pollution control of buildings: Introduction and application. In Building Simulation; Tsinghua University Press: Beijing, China, 2020; pp. 1–10. [Google Scholar]
- Li, D.; Jia, J.; Zheng, T.; Cheng, X.; Yu, X. Construction and characterization of visible light active Pd nano-crystallite decorated and CNS-co-doped TiO2 nanosheet array photoelectrode for enhanced photocatalytic degradation of acetylsalicylic acid. Appl. Catal. B Environ. 2016, 188, 259–271. [Google Scholar] [CrossRef]
- Liqun, G.; Yanqun, G. Study on building materials and indoor pollution. Procedia Eng. 2011, 21, 789–794. [Google Scholar] [CrossRef] [Green Version]
- Sawicki, M.; Szóstak, M. Impact of Alcohol on Occupational Health and Safety in the Construction Industry at Workplaces with Scaffoldings. Appl. Sci. 2020, 10, 6690. [Google Scholar] [CrossRef]
- Vitharana, V.H.P.; Chinda, T. Structural equation modelling of lower back pain due to whole-body vibration exposure in the construction industry. Int. J. Occup. Saf. Ergon. 2019, 25, 257–267. [Google Scholar] [CrossRef] [PubMed]
- Chang, T.; Ren, D.; Shen, Z.; Huang, Y.; Sun, J.; Cao, J.; Zhou, J.; Liu, H.; Xu, H.; Zheng, C.; et al. Indoor air pollution levels in decorated residences and public places over Xi’an, China. Aerosol. Air. Qual. Res. 2017, 17, 2197–2205. [Google Scholar] [CrossRef] [Green Version]
- Shepherd, S.; Woskie, S.R. Case study to identify barriers and incentives to implementing an engineering control for concrete grinding dust. J. Constr. Eng. Manag. 2010, 136, 1238–1248. [Google Scholar] [CrossRef]
- Feng, Y.; Zhao, D.; Wu, P.; Xia, B. Risk compensation in construction workers’ activities. In Proceedings of the 38th Australasian Universities Building Education Association Conference (AUBEA), Auckland, New Zealand, 20–22 November 2013; pp. 1–10. [Google Scholar]
- Goto, K.; Abe, K. Gait characteristics in women’s safety shoes. Appl. Ergon. 2017, 65, 163–167. [Google Scholar] [CrossRef]
- Suo, Q.; Zhang, D. Investigation and identification of factors affecting migrating peasant workers’ usage of safety footwear in the Chinese construction industry. Int. J. Occup. Saf. Ergon. 2017, 23, 424–430. [Google Scholar] [CrossRef]
- Kohlman-Rabbani, E.R.; Shapira, A.; Martins, A.R.B.; Barkokébas, B., Jr. Characterization and evaluation of dust on building construction sites in brazil. Open Occup. Health Saf. J. 2014, 5, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Yi, W.; Chan, A. Health profile of construction workers in Hong Kong. Int. J. Environ. Res. Public Health 2016, 13, 1232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brahmachary, T.K.; Ahmed, S.; Mia, M.S. Health, safety and quality management practices in construction sector: A case study. J. Syst. Manag. Sci. 2018, 8, 47–64. [Google Scholar]
- Kim, J.; Philips, P. Health insurance and worker retention in the construction industry. J. Labor Res. 2010, 31, 20–38. [Google Scholar] [CrossRef]
- Adsul, B.B.; Laad, P.S.; Howal, P.V.; Chaturvedi, R.M. Health problems among migrant construction workers: A unique public-private partnership project. Indian J. Occup. Environ. Med. 2011, 15, 29–32. [Google Scholar]
- Baki, B.; Çakar, K. Determining the ERP package-selecting criteria: The case of Turkish manufacturing companies. Bus. Process Manag. J. 2005, 11, 75–86. [Google Scholar] [CrossRef]
- Sajady, H.; Dastgir, M.; Nejad, H.H. Evaluation of the effectiveness of accounting information systems. Int. J. Inf. Sci. Manag. 2012, 6, 49–59. [Google Scholar]
- Pallant, J. SPSS Survival Manual: A Step by Step Guide to Data Analysis Using SPSS for Windows; Open University Press: London, UK, 2001. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Publications: New York, NY, USA, 2017. [Google Scholar]
- Baron, R.M.; Kenny, D.A. The moderator–mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. J. Personal. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef]
- Kenny, D.A.; Kashy, D.A.; Bolger, N. Data analysis in social psychology. Handb. Soc. Psychol. 1998, 1, 233–265. [Google Scholar]
- MacKinnon, D.P.; Lockwood, C.M.; Hoffman, J.M.; West, S.G.; Sheets, V. A compari- son of methods to test mediation and other intervening variable effects. Psychol. Methods 2002, 7, 83–104. [Google Scholar] [CrossRef]
- Preacher, K.; Hayes, A. SPSS and SAS procedures for estimating indirect effects in simple mediation models. Behav. Res. Methods Instrum. Comput. 2004, 36, 717–731. [Google Scholar] [CrossRef] [Green Version]
- Chan, A.P.; Javed, A.A.; Lyu, S.; Hon, C.K.; Wong, F.K. Strategies for improving safety and health of ethnic minority construction workers. J. Constr. Eng. Manag. 2016, 142, 05016007. [Google Scholar] [CrossRef] [Green Version]
- Yuan, J.; Yi, W.; Miao, M.; Zhang, L. Evaluating the impacts of health, social network and capital on craft efficiency and productivity: A case study of construction workers in China. Int. J. Environ. Res. Public Health 2018, 15, 345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, B.; Chen, Y.; Wei, N. Engineering biocatalytic and biosorptive materials for environmental applications. Trends Biotechnol. 2019, 37, 661–676. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.; Chen, J. Evolutionary game analysis and countermeasure study of construction enterprises safety supervision in China. In Proceedings of the 19th International Symposium on Advancement of Construction Management and Real Estate, Chongqing, China, 7–9 November 2014; Springer: Berlin/Heidelberg, Germany, 2015; pp. 771–786. [Google Scholar]
- Wong, T.K.M.; Man, S.S.; Chan, A.H.S. Critical factors for the use or non-use of personal protective equipment amongst construction workers. Saf. Sci. 2020, 126, 104663. [Google Scholar] [CrossRef]
- Wilkins, J.R. Construction workers’ perceptions of health and safety training programmes. Construction Management and Economics. Constr. Manag. Econ. 2011, 29, 1017–1026. [Google Scholar] [CrossRef]
- Liu, L.L. Chinese Construction Enterprises HSE Management. Adv. Mater. Res. 2013, 838–841, 237–240. [Google Scholar] [CrossRef]
- Top, Y.; Adanur, H.; Öz, M. Comparison of practices related to occupational health and safety in microscale wood-product enterprises. Saf. Sci. 2016, 82, 374–381. [Google Scholar] [CrossRef]
- Lunde, L.K.; Koch, M.; Veiersted, K.B.; Moen, G.H.; Waersted, M.; Knardahl, S. Heavy physical work: Cardiovascular load in male construction workers. Int. J. Environ. Res. Public Health 2016, 13, 356. [Google Scholar] [CrossRef] [Green Version]
- Gündüz, Ş.; Erbulut, C.; Öznacar, B.; Baştaş, M. Determination of consciousness and awareness of the public in Lefka about the Cyprus Mining Corporation (CMC). Eurasia J. Math. Sci. Technol. Educ. 2016, 12, 783–792. [Google Scholar]
- Lin, K.Y.; Lee, W.; Azari, R.; Migliaccio, G.C. Training of low-literacy and low-english-proficiency hispanic workers on construction fall fatality. J. Manag. Eng 2018, 34, 05017009. [Google Scholar] [CrossRef]
- Jiang, Z.; Fang, D.; Zhang, M. Understanding the causation of construction workers’ unsafe behaviors based on system dynamics modeling. J. Manag. Eng. 2015, 31, 04014099. [Google Scholar] [CrossRef] [Green Version]
- Diener, E.; Ng, W.; Harter, J.; Arora, R. Wealth and happiness across the world: Material prosperity predicts life evaluation, whereas psychosocial prosperity predicts positive feeling. J. Personal. Soc. Psychol. 2010, 99, 52–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gehner, J. Libraries, low-income people, and social exclusion. Public Libr. Q. 2010, 29, 39–47. [Google Scholar] [CrossRef]
- Xiang, J.; Bi, P.; Pisaniello, D.; Hansen, A. Health impacts of workplace heat exposure: An epidemiological review. Ind. Health 2014, 52, 91–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y. The Questions and Solution Policies of Employees in Welfare Management in New Normal. Modern Management Forum. Int. J. New Dev. Eng. Soc. 2019, 3, 60–69. [Google Scholar]
- Ramos, D.; Afonso, P.; Rodrigues, M.A. Integrated management systems as a key facilitator of occupational health and safety risk management: A case study in a medium sized waste management firm. J. Clean. Prod. 2020, 262, 121346. [Google Scholar] [CrossRef]
- Pęciłło, M. The resilience engineering concept in enterprises with and without occupational safety and health management systems. Saf. Sci. 2016, 82, 190–198. [Google Scholar] [CrossRef]
- Bedi, P.; Lakra, P.; Gupta, E. Workforce Diversity Management: Biggest Challenge or Opportunity For 21st Century Organizations. IOSR J. Bus. Manag. 2014, 16, 102–107. [Google Scholar] [CrossRef]
- Albert, A.; Pandit, B.; Patil, Y. Focus on the fatal-four: Implications for construction hazard recognition. Saf. Sci. 2020, 128, 104774. [Google Scholar] [CrossRef]
- Jarkas, A.M.; Bitar, C.G. Factors Affecting Construction Labor Productivity in Kuwait. J. Constr. Eng. Manag. 2012, 138, 811–820. [Google Scholar] [CrossRef]
- Winge, S.; Albrechtsen, E.; Mostue, B.A. Causal factors and connections in construction accidents. Saf. Sci. 2019, 112, 130–141. [Google Scholar] [CrossRef]
- Williams, Q.; Ochsner, M.; Marshall, E.; Kimmel, L.; Martino, C. The impact of a peer-led participatory health and safety training program for Latino day laborers in construction. J. Saf. Res. 2010, 41, 253–261. [Google Scholar] [CrossRef]
- Forst, L.; Ahonen, E.; Zanoni, J.; Holloway-Beth, A.; Oschner, M.; Kimmel, L.; Sokas, R. More than training: Community-based participatory research to reduce injuries among hispanic construction workers. Am. J. Ind. Med. 2013, 56, 827–837. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.; Kim, T.; Park, Y.; Kim, J. Improving Effectiveness of Safety Training at Construction Worksite Using 3D BIM Simulation. Adv. Civ. Eng. 2020, 2020, 2473138. [Google Scholar] [CrossRef]
- Harth, N.S.; Leach, C.W.; Kessler, T. Guilt, anger, and pride about in-group environmental behaviour: Different emotions predict distinct intentions. J. Environ. Psychol. 2013, 34, 18–26. [Google Scholar] [CrossRef]
- Sargeant, M.; Tucker, E. Layers of vulnerability in occupational safety and health for migrant workers: Case studies from Canada and the UK. Policy Pract. Health Saf. 2009, 7, 51–73. [Google Scholar] [CrossRef]
- Shamsuddin, K.A.; Ani, M.N.C.; Ismail, A.K.; Ibrahim, M.R. Investigation the Safety, Health and Environment (SHE) protection in construction area. Int. Res. J. Eng. Technol. 2015, 2, 624–636. [Google Scholar]
- Vigoroso, L.; Caffaro, F.; Cavallo, E. Occupational safety and visual communication: User-centred design of safety training material for migrant farmworkers in Italy. Saf. Sci. 2020, 121, 562–572. [Google Scholar] [CrossRef]
- Burke, M.J.; Sarpy, S.A.; Smith-Crowe, K.; Chan-Serafin, S.; Salvador, R.O.; Islam, G. Relative effectiveness of worker safety and health training methods. Am. J. Public Health 2006, 96, 315–324. [Google Scholar] [CrossRef]
- Menger, L.M.; Rosecrance, J.; Stallones, L.; Roman-Muniz, I.N. A guide to the design of occupational safety and health training for immigrantLatino/a dairy workers. Front. Public Health 2016, 4, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Categories | Indicator | Literature Sources |
|---|---|---|
| Risk Perception | Hazardous substances are generated | Li et al. (2019) [99]; Shim et al. (2017) [100] |
| Dust exposure leads to pneumoconiosis | Chen et al. (2019) [33]; Wu et al. (2016) [101] | |
| Formaldehyde causes chronic respiratory diseases | Zhuo (2018) [102]; Xia et al. (2012) [103] | |
| Inhalation of irritant gas causes headache | Chong et al. (2018) [104]; Cui et al. (2020) [105] | |
| Materials with less pollution reduce the probability of illness | Cincinelli et al. (2017) [106]; Yan et al. (2017) [107] | |
| Protective equipment (dust masks, gas masks, etc.) reduces harm caused by pollution | Li et al. (2017) [108]; Lette et al. (2018) [109]; Tadesse et al. (2016) [110] | |
| Ventilation reduces harm of formaldehyde, benzene, and dust to the body | Weidman et al. (2016) [111]; Chen et al. (2020) [112] | |
| Decoration pollution can be prevented | Li et al. (2016) [113]; Liqun et al. (2011) [114] | |
| More exercise and less smoking can reduce the probability of illness | Tadesse et al. (2016) [110]; Sawicki et al. (2020) [115]; Vitharana et al. (2019) [116] | |
| Coping Behavior | Maintain ventilation | Yan (2017) [107]; Chang et al. (2017) [117] |
| Wear dust mask | Shepherd et al. (2010) [118]; Feng et al. (2013) [119] | |
| Wear labor protection shoes | Goto et al. (2017) [120]; Suo et al. (2017) [121] | |
| Use other personal protective equipment | Kohlman et al. (2014) [122]; Li et al. (2019) [99] | |
| Avoid eating and resting on site | Yi et al. (2016) [123]; Brahmachary et al. (2018) [124] | |
| Pay insurance and carry out physical examination | Kim et al. (2010) [125]; Adsul et al. (2011) [126] |
| Variable | Classification | NO. | Proportion | Variable | Classification | NO. | Proportion |
|---|---|---|---|---|---|---|---|
| Gender | Male | 321 | 94.10% | Education level | Junior middle school or below | 188 | 55.10% |
| Female | 20 | 5.90% | Technical secondary school or high school | 111 | 32.60% | ||
| Marital status | Married | 307 | 90.00% | Junior college or above | 42 | 12.30% | |
| Single | 34 | 10.00% | Monthly income (RMB) | ≤5000 | 47 | 13.80% | |
| Trades | Carpenters | 76 | 22.30% | 5000–7000 | 164 | 48.10% | |
| Bricklayers | 70 | 20.50% | 7000–9000 | 109 | 32.00% | ||
| Electricians | 70 | 20.50% | ≥9000 | 21 | 6.20% | ||
| Plumbers | 45 | 13.20% | Unit qualification | Level A | 79 | 23.20% | |
| Painters | 66 | 19.40% | Level B | 40 | 11.70% | ||
| Other | 14 | 4.10% | Level C | 23 | 6.70% | ||
| Age | ≤30 | 35 | 10.30% | No qualification | 78 | 22.90% | |
| 30~50 | 243 | 71.30% | Unclear | 121 | 35.50% | ||
| ≥50 | 63 | 18.50% |
| Variable | Item | Factors | Cronbach’s α a | |||
|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |||
| Occupational health risk perception | B1 | 0.682 | 0.872 | |||
| B2 | 0.767 | |||||
| B3 | 0.754 | |||||
| B4 | 0.707 | |||||
| B5 | 0.467 | |||||
| B6 | 0.628 | |||||
| B7 | 0.602 | |||||
| B8 | 0.523 | |||||
| B9 | 0.561 | |||||
| Coping behaviors | C1 | 0.277 | 0.668 | |||
| C2 | 0.531 | |||||
| C3 | 0.531 | |||||
| C4 | 0.699 | |||||
| C5 | 0.347 | |||||
| C6 | 0.669 | |||||
| Personal knowledge | D1 | 0.699 | 0.834 | |||
| D2 | 0.854 | |||||
| D3 | 0.854 | |||||
| D4 | 0.744 | |||||
| D5 | 0.294 | |||||
| D6 | 0.688 | |||||
| D7 | 0.675 | |||||
| Social influence factors | E1 | 0.877 | 0.936 | |||
| E2 | 0.882 | |||||
| E3 | 0.721 | |||||
| E4 | 0.884 | |||||
| E5 | 0.712 | |||||
| E6 | 0.737 | |||||
| E7 | 0.791 | |||||
| E8 | 0.795 | |||||
| E9 | 0.851 | |||||
| E10 | 0.493 | |||||
| E11 | 0.688 | |||||
| KMO = 0.889, Bartlett Χ2(df) = 6298.903(528) *** | ||||||
| Variable | Mean ± SD |
|---|---|
| Hazardous substances are generated | 4.28 ± 0.88 |
| Dust exposure leads to pneumoconiosis | 4.29 ± 0.86 |
| Formaldehyde causes chronic respiratory diseases | 4.19 ± 0.93 |
| Inhalation of irritant gas causes headache | 3.92 ± 1.00 |
| Materials with less pollution reduce the probability of illness | 3.93 ± 1.14 |
| Protective equipment (dust masks, gas masks, etc.) reduces harm caused by pollution | 3.86 ± 1.00 |
| Ventilation reduces harm of formaldehyde, benzene, and dust to the body | 4.10 ± 0.92 |
| construction pollution can be prevented | 4.05 ± 0.97 |
| More exercise and less smoking can reduce the probability of illness | 3.77 ± 1.24 |
| Risk perception | 4.03 ± 0.70 |
| Variable | Mean ± SD |
|---|---|
| Maintain ventilation | 3.97 ± 0.93 |
| Wear dust mask | 3.33 ± 1.19 |
| Wear labor protection shoes | 3.53 ± 1.13 |
| Use other personal protective equipment | 2.40 ± 1.23 |
| Avoid eating and resting on site | 3.36 ± 1.16 |
| Pay insurance and carry out physical examination | 2.25 ± 1.24 |
| Coping behavior | 3.15 ± 0.70 |
| Variable | Classification | Mean ± SD | Levene’s Test (Sig) | p-Value | F-Value | T-Value |
|---|---|---|---|---|---|---|
| Gender | Male | 4.02 ± 0.71 | 0.051 | 0.035 | / | −2.116 |
| Female | 4.36 ± 0.54 | |||||
| Age | ≤30 | 4.32 ± 0.72 | 0.274 | 0.007 | 5.083 | / |
| 30–50 | 3.97 ± 0.69 | |||||
| ≥50 | 4.17 ± 0.71 | |||||
| Marital status | Married | 4.05 ± 0.72 | 0.044 | 0.194 | 1.319 | |
| Single | 3.91 ± 0.55 | |||||
| Education level | Junior middle school or below | 3.87 ± 0.76 | 0.000 | 0.000 | 15.109 | / |
| Technical secondary school or high school | 4.21 ± 0.60 | |||||
| Junior college or above | 4.32 ± 0.48 | |||||
| Monthly income (RMB) | <5000 | 3.63 ± 0.95 | 0.000 | 0.033 | 3.055 | / |
| 5000–7000 | 4.04 ± 0.69 | |||||
| 7000–9000 | 4.10 ± 0.62 | |||||
| >9000 | 4.23 ± 0.67 | |||||
| Unit qualification | Level A | 4.20 ± 0.64 | 0.000 | 0.002 | 4.636 | / |
| Level B | 4.03 ± 0.61 | |||||
| Level C | 3.86 ± 0.52 | |||||
| No qualification | 3.76 ± 0.85 | |||||
| Unclear | 4.15 ± 0.64 |
| Model | Non-Standardized Coefficient | Standardized Coefficient | t-Value | p | |
|---|---|---|---|---|---|
| B | SE | β | |||
| Constant | 2.858 | 0.111 | 25.849 | 0.000 | |
| personal knowledge | 2.069 | 0.185 | 0.519 | 11.182 | 0.000 |
| Model | Standardized Coefficient | t-Value | p |
|---|---|---|---|
| Constant | 30.985 | 0.000 | |
| Unit training | −0.090 | −0.944 | 0.346 |
| Related rules and regulations | −0.093 | −0.823 | 0.411 |
| Manager’s attitude | −0.161 | −1.784 | 0.075 |
| Group effect | 0.268 | 3.201 | 0.002 a |
| Family environment | 0.034 | 0.466 | 0.642 |
| Model | Non-Standardized Coefficient | Standardized Coefficient | t-Value | p | |
|---|---|---|---|---|---|
| B | SE | β | |||
| Constant | 1.822 | 0.212 | 8.578 | 0.000 | |
| Risk perception | 0.325 | 0.052 | 0.323 | 6.278 | 0.000 |
| Independent Variable (Xi1) | Model 1 (Y: Coping Behavior) | Model 2 (Y: Risk Perception) | Model 3 (Y: Coping Behavior) | Boot95%CI | |||||
|---|---|---|---|---|---|---|---|---|---|
| Xi1 | Xi1 | Xi1 | Xi2 = Risk Perception | ||||||
| β | t | β | t | β | t | β | t | ||
| Gender | 0.35 | 1.5070.133 | |||||||
| Age | −0.07 | −1.2330.222 | |||||||
| Marital status | 0.24 | 1.3350.183 | |||||||
| Education level | 0.22 | 4.188 *** | 0.25 | 4.69 *** | 0.15 | 2.883 ** | 0.29 | 5.437 *** | (0.036, 0.098) |
| Monthly income | 0.18 | 3.283 ** | 0.18 | 3.287 ** | 0.12 | 2.364 * | 0.30 | 5.806 *** | (0.016, 0.081) |
| Unit qualification | −0.25 | −4.757 *** | −0.05 | −0.9740.331 | −0.23 | −4.679 *** | 0.31 | 6.212 *** | (−0.021, 0.010) |
| Personal knowledge | 0.26 | 4.86 *** | 0.52 | 11.18 *** | 0.12 | 2.01 * | 0.26 | 4.35 *** | (0.315, 0.789) |
| Unit training | 0.33 | 6.472 *** | 0.07 | −1.3530.177 | 0.36 | 7.468 *** | 0.35 | 7.295 *** | (−0.034, 0.005) |
| Related rules and regulations | 0.39 | 7.903 *** | −0.09 | −1.5920.112 | 0.43 | 9.207 *** | 0.36 | 7.778 *** | (−0.044, 0.003) |
| Manager’s attitude | 0.34 | 6.651 *** | −0.11 | −1.9470.052 | 0.38 | 7.952 *** | 0.36 | 7.628 *** | (−0.044, 0.001) |
| Group effect | 0.38 | 7.542 *** | 0.06 | 1.1300.260 | 0.36 | 7.561 *** | 0.30 | 6.302 *** | (−0.009, 0.037) |
| Family environment | 0.35 | 6.866 *** | 0.01 | 0.1680.867 | 0.35 | 7.232 *** | 0.32 | 6.670 ** | (−0.018, 0.022) |
| Hypothesized Paths | Effect Type | Effect Value | BootSE | Boot95%CI | Percentage |
|---|---|---|---|---|---|
| Education level→risk perception→coping behavior | Total effect | 0.202 | 0.058 | (0.122, 0.352) | |
| Direct effect | 0.138 | 0.056 | (0.031, 0.250) | 68.32% | |
| Indirect effect | 0.064 | 0.016 | (0.036, 0.098) | 31.68% | |
| Monthly income→risk perception→coping behavior | Total effect | 0.158 | 0.052 | (0.053, 0.259) | |
| Direct effect | 0.110 | 0.049 | (0.015, 0.205) | 69.62% | |
| Indirect effect | 0.048 | 0.017 | (0.016, 0.081) | 30.38% | |
| Personal knowledge→risk perception→coping behavior | Total effect | 1.025 | 0.192 | (0.654, 1.406) | |
| Direct effect | 0.482 | 0.225 | (0.050, 0.929) | 47.02% | |
| Indirect effect | 0.543 | 0.122 | (0.315, 0.789) | 52.98% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, H.; Li, J.; Li, H.; Li, H.; Mao, P.; Yuan, J. Risk Perception and Coping Behavior of Construction Workers on Occupational Health Risks—A Case Study of Nanjing, China. Int. J. Environ. Res. Public Health 2021, 18, 7040. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137040
Liu H, Li J, Li H, Li H, Mao P, Yuan J. Risk Perception and Coping Behavior of Construction Workers on Occupational Health Risks—A Case Study of Nanjing, China. International Journal of Environmental Research and Public Health. 2021; 18(13):7040. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137040
Chicago/Turabian StyleLiu, Hui, Jie Li, Hongyang Li, He Li, Peng Mao, and Jingfeng Yuan. 2021. "Risk Perception and Coping Behavior of Construction Workers on Occupational Health Risks—A Case Study of Nanjing, China" International Journal of Environmental Research and Public Health 18, no. 13: 7040. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137040