
Hospital Admissions Due to Ischemic Heart Diseases and Prescriptions of Cardiovascular Diseases Medications in England and Wales in the Past Two Decades


 , , , ,
, , , ,  , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Study Sources and the Population
2.2. Statistical Analysis
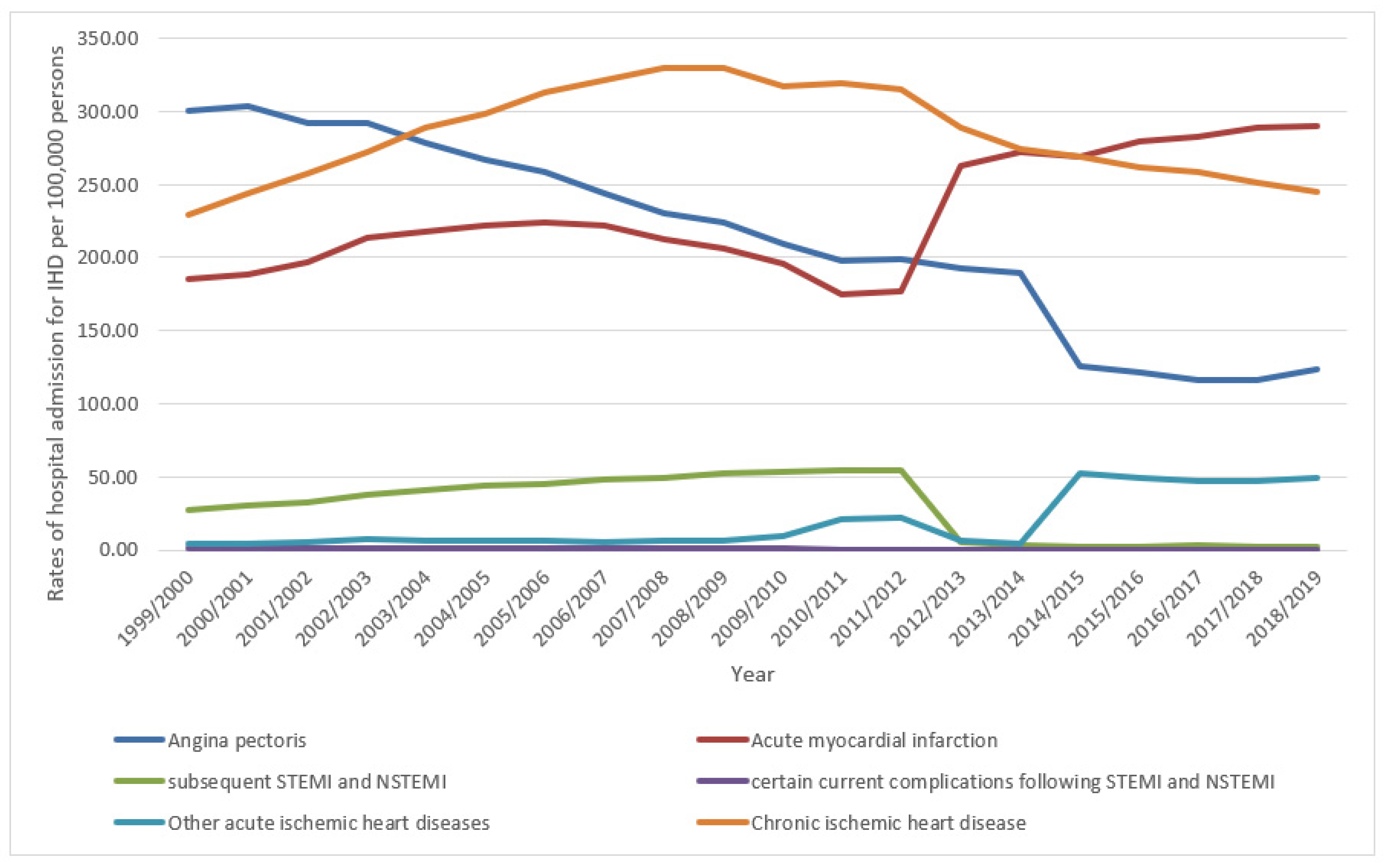
3. Results
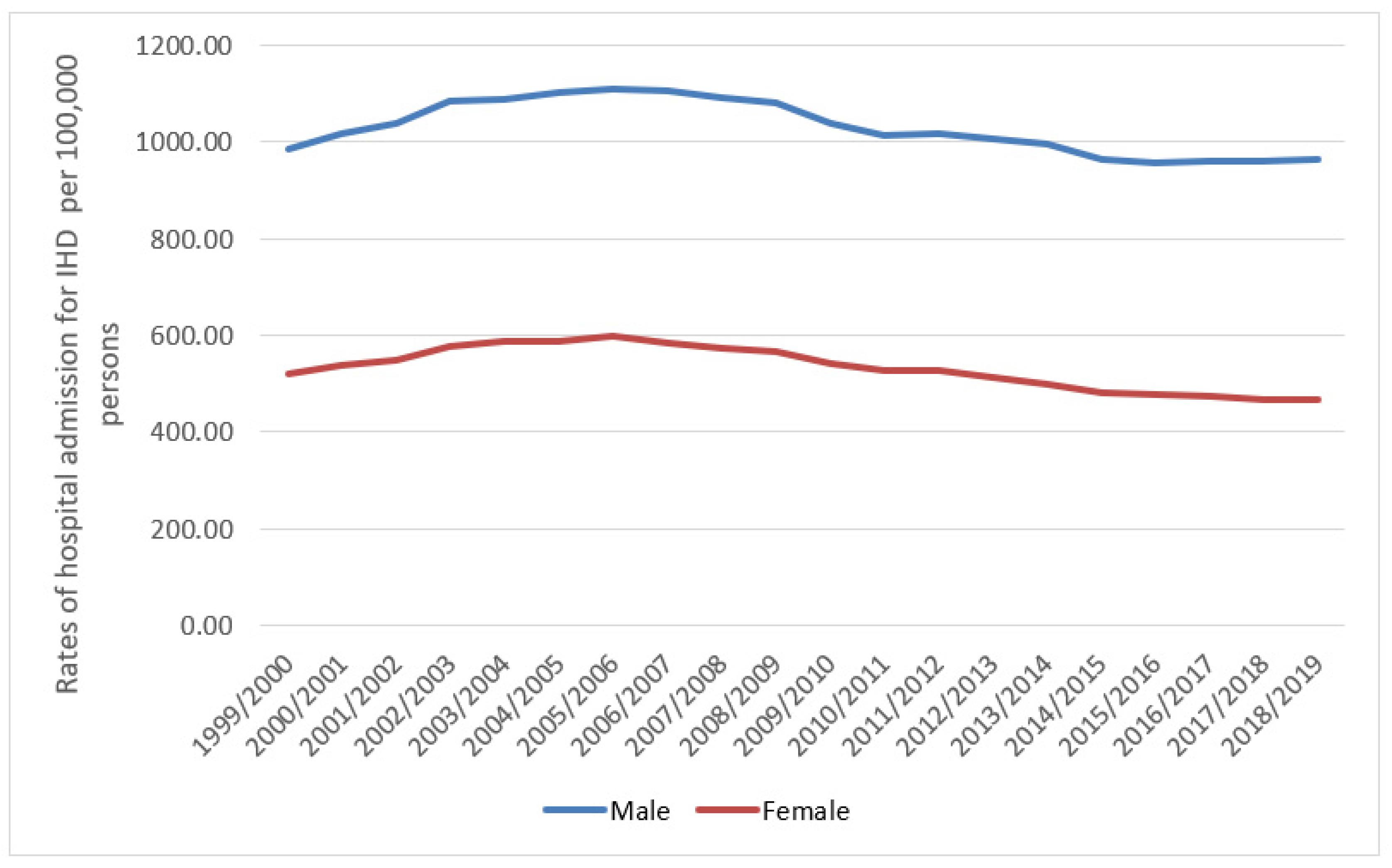
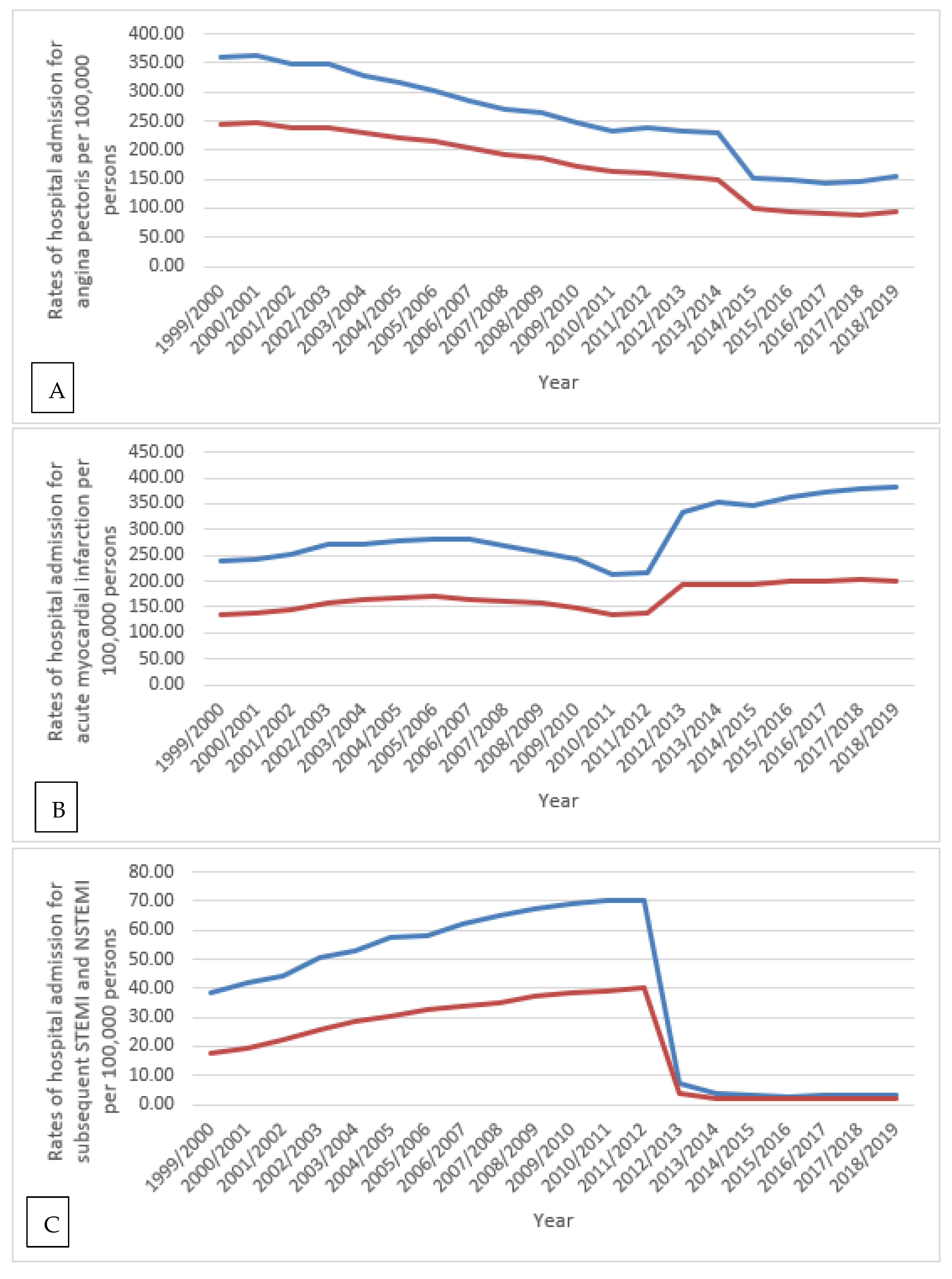
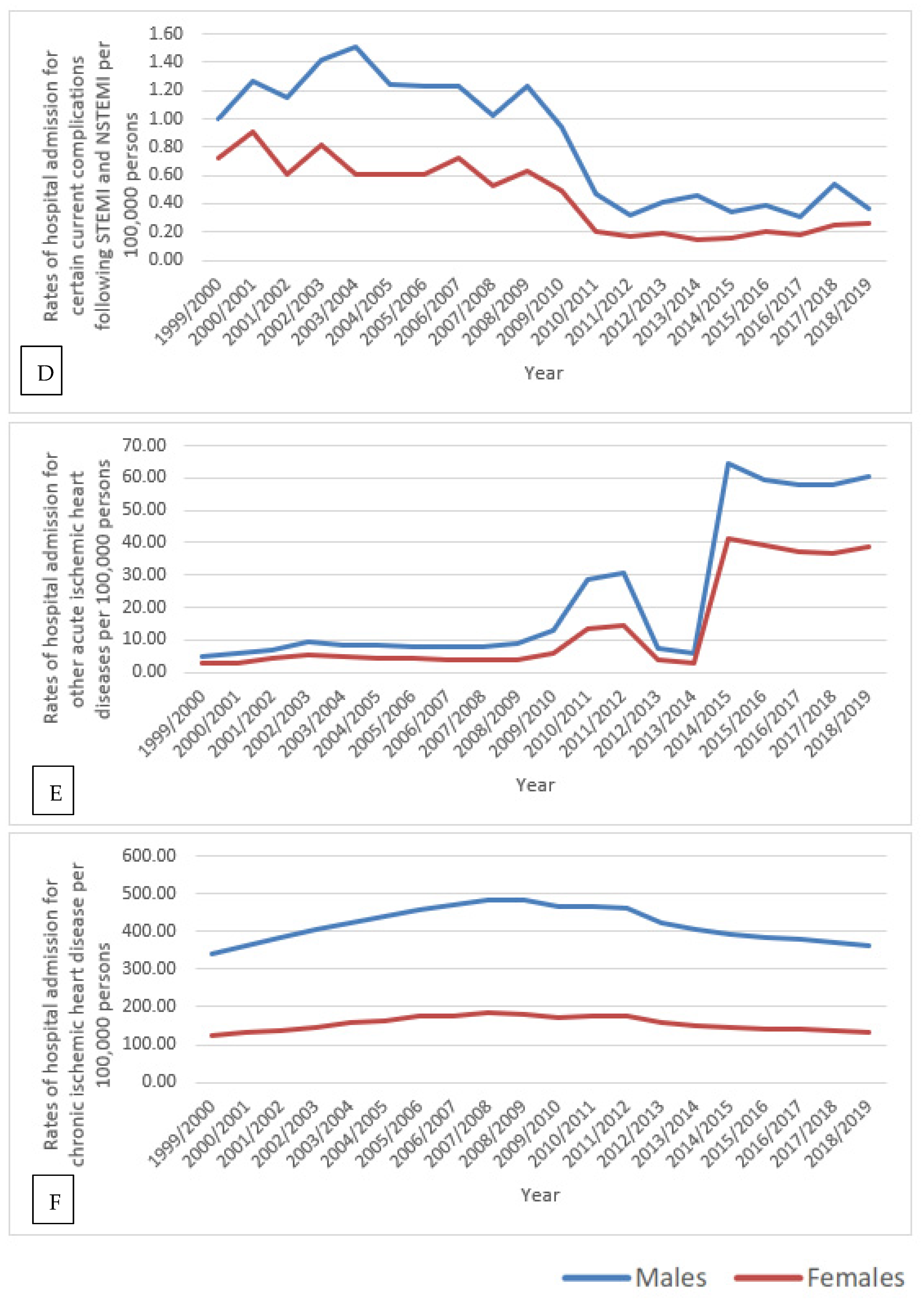
3.1. IHD Hospital Admission Rate by Gender
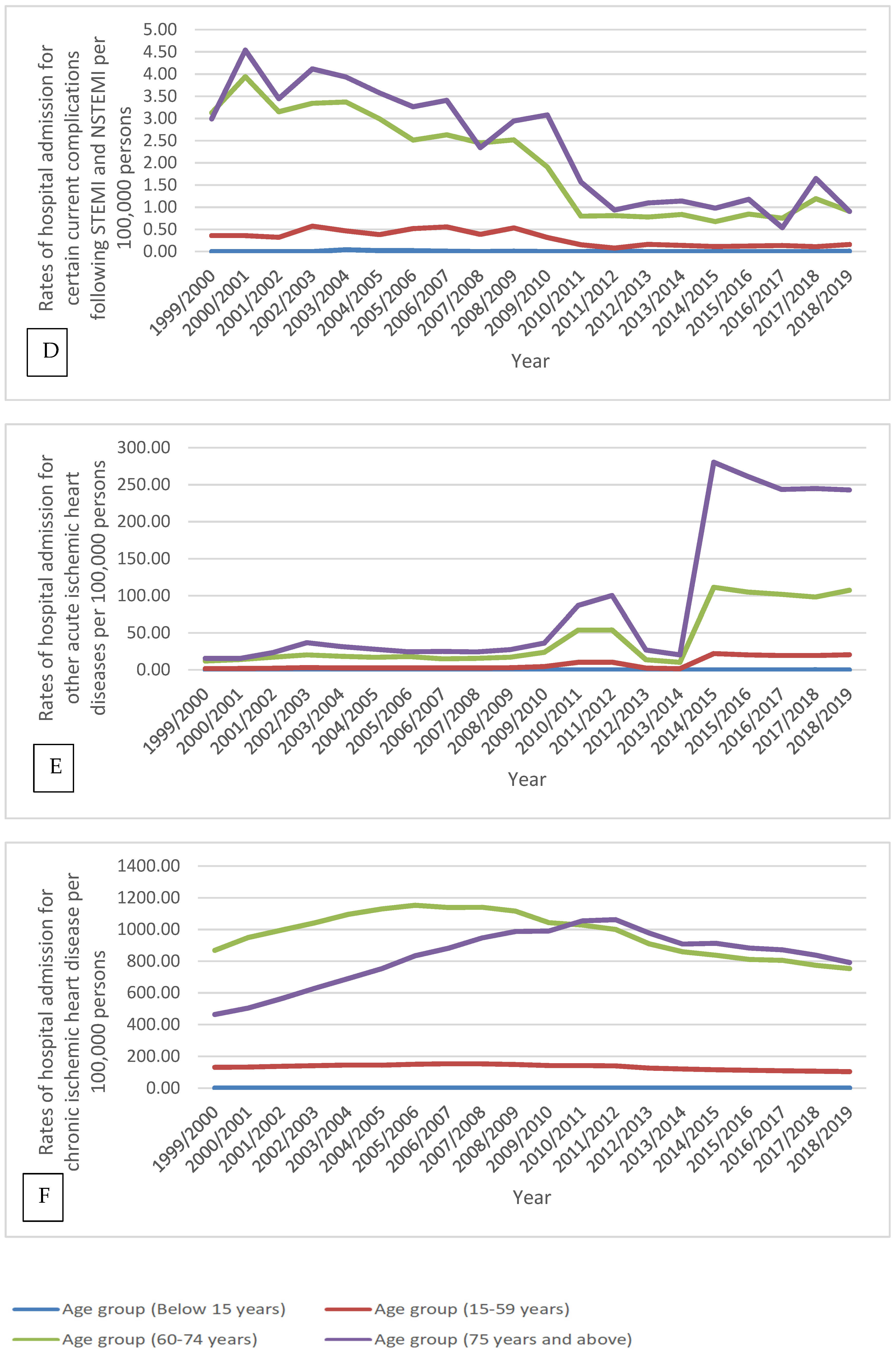
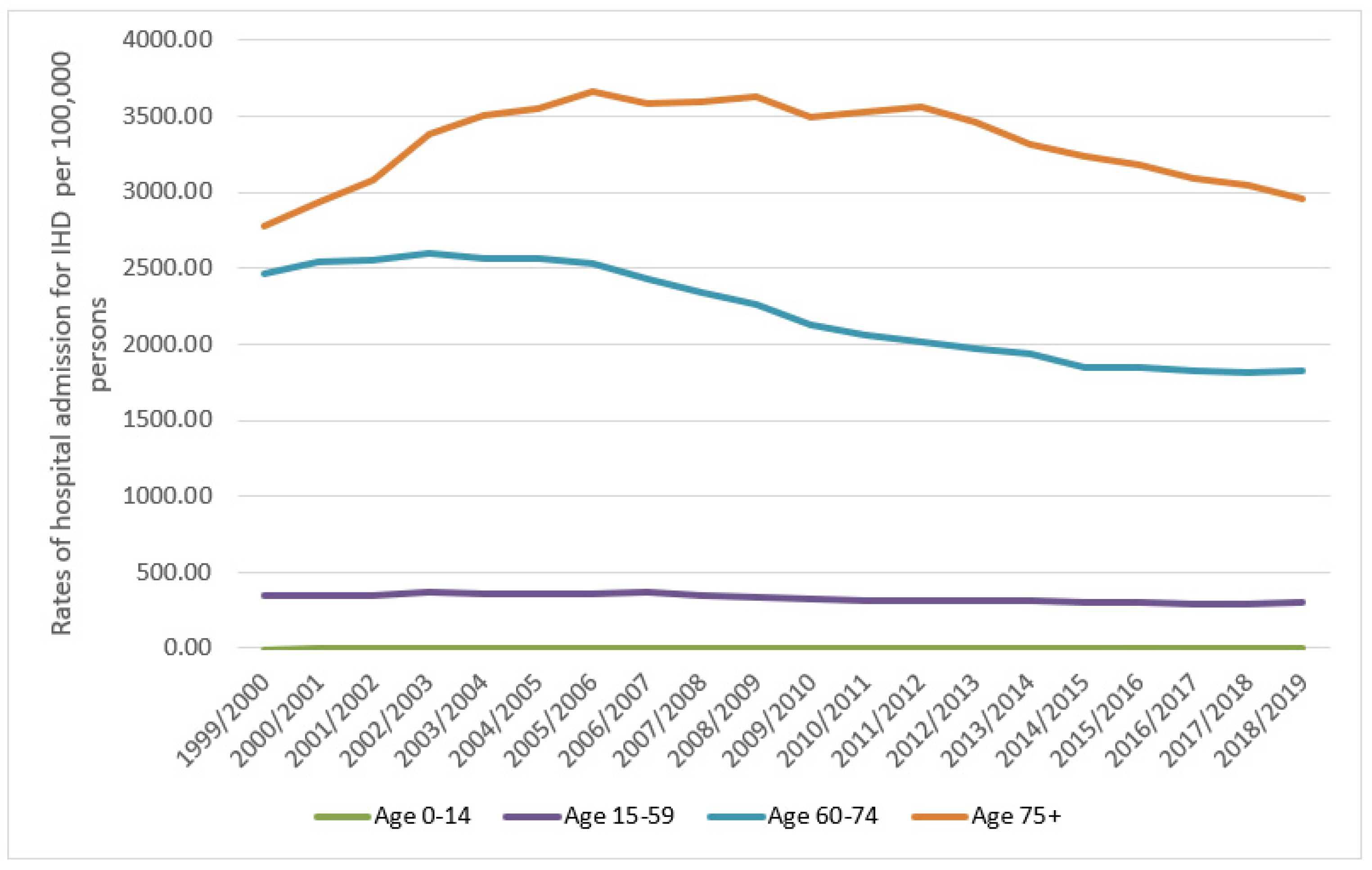
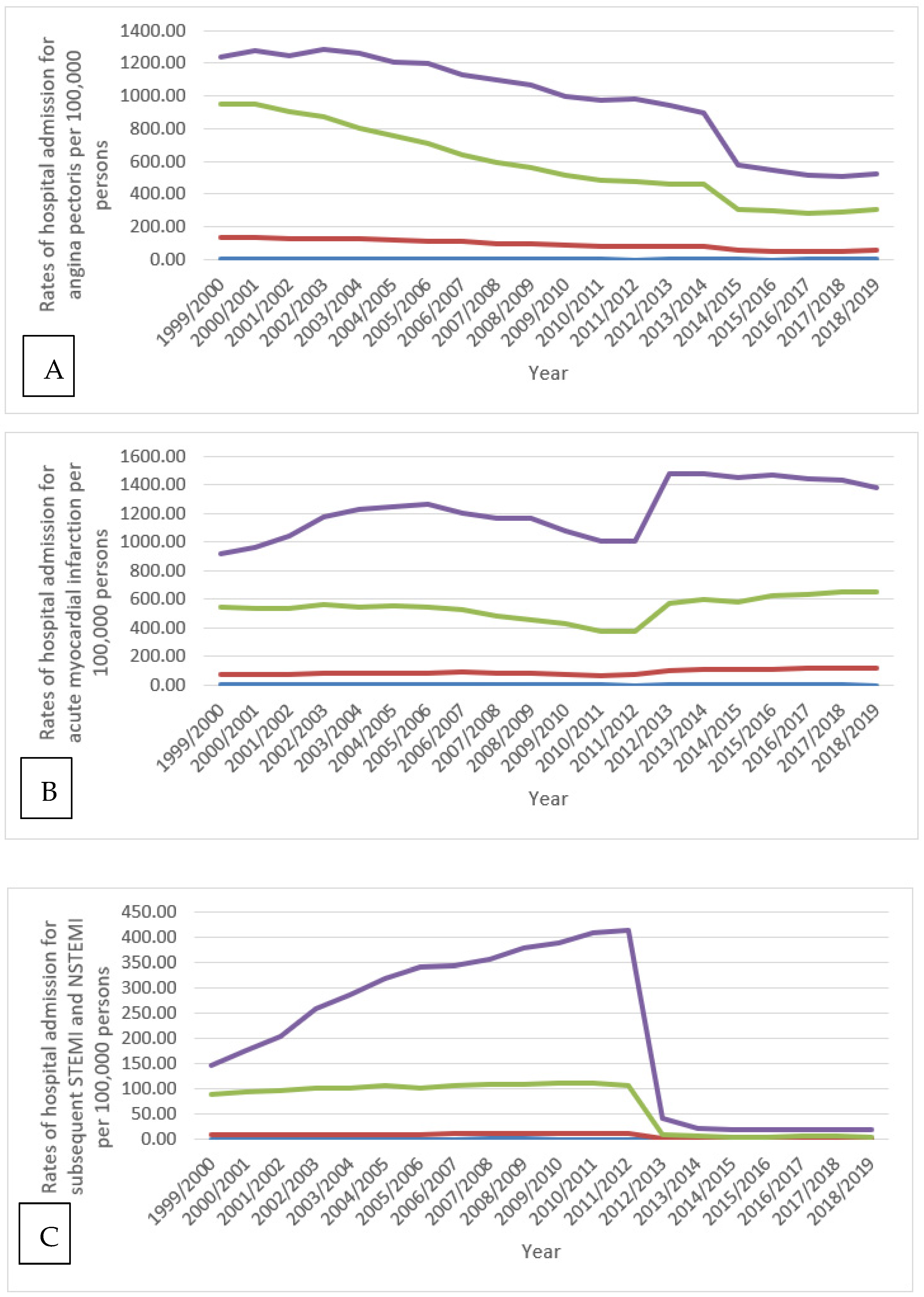
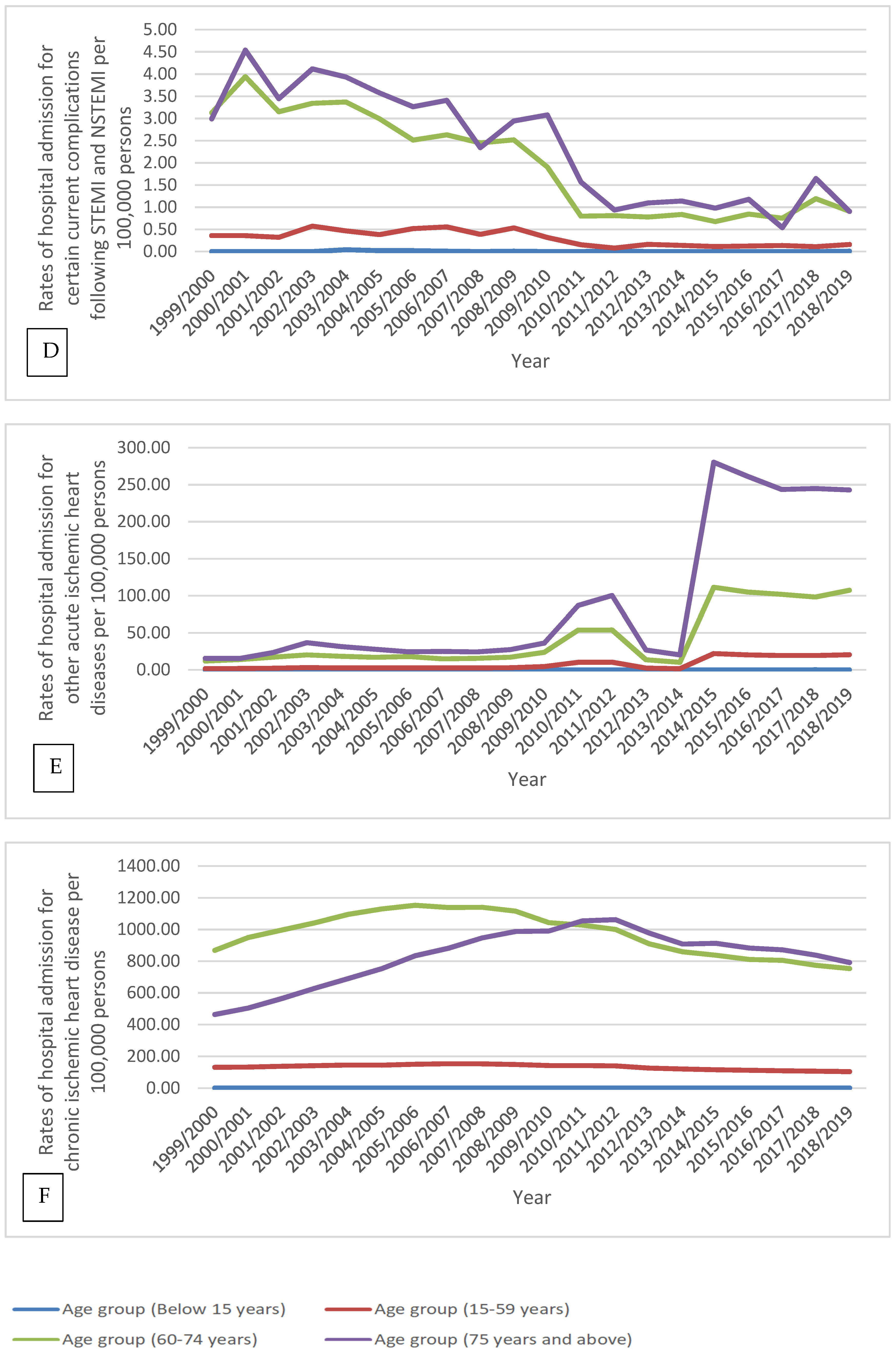
3.2. IHD Hospital Admission Rate by Age Group
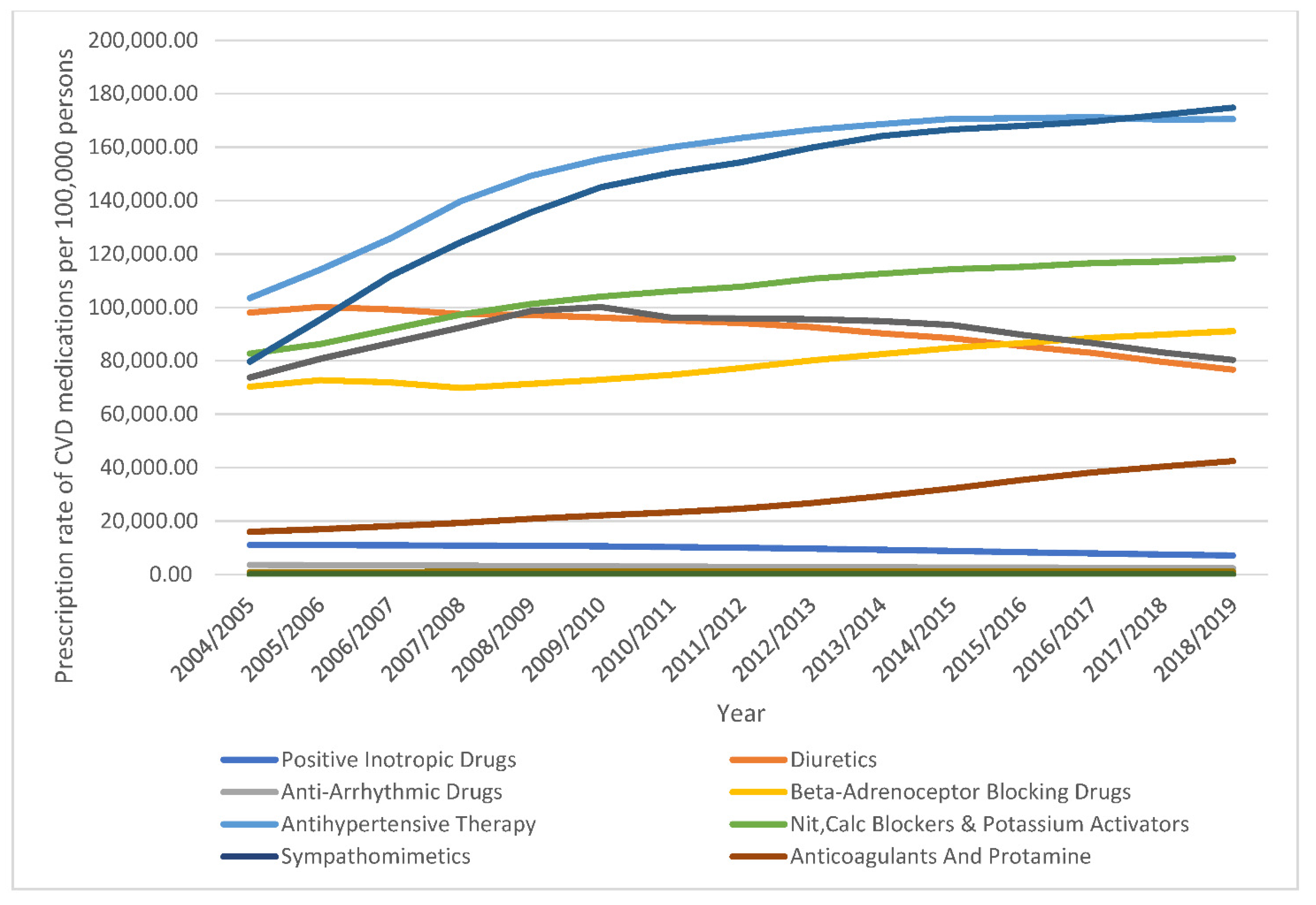
3.3. Cardiovascular Disease-Related Medication Prescriptions.
3.4. Correlation between IHD Hospitalisation and the Prescription of CVD Medications
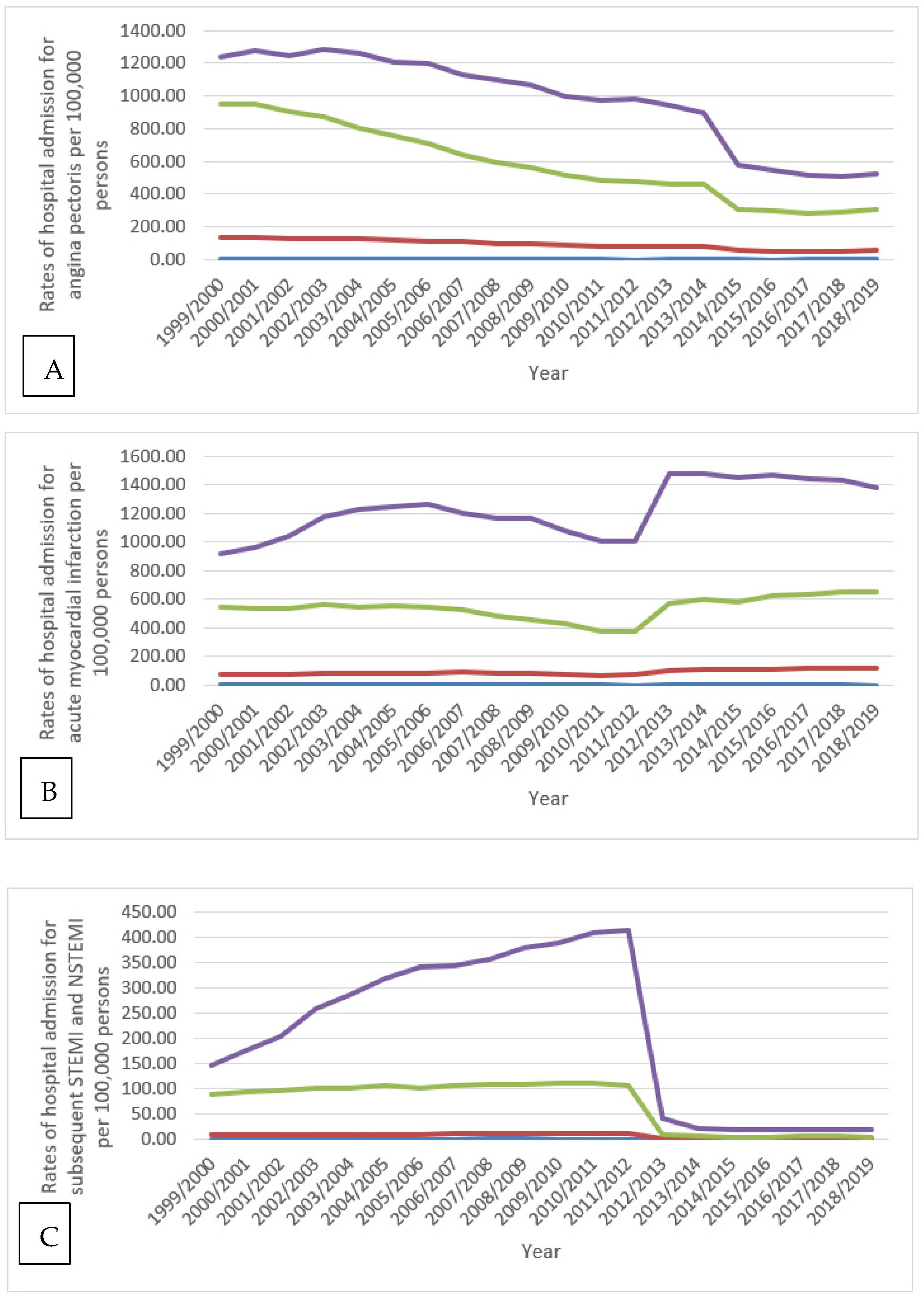
3.4.1. Angina Pectoris
3.4.2. Acute Myocardial Infarction
3.4.3. Subsequent ST Elevation (STEMI) and Non-ST Elevation (NSTEMI) Myocardial Infarction
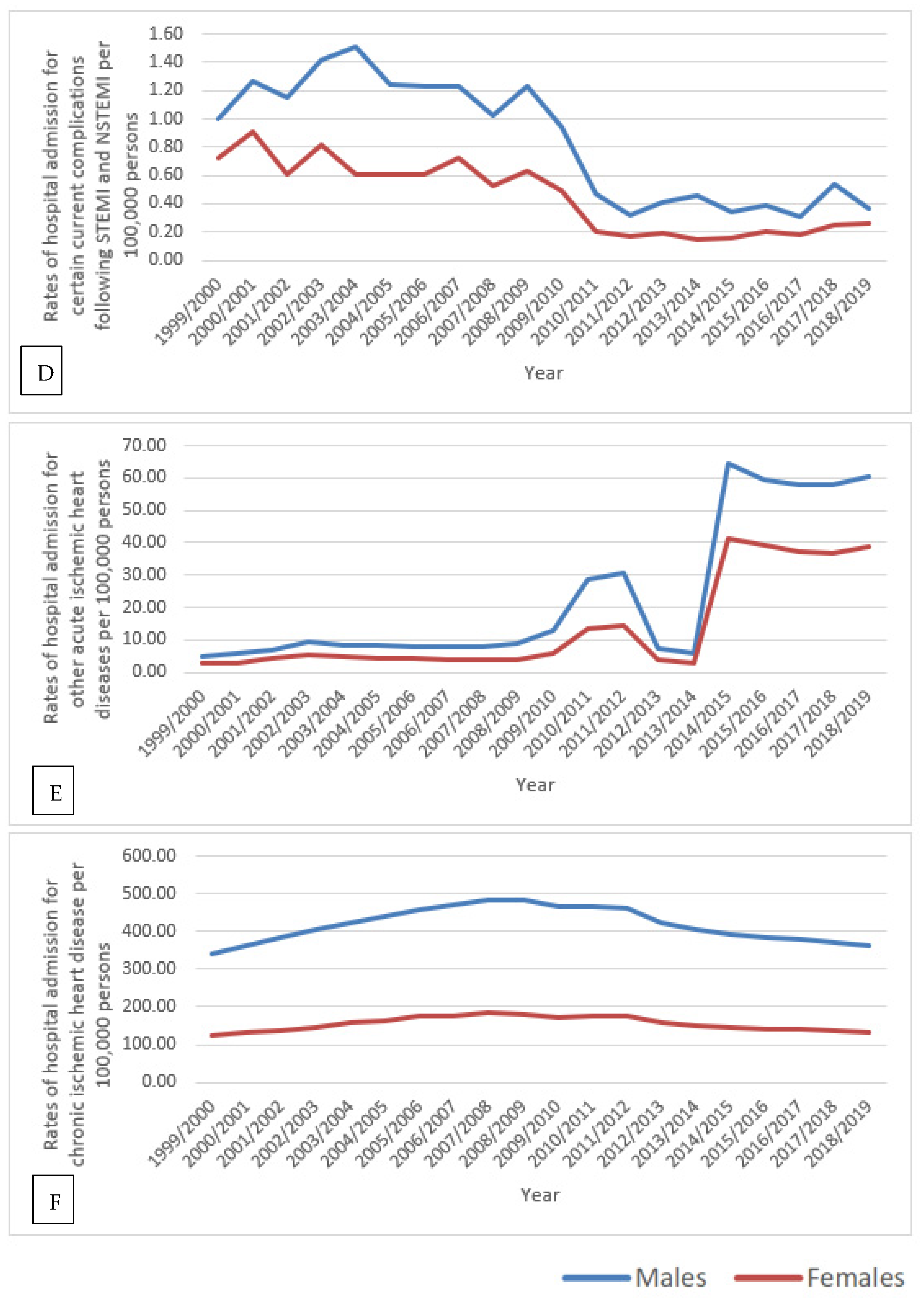
3.4.4. Certain Current Complications Following ST Elevation (STEMI) and Non-ST Elevation (NSTEMI) Myocardial Infarction (Within the 28-Day Period)
3.4.5. Chronic Ischemic Heart Disease
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Cardiovascular Diseases (CVDs). 2017. Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 27 March 2021).
- Nowbar, A.N.; Gitto, M.; Howard, J.P.; Francis, D.P.; Al-Lamee, R. Mortality from Ischemic Heart Disease. Circ. Cardiovasc. Qual. Outcomes 2019, 12, e005375. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.; Hashim, M.J.; Mustafa, H.; Baniyas, M.Y.; Al Suwaidi, S.K.B.M.; AlKatheeri, R.; Alblooshi, F.M.K.; Almatrooshi, M.E.A.H.; Alzaabi, M.E.H.; Al Darmaki, R.S.; et al. Global Epidemiology of Ischemic Heart Disease: Results from the Global Burden of Disease Study. Cureus 2020, 12, e9349. [Google Scholar] [CrossRef] [PubMed]
- Bhatnagar, P.; Townsend, N.; Wilkins, E.; Wickramasinghe, K.; Rayner, M. Cardiovascular Disease Statistics; British Heart Foundation: London, UK, 2015; pp. 1–75. [Google Scholar]
- Office for National Statistics (ONS). Leading Causes of Death, UK: 2001 to 2018. 2020. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/causesofdeath/articles/leadingcausesofdeathuk/2001to2018 (accessed on 29 May 2021).
- Di Giosia, P.; Passacquale, G.; Petrarca, M.; Giorgini, P.; Marra, A.M.; Ferro, A. Gender differences in cardiovascular prophylaxis: Focus on antiplatelet treatment. Pharmacol. Res. 2017, 119, 36–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maas, A.H.; Appelman, Y.E. Gender differences in coronary heart disease. Neth. Heart J. 2010, 18, 598–602. [Google Scholar] [CrossRef] [PubMed]
- Capodanno, D.; Angiolillo, D. Impact of race and gender on antithrombotic therapy. Thromb. Haemost. 2010, 104, 471–484. [Google Scholar] [CrossRef]
- Chandra, N.; Ziegelstein, R.C.; Rogers, W.J.; Tiefenbrunn, A.J.; Gore, J.M.; French, W.J.; Rubison, M. Observations of the treatment of women in the United States with myocardial infarction: A report from the National Registry of Myocardial Infarction-I. Arch. Intern. Med. 1998, 158, 981–988. [Google Scholar] [CrossRef] [Green Version]
- Cross Government Obesity Unit. Healthy Weight, Healthy Lives: A Cross-Government Strategy for England; Department of Health and Department for Children, Schools and Families: London, UK, 2008.
- Moran, A.; Forouzanfar, M.H.; Roth, G.; Ezzati, M.; Mensah, G.; Flaxman, A.; Murray, C.J.; Naghavi, M. The global burden of ischemic heart disease in 1990 and 2010: The Global Burden of Disease 2010 study. Circulation 2014, 129, 1493–1501. [Google Scholar] [CrossRef]
- Health and Social Care Information Centre (HSCIC). Hospital Episode Statistics. 2021. Available online: http://http//content. digital.nhs.uk/hes (accessed on 1 March 2021).
- NHS Wales Informatics Service. Annual PEDW Data Tables. 2021. Available online: http://www.infoandstats.wales.nhs.uk/page.cfm?pid=41010&orgid=869 (accessed on 1 March 2021).
- ICD10Data.com. 2021 ICD-10-CM Codes. 2021. Available online: https://www.icd10data.com/ICD10CM/Codes (accessed on 1 March 2021).
- NHS Wales Informatics Service. Data Quality Status Report: Admitted Patient Care Data Set. 2021. Available online: http://www.infoandstats.wales.nhs.uk/documents/869/20191007-APC DQ Status Report 2018-19-v1.pdf (accessed on 1 March 2021).
- Office for National Statistics (ONS). Population Estimates. 2021. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates/datasets/populationestimatesforukenglandandwalesscotlandandnorthernireland (accessed on 1 March 2021).
- National Health Service. Prescription Cost Analysis. 2021. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/prescription-cost-analysis (accessed on 1 March 2021).
- OpenPrescribing. All BNF Sections. 2021. Available online: https://openprescribing.net/bnf/ (accessed on 1 March 2021).
- National Institute for Health and Care Excellence. NICE Pathways. 2021. Available online: https://pathways.nice.org.uk/pathways/acute-coronary-syndromes-early-management#path=view%3A/pathways/acute-coronary-syndromes-early-management/acute-coronary-syndromes-early-management-of-acute-stemi.xml&content=view-node%3Anodes-initial-drug-therapy (accessed on 1 March 2021).
- Bhatnagar, P.; Wickramasinghe, K.; Wilkins, E.; Townsend, N. Trends in the epidemiology of cardiovascular disease in the UK. Heart 2016, 102, 1945–1952. [Google Scholar] [CrossRef]
- Pearson-Stuttard, J.; Bajekal, M.; Scholes, S.; O’Flaherty, M.; Hawkins, N.M.; Raine, R.; Capewell, S. Recent UK trends in the unequal burden of coronary heart disease. Heart 2012, 98, 1573–1582. [Google Scholar] [CrossRef]
- Craig, R.; Mindell, J. Health Survey for England 2006: CVD and Risk Factors Adults, Obesity and Risk Factors Children. 2008. Available online: https://digital.nhs.uk/data-and-information/publications/statistical/health-survey-for-england/health-survey-for-england-2006-cvd-and-risk-factors-for-adults-obesity-and-risk-factors-for-children (accessed on 1 March 2021).
- Timmis, A.; Townsend, N.; Gale, C.P.; Torbica, A.; Lettino, M.; E Petersen, S.; A Mossialos, E.; Maggioni, A.P.; Kazakiewicz, D.; May, H.T.; et al. European Society of Cardiology: Cardiovascular Disease Statistics 2019. Eur. Heart J. 2020, 41, 12–85. [Google Scholar] [CrossRef]
- World Health Organization. Global Atlas on Cardiovascular Disease Prevention and Control. 2021. Available online: http://www.who.int/cardiovascular diseases/publications/atlas cvd/en/ (accessed on 27 June 2021).
- Greco, A.; Brugnera, A.; Adorni, R.; D’Addario, M.; Fattirolli, F.; Franzelli, C.; Giannattasio, C.; Maloberti, A.; Zanatta, F.; Steca, P. Protein Intake and Physical Activity in Newly Diagnosed Patients with Acute Coronary Syndrome: A 5-Year Longitudinal Study. Nutrients 2021, 13, 634. [Google Scholar] [CrossRef] [PubMed]
- Möller-Leimkühler, A.M. Gender differences in cardiovascular disease and comorbid depression. Dialogues Clin. Neurosci. 2007, 9, 71–83. [Google Scholar]
- Rozanski, A.; Blumenthal, J.; Kaplan, J. Impact of psychological factors on the pathogenesis of cardiovascular disease and implications for therapy. Circulation 1999, 99, 2192–2217. [Google Scholar] [CrossRef] [Green Version]
- Hemingway, H.; Marmot, M. Psychosocial factors in the aetiology and prognosis of coronary heart disease: Systematic review of prospective cohort studies. BMJ 1999, 318, 1460–1467. [Google Scholar] [CrossRef]
- NHS Digital. Health Survey for England 2017. In Summary of Key Findings; NHS Digital: Leeds, UK, 2018; pp. 1–32. [Google Scholar]
- Scarborough, P.; Wickramasinghe, K.; Bhatnagar, P.; Rayner, P. Trends in Coronary Heart Disease 1961–2011; British Heart Foundation: London, UK, 2011. [Google Scholar]
- Koopman, C.; Bots, M.L.; Van Dis, I.; Vaartjes, I. Shifts in the age distribution and from acute to chronic coronary heart disease hospitalizations. Eur. J. Prev. Cardiol. 2016, 23, 170–177. [Google Scholar] [CrossRef]
- British Heart Foundation. Heart and Circulatory Disease Statistics 2019. 2020. Available online: https://www.bhf.org.uk/what-we-do/our-research/heart-statistics/heart-statistics-publications/cardiovascular-disease-statistics-2019 (accessed on 1 March 2021).
- Naser, A.; Wang, Q.; Wong, L.Y.L.; Ilomaki, J.; Bell, J.S.; Fang, G.; Wong, I.C.K.; Wei, L. Hospital Admissions due to Dysglycaemia and Prescriptions of Antidiabetic Medications in England and Wales: An Ecological Study. Diabetes Ther. 2018, 9, 153–163. [Google Scholar] [CrossRef] [Green Version]
- Mills, E.; O’Regan, C.; Eyawo, O.; Wu, P.; Mills, F.; Berwanger, O.; Briel, M. Intensive statin therapy compared with moderate dosing for prevention of cardiovascular events: A meta-analysis of >40,000 patients. Eur. Heart J. 2011, 32, 1409–1415. [Google Scholar] [CrossRef]
- Parker, J.; Parker, J. Nitrate therapy for stable angina pectoris. N. Engl. J. Med. 1998, 338, 520–531. [Google Scholar] [CrossRef] [PubMed]
- Teo, K.; Yusuf, S.; Furberg, C. Effects of prophylactic antiarrhythmic drug therapy in acute myocardial infarction. An overview of results from randomized controlled trials. JAMA 1993, 270, 1589–1595. [Google Scholar] [CrossRef] [PubMed]
- Warren, S.; Brewer, D.; Orgain, E. Long-term propranolol therapy for angina pectoris. Am. J. Cardiol. 1976, 37, 420–426. [Google Scholar] [CrossRef]
- Weiss, R.; Ferry, D.; Pickering, E.; Smith, L.; Dennish, G.; Krug-Gourley, S.; Lukas, M. Effectiveness of three different doses of carvedilol for exertional angina. Carvedilol-Angina Study Group. Am. J. Cardiol. 1998, 82, 927–931. [Google Scholar] [CrossRef]
- Conrad, N.; Judge, A.; Tran, J.; Mohseni, H.; Hedgecott, D.; Crespillo, A.P.; Allison, M.; Hemingway, H.; Cleland, J.G.; McMurray, J.J.V.; et al. Temporal trends and patterns in heart failure incidence: A population-based study of 4 million individuals. Lancet 2018, 291, 572–580. [Google Scholar] [CrossRef] [Green Version]
- Murphy, N.; Macintyre, K.; Stewart, S.; Hart, C.L.; Hole, D.; McMurray, J.J.V. Long-term cardiovascular consequences of obesity: 20-year follow-up of more than 15,000 middle-aged men and women (the Renfrew-Paisley study). Eur. Heart J. 2006, 27, 96–106. [Google Scholar] [CrossRef]
- Finucane, M.; Stevens, G.; Cowan, M.J.; Danaei, G.; Lin, J.K.; Paciorek, C.J.; Singh, G.M.; Gutierrez, H.R.; Lu, Y.; Bahalim, A.N.; et al. Global Burden of Metabolic Risk Factors of Chronic Diseases Collaborating Group (Body Mass Index). National, regional, and global trends in body-mass index since 1980: Systematic analysis of health examination surveys and epidemiological studies with 960 country-years and 9·1 million participants. Lancet 2011, 377, 557–567. [Google Scholar] [PubMed] [Green Version]
- Howel, D. Trends in the prevalence of obesity and overweight in English adults by age and birth cohort, 1991–2006. Public Health Nutr. 2011, 14, 27–33. [Google Scholar] [CrossRef] [Green Version]
- Rokholm, B.; Baker, J.; Sørensen, T. The levelling off of the obesity epidemic since the year 1999—A review of evidence and perspectives. Obes. Rev. 2010, 11, 835–846. [Google Scholar] [CrossRef] [PubMed]
- Department of Health. Choosing Health: Making Healthy Choices Easier; The Stationery Office: London, UK, 2004. [Google Scholar]
- Falk, E.; Shah, P.; Fuster, V. Coronary plaque disruption. Circulation 1995, 92, 657–671. [Google Scholar] [CrossRef]
- Agatston, A.; Janowitz, F.W.R.; Hildner, F.J.; Zusmer, N.R.; Viamonte, M., Jr.; Detrano, R. Quantification of coronary artery calcium using ultrafast computed tomography. J. Am. Coll. Cardiol. 1990, 15, 827–832. [Google Scholar] [CrossRef] [Green Version]
- Kalra, D.; Heo, R.; Valenti, V.; Nakazato, R.; Min, J.K. Role of computed tomography for diagnosis and risk stratification of patients with suspected or known coronary artery disease. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 1144–1154. [Google Scholar] [CrossRef] [Green Version]
- SCOT-HEART Investigators. Coronary CT Angiography and 5-Year Risk of Myocardial Infarction. N. Engl. J. Med. 2018, 379, 924–933.
- Dangas, G.; Claessen, B.E.; Caixeta, A.; Sanidas, E.A.; Mintz, G.S.; Mehran, R. In-stent restenosis in the drug-eluting stent era. J. Am. Coll. Cardiol. 2010, 56, 1897–1907. [Google Scholar] [CrossRef] [Green Version]
- James, S.; Åkerblom, A.; Cannon, C.P.; Emanuelsson, H.; Husted, S.; Katus, H.; Skene, A.; Steg, P.G.; Storey, R.; Harrington, R.; et al. Comparison of ticagrelor, the first reversible oral P2Y(12) receptor antagonist, with clopidogrel in patients with acute coronary syndromes: Rationale, design, and baseline characteristics of the PLATelet inhibition and patient Outcomes (PLATO) trial. Am. Heart J. 2009, 157, 599–605. [Google Scholar] [CrossRef] [PubMed]
- Varghese, M.; Bhatheja, S.; Baber, U.; Kezbor, S.; Chincholi, A.; Chamaria, S.; Buckstein, M.; Bakst, R.; Kini, A.; Sharma, S.; et al. Intravascular Brachytherapy for the Management of Repeated Multimetal-Layered Drug-Eluting Coronary Stent Restenosis. Circ. Cardiovasc. Interv. 2018, 11, e006832. [Google Scholar] [CrossRef] [PubMed]
- Peretti, A.; Maloberti, A.; Garatti, L.; Palazzini, M.; Triglione, N.; Occhi, L.; Sioli, S.; Sun, J.W.; Moreo, A.; Beretta, G.; et al. Functional Improvement After Outpatient Cardiac Rehabilitation in Acute Coronary Syndrome Patients is Not Related to Improvement in Left Ventricular Ejection Fraction. High Blood Press. Cardiovasc. Prev. 2020, 27, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Office for National Statistics (ONS). National Life Tables—Life Expectancy in the UK: 2017 to 2019. 2021. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/lifeexpectancies/bulletins/nationallifetablesunitedkingdom/2017to2019 (accessed on 23 May 2021).
- Libby, P.; Aikawa, M. Mechanisms of plaque stabilization with statins. Am. J. Cardiol. 2003, 91, 4B–8B. [Google Scholar] [CrossRef]
- Rockenschaub, P.; Nguyen, V.; Aldridge, R.W.; Acosta, D.; Garcia-Gomez, J.M.; Sáez, C. Data-Driven discovery of changes in clinical code usage over time: A case-study on changes in cardiovascular disease recording in two English electronic health records databases (2001–2015). BMJ Open 2020, 10, e034396. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Codes | Indication | Percentage from Total Number of Admissions |
|---|---|---|
| I20 | Angina pectoris | 27.3% |
| I21 | Acute myocardial infarction | 29.7% |
| I22 | Subsequent ST elevation (STEMI) and non-ST elevation (NSTEMI) myocardial infarction | 3.7% |
| 123 | Certain current complications following ST elevation (STEMI) and non-ST elevation (NSTEMI) myocardial infarction (within the 28-day period) | 0.1% |
| I24 | Other acute ischemic heart diseases | 2.4% |
| I25 | Chronic ischemic heart disease | 36.7% |
| CVD Medication | Prescriptions Rate in 2004 Prescriptions per 100,000 Persons (95% CI) | Prescriptions Rate in 2019 Prescriptions per 100,000 Persons (95% CI) | % Change from 2004–2019 | p-Value |
|---|---|---|---|---|
| Positive Inotropic Drugs | 11,028.16 (11,018.49–11,037.82) | 7102.62 (7095.15–7110.09) | −35.6% | <0.01 |
| Diuretics | 98,042.82 (98,038.55–98,047.10) | 76,695.80 (76,683.51–76,708.09) | −21.8% | <0.01 |
| Anti-Arrhythmic Drugs | 3540.07 (3534.37–3545.77) | 2296.04 (2291.68–2300.39) | −35.1% | <0.001 |
| Beta-Adrenoceptor Blocking Drugs | 70,323.27 (70,309.17–70,337.36) | 91,063.67 (91,055.38–91,071.96) | 29.5% | <0.001 |
| Antihypertensive Therapy | 103,520.74 (103,491.01–103,550.47) | 170,476.79 (170,442.22–170,511.36) | 64.7% | <0.001 |
| Nitrates, Calcium Channel Blockers, and Potassium Activators | 82,651.10 (82,624.23–82,677.98) | 118,274.89 (118,245.21–118,304.58) | 43.1% | <0.001 |
| Sympathomimetic | 9.34 (9.04–9.64) | 201.74 (200.44–203.05) | 2060.4% | <0.01 |
| Anticoagulants And Protamine | 15,909.04 (15,897.75–15,920.33) | 42,420.62 (42,406.26–42,434.99) | 166.6% | <0.001 |
| Antiplatelet Drugs | 73,775.65 (73,762.08–73,789.22) | 80,284.59 (80,273.02–80,296.15) | 8.8% | 0.095 |
| Anti-fibrinolytic Drugs and Haemostatics | 821.21 (818.43–824.00) | 983.75 (980.88–986.62) | 19.8% | 0.001 |
| Lipid-Regulating Drugs | 79,712.64 (79,686.21–79,739.08) | 174,784.02 (174,749.11–174,818.93) | 119.3% | <0.001 |
| Local Sclerosants | 0.90 (0.81–1.00) | 0.02 (0.01–0.03) | −98.1% | <0.001 |
| Table | Positive Inotropic Drugs | Diuretics | Anti-Arrhythmic Drugs | Beta-Adrenoceptor Blocking Drugs | Antihypertensive Therapy | Nitrates, Calcium Channel Blockers, and Potassium Channel Activators | Antiplatelet Drugs | Anti-fibrinolytic Drugs and Haemostatics | Lipid-Regulating Drugs |
|---|---|---|---|---|---|---|---|---|---|
| Angina Pectoris | N/A | N/A | N/A | −0.944 ** | −0.855 ** | −0.926 ** | −0.027 | N/A | −0.893 ** |
| Acute Myocardial Infarction | −0.815 * | −0.795 ** | −0.684 ** | 0.838 ** | 0.448 | 0.589 * | −0.379 | N/A | 0.520 * |
| Subsequent ST Elevation (STEMI) and Non-ST Elevation (NSTEMI) Myocardial Infarction | 0.855 ** | 0.821 ** | 0.795 ** | −0.896 ** | −0.621 * | −0.729 ** | 0.203 | −0.718 ** | −0.674 ** |
| Certain Current Complications Following ST Elevation (STEMI) and Non-ST Elevation (NSTEMI) Myocardial Infarction (within the 28 Day Period) | 0.753 ** | 0.711 ** | 0.869 ** | −0.789 ** | −0.875 ** | −0.879 ** | −0.234 | −0.889 ** | −0.874 ** |
| Chronic Ischemic Heart Disease | 0.935 ** | 0.923 ** | 0.824 ** | −0.951 ** | −0.578 * | −0.715 ** | 0.382 | N/A | −0.648 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hemmo, S.I.; Naser, A.Y.; Alwafi, H.; Mansour, M.M.; Alanazi, A.F.R.; Jalal, Z.; Alsairafi, Z.K.; Paudyal, V.; Alomari, E.; Al-Momani, H.; et al. Hospital Admissions Due to Ischemic Heart Diseases and Prescriptions of Cardiovascular Diseases Medications in England and Wales in the Past Two Decades. Int. J. Environ. Res. Public Health 2021, 18, 7041. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137041
Hemmo SI, Naser AY, Alwafi H, Mansour MM, Alanazi AFR, Jalal Z, Alsairafi ZK, Paudyal V, Alomari E, Al-Momani H, et al. Hospital Admissions Due to Ischemic Heart Diseases and Prescriptions of Cardiovascular Diseases Medications in England and Wales in the Past Two Decades. International Journal of Environmental Research and Public Health. 2021; 18(13):7041. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137041
Chicago/Turabian StyleHemmo, Sara Ibrahim, Abdallah Y. Naser, Hassan Alwafi, Munthir M. Mansour, Abeer F. R. Alanazi, Zahraa Jalal, Zahra Khalil Alsairafi, Vibhu Paudyal, Esra’a Alomari, Hamzeh Al-Momani, and et al. 2021. "Hospital Admissions Due to Ischemic Heart Diseases and Prescriptions of Cardiovascular Diseases Medications in England and Wales in the Past Two Decades" International Journal of Environmental Research and Public Health 18, no. 13: 7041. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137041