
Level of Knowledge of Medical Staff on the Basis of the Survey in Terms of Risk Management, Associated with Clostridioides difficile Infections

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
- -
- Medical personnel can be a vector for the transmission of infections caused by C. difficile;
- -
- Medical workers’ knowledge of C. difficile is insufficient;
- -
- Shortcomings related to the implementation of medical procedures are the result of a limited number of specialist training courses for medical personnel.
- -
- what is the level of knowledge of medical personnel regarding the ways of spreading and preventing the transmission of infections caused by C. difficile in hospitalized patients?
- -
- what is the current status of activities aimed at reducing HAI transmission?
- -
- are the infection risk management tools used in an optimal and adequate manner to the threat level?
- -
- does the seniority and professional experience of medical employees translate into the safety of medical services in terms of the frequency of adverse events?
2. Materials and Methods
3. Results
3.1. General Characteristics
3.2. Knowledge of Healthcare Professionals on Hand Hygiene Procedures and Infections Caused by C. difficile
- Self-assessment of knowledge about the hand hygiene procedure: (p = 0.0002)—a very good and good score was given by 93.4% of all medical personnel, while average and insufficient score was provided by 6.6%. Better knowledge was demonstrated among the nurses and the worse among the rest of the medical staff (doctors, paramedics working in the hospital and other medical professionals employed in the hospital).
- Self-assessment concerning knowledge about CDI: (p < 0.0001)—it was graded as very good and good by 70.1% of all medical personnel, whereas as average or insufficient by 29.9%. Higher percentages of worse results were given by the remaining medical personnel.
- Awareness of the ways CDI are spread in the hospital setting: (p < 0.0001)—the majority of medical personnel knew the routes of transmission of CDI (77.1%), however 22.9% of the respondents lacked this knowledge.
- How often hand hygiene procedures are followed at work: (p = 0.0120)—in 93.8% of cases those procedures are performed routinely, and in 6.2% of cases they are performed rarely or sometimes even totally forgotten.
- The number of professional trainings in hand hygiene procedures organized by the employer: (p = 0.7540)—according to 52.1% of the respondents, it is sufficient or too frequent, while as many as 47.9% claim that it is too small. Very similar percentages were reported among nurses and other medical personnel.
- The frequency of supervision for the implementation of the hand hygiene procedure in the workplace: (p < 0.0001)—the vast majority, i.e., 44.6%, reported very rare controls, while controls that happen every quarter, every six months and once a year accounted for 19.3%, 17.5% and 18.6% respectively.
- In cases where the employer carried out periodic inspections of the compliance with the hand hygiene procedure: the most common (50.1%) was a check-up performed by an epidemiologist or an epidemiological nurse (p = 0.0059), but according to the second common answer (26.9%), no controls were performed (p < 0.0001).
3.3. Answers to Questions Checking the Knowledge of Medical Personnel
- To the question: Does proper hand hygiene of medical personnel influence nosocomial infections? (p = 0.0017)—99.0% of employees gave the correct answer and 1.0% chose the wrong answer.
- To the question: Purposefulness of the hand hygiene procedure: (p = 0.0014)—91.8% of the respondents gave the correct answer and 8.2% responded wrongly.
- To the multiple-choice question: (p = 0.0002)—in a hospital, cross-infection may happen via the following: the most responses indicated that by transmission of microorganisms from an infected patient to another patient (85.9%) and from an infected patient to medical personnel (77.6%). To the question: The main vector of transmission of nosocomial infections is: (p < 0.0001)—the majority of the respondents (93.7%) indicated hands of medical personnel, whereas 6.4% of them pointed to reusable and disposable equipment.
- To the question: When should a hand hygiene procedure be performed when it in necessary to examine a patient suspected of having CDI: 95.3% of the respondents gave the correct answer that both before and after the examination of the patient, while 4.7% submitted a wrong answer.
- To the question: Please choose a hand hygiene method when medical staff have contact with a patient infected or suspected of having CDI: (p < 0.0001)—the correct answer (washing hands under running water with soap) was given by 59.0% of the employees, but as much as 41.0% of the respondents answered wrongly to this question.
- To the question: According to the procedure, the time spent on hand hygiene when staff has contact with a patient infected or suspected of being infected with C. difficile should take: the correct answer (40–60 s) was given by 53.5% of the medical personnel, while as much as 46.5% of the respondents chose too short hand washing time (for p = 0.0065).
- To the question: What is your opinion on the hand hygiene procedure: (p = 0.0401)—the correct answer (protects against infection transmission) was submitted by 98.6% of the respondents, and 1.4% gave the wrong answer.
- To the question: “bare below the elbows” policy (BBE—this strategy involves the dress code of medical personnel. It consists of eliminating wearing jewelry and ties by medical employees, additionally wearing short-sleeved aprons in winter, as well as eliminating wearing varnished and long nails): (p < 0.0001)—the correct answer (limiting the patient’s contact with contaminated clothing of medical personnel, promoting hand and wrist hygiene) was given by 40.3% of the respondents, while 59.7% gave incorrect answers.
3.4. Level of Knowledge of Medical Personnel
3.5. Analysis of the Workplace and the Frequency of Monitoring the Implementation of Hand Hygiene Procedures
3.6. Analysis of the Workplace and the Tools Used by the Employer When Conducting Periodic Inspections of Medical Personnel
3.7. Assessing Various Factors That Have an Impact on Giving the Correct Answer
3.7.1. Work Experience in the Profession vs. the Correct Answers to the Knowledge Check Questions
- Hand hygiene procedure: (p = 0.0084)—the correct answer was most often given by respondents with over 20 years of work experience (94.3%) and 10–15 years of work experience (94.1%).
- The main vector of transmission of nosocomial infections is: (p < 0.0001)—the correct answer was most often given by respondents with over 20 years of work experience (97.0%) and 15–20 years of work experience (96.8%).
- Please select a hand hygiene method when staff come into contact with a patient that is either infected or is suspected of being infected with C. difficile: (p = 0.0102)—the correct answer was most often provided by respondents with work experience up to 5 years (64.5%).
- According to the procedure, the time spent on hand hygiene when staff come into contact with a patient that is either infected or suspected of having CDI should take: (p <0.0001)—the correct answer was most often provided by respondents with up to 5 years of work experience (62.1%).
- “Bare below the elbows” policy (BBE) concerns: (p < 0.0001)—the correct answer was most often given by respondents with up to 5 years of work experience (51.6%).
3.7.2. Workplace vs. the Correctly Answered Knowledge Check Questions
- Hand hygiene procedure: (p = 0.0016)—the correct answer was most often provided by respondents working in hospital surgical wards (93.3%) and non-surgical wards (92.6%).
- The main vector of transmission of nosocomial infections is: (p = 0.0146)—the correct answer was most often provided by the respondents working in non-surgical (95.3%) and surgical (93.7%) wards.
- Please select a hand hygiene method when staff come into contact with a patient that is either infected or is suspected of being infected with C. difficile: (p = 0.0003)—the correct answer was most often provided by the respondents working in a hospital ward (61.7%) and non-surgery ward (60.8%).
3.7.3. Self-Assessment of Knowledge about the Hand Hygiene Procedure vs. Correctly Answered Knowledge Check Questions
- The main vector of transmission of nosocomial infections is: (p = 0.0134)—the correct answer was most often given by the respondents who described their knowledge about hand hygiene as good (94.5%) and very good (93.6%).
- Please choose a hand hygiene method when staff come into contact with a patient that is either infected or is suspected of being infected with C. difficile: (p = 0.0420)—the correct answer was most often provided by the respondents who described their knowledge about hand hygiene as good (61.9%).
- “Bare below the elbows” policy (BBE) concerns: (p = 0.0102)—the correct answer was most often given by the respondents who described their knowledge about hand hygiene as good (43.9%).
3.7.4. Self-Assessment of Knowledge about CDI vs. Correctly Answered Knowledge Check Questions
- Is the number of nosocomial infections influenced by the proper hand hygiene performed by healthcare professionals? (p = 0.0332)—the correct answer was most often given by the respondents who described their knowledge about CDI as good (99.5%), average (99.1%) and very good (98.3%).
- The main vector of transmission of nosocomial infections is: (p = 0.0006)—the correct answer was most often given by the respondents who described their knowledge about infections caused by C. difficile as good (95.4%) and very good (93.6%).
- A medical worker is to examine a patient suspected of having CDI, in which case the procedure involving hand hygiene should be carried out: (p = 0.0025)—the correct answer was most often given by the respondents who described their knowledge as average (96.4%), good (95.6%) and very good (94.8%).
- Please choose a hand hygiene method when staff come into contact with a patient that is either infected or is suspected of being infected with C. difficile: (p < 0.0001)—the correct answer was most often provided by the respondents who described their knowledge about CDI as very good (67.0%).
- According to the procedure, the time spent on hand hygiene when staff come into contact with a patient that is either infected or suspected of having CDI should take: (p = 0.0019)—the correct answer was most often given by the respondents who described their knowledge about CDI as very good (57.1%) and average (57.0%).
- What is your opinion on the hand hygiene procedure? (p = 0.0006)—the correct answer was most often provided by the respondents who described their knowledge about CDI as average (99.3%), good (98.9%) and very good (98.3%).
3.7.5. Number of Professional Trainings vs. Correctly Answered Knowledge Check Questions
- Is the number of nosocomial infections influenced by the proper hand hygiene of healthcare professionals? (p = 0.0058)—the correct answer was most often given by the respondents who believed that the number of trainings was too small (99.3%) and sufficient (99.2%).
- The main vector of transmission of nosocomial infections is: (p = 0.0038)—the correct answer was most often given by the respondents who believed that the number of trainings was sufficient (94.1%) or too small (93.9%).
- A medical worker is to examine a patient suspected of having CDI, in which case the procedure involving hand hygiene should be carried out: (p = 0.0003)—the correct answer was most often provided by the respondents who believed that the number of trainings was sufficient (96.2%) or too small (95.0%).
- What is your opinion on the hand hygiene procedure? (p < 0.0001)—the correct answer was most often given by the respondents who believed that the number of trainings was sufficient (99.2%) or too small (98.9%).
3.7.6. The Frequency of Controls on the Implementation of the Hand Hygiene Procedure in the Workplace vs. Correctly Answered Knowledge Check Questions
3.8. Analysis of Work Experience in the Profession and the Level of Knowledge among Medical Personnel
3.9. Self-Assessment of Knowledge on the Hand Hygiene Procedure vs. the Level of Knowledge among Medical Personnel
3.10. Self-Evaluation of Knowledge on CDI vs. the Level of Knowledge among Medical Personnel
3.11. Performing Hand Hygiene Procedures vs. the Level of Knowledge among Medical Personnel
3.12. The Number of Professional Trainings vs. the Level of Knowledge among Medical Personnel
3.13. The Frequency of Checks on the Implementation of the Hand Hygiene Procedure in the Workplace vs. the Level of Knowledge among Medical Personnel
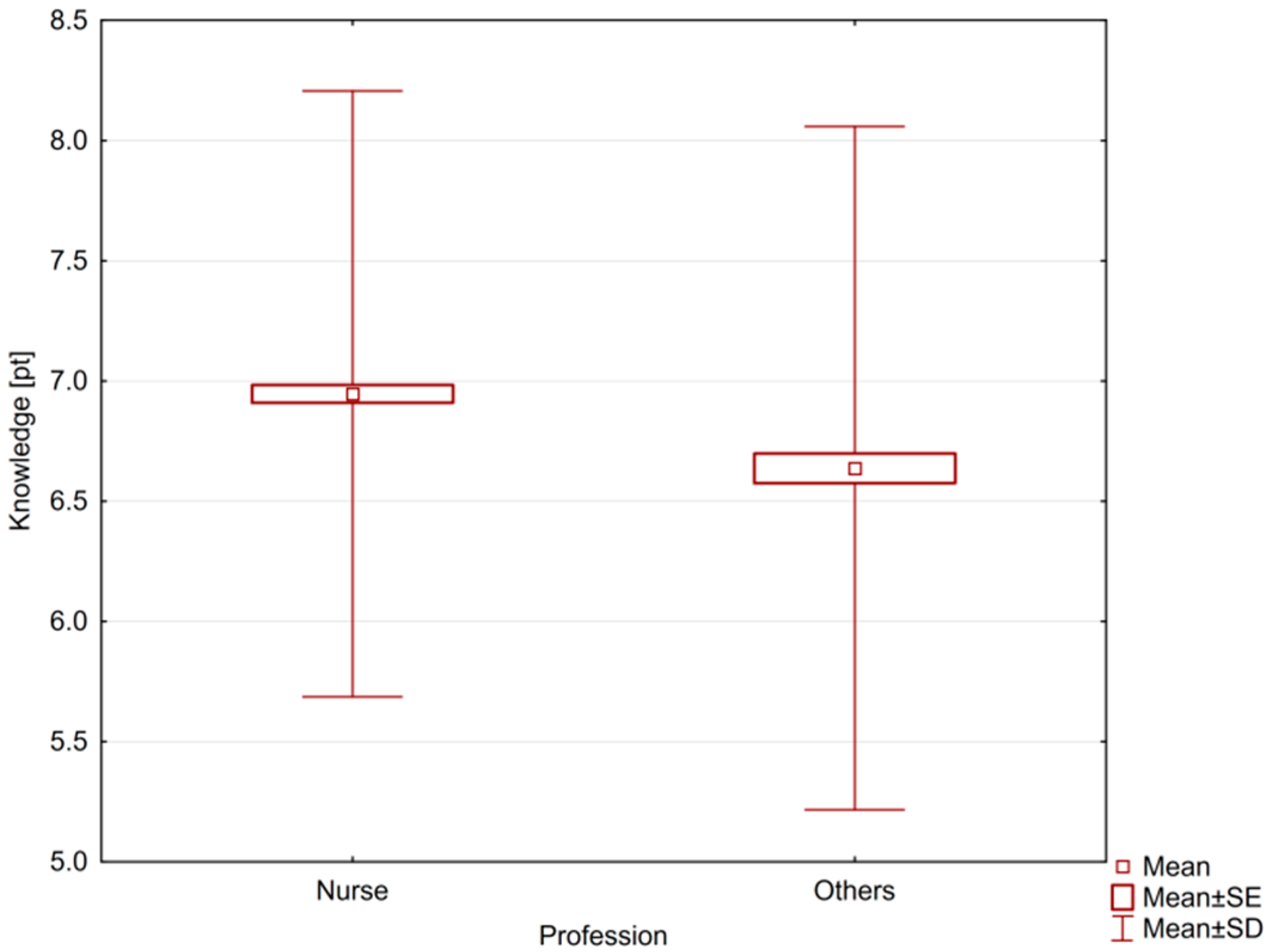
- Despite the average score of 6.85 (out of 10 possible) obtained for correctly answered questions that evaluated the knowledge of medical workers, this value is not satisfactory as differences in the level of knowledge among different groups were noticed. The average rating obtained by the nurses was higher (6.95) than the average score achieved by the other medical workers (6.64).
- The knowledge of healthcare professionals about C. difficile and the transmissions of CDI in a hospital environment is unsatisfactory.
- The risk management of infections in hospitals that included, among others, training and control of the spread of C. difficile outbreaks, was assessed to be at a fairly low level. The number of professional training courses for medical personnel is insufficient to meet the demand, and hand hygiene supervision does not in fact happen in practice. This is also due to insufficient understanding of the staff about ways of transmission of infections, poor knowledge of methods of approaching the patient while still maintaining a satisfactory level of hand hygiene.
- Seniority and professional experience play an important role in preventing HAI. Most of the questions relating to general hospital hygiene were best answered by people with longer work experience, like 20 years or more, and also by those with 10–15 years of work experience. On the other hand, questions about the ways of spreading and preventing transmission of infections caused by C. difficile were better answered by people with short work experience, i.e., ranging from 0 to 5 years.
- The survey analysis showed that transmission of C. difficile-related infections may be a difficult problem to solve in hospitals. This is confirmed not only by the unsatisfactory results of medical personnel’s knowledge about C. difficile and the ways of spreading this pathogen, but also by annual epidemiological data (NIH, GIS), which indicate that the number of CDI continues to grow. In 2019, there was 9698 cases, compared to 4457 in 2013. On the top of that, from among all alarm factors causing outbreaks in hospitals in 2019, C. difficile accounted for the largest percentage, namely 33%.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hota, S.S.; Doll, M.; Bearman, G. Preventing Clostridioides difficile infection in hospitals: What is the endgame? BMJ Qual. Saf. 2020, 29, 157–160. [Google Scholar] [CrossRef]
- Doll, M.; Marra, A.R.; Apisarnthanarak, A.; Saif Al-Maani, A.; Abbas, S.; Rosenthal, V.D. Prevention of Clostridioides difficile in hospitals: A position paper of the International Society for Infectious Diseases. Int. J. Infect. Dis. 2021, 102, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Baur, D.; Gladstone, B.P.; Burket, F.; Carrara, E.; Foschi, F.; Döbele, S. Effect of antibiotic stewardship on the incidence of infection and colonisation with antibiotic-resistant bacteria and Clostridium difficile infection: A systematic review and meta-analysis. Lancet Infect. Dis. 2017, 17, 990–1001. [Google Scholar] [CrossRef]
- Djuikoue, I.C.; Tambo, E.; Tazemda, G.; Njajou, O.; Makoudjou, D. Evaluation of inpatients Clostridium difficile prevalence and risk factors in Cameroon. Infect. Dis. Poverty 2020. [Google Scholar] [CrossRef] [PubMed]
- Kiersnowska, Z.; Lemiech-Mirowska, E.; Michałkiewicz, M.; Marczak, M. Hand hygiene as the basic method of reducing Clostridium difficile infections (CDI) in a hospital environment. Ann. Agric. Environ. Med. 2021. [Google Scholar] [CrossRef]
- Lemiech-Mirowska, E.; Kiersnowska, Z.; Michałkiewicz, M.; Depta, A.; Marczak, M. Nosocomial infections as one of the most important problems of healthcare system. Ann. Agric. Environ. Med. 2020. [Google Scholar] [CrossRef]
- Report—Sanitary Condition of the Country 2018. Poland. Chief Sanitary Inspectorate. Available online: https://gis.gov.pl/wp-content/uploads/2019/09/SSK-2018-www-1.pdf (accessed on 17 May 2021).
- Stanek, J.; Zyzik, R. Prevention of healthcare associated infections—Behavioural perspective. Hygeia Public Health 2018, 53, 333–339. Available online: http://www.h-ph.pl/pdf/hyg-2018/hyg-2018-4-333.pdf (accessed on 17 May 2021).
- Ragusa, R.; Giorgianni, G.; Lupo, L.; Sciacca, A.; Rametta, S.; La Verde, M.; Mulè, S.; Marranzano, M.J. Healthcare-associated Clostridium difficile infection: Role of correct hand hygiene in cross-infection control. Prev. Med. Hyg. 2018, 59, E145–E152. Available online: https://pubmed.ncbi.nlm.nih.gov/30083622/ (accessed on 17 May 2021).
- Nowacka, K.; Flitta, R.; Siminska, J.; Porzych, P.; Grzyb, S.; Hagner, W. Hand hygiene for the management of a patient infected with clostridium difficile in the presence of hospital infections. J. Educ. Health Sport 2017, 7, 6. [Google Scholar] [CrossRef]
- Kabała, M.; Aptekorz, M.; Martirosian, G. The role of hospital environment and the hands of medical staff in the transmission of the Clostridioides (Clostridium) difficile infection. Med. Pr. 2019, 70, 739–745. [Google Scholar] [CrossRef]
- Otter, J.A.; Yezli, S.; Salkeld, J.A.G.; French, G.L. Evidence that contaminated surfaces contribute to the transmission of hospital pathogens and an overview of strategies to address contaminated surfaces in hospital settings. Am. J. Infect. Control 2013, 41, 6–11. [Google Scholar] [CrossRef]
- Ojanperä, H.; Kanste, O.I.; Syrjala, H. Hand-hygiene compliance by hospital staff and incidence of health-care-associated infections. Finland. Bull. World Health Organv. 2020, 98, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Kołpa, M.; Grochowska, A.; Gniadek, A.; Jurkiewicz, B. Level of knowledge among medical personnel about infections transferred through direct contact—Results of questionnaire survey. Przegl. Epidemiol. 2015, 69, 503–506. [Google Scholar] [PubMed]
- Kiersnowska, Z.; Lemiech-Mirowska, E.; Ginter-Kramarczyk, D.; Kruszelnicka, I.; Michałkiewicz, M.; Marczak, M. Problems of Clostridium difficile infection (CDI) in Polish healthcare units. Ann. Agric. Environ. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Chwedoruk, M.; Gotlib, J. Assessment of the knowledge of nurses from surgical wards about nosocomial infections transmitted through contact. Med. Ogólna Nauk. Zdrowiu 2014, 20, 192–198. [Google Scholar] [CrossRef]
- Garba, M.; Uche, L. Knowledge attitude and practice of hand washing among healthcare workers in a tertiary health facility in northwest Nigeria. J. Med. Trop. 2019, 21, 73–80. Available online: http://www.jmedtropics.org/text.asp?2019/21/2/73/272912 (accessed on 17 May 2021).
- Omiye, J.A.; Afolaranmi, O.J.; Ghazal, I.D.; Yahya, M.B.; Oduwale, M.A.; Adeyeye, O.H.; Emenyonu, U.K.; Nwaduru, C.E.; Badmos, B.B.; Adekanmbi, O.A. Hand Hygiene Practice Among Health Care Workers in a Tertiary Hospital in Sub-Saharan Africa (Handy Study). West Afr. J. Med. 2019, 36, 116–121. Available online: https://pubmed.ncbi.nlm.nih.gov/31385596/ (accessed on 18 June 2021).
- Report—Sanitary Condition of the Country 2017. Poland. Chief Sanitary Inspectorate. Available online: https://gis.gov.pl/wp-content/uploads/2018/09/CA%C5%81O%C5%9A%C4%86__STAN_SANITARNY_KRAJU___2017.pdf (accessed on 17 May 2021).
- Data from the Chamber of Nurses and Midwives. Available online: https://nipip.pl/liczba-pielegniarek-poloznych-zarejestrowanych-zatrudnionych/ (accessed on 18 June 2021).
- Data from the Chamber of Physicians and Dentists. Available online: https://nil.org.pl/rejestry/centralny-rejestr-lekarzy/informacje-statystyczne (accessed on 18 June 2021).
- Data from Statistics Poland without Gender Breakdown. Available online: https://ratownicy24.pl/gus-o-pomocy-doraznej-i-ratownictwie-medycznym-w-2019r/ (accessed on 18 June 2021).
- Norén, T. Clostridium difficile and the Disease It Causes. Methods in molecular biology. Clifton. N. J. 2010, 35, 646–649. [Google Scholar] [CrossRef]
- Pérez, A.B.; Morales, O.R.; Regino, W.O.; Zuleta, M.G. Clostridium difficile infections in elderly patients. Rev. Col. Gastroenterol. 2013, 28, 50–59. Available online: http://www.scielo.org.co/pdf/rcg/v28n1/en_v28n1a07.pdf (accessed on 17 May 2021).
- Lessa, F.C.; Mu, Y.; Bamberg, W.B.; Beldavs, Z.G.; Dumyati, G.K.; Dunn, J.R.; Farley, M.M.; Holzbauer, S.M.; Meek, J.I.; Phipps, E.C.; et al. Burden of Clostridium difficile infection in the United States. N. Engl. J. Med. 2015, 372, 825–834. [Google Scholar] [CrossRef] [Green Version]
- Crobach, M.J.T.; Vernon, J.J.; Loo, V.G.; Kong, L.Y.; Péchiné, S.; Wilcox, M.H.; Kuijper, E.J. Understanding Clostridium difficile Colonization. Clin. Microbiol. Rev. 2018, 31, 1–29. [Google Scholar] [CrossRef] [Green Version]
- Schäffler, H.; Breitrück, A. Clostridium difficile—From Colonization to Infection. Front. Microbiol. 2018, 9, 1–12. [Google Scholar] [CrossRef] [Green Version]
- McDonald, L.C.; Gerding, D.N.; Johnson, S.; Bakken, J.S.; Carroll, K.C.; Coffin, S.E.; Dubberke, E.R.; Garey, K.W.; Gould, C.V.; Kelly, C.; et al. Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA). Clin. Infect. Dis. 2018. [Google Scholar] [CrossRef]
- Czepiel, J.; Dróżdż, M.; Pituch, H.; Kuijper, E.J.; Perucki, W.; Mielimonka, A.; Goldman, S.; Wultańska, D.; Garlicki, A.; Biesiada, G. Clostridium difficile infection: Review. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 1211–1221. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Han, S.-H.; Yi, J.; Kim, J.-H.; Lee, S.; Moon, H.-W. Composition of gut microbiota in patients with toxigenic Clostridioides (Clostridium) difficile: Comparison between subgroups according to clinical criteria and toxin gene load. PLoS ONE 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rao, K.; Malani, P.N. Diagnosis and Treatment of Clostridioides (Clostridium) difficile Infection in Adults in 2020. JAMA 2020, 323, 1403–1404. [Google Scholar] [CrossRef] [PubMed]
- Piekarska, A.; Panasiuk, A.; Stępień, P.M. Clinical practice guidelines for clostridioides (clostridium) difficile infection and fecal microbiota transplant protocol –recommendations of the polish society of epidemiology and infectious diseases. Prz. Epidemiol. 2020, 74, 69–87. [Google Scholar] [CrossRef]
- Kachrimanidou, M.; Tsintarakis, E. Insights into the Role of Human Gut Microbiota in Clostridioides difficile Infection. Microorganisms 2020, 8, 200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shafiq, M.; Alturkmani, H.; Zafar, Y.; Mittal, Y.; Lodhi, H.; Ullah, W.; Brewer, J. Effects of co-infection on the clinical outcomes of Clostridium difficile infection. Gut Pathog. 2020. [Google Scholar] [CrossRef] [PubMed]
- van Werkhoven, C.H.; Ducher, A.; Berkell, M.; Mysara, M.; Lammens, C.; Torre-Cisneros, J.; Rodríguez-Baño, J.; Herghea, D.; Cornely, O.A.; Biehl, L.M.; et al. Incidence and predictive biomarkers of Clostridioides difficile infection in hospitalized patients receiving broad-spectrum antibiotics. Nat. Commun. 2021, 12, 2240. [Google Scholar] [CrossRef]
- Burnett, E.; Corlett, J. Understanding risk perceptions and responses of the public and health care professionals toward Clostridium difficile: A qualitative interpretive description study. Am. J. Infect. Control 2017, 45, 133–138. [Google Scholar] [CrossRef]
- Domeniconi, G.; Serafino, S.; De Amicis, M.M.; Formica, S. Clostridium difficile infection epidemiology and management: Comparison of results of a prospective study with a retrospective one in a reference teaching and research hospital in Northern Italy. Am. J. Infect. Control 2016, 11, 1214–1218. [Google Scholar] [CrossRef] [PubMed]
- Ramadan, M.A.; Hamza, W.S.; Alfadhli, M.A. Impact of an intervention on the hand hygiene compliance rates in paediatric surgical intensive care units in two tertiary care hospitals. Int. J. Infect. Control 2018, 14, 1–7. [Google Scholar] [CrossRef]
- Bargellini, A.; Borella, P.; Ferri, P.; Ferranti, G.; Marchesi, I. Hand hygiene of medical and nursing students during clinica rotations: A pilot study on knowledge. attitudes and impact on bacterial contamination. Assist. Inferm. Ric. 2012, 31, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Grayson, M.L.; Stewardson, A.J.; Russo, P.L.; Ryan, K.E.; Olsen, K.L.; Havers, S.M. Effects of the Australian National Hand Hygiene Initiative after 8 years on infection control practices, health-care worker education. and clinical outcomes: A longitudinal study. Lancet Infect. Dis. 2018, 18, 1269–1277. [Google Scholar] [CrossRef]
- World Health Organization. WHO Patient Safety 2009. In Hand Hygiene Technical Reference Manual: To be Used by Health-Care Workers. Trainers and Observers of Hand Hygiene Practices; World Health Organization: Geneva, Switzerland, 2009; Available online: https://apps.who.int/iris/handle/10665/44196 (accessed on 17 May 2021).
- Kong, L.Y.; Dendukuri, N.; Schiller, I.; Bourgault, A.-M.; Brassard, P.; Poirier, L.; Lamothe, F.; Béliveau, C.; Michaud, S.; Turgeon, N.; et al. Predictors of asymptomatic Clostridium difficile colonization on hospital admission. Am. J. Infect. Control 2015, 43, 248–253. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Medical Profession | Female | Male | Age up to 40 Years | Age +41 |
|---|---|---|---|---|
| Nurse (1) | 295,571 | 7640 | 15% | 85% |
| Doctor (2) | 82,892 | 59,138 | 26.8% of men and 32.7% of women | 73.2% of men and 67.3% of women |
| Paramedic (3) | 10,300 | No data | No data | |
| Another medical profession | No data | |||
| Parameter | Total n = 1674 | Nurses n = 1133 | Other Medical Personnel n = 541 |
|---|---|---|---|
| Mean () | 6.85 | 6.95 | 6.64 |
| Std. Dev. (SD) | 1.32 | 1.26 | 1.42 |
| Median (M) | 7.0 | 7.0 | 7.0 |
| Q25 | 6.0 | 6.0 | 6.0 |
| Q75 | 8.0 | 8.0 | 8.0 |
| Min. | 1 | 2 | 1 |
| Max. | 10 | 10 | 10 |
| Range | 0–10 | 0–10 | 0–10 |
| Z | 3.83 | ||
| P | 0.0001 | ||
| How Often Are Hand Hygiene Controls Applied in Your Workplace | Workplace | p | |||||
|---|---|---|---|---|---|---|---|
| Clinic n = 311 | Hospital Treatment Ward n = 728 | Hospital Non-Surgical Ward n = 633 | |||||
| n | % | n | % | n | % | ||
| Every quarter | 31 | 10.0 | 159 | 21.8 | 133 | 21.0 | <0.0001 |
| Every 6 months | 43 | 13.8 | 137 | 18.8 | 113 | 17.9 | |
| Once a year | 48 | 15.4 | 152 | 20.9 | 111 | 17.5 | |
| Very rarely; I don’t remember when | 189 | 60.8 | 280 | 38.5 | 276 | 43.6 | |
| Seniority in the Profession | n | Knowledge (Points) | H | p | ||||
|---|---|---|---|---|---|---|---|---|
| Mean () | Std. Dev. (SD) | Median (M) | Min. | Max. | ||||
| 0–5 years | 543 | 7.03 | 1.35 | 7.0 | 2 | 10 | 20.13 | 0.0005 |
| 5–10 years | 264 | 6.73 | 1.38 | 7.0 | 2 | 10 | ||
| 10–15 years | 152 | 6.84 | 1.40 | 7.0 | 1 | 10 | ||
| 15–20 years | 154 | 6.71 | 1.31 | 7.0 | 2 | 9 | ||
| Over 20 years | 559 | 6.76 | 1.23 | 7.0 | 1 | 10 | ||
| I Would Describe My Knowledge on the Hand Hygiene Procedure as: | n | Knowledge (Points) | H | p | ||||
|---|---|---|---|---|---|---|---|---|
| Mean () | Std. Dev. (SD) | Median (M) | Min. | Max. | ||||
| Very good | 738 | 6.74 | 1.30 | 7.0 | 1 | 10 | 9.44 | 0.0089 |
| Good | 824 | 6.96 | 1.31 | 7.0 | 2 | 10 | ||
| Average or insufficient | 110 | 6.67 | 1.52 | 7.0 | 1 | 9 | ||
| I Would Describe My Knowledge on CDI as: | n | Knowledge (Points) | ||||||
|---|---|---|---|---|---|---|---|---|
| Mean () | Std. Dev. (SD) | Median (M) | Min. | Max. | H | p | ||
| Very good | 233 | 6.85 | 1.32 | 7.0 | 1 | 10 | 23.61 | <0.0001 |
| Good | 940 | 6.89 | 1.30 | 7.0 | 2 | 10 | ||
| Average | 442 | 6.89 | 1.28 | 7.0 | 2 | 10 | ||
| Insufficient | 57 | 5.82 | 1.59 | 6.0 | 1 | 9 | ||
| How Often do You Perform a Hand Hygiene Procedure at Work? | n | Knowledge (Points) | ||||||
|---|---|---|---|---|---|---|---|---|
| Mean () | Std. Dev. (SD) | Median (M) | Min. | Max. | Z | p | ||
| Routinely | 1568 | 6.87 | 1.28 | 7.0 | 2 | 10 | 1.99 | 0.0465 |
| Rarely or I happen to forget | 104 | 6.43 | 1.74 | 7.0 | 1 | 10 | ||
| Do You Think That the Number of Hand Hygiene Trainings Organized by the Employer Is: | n | Knowledge (Points) | ||||||
|---|---|---|---|---|---|---|---|---|
| Mean () | Std. Dev. (SD) | Median (M) | Min. | Max. | H | p | ||
| Too frequent | 26 | 5.73 | 2.36 | 6.0 | 1 | 10 | 8.80 | 0.0123 |
| Enough | 845 | 6.88 | 1.28 | 7.0 | 3 | 10 | ||
| Too small | 801 | 6.85 | 1.31 | 7.0 | 1 | 10 | ||
| How Often Are Hand Hygiene Controls Organized in Your Workplace: | n | Knowledge (Points) | ||||||
|---|---|---|---|---|---|---|---|---|
| Mean () | Std. Dev. (SD) | Median (M) | Min. | Max. | H | p | ||
| Every quarter | 323 | 6.74 | 1.32 | 7.0 | 3 | 10 | 2.37 | 0.4996 |
| Every 6 months | 293 | 6.87 | 1.29 | 7.0 | 4 | 10 | ||
| Once a year | 311 | 6.90 | 1.23 | 7.0 | 2 | 10 | ||
| Very rarely. I don’t remember when | 745 | 6.86 | 1.37 | 7.0 | 1 | 10 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kiersnowska, Z.M.; Lemiech-Mirowska, E.; Semczuk, K.; Michałkiewicz, M.; Sierocka, A.; Marczak, M. Level of Knowledge of Medical Staff on the Basis of the Survey in Terms of Risk Management, Associated with Clostridioides difficile Infections. Int. J. Environ. Res. Public Health 2021, 18, 7060. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137060
Kiersnowska ZM, Lemiech-Mirowska E, Semczuk K, Michałkiewicz M, Sierocka A, Marczak M. Level of Knowledge of Medical Staff on the Basis of the Survey in Terms of Risk Management, Associated with Clostridioides difficile Infections. International Journal of Environmental Research and Public Health. 2021; 18(13):7060. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137060
Chicago/Turabian StyleKiersnowska, Zofia Maria, Ewelina Lemiech-Mirowska, Katarzyna Semczuk, Michał Michałkiewicz, Aleksandra Sierocka, and Michał Marczak. 2021. "Level of Knowledge of Medical Staff on the Basis of the Survey in Terms of Risk Management, Associated with Clostridioides difficile Infections" International Journal of Environmental Research and Public Health 18, no. 13: 7060. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18137060