
Psychological Flexibility Is Key for Reducing the Severity and Impact of Fibromyalgia

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. Combined Index of Severity of Fibromyalgia (ICAF)
2.2.2. FIQ
2.2.3. Acceptance and Action Questionnaire-II (AAQ-II)
2.2.4. Pain Catastrophizing Scale (PCS)
2.3. Data Analysis
3. Results
3.1. Characteristics of the Sample
3.2. FM Severity, Impact, and Psychological Constructs
3.3. Correlational Analysis
3.4. Regression and Moderation Analysis
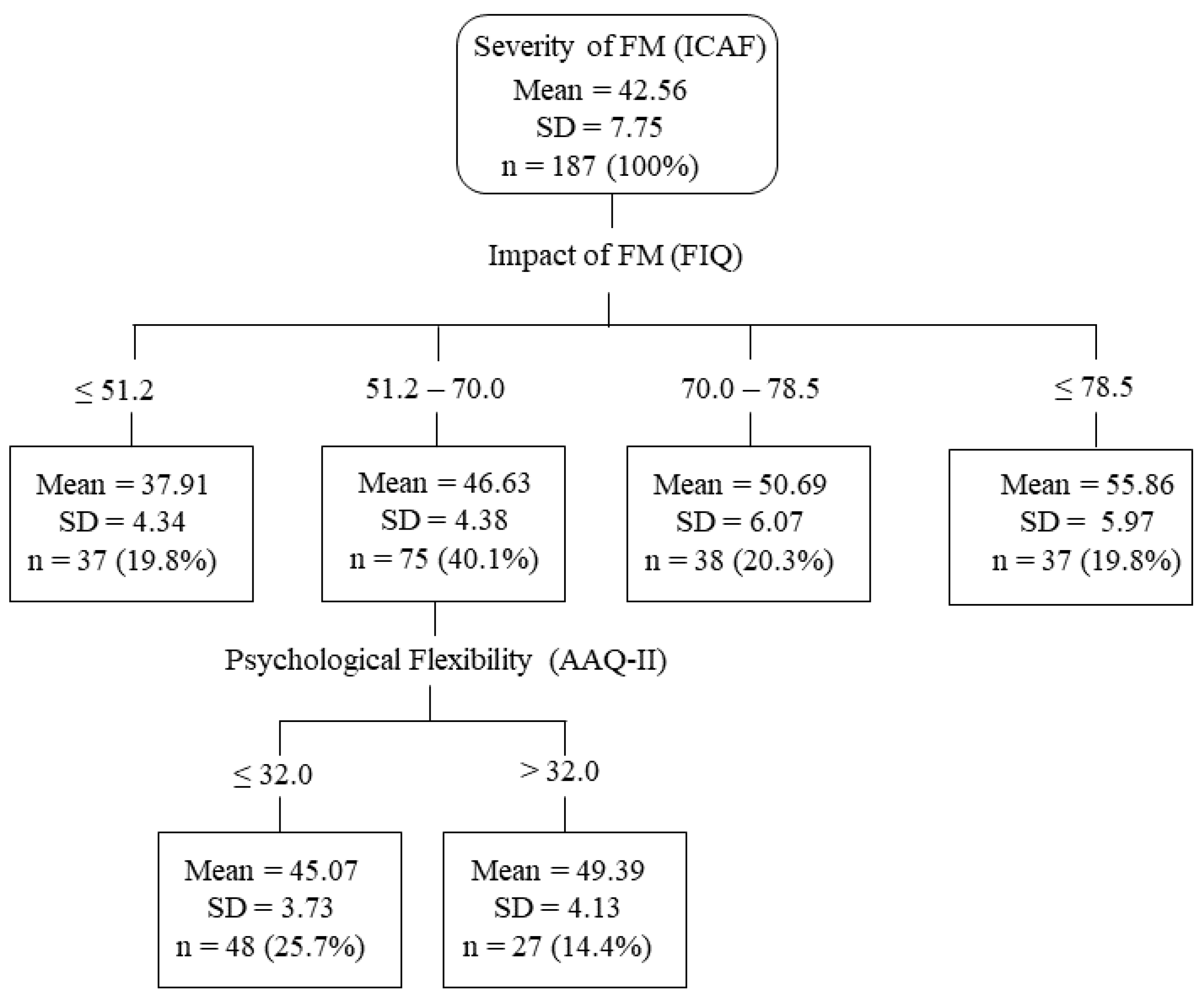
3.5. Decision Tree Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Offenbaecher, M.; Kohls, N.; Ewert, T.; Sigl, C.; Hieblinger, R.; Toussaint, L.L.; Sirois, F.; Hirsch, J.; Vallejo, M.A.; Kramer, S.; et al. Pain is not the major determinant of quality of life in fibromyalgia: Results from a retrospective “real world” data analysis of fibromyalgia patients. Rheumatol. Int. 2021. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.P.; Turner, J.A.; Romano, J.M. Changes in beliefs, catastrophizing, and coping are associated with improvement in multidisciplinary pain treatment. J. Consult. Clin. Psychol. 2001, 69, 655–662. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Maestre, C.; Esteve, R.; López-Martínez, A. Fear-avoidance, pain acceptance and adjustment to chronic pain: A cross-sectional study on a sample of 686 patients with chronic spinal pain. Ann. Behav. Med. 2014, 48, 402–410. [Google Scholar] [CrossRef] [PubMed]
- Lami, M.J.; Martínez, M.P.; Miró, E.; Sánchez, A.I.; Guzmán, M.A. Catastrophizing, Acceptance, and Coping as Mediators Between Pain and Emotional Distress and Disability in Fibromyalgia. J. Clin. Psychol. Med. Set. 2018, 25, 80–92. [Google Scholar] [CrossRef] [PubMed]
- McCracken, L.M. Learning to live with the pain: Acceptance of pain predicts adjustment in persons with chronic pain. Pain 1998, 74, 21–27. [Google Scholar] [CrossRef] [PubMed]
- McCracken, L.M.; Eccleston, C. Coping or acceptance: What to do about chronic pain? Pain 2003, 105, 197–204. [Google Scholar] [CrossRef] [PubMed]
- Esteve, R.; Ramírez-Maestre, C.; López-Martínez, A.E. Adjustment to chronic pain: The role of pain acceptance, coping strategies, and pain-related cognitions. Ann. Behav. Med. 2007, 33, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Baranoff, J.; Hanrahan, S.J.; Kapur, D.; Connor, J.P. Acceptance as a process variable in relation to catastrophizing in multidisciplinary pain treatment. Eur. J. Pain 2013, 17, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Chiros, C.; O’Brien, W.H. Acceptance, appraisals, and coping in relation to migraine headache: An evaluation of interrelationships using daily diary methods. J. Behav. Med. 2011, 34, 307–320. [Google Scholar] [CrossRef] [PubMed]
- Craner, J.R.; Sperry, J.A.; Koball, A.M.; Morrison, E.J.; Gilliam, W.P. Unique Contributions of Acceptance and Catastrophizing on Chronic Pain Adaptation. Int. J. Behav. Med. 2017, 24, 542–551. [Google Scholar] [CrossRef] [PubMed]
- Vowles, K.E.; McCracken, L.M.; Eccleston, C. Patient functioning and catastrophizing in chronic pain: The mediating effects of acceptance. Health Psychol. 2008, 27 (Suppl. 2), S136–S143. [Google Scholar] [CrossRef] [PubMed]
- Catala, P.; Suso-Ribera, C.; Gutierrez, L.; Perez, S.; Lopez-Roig, S.; Peñacoba, C. Is thought management a resource for functioning in women with fibromyalgia irrespective of pain levels? Pain Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Gillanders, D.T.; Ferreira, N.B.; Bose, S.; Esrich, T. The relationship between acceptance, catastrophizing and illness representations in chronic pain. Eur. J. Pain 2013, 17, 893–902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vallejo, M.A.; Rivera, J.; Esteve-Vives, J.; Group ICAF. Development of a self-reporting tool to obtain a combined index of severity of fibromyalgia (ICAF). Health Qual. Life Outcomes 2010, 8, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vallejo, M.A.; Rivera, J.; Esteve-Vives, J.; Rejas, J.; Group ICAF. A confirmatory study of the Combined Index of Severity of Fibromyalgia (ICAF*): Factorial structure, reliability and sensitivity to change. Health Qual. Life Outcomes 2011, 9, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rivera, J.; Vallejo, M.A.; Offenbächer, M. Classifying fibromyalgia patients according to severity: The combined index of severity in fibromyalgia. Rheumatol. Int. 2014, 34, 1683–1689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B.; Yunus, M.B. The American College of Rheumatology preliminary diagnostic criteria for fibromyalgia and measurement of symptom severity. Arthritis Care Res. 2010, 62, 600–610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolfe, F.; Clauw, D.J.; Fitzcharles, M.A.; Goldenberg, D.L.; Häuser, W.; Katz, R.S.; Mease, P.; Russell, A.S.; Russell, I.J.; Winfield, J.B. Fibromyalgia criteria and severity scales for clinical and epidemiological studies: A modification of the ACR Preliminary Diagnostic Criteria for Fibromyalgia. J. Rheumatol. 2011, 38, 1113–1122. [Google Scholar] [CrossRef] [PubMed]
- Burckhardt, C.S.; Clark, S.R.; Bennett, R.M. The fibromyalgia impact questionnaire: Development and validation. J. Rheumatol. 1991, 18, 728–733. [Google Scholar]
- Rivera, J.; González, T. The Fibromyalgia Impact Questionnaire: A validated Spanish version to assess the health status in women with fibromyalgia. Clin. Exp. Rheumatol. 2004, 22, 554–560. [Google Scholar]
- Bennett, R.M.; Bushmakin, A.G.; Cappelleri, J.C.; Zlateva, G.; Sadosky, A.B. Minimal clinically important difference in the fibromyalgia impact questionnaire. J. Rheumatol. 2009, 36, 1304–1311. [Google Scholar] [CrossRef] [PubMed]
- Bond, F.W.; Hayes, S.C.; Baer, R.A.; Carpenter, K.M.; Guenole, N.; Orcutt, H.K.; Waltz, T.; Zettle, R.D. Preliminary psychometric properties of the Acceptance and Action Questionnaire-II: A revised measure of psychological inflexibility and experiential avoidance. Behav. Ther. 2011, 42, 676–688. [Google Scholar] [CrossRef] [Green Version]
- Ruiz, F.J.; Langer Herrera, A.I.; Luciano, C.; Cangas, A.J.; Beltrán, I. Measuring experiential avoidance and psychological inflexibility: The Spanish version of the Acceptance and Action Questionnaire—II. Psicothema 2013, 25, 123–129. [Google Scholar] [PubMed]
- Sullivan, M.J.L.; Bishop, S.R.; Pivik, J. The Pain Catastrophizing Scale: Development and validation. Psychol. Assess. 1995, 7, 524–532. [Google Scholar] [CrossRef]
- García Campayo, J.; Rodero, B.; Alda, M.; Sobradiel, N.; Montero, J.; Moreno, S. Validación de la versión española de la escala de la catastrofización ante el dolor (Pain Catastrophizing Scale) en la fibromialgia [Validation of the Spanish version of the Pain Catastrophizing Scale in fibromyalgia]. Med. Clin. 2008, 131, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis. A Regression-Bases Approach, 2nd ed.; The Guilford Press: New York, NY, USA, 2018. [Google Scholar]
- Loh, W. Fifty years of classification and regression trees. Int. Stat. Rev. 2014, 82, 329–348. [Google Scholar] [CrossRef] [Green Version]
- Stewart, R.W.; Tuerk, P.W.; Metzger, I.W.; Davidson, T.M.; Young, J. A decision-tree approach to the assessment of posttraumatic stress disorder: Engineering empirically rigorous and ecologically valid assessment measures. Psychol. Serv. 2016, 13, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Onwuegbuzie, A.J.; Collins, K.M. An Innovative Method for Stress and Coping Researchers for Analyzing Themes in Mixed Research: Introducing Chi-Square Automatic Interaction Detection (CHAID). In Toward a Broader Understanding of Stress and Coping: Mixed Methods Approaches; Collins, K.M., Onwuegbuzie, A.J., Jio, Q.G., Eds.; Information Age: Charlotte, NC, USA, 2010; pp. 287–301. [Google Scholar]
- Rokach, L.; Maimon, O. Data Mining with Decision Trees: Theory and Applications, 2nd ed.; World Scientific Publishing: Singapore, 2015. [Google Scholar]
- Everitt, B.S. Modern Medical Statistics: A Practical Guide; Hodder Arnold: New York, NY, USA, 2004. [Google Scholar]
- Gayà, T.F.; Ferrer, C.B.; Mas, A.J.; Seoane-Mato, D.; Reyes, F.Á.; Sánchez, M.D.; Dubois, C.M.; Sánchez-Fernández, A.S.; Vargas, L.M.R.; Morales, P.G.; et al. Prevalence of fibromyalgia and associated factors in Spain. Clin. Exp. Rheumatol. 2020, 38, 47–52. [Google Scholar]
- de Boer, M.J.; Steinhagen, H.E.; Versteegen, G.J.; Struys, M.M.; Sanderman, R. Mindfulness, acceptance and catastrophizing in chronic pain. PLoS ONE 2014, 9, e87445. [Google Scholar] [CrossRef] [PubMed]
- Montero-Marín, J.; Navarro-Gil, M.; Puebla-Guedea, M.; Luciano, J.V.; Van Gordon, W.; Shonin, E.; García-Campayo, J. Efficacy of “Attachment-Based Compassion Therapy” in the Treatment of Fibromyalgia: A Randomized Controlled Trial. Front. Psychiatry 2018, 8, 307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armitage, P.; Berry, G.; Matthews, J.N.S. Statistical Methods in Medical Research, 4th ed.; Blackwell: Oxford, UK, 2002. [Google Scholar]
- Trainor, H.; Baranoff, J.; Henke, M.; Winefield, H. Functioning with fibromyalgia: The role of psychological flexibility and general psychological acceptance. Aust. Psychol. 2019, 54, 214–224. [Google Scholar] [CrossRef]
- Åkerblom, S.; Perrin, S.; Rivano Fischer, M.; McCracken, L.M. Predictors and mediators of outcome in cognitive behavioral therapy for chronic pain: The contributions of psychological flexibility. J. Behav. Med. 2021, 44, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Probst, T.; Baumeister, H.; McCracken, L.M.; Lin, J. Baseline Psychological Inflexibility Moderates the Outcome Pain Interference in a Randomized Controlled Trial on Internet-based Acceptance and Commitment Therapy for Chronic Pain. J. Clin. Med. 2018, 8, 24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trompetter, H.R.; Bohlmeijer, E.T.; Fox, J.P.; Schreurs, K.M. Psychological flexibility and catastrophizing as associated change mechanisms during online Acceptance & Commitment Therapy for chronic pain. Behav. Res. Ther. 2015, 74, 50–59. [Google Scholar] [CrossRef] [PubMed]
- Gentili, C.; Rickardsson, J.; Zetterqvist, V.; Simons, L.E.; Lekander, M.; Wicksell, R.K. Psychological Flexibility as a Resilience Factor in Individuals with Chronic Pain. Front. Psychol. 2019, 10, 2016. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Scott, W.; McCracken, L.M. Change in fatigue in acceptance and commitment therapy-based treatment for chronic pain and its association with enhanced psychological flexibility. Eur. J. Pain 2020, 24, 234–247. [Google Scholar] [CrossRef] [PubMed]
- McCracken, L.M.; Zhao-O’Brien, J. General psychological acceptance and chronic pain: There is more to accept than the pain itself. Eur. J. Pain 2010, 14, 170–175. [Google Scholar] [CrossRef] [PubMed]
- Gilpin, H.R.; Keyes, A.; Stahl, D.R.; Greig, R.; McCracken, L.M. Predictors of Treatment Outcome in Contextual Cognitive and Behavioral Therapies for Chronic Pain: A Systematic Review. J. Pain 2017, 18, 1153–1164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turk, D.C.; Okifuji, A.; Sinclair, J.D.; Starz, T.W. Pain, disability, and physical functioning in subgroups of patients with fibromyalgia. J. Rheumatol. 1996, 23, 1255–1262. [Google Scholar] [PubMed]
- De Rooij, A.; Roorda, L.D.; Otten, R.H.; van der Leeden, M.; Dekker, J.; Steultjens, M.P. Predictors of multidisciplinary treatment outcome in fibromyalgia: A systematic review. Disabil. Rehabil. 2013, 35, 437–449. [Google Scholar] [CrossRef] [PubMed]
- Dick, A.M.; Niles, B.L.; Street, A.E.; DiMartino, D.M.; Mitchell, K.S. Examining mechanisms of change in a yoga intervention for women: The influence of mindfulness, psychological flexibility, and emotion regulation on PTSD symptoms. J. Clin. Psychol. 2014, 70, 1170–1182. [Google Scholar] [CrossRef] [PubMed]
- Kosek, E.; Rosen, A.; Carville, S.; Choy, E.; Gracely, R.H.; Marcus, H.; Petzke, F.; Ingvar, M.; Jensen, K.B. Lower Placebo Responses After Long-Term Exposure to Fibromyalgia Pain. J. Pain 2017, 18, 835–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variable | Percent | N | Mean (SD) | Range |
|---|---|---|---|---|
| Age (y) | 187 | 51.63 (8.13) | 28–69 | |
| Duration of illness FM (y) | 187 | 9.99 (4.95) | 1–16 | |
| Sex | ||||
| Female | 94.70% | 177 | ||
| Male | 5.30% | 10 | ||
| Marital status | ||||
| Single | 16.00% | 30 | ||
| Married | 76.50% | 143 | ||
| Widow | 2.10% | 4 | ||
| Separated, divorced | 5.30% | 10 | ||
| Work status (n) | ||||
| Employed | 47.30% | 108 | ||
| Unemployed | 24.20% | 55 | ||
| Homemaker | 8.40% | 19 | ||
| On leave | 9.60% | 22 | ||
| Retired | 10.50% | 24 | ||
| Educational status (n) | ||||
| Low (middle school) | 19.80% | 37 | ||
| Medium (high school) | 45.50% | 85 | ||
| High (college) | 34.80% | 65 |
| Questionnaire | Scores |
|---|---|
| ICAF | 47.55 (29.97–65.41; 7.75) |
| FIQ | 64.08 (23–90; 15.00) |
| Catastrophizing | 27.41 (1–52; 11.02) |
| Rumination | 9.02 (0–16; 3.78) |
| Magnification | 5.65 (0–12; 2.79) |
| Helplessness | 12.74 (0–24; 5.19) |
| AAQ-II | 28.82 (7–49; 10.64) |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
|---|---|---|---|---|---|---|---|
| 1. ICAF | −− | ||||||
| 2. FIQ | 0.77 ** | −− | |||||
| 3. Catastrophizing | 0.67 ** | 0.44 ** | −− | ||||
| 4. Rumination | 0.70 ** | 0.60 ** | 0.64 ** | −− | |||
| 5. Magnification | 0.60 ** | 0.54 ** | 0.55 ** | 0.94 ** | −− | ||
| 6. Helplessness | 0.62 ** | 0.48 ** | 0.57 ** | 0.89 ** | 0.80 ** | −− | |
| 7. AAQ-II | 0.72 ** | 0.60 ** | 0.65 ** | 0.96 ** | 0.84 ** | 0.78 ** | −− |
| Variable | ∆R2 | R2 | F | p | Beta | t | p | 95% CI |
|---|---|---|---|---|---|---|---|---|
| Severity of FM | ||||||||
| (M1) DV = ICAF | 0.01 * | 0.74 | 170.21 | <0.001 | ||||
| FIQ | 0.18 | 3.57 | <0.001 | 0.28, 0.81 | ||||
| AAQ-II | 0.08 | 0.55 | 0.581 | −0.36, 0.20 | ||||
| Interaction | 0.004 | 2.68 | <0.001 | 0.001, 0.008 | ||||
| (M2) DV = ICAF | 0.007 * | 0.69 | 138.25 | <0.001 | ||||
| FIQ | 0.18 | 3.67 | <0.001 | 0.28, 0.81 | ||||
| Catastrophizing | 0.02 | 0.16 | 0.872 | −0.29, 0.25 | ||||
| Interaction | 0.004 | 2.13 | 0.034 | 0.003, 0.007 | ||||
| (M3) DV = ICAF | 0.019 * | 0.75 | 111.42 | <0.001 | ||||
| FIQ (1) | 0.13 | 2.59 | 0.012 | 0.03, 0.23 | ||||
| AAQ-II (2) | 0.08 | 0.46 | 0.642 | −0.44, 0.27 | ||||
| Catastrophizing (3) | 0.05 | 0.31 | 0.751 | −0.27, 0.38 | ||||
| Interaction 1 × 2 | 0.003 | 1.73 | 0.084 | −0.001, 0.008 | ||||
| Interaction 1 × 3 | 0.006 | 0.52 | 0.059 | −0.005, 0.018 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vallejo, M.A.; Vallejo-Slocker, L.; Offenbaecher, M.; Hirsch, J.K.; Toussaint, L.L.; Kohls, N.; Sirois, F.; Rivera, J. Psychological Flexibility Is Key for Reducing the Severity and Impact of Fibromyalgia. Int. J. Environ. Res. Public Health 2021, 18, 7300. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147300
Vallejo MA, Vallejo-Slocker L, Offenbaecher M, Hirsch JK, Toussaint LL, Kohls N, Sirois F, Rivera J. Psychological Flexibility Is Key for Reducing the Severity and Impact of Fibromyalgia. International Journal of Environmental Research and Public Health. 2021; 18(14):7300. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147300
Chicago/Turabian StyleVallejo, Miguel A., Laura Vallejo-Slocker, Martin Offenbaecher, Jameson K. Hirsch, Loren L. Toussaint, Niko Kohls, Fuschia Sirois, and Javier Rivera. 2021. "Psychological Flexibility Is Key for Reducing the Severity and Impact of Fibromyalgia" International Journal of Environmental Research and Public Health 18, no. 14: 7300. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147300