
Modelling Health in University Students: Are Young Women More Complicated Than Men?



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Tools of Measurement
2.2.1. Perceived Health
2.2.2. Psychological Distress (PD)
2.2.3. Sense of Coherence (SoC)
2.2.4. Health Locus of Control (HLoC)
2.2.5. Body Mass Index (BMI)
2.3. Data Collection
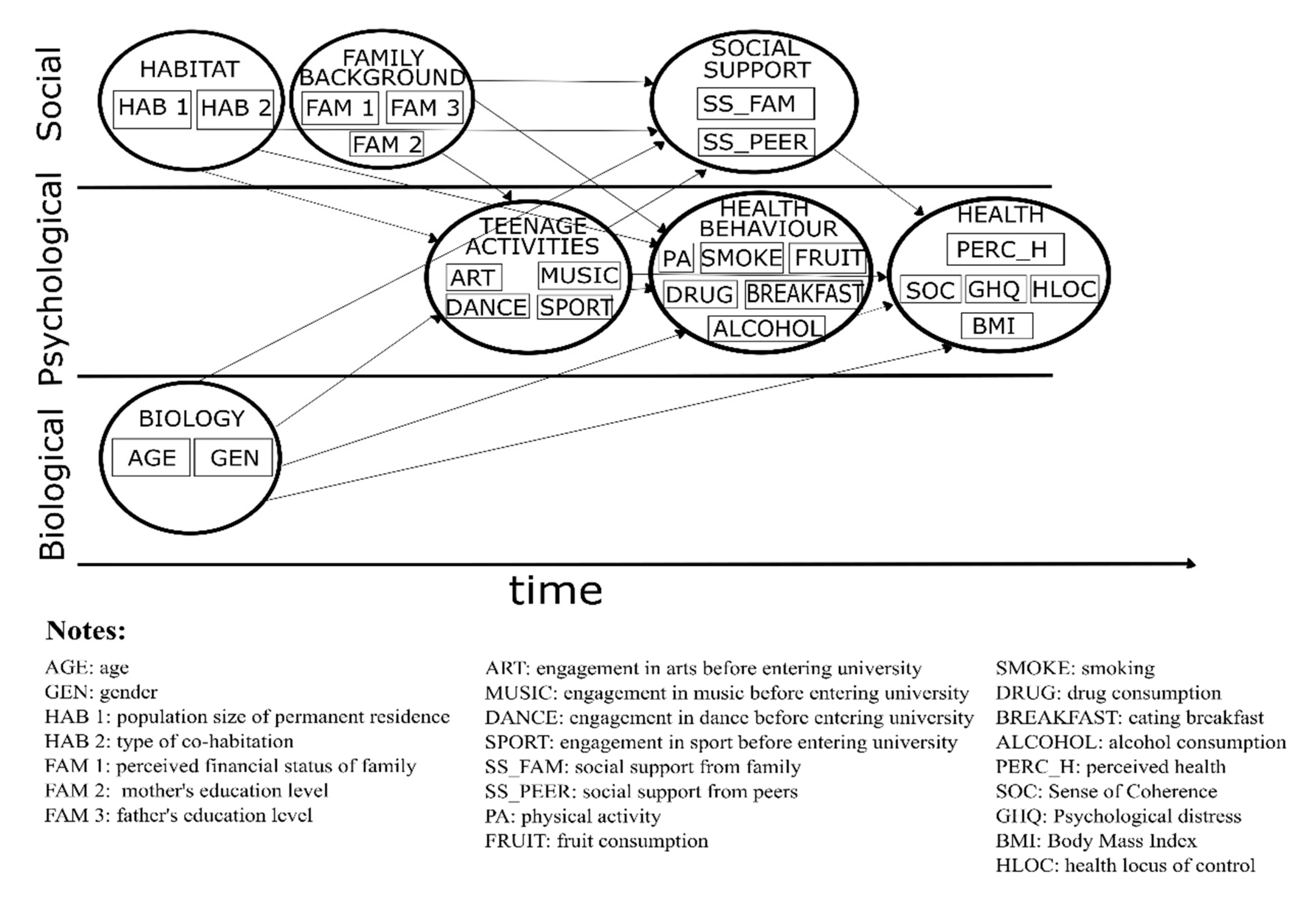
2.4. Construction of the Model
2.5. Multivariate Analysis of Covariance (MANCOVA)
3. Results
3.1. Variable Selection for Modelling “Health”
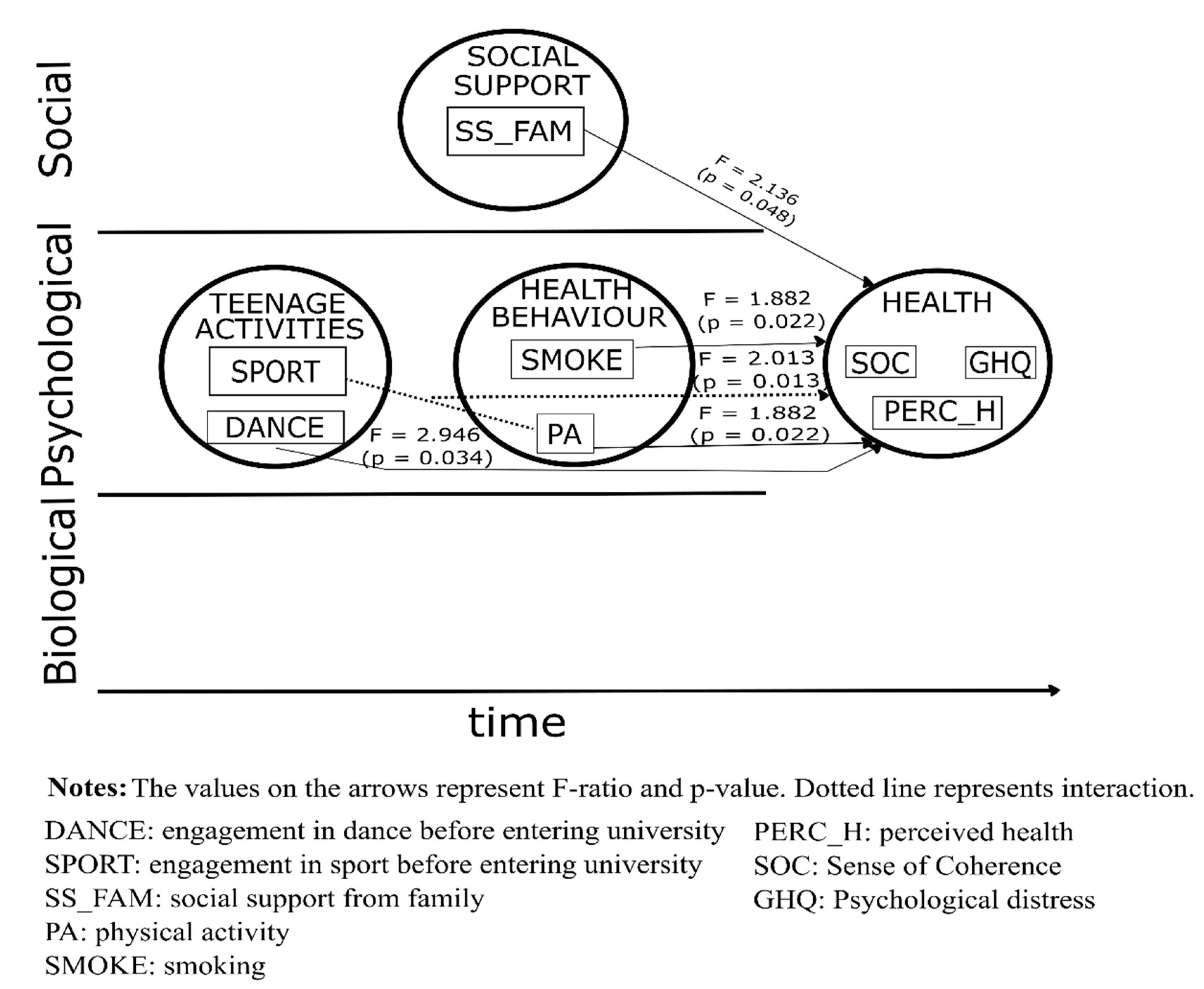
3.2. Result of MANCOVA for Men
3.3. Result of MANCOVA for Women
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Engel, G. The need for a new medical model: A challenge for biomedicine. Science 1977, 196, 129–136. [Google Scholar] [CrossRef]
- Borrell-Carrió, F.; Suchman, A.L.; Epstein, R.M. The biopsychosocial model 25 years later: Principles, practice, and scientific inquiry. Ann. Fam. Med. 2004, 2, 576–582. [Google Scholar] [CrossRef] [Green Version]
- McCollum, L.; Pincus, T. A biopsychosocial model to complement a biomedical model: Patient questionnaire data and socioeconomic status usually are more significant than laboratory tests and imaging studies in prognosis of rheumatoid arthritis. Rheum. Dis. Clin. N. Am. 2009, 35, 699–712. [Google Scholar] [CrossRef] [PubMed]
- Adler, R.H. Engel’s biopsychosocial model is still relevant today. J. Psychosom. Res. 2009, 67, 607–611. [Google Scholar] [CrossRef]
- Hatala, A.R. The status of the “biopsychosocial” model in health psychology: Towards an integrated approach and a critique of cultural conceptions. Open J. Med. Psychol. 2012, 1, 51–62. [Google Scholar] [CrossRef] [Green Version]
- Rodgers, R.F.; Paxton, S.J.; McLean, S.A. A biopsychosocial model of body image concerns and disordered eating in early adolescent girls. J. Youth Adolesc. 2014, 43, 814–823. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Towards a common language for functioning, disability and health: ICF. In The International Classification of Functioning, Disability and Health; World Health Organization: Geneva, Switzerland, 2002. [Google Scholar]
- Becker, S.P.; Langberg, J.M.; Byars, K.C. Advancing a biopsychosocial and contextual model of sleep in adolescence: A review and introduction to the special issue. J. Youth Adolesc. 2015, 44, 239–270. [Google Scholar] [CrossRef] [Green Version]
- Mitra, S.; Shakespeare, T. Remodeling the ICF. Disabil. Health J. 2019, 12, 337–339. [Google Scholar] [CrossRef]
- McDermott, S.; Turk, M.A. Support for reevaluation of the International Classification of functioning, disability, and health (ICF): A view from the US. Disabil. Health J. 2019, 12, 137–138. [Google Scholar] [CrossRef] [PubMed]
- Henningsen, P. Still modern? Developing the biopsychosocial model for the 21st century. J. Psychosom. Res. 2015, 79, 362–363. [Google Scholar] [CrossRef] [PubMed]
- Ghaemi, S.N. The rise and fall of the biopsychosocial model. Br. J. Psychiatry 2009, 195, 3–4. [Google Scholar] [CrossRef] [Green Version]
- Alvarez, A.S.; Pagani, M.; Meucci, P. The clinical application of the biopsychosocial model in mental health: A research critique. Am. J. Phys. Med. Rehabil. 2012, 91, S173–S180. [Google Scholar] [CrossRef]
- Ghaemi, S.N. The biopsychosocial model in psychiatry: A critique. Existenz 2011, 6, 1–8. [Google Scholar]
- McLaren, N. A critical review of the biopsychosocial model. Aust. N. Z. J. Psychiatry 1998, 32, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Pilgrim, D. The biopsychosocial model in Anglo-American psychiatry: Past, present and future? J. Ment. Health 2002, 11, 585–594. [Google Scholar] [CrossRef]
- Kuh, D.; Ben-Shlomo, Y.; Lynch, J.; Hallqvist, J.; Power, C. Life course epidemiology. J. Epidemiol. Community Health 2003, 57, 778–783. [Google Scholar] [CrossRef] [PubMed]
- Ben-Shlomo, Y.; Kuh, D. A life course approach to chronic disease epidemiology: Conceptual models, empirical challenges and interdisciplinary perspectives. Int. J. Epidemiol. 2002, 31, 285–293. [Google Scholar] [CrossRef]
- Balajti, I.; Daragó, L.; Ádány, R.; Kósa, K. College students’ response rate to an incentivized combination of postal and web-based health survey. Eval. Health Prof. 2010, 33, 164–176. [Google Scholar] [CrossRef]
- Országos Epidemiológiai Központ. Önkitöltős kérdőív Országos Lakossági Egészségfelmérés 2003; Self-Administered Questionnaire Hungarian National Health Interview Survey 2003; Országos Epidemiológiai Központ: Budapest, Hungary, 2003. [Google Scholar]
- De Bruin, A.; Picavet, H.S.J.; Nossikov, A. Health Interview Surveys: Towards International Harmonization of Methods and Instruments. WHO Regional Publications European; Series No. 58; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 1996. [Google Scholar]
- Goldberg, D.P.; Gater, R.; Sartorius, N.; Ustun, T.B.; Piccinelli, M.; Gureje, O.; Rutter, C. The validity of two versions of the GHQ in the WHO Study of Mental Illness in General Health Care. Psychol. Med. 1997, 27, 191–197. [Google Scholar] [CrossRef]
- Antonovsky, A. Unraveling the Mystery of Health; Jossey-Bass Publishers: San Francisco, CA, USA, 1987. [Google Scholar]
- Balajti, I.; Vokó, Z.; Ádány, R.; Kósa, K. A rövidített koherencia-érzés és az általános egészség (GHQ) kérdőívek magyar nyelvű változatának validálása (Validation of the Hungarian versions of the abbreviated sense of coherence (SoC) and the general health questionnaire (GHQ-12)). Mentálhig. Pszichoszomat 2007, 8, 147–161. [Google Scholar] [CrossRef] [Green Version]
- Bälter, K.A.; Bälter, O.; Fondell, E.; Lagerros, Y.T. Web-based and mailed questionnaires: A comparison of response rates and compliance. Epidemiology 2005, 16, 577–579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Field, A. Discovering Statistics Using SPSS; SAGE Publications Ltd.: London, UK, 2009. [Google Scholar]
- Vlassoff, C. Gender differences in determinants and consequences of health and illness. J. Health Popul. Nutr. 2007, 25, 47–61. [Google Scholar]
- Denton, M.; Prus, S.; Walters, V. Gender differences in health: A Canadian study of the psychosocial, structural and behavioural determinants of health. Soc. Sci. Med. 2004, 58, 2585–2600. [Google Scholar] [CrossRef] [Green Version]
- Commission on Social Determinants of Health. Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health; Final Report of the Commission on Social Determinants of Health; World Health Organization: Geneva, Switzerland, 2008; Available online: http://whqlibdoc.who.int/publications/2008/9789241563703_eng.pdf (accessed on 25 June 2021).
- Sustainable Development Goals. United Nations 2015. Available online: https://sdgs.un.org/goals/goal5 (accessed on 25 May 2021).
- World Health Organization. Why Using a Gender Approach Can Accelerate Noncommunicable Disease Prevention and Control in the WHO European Region; WHO Regional Office for Europe: Copenhagen, Denmark, 2019; Available online: https://www.euro.who.int/__data/assets/pdf_file/0003/399063/GenderApproachAndNCDsPreventionAndControl-eng.PDF (accessed on 25 June 2021).
- A Look into Masculine Identity in Mexican Young Men. Available online: http://editorial.upnvirtual.edu.mx/index.php/publicaciones/descargas/category/1-pdf?download=423:a-look-into-masculine-identity (accessed on 25 June 2021).
- García-Vega, E. Acerca del género y la salud. Pap. Psicól. 2011, 32, 282–288. [Google Scholar]
- Aznar, M.; Pilar, M. Género y salud. Suma Psicol 2008, 15, 75–94. [Google Scholar]
- Valls Llobet, C.; Banqué, M.; Fuentes, M.; Ojuel, J. Morbilidad diferencial entre mujeres y hombres. Anu. Psicol. 2008, 39, 9–22. [Google Scholar] [CrossRef] [Green Version]
- Mackenbach, J.P.; Simon, J.G.; Looman, C.W.; Joung, I.M. Self-assessed health and mortality: Could psychosocial factors explain the association? Int. J. Epidemiol. 2002, 31, 1162–1168. [Google Scholar] [CrossRef]
- Greenland, S. Principles of multilevel modelling. Int. J. Epidemiol. 2000, 29, 158–167. [Google Scholar] [CrossRef]
- Johnson, S.; Cooper, C.; Cartwright, S.; Donald, I.; Taylor, P.; Millet, C. The experience of work-related stress among occupations. J. Manag. Psychol. 2005, 20, 178–187. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.Y.; Goldstein, S.E. Loneliness, Stress, and Social Support in Young Adulthood: Does the Source of Support Matter? J. Youth Adolesc. 2016, 45, 568–580. [Google Scholar] [CrossRef]
- Lehrer, P.M.; Woolfolk, R.L. Principles and Practice of Stress Management, 3rd ed.; Sime, W.E., Ed.; The Guilford Press: New York, NY, USA, 2007. [Google Scholar]
- World Health Organization. 2008–2013 Action Plan for the Global Strategy for the Prevention and Control of Noncommunicable Diseases; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Stringhini, S.; Dugravot, A.; Shipley, M.; Goldberg, M.; Zins, M.; Kivimäki, M.; Marmot, M.; Sabia, S.; Singh-Manoux, A. Health behaviours, socioeconomic status, and mortality: Further analyses of the British Whitehall II and the French GAZEL prospective cohorts. PLoS Med. 2011, 8, e1000419. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, J.S.; Hernán, M.A. Epidemiologic methods are useless: They can only give you answers. Epidemiology 2012, 23, 785–786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, K.C.; Ehsani, J.P.; McQueen, D.V. Evidence based health promotion: Recollections, reflections, and reconsiderations. J. Epidemiol. Community Health 2003, 57, 841–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | Sense of Coherence 1 | Psychological Distress 2 | Perceived Health 3 | Overall Effect on the Multivariate Outcome | Partial Eta Squared 4 |
|---|---|---|---|---|---|
| F-ratios from the Tests of between Subject Effects | p-Value | According to Wilks’ Lambda | |||
| Intercept | 71.254 ** | 62.273 ** | 65.218 ** | <0.001 | 0.558 |
| Social support from peers at the university | 0.702 | 0.234 | 0.328 | 0.855 | 0.005 |
| Social support from family, friends | 3.528 * | 0.757 | 0.258 | 0.048 | 0.031 |
| Use of sedatives with prescription | 0.199 | 0.367 | 0.919 | 0.937 | 0.005 |
| Use of sedatives without prescription | 0.160 | 0.770 | 0.725 | 0.957 | 0.007 |
| Fruit consumption | 2.058 | 1.666 | 1.150 | 0.378 | 0.021 |
| Physical activity | 1.506 | 1.143 | 2.262 * | 0.022 | 0.052 |
| Smoking | 0.693 | 1.167 | 2.490 * | 0.022 | 0.052 |
| Arts | 0.000 | 1.843 | 2.258 | 0.306 | 0.015 |
| Dance | 1.615 | 2.079 | 8.679 ** | 0.034 | 0.035 |
| Sport | 0.317 | 0.442 | 0.034 | 0.724 | 0.005 |
| Age | 0.058 | 0.021 | 0.699 | 0.814 | 0.004 |
| Social support from peers × sport | 1.550 | 1.780 | 0.252 | 0.302 | 0.015 |
| Smoking × sport | 0.314 | 1.178 | 1.075 | 0.507 | 0.019 |
| Physical activity × sport | 1.492 | 2.625 * | 1.551 | 0.013 | 0.039 |
| Social support from family, friends × age | 2.024 | 0.845 | 0.193 | 0.341 | 0.014 |
| Variable | Sense of Coherence 1 | Psychological Distress 2 | Perceived Health 3 | Overall Effect on the Multivariate Outcome | Partial Eta Squared 4 |
|---|---|---|---|---|---|
| F-Ratios from the Tests of between Subject Effects | p-Value | According to Wilks’ Lambda | |||
| Intercept | 82.360 | 130.549 | 42.212 | <0.001 | 0.401 |
| Social support from peers at the university | 4.827 ** | 0.183 | 0.764 | 0.035 | 0.012 |
| Social support from family, friends | 1.626 | 6.084 ** | 2.011 | 0.021 | 0.013 |
| Use of sedatives with prescription | 1.294 | 0.999 | 2.791 * | 0.149 | 0.012 |
| Use of sedatives without prescription | 4.761 ** | 2.545 * | 3.085 * | 0.001 | 0.020 |
| Fruit consumption | 2.094 | 3.658 ** | 4.500 ** | 0.001 | 0.023 |
| Physical activity | 2.698 * | 1.887 | 1.831 | 0.084 | 0.014 |
| Smoking | 1.819 | 1.320 | 2.830 * | 0.018 | 0.017 |
| Arts | 1.295 | 1.432 | 0.101 | 0.565 | 0.004 |
| Dance | 0.074 | 7.438 ** | 0.078 | 0.024 | 0.017 |
| Sport | 0.078 | 0.882 | 2.119 | 0.364 | 0.006 |
| Age | 7.353 ** | 1.377 | 5.580 * | 0.014 | 0.019 |
| Social support from peers × sport | 0.529 | 4.288 * | 1.754 | 0.021 | 0.013 |
| Smoking × sport | 1.783 | 1.007 | 3.579 ** | 0.030 | 0.016 |
| Physical activity × sport | 2.211 | 1.289 | 0.405 | 0.378 | 0.010 |
| Social support from family, friends × age | 0.263 | 4.182 * | 1.241 | 0.135 | 0.009 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bíró, É.; Kovács, S.; Veres-Balajti, I.; Ádány, R.; Kósa, K. Modelling Health in University Students: Are Young Women More Complicated Than Men? Int. J. Environ. Res. Public Health 2021, 18, 7310. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147310
Bíró É, Kovács S, Veres-Balajti I, Ádány R, Kósa K. Modelling Health in University Students: Are Young Women More Complicated Than Men? International Journal of Environmental Research and Public Health. 2021; 18(14):7310. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147310
Chicago/Turabian StyleBíró, Éva, Sándor Kovács, Ilona Veres-Balajti, Róza Ádány, and Karolina Kósa. 2021. "Modelling Health in University Students: Are Young Women More Complicated Than Men?" International Journal of Environmental Research and Public Health 18, no. 14: 7310. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147310