
Iliotibial Band Autograft Provides the Fastest Recovery of Knee Extensor Mechanism Function in Pediatric Anterior Cruciate Ligament Reconstruction

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
3. Results
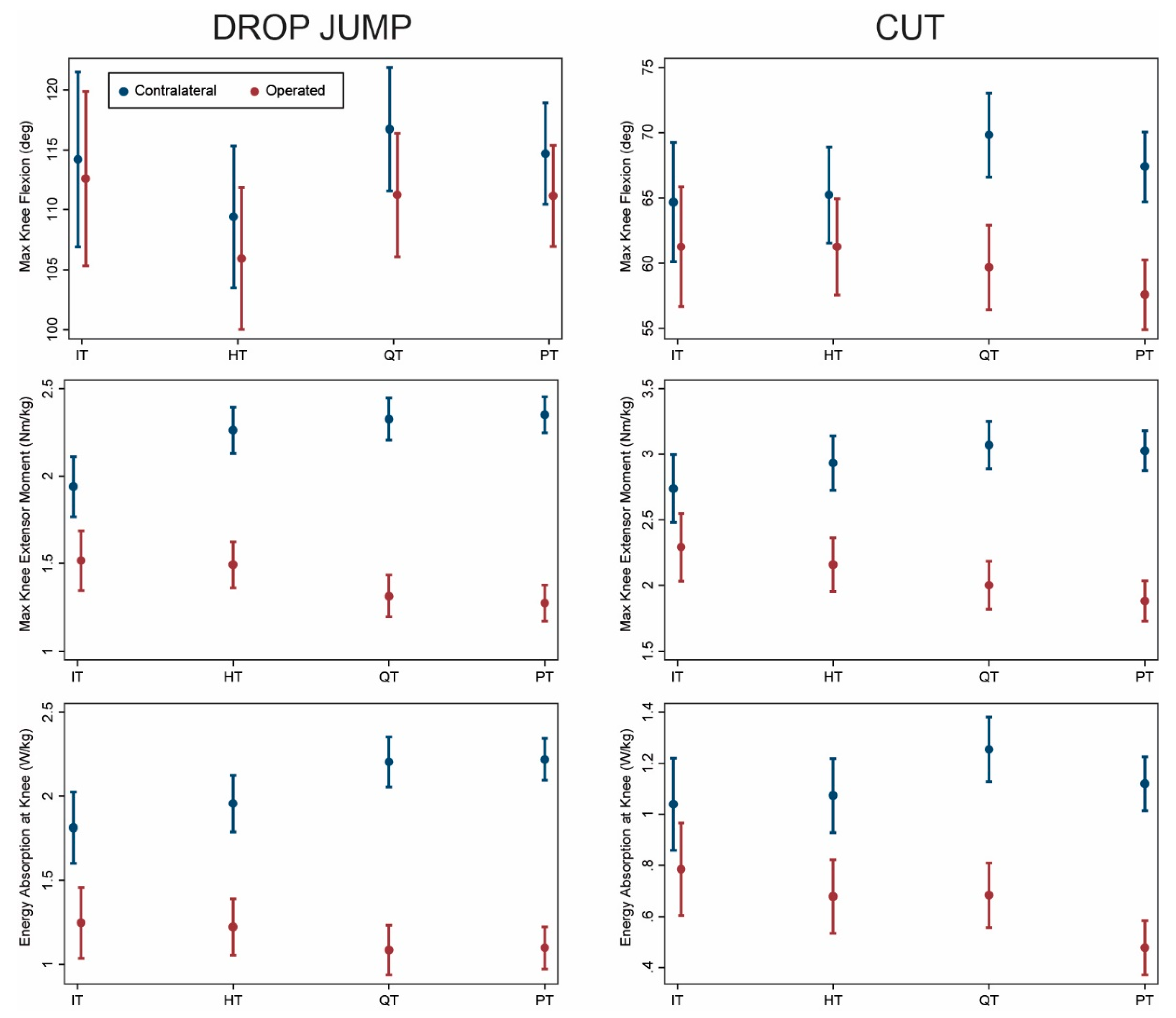
3.1. Isolated ACL Reconstruction
3.2. ACL Reconstruction with Meniscus Procedure
3.3. Younger Patients at Least 6 Months Post-Surgery
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drop Jump | Mean (SE) | p-Value | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Isolated ACLR | IT (n = 17 Visits) | HT (n = 25 Visits) | QT (n = 24 Visits) | PT (n = 47 Visits) | HT vs. IT | QT vs. IT | PT vs. IT | QT vs. HT | PT vs. HT | PT vs. QT |
| Max Knee Angle (°) | ||||||||||
| Non-op | 113 (5) | 110 (4) | 118 (4) | 113 (3) | 0.80 | 0.47 | 0.96 | 0.14 | 0.77 | 0.77 |
| Op | 112 (5) | 106 (4) | 112 (4) | 109 (3) | 0.56 | 0.95 | 0.71 | 0.33 | 0.82 | 0.42 |
| Asymmetry | −0.5 (2) | −3 (2) | −6 (2) | −4 (1) | 0.26 | 0.03 | 0.15 | 0.24 | 0.85 | 0.24 |
| Max Knee Moment (N·m/kg) | ||||||||||
| Non-op | 1.9 (0.1) | 2.2 (0.1) | 2.3 (0.1) | 2.5 (0.1) | 0.04 | 0.002 | <0.001 | 0.11 | 0.001 | 0.07 |
| Op | 1.5 (0.1) | 1.5 (0.1) | 1.3 (0.1) | 1.2 (0.1) | 0.61 | 0.20 | 0.21 | 0.01 | 0.008 | 0.92 |
| Asymmetry | −0.4 (0.1) | −0.6 (0.1) | −1.0 (0.1) | −1.2 (0.1) | 0.17 | <0.001 | <0.001 | 0.003 | <0.001 | 0.14 |
| Energy Absorption at Knee (J/kg) | ||||||||||
| Non-op | 1.7 (0.1) | 1.8 (0.1) | 2.3 (0.1) | 2.3 (0.1) | 0.61 | 0.01 | 0.03 | 0.004 | 0.003 | 0.95 |
| Op | 1.3 (0.1) | 1.3 (0.1) | 1.1 (0.1) | 1.0 (0.1) | 0.93 | 0.33 | 0.27 | 0.20 | 0.09 | 0.68 |
| Asymmetry | −0.4 (0.1) | −0.6 (0.1) | −1.2 (0.1) | −1.2 (0.1) | 0.46 | <0.001 | <0.001 | <0.001 | <0.001 | 0.72 |
| Cut | Mean (SE) | p-Value | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Isolated ACLR | IT (n = 17 Visits) | HT (n = 25 Visits) | QT (n = 24 Visits) | PT (n = 47 Visits) | HT vs. IT | QT vs. IT | PT vs. IT | QT vs. HT | PT vs. HT | PT vs. QT |
| Max Knee Angle (°) | ||||||||||
| Non-op | 63 (3) | 67 (2) | 70 (2) | 68 (2) | 0.21 | 0.07 | 0.33 | 0.41 | 0.84 | 0.27 |
| Op | 59 (3) | 64 (2) | 59 (2) | 57 (2) | 0.16 | 0.90 | 0.67 | 0.06 | 0.005 | 0.32 |
| Asymmetry | −4 (2) | −3 (2) | −11 (2) | −11 (1) | 0.81 | 0.005 | 0.003 | 0.001 | <0.001 | 0.89 |
| Max Knee Moment (N·m/kg) | ||||||||||
| Non-op | 2.6 (0.1) | 2.8 (0.1) | 3.2 (0.1) | 3.1 (0.1) | 0.27 | 0.003 | 0.02 | 0.006 | 0.03 | 0.51 |
| Op | 2.2 (0.1) | 2.3 (0.1) | 2.0 (0.1) | 1.8 (0.1) | 0.52 | 0.89 | 0.36 | 0.26 | 0.01 | 0.16 |
| Asymmetry | −0.4 (0.1) | −0.5 (0.1) | −1.2 (0.1) | −1.3 (0.1) | 0.55 | <0.001 | <0.001 | <0.001 | <0.001 | 0.43 |
| Energy Absorption at Knee (J/kg) | ||||||||||
| Non-op | 0.9 (0.1) | 1.0 (0.1) | 1.3 (0.1) | 1.2 (0.1) | 0.32 | 0.003 | 0.03 | 0.004 | 0.03 | 0.38 |
| Op | 0.7 (0.1) | 0.7 (0.1) | 0.7 (0.1) | 0.4 (0.1) | 0.39 | 0.51 | 0.35 | 0.78 | 0.006 | 0.009 |
| Asymmetry | −0.2 (0.1) | −0.3 (0.1) | −0.6 (0.1) | −0.8 (0.1) | 0.89 | 0.007 | <0.001 | 0.005 | <0.001 | 0.10 |
| Drop Jump | Mean (SE) | p-Value | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Concomitant Meniscus Procedure | IT (n = 7 Visits) | HT (n = 13 Visits) | QT (n = 24 Visits) | PT (n = 18 Visits) | HT vs. IT | QT vs. IT | PT vs. IT | QT vs. HT | PT vs. HT | PT vs. QT |
| Max Knee Angle (°) | ||||||||||
| Non-op | 118 (6) | 109 (5) | 113 (4) | 120 (4) | 0.23 | 0.56 | 0.87 | 0.43 | 0.25 | 0.54 |
| Op | 113 (6) | 107 (5) | 108 (4) | 116 (4) | 0.31 | 0.46 | 0.84 | 0.76 | 0.38 | 0.45 |
| Asymmetry | −4 (3) | −3 (3) | −6 (2) | −5 (2) | 0.71 | 0.71 | 0.90 | 0.33 | 0.52 | 0.74 |
| Max Knee Moment (N·m/kg) | ||||||||||
| Non-op | 2.1 (0.2) | 2.4 (0.1) | 2.4 (0.1) | 2.4 (0.1) | 0.40 | 0.56 | 0.94 | 0.73 | 0.36 | 0.46 |
| Op | 1.7 (0.2) | 1.4 (0.1) | 1.3 (0.1) | 1.4 (0.1) | 0.10 | 0.01 | 0.04 | 0.24 | 0.44 | 0.73 |
| Asymmetry | −0.5 (0.2) | −1.0 (0.2) | −1.2 (0.1) | −1.0 (0.1) | 0.06 | 0.01 | 0.06 | 0.54 | 0.91 | 0.42 |
| Energy Absorption at Knee (J/kg) | ||||||||||
| Non-op | 2.1 (0.2) | 2.1 (0.1) | 2.2 (0.1) | 2.4 (0.1) | 0.65 | 0.84 | 0.94 | 0.73 | 0.52 | 0.67 |
| Op | 1.3 (0.2) | 1.2 (0.1) | 1.1 (0.1) | 1.2 (0.1) | 0.39 | 0.13 | 0.33 | 0.32 | 0.74 | 0.51 |
| Asymmetry | −0.9 (0.2) | −0.9 (0.2) | −1.2 (0.1) | −1.1 (0.1) | 0.73 | 0.19 | 0.26 | 0.25 | 0.36 | 0.84 |
| Cut | Mean (SE) | p-Value | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Concomitant Meniscus Procedure | IT (n = 7 Visits) | HT (n = 13 Visits) | QT (n = 24 Visits) | PT (n = 18 Visits) | HT vs. IT | QT vs. IT | PT vs. IT | QT vs. HT | PT vs. HT | PT vs. QT |
| Max Knee Angle (°) | ||||||||||
| Non-op | 68 (4) | 64 (3) | 69 (3) | 66 (3) | 0.33 | 0.80 | 0.54 | 0.09 | 0.79 | 0.14 |
| Op | 65 (4) | 57 (3) | 59 (3) | 59 (3) | 0.09 | 0.37 | 0.21 | 0.32 | 0.87 | 0.39 |
| Asymmetry | −3 (4) | −7 (3) | −10 (2) | −7 (2) | 0.40 | 0.11 | 0.32 | 0.40 | 0.89 | 0.44 |
| Max Knee Moment (N·m/kg) | ||||||||||
| Non-op | 3.0 (0.2) | 3.2 (0.2) | 2.9 (0.1) | 3.2 (0.1) | 0.36 | 0.99 | 0.49 | 0.21 | 0.90 | 0.23 |
| Op | 2.4 (0.2) | 2.0 (0.2) | 1.9 (0.1) | 2.1 (0.1) | 0.13 | 0.10 | 0.37 | 0.84 | 0.57 | 0.36 |
| Asymmetry | −0.5 (0.3) | −1.3 (0.2) | −1.0 (0.2) | −1.1 (0.2) | 0.04 | 0.12 | 0.09 | 0.37 | 0.52 | 0.81 |
| Energy Absorption at Knee (J/kg) | ||||||||||
| Non-op | 1.3 (0.2) | 1.2 (0.1) | 1.1 (0.1) | 1.1 (0.1) | 0.70 | 0.53 | 0.37 | 0.72 | 0.42 | 0.54 |
| Op | 1.0 (0.2) | 0.6 (0.1) | 0.6 (0.1) | 0.6 (0.1) | 0.04 | 0.07 | 0.10 | 0.82 | 0.90 | 0.92 |
| Asymmetry | −0.3 (0.2) | −0.7 (0.1) | −0.5 (0.1) | −0.5 (0.1) | 0.10 | 0.18 | 0.36 | 0.57 | 0.32 | 0.60 |
| Drop Jump | Mean (SE) | p-Value | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Age < 16 yr and ≥6 Months Post-Surgery | IT (n = 16 Visits) | HT (n = 19 Visits) | QT (n = 22 Visits) | PT (n = 21 Visits) | HT vs. IT | QT vs. IT | PT vs. IT | QT vs. HT | PT vs. HT | PT vs. QT |
| Max Knee Angle (°) | ||||||||||
| Non-op | 118 (4) | 110 (4) | 117 (3) | 114 (4) | 0.94 | 0.33 | 0.52 | 0.11 | 0.25 | 0.76 |
| Op | 116 (4) | 107 (4) | 112 (3) | 109 (4) | 0.84 | 0.52 | 0.68 | 0.20 | 0.34 | 0.82 |
| Asymmetry | −2 (1) | −3 (1) | −5 (1) | −4 (1) | 0.59 | 0.18 | 0.26 | 0.40 | 0.55 | 0.81 |
| Max Knee Moment (N·m/kg) | ||||||||||
| Non-op | 1.9 (0.1) | 2.1 (0.1) | 2.3 (0.1) | 2.3 (0.1) | 0.10 | 0.001 | 0.003 | 0.04 | 0.03 | 0.79 |
| Op | 1.6 (0.1) | 1.5 (0.1) | 1.3 (0.1) | 1.3 (0.1) | 0.81 | 0.15 | 0.20 | 0.10 | 0.12 | 1.00 |
| Asymmetry | −0.3 (0.1) | −0.6 (0.1) | −1.0 (0.1) | −1.0 (0.1) | 0.08 | <0.001 | <0.001 | 0.006 | 0.003 | 0.84 |
| Energy Absorption at Knee (J/kg) | ||||||||||
| Non-op | 1.8 (0.1) | 1.8 (0.1) | 2.1 (0.1) | 2.1 (0.1) | 0.83 | 0.05 | 0.09 | 0.02 | 0.03 | 0.98 |
| Op | 1.4 (0.1) | 1.3 (0.1) | 1.1 (0.1) | 1.1 (0.1) | 0.74 | 0.33 | 0.40 | 0.38 | 0.42 | 0.99 |
| Asymmetry | −0.5 (0.1) | −0.6 (0.1) | −1.0 (0.1) | −1.0 (0.1) | 0.52 | 0.001 | 0.001 | 0.004 | 0.004 | 0.98 |
| Cut | Mean (SE) | p-Value | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Age <16 yr and ≥6 Months Post-Surgery | IT (n = 16 Visits) | HT (n = 19 Visits) | QT (n = 22 Visits) | PT (n = 21 Visits) | HT vs. IT | QT vs. IT | PT vs. IT | QT vs. HT | PT vs. HT | PT vs. QT |
| Max Knee Angle (°) | ||||||||||
| Non-op | 68 (3) | 66 (2) | 72 (2) | 67 (2) | 0.61 | 0.49 | 0.51 | 0.07 | 0.71 | 0.03 |
| Op | 65 (3) | 65 (2) | 62 (2) | 58 (2) | 0.74 | 0.29 | 0.08 | 0.29 | 0.02 | 0.16 |
| Asymmetry | −3 (2) | −2 (2) | −11 (2) | −8 (2) | 0.73 | 0.001 | 0.01 | <0.001 | 0.003 | 0.30 |
| Max Knee Moment (N·m/kg) | ||||||||||
| Non-op | 2.8 (0.1) | 2.8 (0.1) | 3.2 (0.1) | 2.9 (0.1) | 0.81 | 0.04 | 0.43 | 0.01 | 0.36 | 0.13 |
| Op | 2.4 (0.1) | 2.1 (0.1) | 2.0 (0.1) | 1.9 (0.1) | 0.34 | 0.17 | 0.14 | 0.56 | 0.33 | 0.65 |
| Asymmetry | −0.4 (0.1) | −0.7 (0.1) | −1.2 (0.1) | −1.0 (0.1) | 0.12 | <0.001 | 0.001 | 0.002 | 0.05 | 0.27 |
| Energy Absorption at Knee (J/kg) | ||||||||||
| Non-op | 1.1 (0.1) | 1.1 (0.1) | 1.5 (0.1) | 1.1 (0.1) | 0.44 | 0.22 | 0.42 | 0.004 | 0.85 | 0.003 |
| Op | 0.9 (0.1) | 0.7 (0.1) | 0.7 (0.1) | 0.5 (0.1) | 0.17 | 0.11 | 0.006 | 0.76 | 0.02 | 0.03 |
| Asymmetry | −0.2 (0.1) | −0.3 (0.1) | −0.7 (0.1) | −0.6 (0.1) | 0.46 | <0.001 | 0.004 | 0.003 | 0.03 | 0.42 |
References
- Shaw, L.; Finch, C.F. Trends in Pediatric and Adolescent Anterior Cruciate Ligament Injuries in Victoria, Australia 2005–2015. Int. J. Environ. Res. Public Health 2017, 14, 599. [Google Scholar] [CrossRef] [Green Version]
- Werner, B.C.; Yang, S.; Looney, A.M.; Gwathmey, F.W., Jr. Trends in Pediatric and Adolescent Anterior Cruciate Ligament Injury and Reconstruction. J. Pediatr. Orthop. 2016, 36, 447–452. [Google Scholar] [CrossRef]
- Ardern, C.L.; Ekas, G.; Grindem, H.; Moksnes, H.; Anderson, A.F.; Chotel, F.; Cohen, M.; Forssblad, M.; Ganley, T.J.; Feller, J.A.; et al. 2018 International Olympic Committee Consensus Statement on Prevention, Diagnosis, and Management of Pediatric Anterior Cruciate Ligament Injuries. Orthop. J. Sports Med. 2018, 6, 2325967118759953. [Google Scholar]
- Woo, S.L.; Wu, C.; Dede, O.; Vercillo, F.; Noorani, S. Biomechanics and anterior cruciate ligament reconstruction. J. Orthop. Surg. Res. 2006, 1, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Kaeding, C.C.; Aros, B.; Pedroza, A.; Pifel, E.; Amendola, A.; Andrish, J.T.; Dunn, W.R.; Marx, R.G.; McCarty, E.C.; Parker, R.D.; et al. Allograft Versus Autograft Anterior Cruciate Ligament Reconstruction: Predictors of Failure From a MOON Prospective Longitudinal Cohort. Sports Health 2011, 3, 73–81. [Google Scholar] [CrossRef] [Green Version]
- Joseph, S.M.; Huleatt, J.B.; Vogel-Abernathie, L.A.; Pace, J.L. Treatment of ACL Tears in the Skeletally Immature Patient. Sports Med. Arthrosc. Rev. 2018, 26, 153–156. [Google Scholar] [CrossRef] [PubMed]
- Milewski, M.D.; Beck, N.A.; Lawrence, J.T.; Ganley, T.J. Anterior cruciate ligament reconstruction in the young athlete: A treatment algorithm for the skeletally immature. Clin. Sports Med. 2011, 30, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Chicorell, A.M.; Nasreddine, A.Y.; Kocher, M.S. Physeal-sparing anterior cruciate ligament reconstruction with iliotibial band. Clin. Sports Med. 2011, 30, 767–777. [Google Scholar] [CrossRef] [PubMed]
- Kocher, M.S.; Garg, S.; Micheli, L.J. Physeal sparing reconstruction of the anterior cruciate ligament in skeletally immature prepubescent children and adolescents. J. Bone Jt. Surg. Am. 2005, 87, 2371–2379. [Google Scholar] [CrossRef]
- Kocher, M.S.; Heyworth, B.E.; Fabricant, P.D.; Tepolt, F.A.; Micheli, L.J. Outcomes of Physeal-Sparing ACL Reconstruction with Iliotibial Band Autograft in Skeletally Immature Prepubescent Children. J. Bone Jt. Surg. Am. 2018, 100, 1087–1094. [Google Scholar] [CrossRef]
- Micheli, L.J.; Metzl, J.D.; Di Canzio, J.; Zurakowski, D. Anterior cruciate ligament reconstructive surgery in adolescent soccer and basketball players. Clin. J. Sport Med. 1999, 9, 138–141. [Google Scholar] [CrossRef] [PubMed]
- Kocher, M.S.; Garg, S.; Micheli, L.J. Physeal sparing reconstruction of the anterior cruciate ligament in skeletally immature prepubescent children and adolescents. J. Bone Jt. Surg. Am. 2006, 88 (Suppl. 1), 283–293. [Google Scholar] [CrossRef]
- Kaeding, C.C.; Pedroza, A.D.; Reinke, E.K.; Huston, L.J.; Consortium, M.; Spindler, K.P. Risk Factors and Predictors of Subsequent ACL Injury in Either Knee After ACL Reconstruction: Prospective Analysis of 2488 Primary ACL Reconstructions From the MOON Cohort. Am. J. Sports Med. 2015, 43, 1583–1590. [Google Scholar] [CrossRef] [PubMed]
- Maletis, G.B.; Chen, J.; Inacio, M.C.; Funahashi, T.T. Age-Related Risk Factors for Revision Anterior Cruciate Ligament Reconstruction: A Cohort Study of 21,304 Patients From the Kaiser Permanente Anterior Cruciate Ligament Registry. Am. J. Sports Med. 2016, 44, 331–336. [Google Scholar] [CrossRef] [PubMed]
- Hewett, T.E. Prediction of Future Injury in Sport: Primary and Secondary Anterior Cruciate Ligament Injury Risk and Return to Sport as a Model. J. Orthop. Sports Phys. Ther. 2017, 47, 228–231. [Google Scholar] [CrossRef] [PubMed]
- Paterno, M.V.; Schmitt, L.C.; Ford, K.R.; Rauh, M.J.; Myer, G.D.; Huang, B.; Hewett, T.E. Biomechanical measures during landing and postural stability predict second anterior cruciate ligament injury after anterior cruciate ligament reconstruction and return to sport. Am. J. Sports Med. 2010, 38, 1968–1978. [Google Scholar]
- Leppanen, M.; Pasanen, K.; Krosshaug, T.; Kannus, P.; Vasankari, T.; Kujala, U.M.; Bahr, R.; Perttunen, J.; Parkkari, J. Sagittal Plane Hip, Knee, and Ankle Biomechanics and the Risk of Anterior Cruciate Ligament Injury: A Prospective Study. Orthop. J. Sports Med. 2017, 5, 2325967117745487. [Google Scholar] [CrossRef] [Green Version]
- Wren, T.A.L.; Mueske, N.M.; Brophy, C.H.; Pace, J.L.; Katzel, M.J.; Edison, B.R.; Vandenberg, C.D.; Zaslow, T.L. Hop Distance Symmetry Does Not Indicate Normal Landing Biomechanics in Adolescent Athletes With Recent Anterior Cruciate Ligament Reconstruction. J. Orthop. Sports Phys. Ther. 2018, 48, 622–629. [Google Scholar] [CrossRef] [PubMed]
- Ithurburn, M.P.; Altenburger, A.R.; Thomas, S.; Hewett, T.E.; Paterno, M.V.; Schmitt, L.C. Young athletes after ACL reconstruction with quadriceps strength asymmetry at the time of return-to-sport demonstrate decreased knee function 1 year later. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Gokeler, A.; Welling, W.; Benjaminse, A.; Lemmink, K.; Seil, R.; Zaffagnini, S. A critical analysis of limb symmetry indices of hop tests in athletes after anterior cruciate ligament reconstruction: A case control study. Orthop. Traumatol. Surg. Res. 2017, 103, 947–951. [Google Scholar] [CrossRef]
- Wellsandt, E.; Failla, M.J.; Snyder-Mackler, L. Limb Symmetry Indexes Can Overestimate Knee Function After Anterior Cruciate Ligament Injury. J. Orthop. Sports Phys. Ther. 2017, 47, 334–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hewett, T.E.; Ford, K.R.; Xu, Y.Y.; Khoury, J.; Myer, G.D. Utilization of ACL Injury Biomechanical and Neuromuscular Risk Profile Analysis to Determine the Effectiveness of Neuromuscular Training. Am. J. Sports Med. 2016, 44, 3146–3151. [Google Scholar] [CrossRef] [Green Version]
- Mueske, N.M.; VandenBerg, C.D.; Pace, J.L.; Katzel, M.J.; Zaslow, T.L.; Padilla, R.A.; Wren, T.A.L. Comparison of drop jump landing biomechanics and asymmetry among adolescents with hamstring, patellar and quadriceps tendon autografts for anterior cruciate ligament reconstruction. Knee 2018, 25, 1065–1073. [Google Scholar] [CrossRef] [PubMed]
- Wren, T.A.L.; O’Callahan, B.; Katzel, M.J.; Zaslow, T.L.; Edison, B.R.; VandenBerg, C.D.; Conrad-Forrest, A.; Mueske, N.M. Movement variability in pre-teen and teenage athletes performing sports related tasks. Gait Posture 2020, 80, 228–233. [Google Scholar] [CrossRef]
- Boden, B.P.; Dean, G.S.; Feagin, J.A., Jr.; Garrett, W.E., Jr. Mechanisms of anterior cruciate ligament injury. Orthopedics 2000, 23, 573–578. [Google Scholar] [CrossRef]
- Withrow, T.J.; Huston, L.J.; Wojtys, E.M.; Ashton-Miller, J.A. The effect of an impulsive knee valgus moment on in vitro relative ACL strain during a simulated jump landing. Clin. Biomech. (Bristol Avon) 2006, 21, 977–983. [Google Scholar] [CrossRef]
- Perkins, C.A.; Willimon, S.C. Pediatric Anterior Cruciate Ligament Reconstruction. Orthop. Clin. N. Am. 2020, 51, 55–63. [Google Scholar] [CrossRef]
- Bloom, D.A.; Wolfert, A.J.; Michalowitz, A.; Jazrawi, L.M.; Carter, C.W. ACL Injuries Aren’t Just for Girls: The Role of Age in Predicting Pediatric ACL Injury. Sports Health 2020, 12, 559–563. [Google Scholar] [CrossRef]




| IT (n = 20 Subjects) | HT (n = 29 Subjects) | QT (n = 39 Subjects) | PT (n = 57 Subjects) | p-Value | All (n = 145 Subjects) | |
|---|---|---|---|---|---|---|
| Sex | 0.03 | |||||
| Female | 5 (25%) | 13 (45%) | 23 (59%) | 35 (61%) | 876 (52%) | |
| Male | 15 (75%) | 16 (55%) | 16 (41%) | 22 (39%) | 69 (48%) | |
| Age at surgery (years) | 11.3 (1.6) | 14.5 (1.0) | 15.0 (1.4) | 16.4 (1.6) | <0.001 | 15.0 (2.2) |
| Height (cm) | 151.1 (13.3) | 169.2 (9.8) | 165.9 (9.2) | 166.9 (10.7) | <0.001 | 164.9 (11.9) |
| Body mass (kg) | 45.8 (12.2) | 74.0 (25.3) | 64.2 (14.2) | 69.1 (15.8) | <0.001 | 65.5 (19.2) |
| BMI (kg/m2) | 19.9 (4.5) | 25.4 (6.7) | 23.2 (3.5) | 24.7 (5.1) | 0.001 | 23.8 (5.3) |
| Meniscus procedure | 0.09 | |||||
| None | 14 (70%) | 18 (62%) | 22 (56%) | 41 (72%) | 95 (66%) | |
| Debridement | 0 | 0 | 2 (5%) | 2 (4%) | 4 (3%) | |
| Repair | 6 (30%) | 9 (31%) | 10 (26%) | 8 (14%) | 33 (23%) | |
| Menisectomy | 0 | 2 (7%) | 5 (13%) | 6 (11%) | 13 (9%) | |
| Sports | ||||||
| Baseball/Softball | 4 (20%) | 5 (17%) | 3 (8%) | 3 (5%) | 0.15 | 15 (10%) |
| Basketball | 9 (45%) | 6 (21%) | 11 (28%) | 15 (26%) | 0.30 | 41 (28%) |
| Dance/Cheer/Gymnastics | 1 (5%) | 2 (7%) | 3 (8%) | 5 (9%) | 0.96 | 11 (8%) |
| Football | 7 (35%) | 8 (28%) | 7 (18%) | 7 (12%) | 0.11 | 29 (20%) |
| Soccer | 8 (40%) | 10 (34%) | 16 (41%) | 22 (39%) | 0.96 | 56 (39%) |
| Track/Cross-country | 0 | 0 | 4 (13%) | 9 (16%) | 0.04 | 13 (10%) |
| Volleyball | 2 (10%) | 5 (17%) | 4 (10%) | 6 (11%) | 0.79 | 17 (12%) |
| Other | 8 (40%) | 6 (21%) | 10 (26%) | 11 (19%) | 0.30 | 35 (24%) |
| Time playing each sport (h/week) | 5.8 (3.1) | 9.7 (6.1) | 8.5 (4.3) | 10.6 (7.1) | <0.001 | 9.1 (6.0) |
| n = 24 visits | n = 38 visits | n = 48 visits | n = 65 visits | n = 175 visits | ||
| Time post-surgery (months) | 7.8 (3.4) | 7.0 (3.0) | 6.8 (2.2) | 7.9 (2.5) | 0.09 | 7.4 (2.7) |
| Drop Jump | Mean (SE) | p-Value | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| All Subjects | IT (n = 24 Visits) | HT (n = 38 Visits) | QT (n = 48 Visits) | PT (n = 65 Visits) | HT vs. IT | QT vs. IT | PT vs. IT | QT vs. HT | PT vs. HT | PT vs. QT |
| Max Knee Angle (°) | ||||||||||
| Non-op | 114 (4) | 109 (3) | 116 (3) | 115 (2) | 0.39 | 0.81 | 0.79 | 0.11 | 0.47 | 0.36 |
| Op | 113 (4) | 106 (3) | 110 (3) | 111 (2) | 0.27 | 0.66 | 0.54 | 0.35 | 0.60 | 0.67 |
| Asymmetry | −2 (2) | −3 (1) | −6 (1) | −4 (1) | 0.48 | 0.04 | 0.22 | 0.13 | 0.60 | 0.24 |
| Max Knee Moment (N·m/kg) | ||||||||||
| Non-op | 2.0 (0.1) | 2.3 (0.1) | 2.4 (0.1) | 2.4 (0.05) | 0.06 | 0.006 | 0.004 | 0.21 | 0.08 | 0.57 |
| Op | 1.5 (0.1) | 1.5 (0.1) | 1.3 (0.1) | 1.3 (0.05) | 0.33 | 0.004 | 0.005 | 0.007 | 0.004 | 0.83 |
| Asymmetry | −0.4 (0.1) | −0.8 (0.1) | −1.1 (0.1) | −1.2 (0.1) | 0.02 | <0.001 | <0.001 | 0.005 | <0.001 | 0.56 |
| Energy Absorption at Knee (J/kg) | ||||||||||
| Non-op | 1.8 (0.1) | 1.9 (0.1) | 2.2 (0.1) | 2.3 (0.1) | 0.92 | 0.04 | 0.07 | 0.005 | 0.007 | 1.00 |
| Op | 1.3 (0.1) | 1.2 (0.1) | 1.1 (0.1) | 1.1 (0.1) | 0.43 | 0.06 | 0.07 | 0.11 | 0.07 | 0.78 |
| Asymmetry | −0.6 (0.1) | −0.7 (0.1) | −1.2 (0.1) | −1.2 (0.1) | 0.35 | <0.001 | <0.001 | <0.001 | <0.001 | 0.79 |
| Cut | Mean (SE) | p-Value | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| All Subjects | IT (n = 24 Visits) | HT (n = 38 Visits) | QT (n = 48 Visits) | PT (n = 65 Visits) | HT vs. IT | QT vs. IT | PT vs. IT | QT vs. HT | PT vs. HT | PT vs. QT |
| Max Knee Angle (°) | ||||||||||
| Non-op | 65 (2) | 65 (2) | 70 (2) | 67 (1) | 0.78 | 0.17 | 0.89 | 0.10 | 0.88 | 0.05 |
| Op | 61 (2) | 61 (2) | 59 (2) | 57 (1) | 0.99 | 0.54 | 0.14 | 0.36 | 0.02 | 0.09 |
| Asymmetry | −3 (2) | −4 (2) | −11 (1) | −10 (1) | 0.71 | 0.002 | 0.003 | 0.002 | 0.002 | 0.74 |
| Max Knee Moment (N·m/kg) | ||||||||||
| Non-op | 2.7 (0.1) | 2.9 (0.1) | 3.1 (0.1) | 3.1 (0.1) | 0.18 | 0.03 | 0.03 | 0.17 | 0.13 | 0.83 |
| Op | 2.3 (0.1) | 2.2 (0.1) | 2.0 (0.1) | 1.9 (0.1) | 0.64 | 0.22 | 0.12 | 0.27 | 0.08 | 0.42 |
| Asymmetry | −0.4 (0.1) | −0.8 (0.1) | −1.1 (0.1) | −1.2 (0.1) | 0.05 | <0.001 | <0.001 | 0.02 | 0.001 | 0.32 |
| Energy Absorption at Knee (J/kg) | ||||||||||
| Non-op | 1.0 (0.1) | 1.1 (0.1) | 1.2 (0.1) | 1.2 (0.1) | 0.71 | 0.11 | 0.38 | 0.08 | 0.40 | 0.32 |
| Op | 0.8 (0.1) | 0.7 (0.1) | 0.7 (0.1) | 0.5 (0.1) | 0.48 | 0.39 | 0.03 | 0.82 | 0.02 | 0.01 |
| Asymmetry | −0.2 (0.1) | −0.4 (0.1) | −0.6 (0.1) | −0.7 (0.1) | 0.25 | 0.005 | <0.001 | 0.07 | 0.001 | 0.16 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wren, T.L.; Beltran, V.; Katzel, M.J.; Conrad-Forrest, A.S.; VandenBerg, C.D. Iliotibial Band Autograft Provides the Fastest Recovery of Knee Extensor Mechanism Function in Pediatric Anterior Cruciate Ligament Reconstruction. Int. J. Environ. Res. Public Health 2021, 18, 7492. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147492
Wren TL, Beltran V, Katzel MJ, Conrad-Forrest AS, VandenBerg CD. Iliotibial Band Autograft Provides the Fastest Recovery of Knee Extensor Mechanism Function in Pediatric Anterior Cruciate Ligament Reconstruction. International Journal of Environmental Research and Public Health. 2021; 18(14):7492. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147492
Chicago/Turabian StyleWren, Tishya L., Veronica Beltran, Mia J. Katzel, Adriana S. Conrad-Forrest, and Curtis D. VandenBerg. 2021. "Iliotibial Band Autograft Provides the Fastest Recovery of Knee Extensor Mechanism Function in Pediatric Anterior Cruciate Ligament Reconstruction" International Journal of Environmental Research and Public Health 18, no. 14: 7492. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147492