
Home Smoking Bans and Urinary NNAL Levels to Measure Tobacco Smoke Exposure in Chinese American Household Pairs

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Tobacco-Specific Nitrosamine Biomarker of Tobacco Smoke Exposure
2.2. Home Smoking Ban Categories for Household Pairs
2.3. Covariates
2.4. Statistical Analysis
3. Results
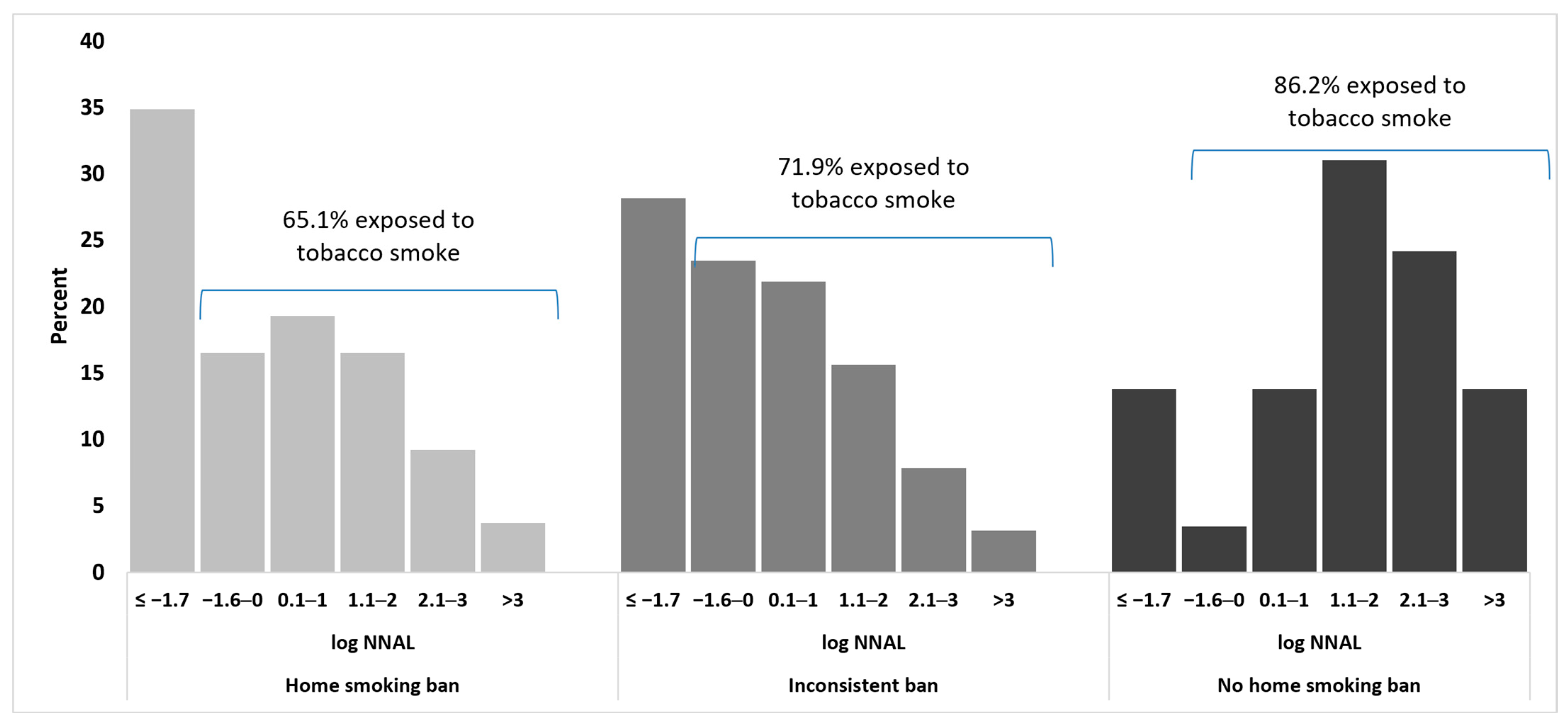
3.1. Nonsmoker Exposure to Secondhand Smoke
3.2. Multivariate Analysis
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Trial Registration
References
- Hennessy, M.; Bleakley, A.; Mallya, G.; Romer, D. The effect of household smoking bans on household smoking. Am. J. Public Health 2014, 104, 721–727. [Google Scholar] [CrossRef]
- Rumchev, K.; Jamrozik, K.; Stick, S.; Spickett, J. How free of tobacco smoke are ‘smoke-free’ homes? Indoor Air 2008, 18, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Johansson, A.; Hermansson, G.; Ludvigsson, J. How should parents protect their children from environmental tobacco-smoke exposure in the home? Pediatrics 2004, 113, e291–e295. [Google Scholar] [CrossRef] [Green Version]
- U.S. Department of Health and Human Services. The Health Consequences of Involuntary Exposure to Tobacco Smoke: A Report of the Surgeon General; U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, Coordinating Center for Health Promotion, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health: Atlanta, GA, USA, 2006.
- Strulovici-Barel, Y.; Omberg, L.; O’Mahony, M.; Gordon, C.; Hollmann, C.; Tilley, A.E.; Salit, J.; Mezey, J.; Harvey, B.-G.; Crystal, R.G. Threshold of biologic responses of the small airway epithelium to low levels of tobacco smoke. Am. J. Respir. Crit. Care Med. 2010, 182, 1524–1532. [Google Scholar] [CrossRef] [PubMed]
- Willis, G.; Hartman, A.; Reyes-Guzman, C.; Seaman, E.L.; Gibson, J.T.; Goettsche, E.; Chomenko, D.; Mangold, K.; Bloch, M. The 2014–2015 Tobacco Use Supplement to the Current Population Survey. U.S. Department of Health and Human Services, National Cancer Institute, Tobacco Control Research Branch. November 2017. Available online: https://cancercontrol.cancer.gov/brp/tcrb/tus-cps/TUS-CPS_2014-15_SummaryDocument.pdf (accessed on 9 August 2019).
- Avila-Tang, E.; Elf, J.L.; Cummings, K.M.; Fong, G.T.; Hovell, M.F.; Klein, J.D.; McMillen, R.; Winickoff, J.P.; Samet, J.M. Assessing secondhand smoke exposure with reported measures. Tob. Control 2013, 22, 156–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wakefield, M.; Banham, D.; Ruffin, R.; McCaul, K.; Badcock, N. Restrictions on smoking at home and urinary cotinine levels among children with asthma. Am. J. Prev. Med. 2000, 19, 188–192. [Google Scholar] [CrossRef]
- Spencer, N.; Blackburn, C.; Bonas, S.; Coe, C.; Dolan, A. Parent reported home smoking bans and toddler (18–30 month) smoke exposure: A cross-sectional survey. Arch. Dis. Child 2005, 90, 670–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Protano, C.; Andreoli, R.; Manini, P.; Vitali, M. How home-smoking habits affect children: A cross-sectional study using urinary cotinine measurements in Italy. Int. J. Public Health 2012, 57, 885–892. [Google Scholar] [CrossRef]
- Fallavollita, W.L.; Do, E.K.; Schechter, J.C.; Kollins, S.H.; Zheng, J.; Qin, J.; Maguire, R.L.; Hoyo, C.; Murphy, S.K.; Fuemmeler, B.F. Smoke-free home rules and association with child secondhand smoke exposure among mother-child dyad relationships. Int. J. Environ. Res. Public Health 2021, 18, 5256. [Google Scholar] [CrossRef]
- Zhang, X.; Martinez-Donate, A.P.; Kuo, D.; Jones, N.R. “How is smoking handled in your home?”: Agreement between parental reports on home smoking bans in the United States, 1995–2007. Nicotine Tob. Res. 2012, 14, 1170–1179. [Google Scholar] [CrossRef] [Green Version]
- Shelley, D.; Nguyen, N.; Yerneni, R.; Fahs, M. Tobacco use behaviors and household smoking bans among Chinese Americans. Am. J. Health Promot. 2008, 22, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Shelley, D.; Fahs, M.C.; Yerneni, R.; Qu, J.; Burton, D. Correlates of household smoking bans among Chinese Americans. Nicotine Tob. Res. 2006, 8, 103–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, D.; Wahlgren, D.R.; Liles, S.; Matt, G.; Oliver, M.; Jones, J.A.; Hovell, M.F. A second reporter matters: Agreement between parents’ and children’s reports of smoking bans in families. Am. J. Prev. Med. 2011, 40, 572–575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tong, E.K.; Tang, H.; Tsoh, J.; Wong, C.; Chen, M.S. Smoke-free policies among Asian-American women: Comparisons by education status. Am. J. Prev. Med. 2009, 37 (Suppl. 2), S144–S150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tong, E.K.; Saw, A.; Fung, L.; Li, C.; Liu, Y.; Tsoh, J.Y. Impact of a smoke-free-living educational intervention for smokers and household nonsmokers: A randomized trial of Chinese American pairs. Cancer 2018, 124 (Suppl. 7), 1590–1598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goniewicz, M.L.; Havel, C.M.; Peng, M.W.; Jacob, P.; Dempsey, D.; Yu, L.; Zielińska-Danch, W.; Koszowski, B.; Czogala, J.; Sobczak, A.; et al. Elimination kinetics of the tobacco-specific biomarker and lung carcinogen 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanol. Cancer Epidemiol. Biomark. Prev. 2009, 18, 3421–3425. [Google Scholar] [CrossRef] [Green Version]
- Benowitz, N.L. Cotinine as a biomarker of environmental tobacco smoke exposure. Epidemiol. Rev. 1996, 18, 188–204. [Google Scholar] [CrossRef] [Green Version]
- Goniewicz, M.L.; Eisner, M.D.; Lazcano-Ponce, E.; Zielinska-Danch, W.; Koszowski, B.; Sobczak, A.; Havel, C.; Jacob, P.; Benowitz, N.L. Comparison of urine cotinine and the tobacco-specific nitrosamine metabolite 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanol (NNAL) and their ratio to discriminate active from passive smoking. Nicotine Tob. Res. 2011, 13, 202–208. [Google Scholar] [CrossRef] [Green Version]
- Benowitz, N.L.; Bernert, J.T.; Caraballo, R.S.; Holiday, D.B.; Wang, J. Optimal serum cotinine levels for distinguishing cigarette smokers and nonsmokers within different racial/ethnic groups in the United States between 1999 and 2004. Am. J. Epidemiol. 2009, 169, 236–248. [Google Scholar] [CrossRef] [Green Version]
- Jacob, P.; Havel, C.; Lee, D.H.; Yu, L.; Eisner, M.D.; Benowitz, N.L. Subpicogram per milliliter determination of the tobacco-specific carcinogen metabolite 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanol in human urine using liquid chromatography-tandem mass spectrometry. Anal. Chem. 2008, 80, 8115–8121. [Google Scholar] [CrossRef] [Green Version]
- National Health and Nutrition Examination Survey. 2011–2012 Data Documentation, Codebook, and Frequencies: Cotinine—Serum & Total NNAL—Urine (COTNAL_G). Available online: https://wwwn.cdc.gov/Nchs/Nhanes/2011-2012/COTNAL_G.htm (accessed on 9 August 2019).
- Ockene, J.K.; Emmons, K.M.; Mermelstein, R.J.; Perkins, K.A.; Bonollo, D.S.; Voorhees, C.C.; Hollis, J.F. Relapse and maintenance issues for smoking cessation. Health Psychol. 2000, 19, 17–31. [Google Scholar] [CrossRef] [PubMed]
- King, B.A.; Travers, M.J.; Cummings, K.M.; Mahoney, M.C.; Hyland, A.J. Secondhand smoke transfer in multiunit housing. Nicotine Tob. Res. 2010, 12, 1133–1141. [Google Scholar] [CrossRef] [PubMed]
- Saw, A.; Tang, H.; Tsoh, J.Y.; Chen, M.S., Jr.; Tong, E.K. Non-smoker assertive behaviour against smoke exposure: Chinese and Korean American non-smokers. Drug Alcohol Rev. 2017, 36, 779–787. [Google Scholar] [CrossRef] [PubMed]
- Tong, E.K.; Nguyen, T.T.; Vittinghoff, E.; Pérez-Stable, E.J. Smoking behaviors among immigrant Asian Americans: Rules for smoke-free homes. Am. J. Prev. Med. 2008, 35, 64–67. [Google Scholar] [CrossRef] [Green Version]
- Bernert, J.T.; Pirkle, J.L.; Xia, Y.; Jain, R.B.; Ashley, D.L.; Sampson, E.J. Urine concentrations of a tobacco-specific nitrosamine carcinogen in the U.S. population from secondhand smoke exposure. Cancer Epidemiol. Biomark. Prev. 2010, 19, 2969–2977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vuong, T.D.; Zhang, X.; Roeseler, A. California Tobacco Facts and Figures 2019; California Department of Public Health: Sacramento, CA, USA, 2019.
- Department of Public Health, City and County of San Francisco. San Francisco Health Code, Article 19F: Smoke Free Ordinance General Requirements; San Francisco Department of Public Health: San Francisco, CA, USA, 2013.
- Saw, A.; Paterniti, D.; Fung, L.C.; Tsoh, J.; Chen, M.S.; Tong, E.K. Social Environmental Influences on Smoking and Cessation: Qualitative Perspectives Among Chinese-Speaking Smokers and Nonsmokers in California. J. Immigr. Minority Health 2017, 19, 1404–1411. [Google Scholar] [CrossRef]
- Saw, A.; Paterniti, D.A.; Fung, L.C.; Tsoh, J.Y.; Tong, E.K. Perspectives of Chinese American smoker and nonsmoker household pairs about the creating smokefree living together program. Cancer 2018, 124 (Suppl. 7), 1599–1606. [Google Scholar] [CrossRef] [Green Version]
- Zhao, J.; Li, X.; Stewart, S.L.; Gao, W.; Qi, F.; Zhang, L.; Pang, Z.; Qiao, Q.; Ning, F.; Tong, E. Cigarette Smoking and Secondhand Smoke Exposure Before and After a Tobacco-Free Olympic Policy Period: Qingdao, China. Nicotine Tob. Res. 2019, 21, 1531–1538. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Characteristics | Total | Home Smoking Ban Category | |||
|---|---|---|---|---|---|
| Ban | Inconsistent | No Ban | p-Value | ||
| Participant pairs, n (%) | 202 | 109 (53.9%) | 64 (31.7%) | 29 (14.4%) | |
| Household pairs | |||||
| Married, n (%) | 173 (85.6%) | 98 (89.9%) | 49 (76.6%) | 26 (89.7%) | 0.05 |
| Years pairs lived together, mean (std) | 20.4 (14.5) | 18.3 (14.1) | 21.8 (13.9) | 25.1 (16.2) | 0.06 |
| Children in household (n = 143), n (%) | 109 (76.2%) | 60 (73.2%) | 33 (82.5%) | 16 (76.2%) | 0.58 |
| Other smoker (besides partner) in the house, n (%) | 28 (14.1%) | 9 (8.4%) | 13 (20.6%) | 6 (20.7%) | 0.04 |
| Nonsmoker | |||||
| Age, mean (std) | 49.5 (13.0) | 48.8 (12.7) | 49.2 (13.7) | 52.8 (12.6) | 0.34 |
| Less than high school education, n (%) | 64 (31.8%) | 34 (31.5%) | 17 (26.6%) | 13 (44.8%) | 0.21 |
| Years lived in the U.S., mean (std) | 8.9 (8.0) | 7.8 (7.2) | 10.0 (7.9) | 10.7 (10.3) | 0.10 |
| Low English fluency: “not too well/not at all”, n (%) | 143 (71.1%) | 68 (63.0%) | 50 (78.1%) | 25 (86.2%) | 0.02 |
| Knowledge, n (%) | |||||
| Tobacco smoke exposure harms: 4 health conditions | 95 (47.3%) | 54 (50.0%) | 32 (50.0%) | 9 (31.0%) | 0.57 |
| Ventilation does not eliminate exposure | 76 (37.8%) | 40 (37.0%) | 24 (37.5%) | 12 (41.4%) | 0.91 |
| Attitudes, n (%) | |||||
| Smoke is harmful to smoker | 179(89.5%) | 99 (92.5%) | 55 (85.9%) | 25 (86.2%) | 0.28 |
| Smoke is harmful to nonsmoker | 160 (80.0%) | 88 (82.2%) | 49 (76.6%) | 23 (79.3%) | 0.66 |
| Confident to keep a smoke-free home | 149 (74.5%) | 87 (81.3%) | 45 (70.3%) | 17 (58.6%) | 0.03 |
| Smoker | |||||
| Age, mean (std) | 53.2 (14.3) | 52.5 (14.2) | 52.7 (14.4) | 57.2 (14.5) | 0.28 |
| Less than high school education, n (%) | 65 (32.3%) | 37 (33.9%) | 18 (28.6%) | 10 (34.5%) | 0.74 |
| Years lived in the U.S., mean (std) | 10.8 (9.6) | 10.0 (9.6) | 11.7 (9.0) | 12.0 (10.6) | 0.42 |
| Low English fluency: “not too well/not at all”, n (%) | 153 (76.1%) | 79 (72.5%) | 51 (81.0%) | 23 (79.3%) | 0.41 |
| Knowledge, n (%) | |||||
| Tobacco smoke exposure harms: 4 health conditions | 117 (58.2%) | 71 (65.1%) | 33 (52.4%) | 13 (44.8%) | 0.20 |
| Ventilation does not eliminate exposure | 64 (32.3%) | 41 (37.6%) | 13 (21.3%) | 10 (35.7%) | 0.09 |
| Attitudes, n (%) | |||||
| Smoke is harmful to smoker | 153 (76.1%) | 81 (74.3%) | 52 (82.5%) | 20 (69.0%) | 0.30 |
| Smoke is harmful to nonsmoker | 141 (70.2%) | 75 (68.8%) | 46 (73.0%) | 20 (69.0%) | 0.84 |
| Confident to keep a smoke-free home | 170 (84.6%) | 96 (88.1%) | 53 (84.1%) | 21 (72.4%) | 0.12 |
| Non-smoker helpful in quitting | 144 (72.4%) | 81 (75.0%) | 44 (69.8%) | 19 (67.9%) | 0.65 |
| Tobacco behavior, n (%) | |||||
| Quit attempt in past year | 108 (53.5%) | 64 (58.7%) | 33 (51.6%) | 11 (37.9%) | 0.13 |
| Plan to quit in the next 30 days | 56 (28.0%) | 35 (32.1%) | 14 (21.9%) | 7 (25.9%) | 0.25 |
| Cigarettes smoked per day, mean (std) | 10.2 (6.6) | 10.1 (6.3) | 8.9 (5.2) | 13.5 (8.9) | 0.01 |
| NNAL, geometric mean in pg/mg, (std) | 47.3 (7.1) | 46.3 (7.3) | 41.5 (6.7) | 67.5 (7.5) | 0.54 |
| Setting | Home Smoking Ban Category | |||||
|---|---|---|---|---|---|---|
| Ban (n = 72) | Inconsistent Ban (n = 46) | No Ban (n = 25) | ||||
| n | Percent | n | Percent | n | Percent | |
| Home | 17 | 23.6% | 14 | 30.4% | 14 | 56.0% |
| Car | 9 | 12.5% | 7 | 15.2% | 2 | 8.0% |
| Work | 11 | 15.3% | 4 | 8.7% | 7 | 28.0% |
| Outdoors | 53 | 73.6% | 35 | 76.1% | 9 | 36.0% |
| Restaurant or bar | 10 | 13.9% | 8 | 17.4% | 6 | 24.0% |
| Other | 13 | 18.1% | 8 | 17.4% | 5 | 20.0% |
| Home Smoking Ban Category and Covariates | Geometric Mean (95% CI) (pg/mg) | Unadjusted Ratio of Geometric Means (95% CI) | p-Value | Model 1 Adjusted Ratio of Geometric Means (95% CI) | p-Value | Model 2 Adjusted Ratio of Geometric Means (95% CI) | p-Value |
|---|---|---|---|---|---|---|---|
| Total | 1.24 (0.98, 1.56) | ||||||
| Home smoking ban | |||||||
| Ban | 0.97 (0.71, 1.33) | Reference | Reference | Reference | |||
| Inconsistent | 1.06 (0.73, 1.54) | 1.09 (0.66, 1.81) | 0.73 | 0.82 (0.43, 1.55) | 0.54 | 0.96 (0.52, 1.77) | 0.90 |
| No ban | 4.23 (2.18, 8.22) | 4.35 (2.23, 8.50) | < 0.001 | 2.61 (1.11, 6.09) | 0.03 | 2.65 (1.18, 5.94) | 0.02 |
| Smoker log NNAL | 1.38 (1.24, 1.55) | < 0.0001 | 1.34 (1.16, 1.54) | < 0.0001 | |||
| Nonsmoker English fluency | |||||||
| Low | 1.53 (1.16, 2.05) | Reference | Reference | Reference | |||
| High | 0.74 (0.50, 1.10) | 0.48 (0.29, 0.81) | 0.006 | 0.50 (0.27, 0.94) | 0.03 | 0.54 (0.30, 0.98) | 0.04 |
| Smoker planning to quit | |||||||
| Next 6 months | 0.91 (0.67, 1.24) | 0.53 (0.33, 0.84) | 0.007 | 0.67 (0.39, 1.16) | 0.15 | 0.80 (0.47, 1.35) | 0.40 |
| >6 months | 1.72 (1.21, 2.45) | Reference | Reference | Reference | |||
| Children in home | |||||||
| Yes | 1.22 (0.89, 1.67) | Reference | Reference | Reference | |||
| No | 1.63 (0.88, 3.04) | 1.34 (0.70, 2.58) | 0.38 | 1.03 (0.54, 1.97) | 0.93 | 1.14 (0.61, 2.11) | 0.68 |
| Adjusted R squared | 0.08 | 0.08 | 0.18 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, E.; Dove, M.; Saw, A.; Tsoh, J.Y.; Fung, L.-C.; Tong, E.K. Home Smoking Bans and Urinary NNAL Levels to Measure Tobacco Smoke Exposure in Chinese American Household Pairs. Int. J. Environ. Res. Public Health 2021, 18, 7682. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147682
Chang E, Dove M, Saw A, Tsoh JY, Fung L-C, Tong EK. Home Smoking Bans and Urinary NNAL Levels to Measure Tobacco Smoke Exposure in Chinese American Household Pairs. International Journal of Environmental Research and Public Health. 2021; 18(14):7682. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147682
Chicago/Turabian StyleChang, Emiley, Melanie Dove, Anne Saw, Janice Y. Tsoh, Lei-Chun Fung, and Elisa K. Tong. 2021. "Home Smoking Bans and Urinary NNAL Levels to Measure Tobacco Smoke Exposure in Chinese American Household Pairs" International Journal of Environmental Research and Public Health 18, no. 14: 7682. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18147682