
Success Factors for Community Health Workers in Implementing an Integrated Group-Based Child Development Intervention in Rural Bangladesh

 , ,
, , 
 ,
,  , ,
, ,  ,
,  , ,
, ,
Abstract
:1. Introduction
- (1)
- Can they be implemented by community health workers (CHWs) at a large scale? and
- (2)
- Can they be integrated with other maternal and child health and nutrition interventions, without losing their effectiveness?
2. Materials and Methods
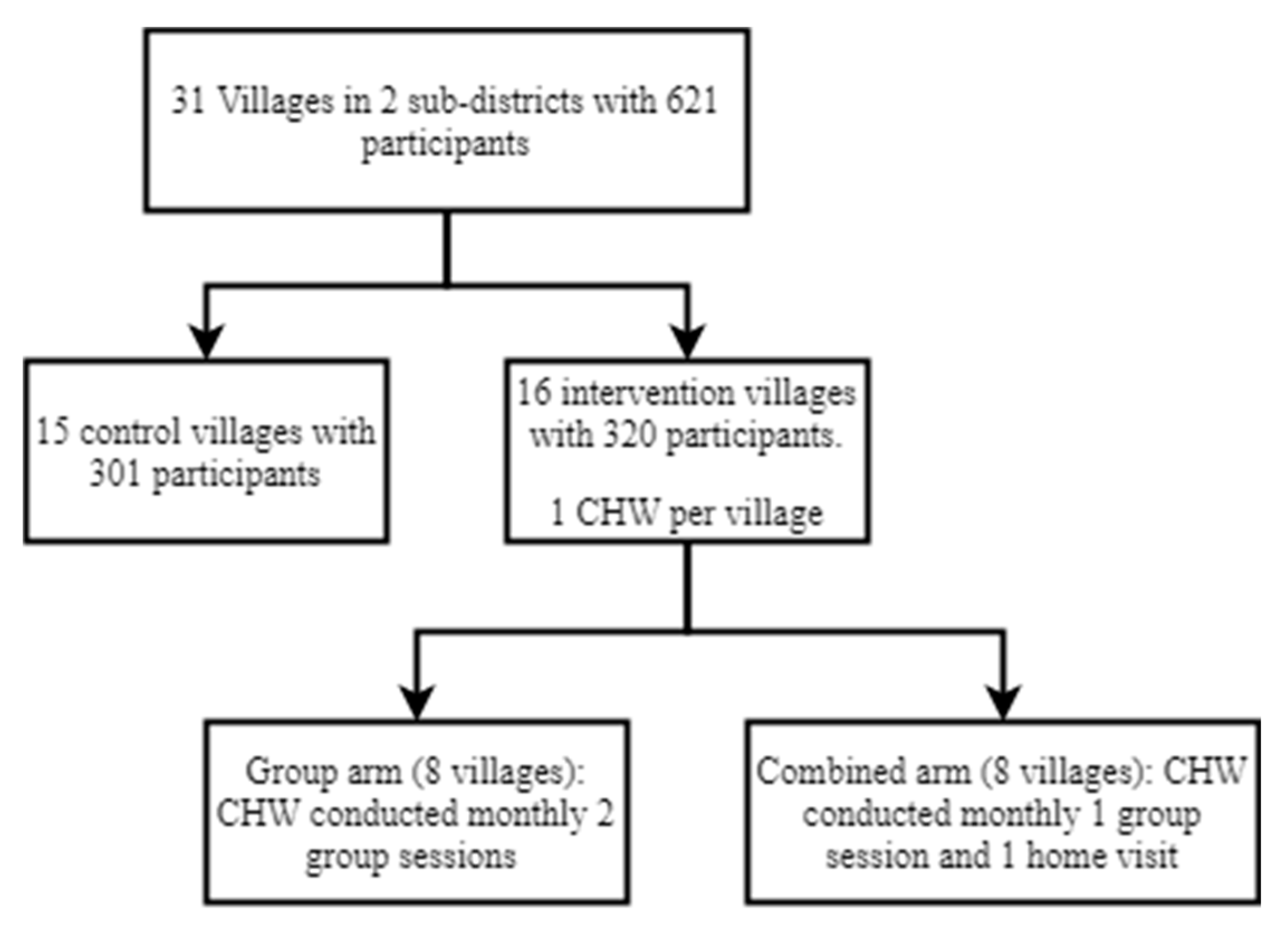
2.1. Study Context
2.2. Recruitment and Training of CHWs
2.3. Responsibilities and Supervision of CHWs
2.4. Methods of Qualitative Evaluation
2.5. Ethical Consideration
3. Results
3.1. Enablers of Successful Intervention Implementation
The behavior and attitude of all our supervisors and other officials was very positive and nice to us. This also raised our acceptance and respect in the community. In my previous job, I did not find this. This is another fact, I would love to join another project of iccdr,b, if I get a chance.
I could enter my assigned households at any time; even if mothers were absent, I experienced a warm welcome from their family members. Sometimes I waited alone in their room; they had trust upon me and allowed me to sit in their own room in absence of the mother.
While observing sessions I found, mothers become very happy when the CHW showed them how to play with toys with their babies and they could do it properly. Mothers were interested and very proud when they found their babies could properly follow CHW’s instruction.
As we have a tablet computer in our hand, people respect us because they thought we are doing a very high-class job.
3.2. Difficulties of Implementing the Integrated Intervention
3.2.1. Problems Faced Attending the Required Training
I never stayed overnight outside without my family members. Yes, sometimes I stayed at my parents’ house with my children, but after my marriage, I did not stay outside alone. I always think of what my children are doing and what my in-laws would think about me. They must be thinking that I’m staying there so that I might not do household chores. I always remain concerned whether any of my family members is calling me over phone. That’s why I could not pay full attention to the sessions.
It takes two hours to come to the training venue from my residence. I started very early in the morning. For this reason, I needed to wake up early and complete all household chores. I found my entire attempt to join training session on time, were in vain, because I needed to wait for vehicle. Sometimes it took an hour to get into a bus to reach the training venue.
Sometimes, after completing training sessions, when I get back to my home, it is almost night. My in-laws are not happy with that. They did not allow me to stay outside till night. Sometimes my brother-in-law says harsh words to me due to my late arrival at home.
3.2.2. Difficulties in Conducting and Managing Group Sessions
We were supposed to show the baby how to play with toys according to their age group in one session, I was showing a baby how to play with a flower puzzle, then babies from other age groups also demanded the same toy. At the time, I did not have enough flower puzzles. The children continued to cry and grabbed the toy from other children. Some mothers left early as the sessions became chaotic and loud. As a result, I could not complete that particular session.
Pregnant mothers have various “sharirik-lokkhon” if they sit in one place, they feel sleepy and sometimes pain in their body parts. Then we suggested them to stand up and take a walk around. At that time either we paused the session or talked to the lactating mothers.
3.2.3. Difficulties with Distribution of Equipment and Commodities
3.2.4. Problems Faced in Delivery of Session Content
We are telling mothers to share their problem in meetings. Mothers thought if they had any issue with their husbands or in-laws and they share it in group meetings, other mothers of these meetings will taunt them and laugh at them, which will increase their problems rather reducing them.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lu, C.; Black, M.M.; Richter, L.M. Risk of poor development in young children in low-income and middle-income countries: An estimation and analysis at the global, regional, and country level. Lancet Glob. Health 2016, 4, e916. [Google Scholar] [CrossRef] [Green Version]
- Britto, P.R.; Lye, S.J.; Proulx, K.; Yousafzai, A.K.; Matthews, S.G.; Vaivada, T.; Perez-Escamilla, R.; Rao, N.; Ip, P.; Fernald, L.C. Nurturing care: Promoting early childhood development. Lancet 2017, 389, 91. [Google Scholar] [CrossRef] [Green Version]
- Aboud, F.E.; Yousafzai, A.K. Global health and development in early childhood. Annu. Rev. Psychol. 2015, 66, 433. [Google Scholar] [CrossRef] [PubMed]
- Black, M.M.; Walker, S.P.; Fernald, L.C.; Andersen, C.T.; DiGirolamo, A.M.; Lu, C.; McCoy, D.C.; Fink, G.; Shawar, Y.R.; Shiffman, J.; et al. Early childhood development coming of age: Science through the life course. Lancet 2017, 389, 77. [Google Scholar] [CrossRef] [Green Version]
- Cacal, S.L.; Spock, N.; Quensell, M.L.; Sentell, T.L.; Stupplebeen, D.A. Legislative Definitions of Community Health Workers: Examples from Other States to Inform Hawaii. Hawaii J. Med. Public Health 2019, 78 (Suppl. 1), 23. [Google Scholar]
- MOHFW. Bangladesh National Strategy for Community Health Workers; Ministry of Health and Family Welfare Government of Bangladesh: Dhaka, Bangladesh, 2019. [Google Scholar]
- Attanasio, O.P.; Fernández, C.; Fitzsimons, E.O.; Grantham-McGregor, S.M.; Meghir, C.; Rubio-Codina, M. Using the infrastructure of a conditional cash transfer program to deliver a scalable integrated early child development program in Colombia: Cluster randomized controlled trial. BMJ 2014, 349, g5785. [Google Scholar] [CrossRef] [Green Version]
- Yousafzai, A.K.; Rasheed, M.A.; Rizvi, A.; Armstrong, R.; Bhutta, Z.A. Effect of integrated responsive stimulation and nutrition interventions in the Lady Health Worker programme in Pakistan on child development, growth, and health outcomes: A cluster-randomised factorial effectiveness trial. Lancet 2014, 384, 1282. [Google Scholar] [CrossRef]
- Powell, C.; Grantham-McGregor, S. Home visiting of varying frequency and child development. Pediatrics 1989, 84, 157. [Google Scholar]
- Lewin, S.; Munabi-Babigumira, S.; Glenton, C.; Daniels, K.; Bosch-Capblanch, X.; van Wyk, B.E.; Odgaard-Jensen, J.; Johansen, M.; Aja, G.N.; Zwarenstein, M.; et al. Lay health workers in primary and community health care for maternal and child health and the management of infectious diseases. Cochrane Database Syst. Rev. 2010. [Google Scholar] [CrossRef]
- Kok, M.C.; Dieleman, M.; Taegtmeyer, M.; Broerse, J.E.; Kane, S.S.; Ormel, H.; Tijm, M.M.; de Koning, K.A. Which intervention design factors influence performance of community health workers in low-and middle-income countries? A systematic review. Health Policy Plan. 2015, 30, 1207. [Google Scholar] [CrossRef] [PubMed]
- Tran, N.T.; Portela, A.; de Bernis, L.; Beek, K. Developing capacities of community health workers in sexual and reproductive, maternal, newborn, child, and adolescent health: A mapping and review of training resources. PLoS ONE 2014, 9, e94948. [Google Scholar] [CrossRef]
- Unicomb, L.; Begum, F.; Leontsini, E.; Rahman, M.; Ashraf, S.; Naser, A.M.; Nizame, F.A.; Jannat, K.; Hussain, F.; Parvez, S.M.; et al. WASH Benefits Bangladesh trial: Management structure for achieving high coverage in an efficacy trial. Trials 2018, 19, 359. [Google Scholar] [CrossRef]
- Puett, C.; Alderman, H.; Sadler, K.; Coates, J. ‘Sometimes they fail to keep their faith in us’: Community health worker perceptions of structural barriers to quality of care and community utilisation of services in Bangladesh. Matern. Child. Nutr. 2015, 11, 1011. [Google Scholar] [CrossRef]
- Zalani, G.S.; Bayat, M.; Shokri, A.; Mirbahaeddin, S.E.; Rasi, V.; Alirezaei, S.; Manafi, F. Affecting factors on the performance of community health workers in Iran’s rural areas: A review article. Iran. J. Public Health 2016, 45, 1399. [Google Scholar]
- Nahar, B.; Hossain, M.; Hamadani, J.; Ahmed, T.; Huda, S.; Grantham-McGregor, S.; Persson, L. Effects of a community-based approach of food and psychosocial stimulation on growth and development of severely malnourished children in Bangladesh: A randomised trial. Eur. J. Clin. Nutr. 2012, 66, 701. [Google Scholar] [CrossRef]
- Pitchik, H.O.; Tofail, F.; Rahman, M.; Akter, F.; Sultana, J.; Shoab, A.K.; Huda, T.M.N.; Jahir, T.; Amin, M.R.; Hossain, M.K.; et al. A holistic approach to promoting early child development: A cluster randomised trial of a group-based, multicomponent intervention in rural Bangladesh. BMJ Glob. Health 2021, 6, e004307. [Google Scholar] [CrossRef] [PubMed]
- Sikander, S.; Lazarus, A.; Bangash, O.; Fuhr, D.C.; Weobong, B.; Krishna, R.N.; Ahmad, I.; Weiss, H.A.; Price, L.; Rahman, A.; et al. The effectiveness and cost-effectiveness of the peer-delivered Thinking Healthy Programme for perinatal depression in Pakistan and India: The SHARE study protocol for randomised controlled trials. Trials 2015, 16, 534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahman, A.; Malik, A.; Sikander, S.; Roberts, C.; Creed, F. Cognitive behaviour therapy-based intervention by community health workers for mothers with depression and their infants in rural Pakistan: A cluster-randomised controlled trial. Lancet 2008, 372, 902. [Google Scholar] [CrossRef] [Green Version]
- Matias, S.L.; Mridha, M.K.; Young, R.T.; Hussain, S.; Dewey, K.G. Daily Maternal Lipid-Based Nutrient Supplementation with 20 mg Iron, Compared with Iron and Folic Acid with 60 mg Iron, Resulted in Lower Iron Status in Late Pregnancy but Not at 6 Months Postpartum in Either the Mothers or Their Infants in Bangladesh. J. Nutr. 2018, 148, 1615. [Google Scholar] [CrossRef]
- Luby, S.P.; Rahman, M.; Arnold, B.F.; Unicomb, L.; Ashraf, S.; Winch, P.J.; Stewart, C.P.; Begum, F.; Hussain, F.; Benjamin-Chung, J.; et al. Effects of water quality, sanitation, handwashing, and nutritional interventions on diarrhoea and child growth in rural Bangladesh: A cluster randomised controlled trial. Lancet Glob. Health 2018, 6, e302. [Google Scholar] [CrossRef] [Green Version]
- Forsyth, J.E.; Nurunnahar, S.; Islam, S.S.; Baker, M.; Yeasmin, D.; Islam, M.S.; Rahman, M.; Fendorf, S.; Ardoin, N.M.; Winch, P.J.; et al. Turmeric means “yellow” in Bengali: Lead chromate pigments added to turmeric threaten public health across Bangladesh. Environ. Res. 2019, 179, 108722. [Google Scholar] [CrossRef] [PubMed]
- Akter, F.; Rahman, M.; Pitchik, H.O.; Winch, P.J.; Fernald, L.C.; Huda, T.M.N.; Jahir, T.; Amin, R.; Das, J.B.; Hossain, K.; et al. Adaptation and Integration of Psychosocial Stimulation, Maternal Mental Health and Nutritional Interventions for Pregnant and Lactating Women in Rural Bangladesh. Int. J. Environ. Res. Public Health 2020, 17, 6233. [Google Scholar] [CrossRef] [PubMed]
- Mehrin, S.F.; Hasan, M.I.; Salveen, N.; Hossain, S.J.; Grantham-McGregor, S.M.; Tofail, F.; Hamadani, J.D.; Baker-Henningham, H. Impact of integrated early childhood development program and primary health care service on the development of malnourished children—A cluster-randomized controlled trial. 2020; Manuscript in preparation. [Google Scholar]
- Tofail, F.; Islam, M.; Hamadani, J.; Akter, F.; Akter, S.; Koli, S.; Tabassum, N.; Roy, B.; Hossain, S.J.; Goswami, D.; et al. The Effect of integrated management of childhood maltreatment, maternal depression, psychosocial stimulation and nutritional intervention on child development—A randomized controlled trial. 2020; Manuscript in preparation. [Google Scholar]
- Hamadani, J.D.; Mehrin, S.F.; Tofail, F.; Hasan, M.I.; Huda, S.N.; Baker-Henningham, H.; Ridout, D.; Grantham-McGregor, S. Integrating an early childhood development programme into Bangladeshi primary health-care services: An open-label, cluster-randomised controlled trial. Lancet Glob. Health 2019, 7, e366. [Google Scholar] [CrossRef] [Green Version]
- Qualcomm. mSakhi: Improving Maternal, Neonatal and Child Health with User-friendly, Mobile Applications for Frontline Health Workers; Qualcomm Wireless Reach: San Diego, CA, USA, 11 September 2015. [Google Scholar]
- Braun, R.; Catalani, C.; Wimbush, J.; Israelski, D. Community health workers and mobile technology: A systematic review of the literature. PLoS ONE 2013, 8, e65772. [Google Scholar] [CrossRef] [PubMed]
- Masood, S. Intimate Partner Violence: Childhood Exposure and Respective Attitudes among Pakistani Young Adults. Ph.D. Thesis, University of Warwick, Coventry, UK, 2014. [Google Scholar]
- Schoepf, B.G. AIDS action-research with women in Kinshasa, Zaire. Soc. Sci. Med. 1993, 37, 1401. [Google Scholar] [CrossRef]
- Yeasmin, F.; Winch, P.J.; Hwang, S.T.; Leontsini, E.; Jahir, T.; Das, J.B.; Amin, M.R.; Hossain, M.K.; Huda, T.M.N.; Akter, F.; et al. Exploration of Attendance, Active Participation, and Behavior Change in a Group-Based Responsive Stimulation, Maternal and Child Health, and Nutrition Intervention. Am. J. Trop. Med. Hyg. 2021, 104, 1586. [Google Scholar] [CrossRef]
- Rahman, M.; Ashraf, S.; Unicomb, L.; Mainuddin, A.; Parvez, S.M.; Begum, F.; Das, K.K.; Naser, A.M.; Hussain, F.; Clasen, T.; et al. WASH Benefits Bangladesh trial: System for monitoring coverage and quality in an efficacy trial. Trials 2018, 19, 360. [Google Scholar] [CrossRef]
- Tomlinson, M.; Rotheram-Borus, M.J.; Harwood, J.; Le Roux, I.M.; O’Connor, M.; Worthman, C. Community health workers can improve child growth of antenatally-depressed, South African mothers: A cluster randomized controlled trial. BMC Psychiatry 2015, 15, 225. [Google Scholar] [CrossRef] [Green Version]
- Rothstein, J.D.; Caulfield, L.E.; Broaddus-Shea, E.T.; Muschelli, J.; Gilman, R.H.; Winch, P.J. “The doctor said formula would help me”: Health sector influences on use of infant formula in peri-urban Lima, Peru. Soc. Sci. Med. 2020, 244. [Google Scholar] [CrossRef]
- Glenton, C.; Colvin, C.J.; Carlsen, B.; Swartz, A.; Lewin, S.; Noyes, J.; Rashidian, A. Barriers and facilitators to the implementation of lay health worker programmes to improve access to maternal and child health: A qualitative evidence synthesis. Cochrane Database Syst. Rev. 2013, 10. [Google Scholar] [CrossRef]
- Campbell, C.; Scott, K. Retreat from Alma Ata? The WHO’s report on Task Shifting to community health workers for AIDS care in poor countries. Glob. Public Health 2011, 6, 125. [Google Scholar] [PubMed] [Green Version]
- Målqvist, M.; Yuan, B.; Trygg, N.; Selling, K.; Thomsen, S. Targeted interventions for improved equity in maternal and child health in low-and middle-income settings: A systematic review and meta-analysis. PLoS ONE 2013, 8, e66453. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Group Arm (Group + Group) | Combined Arm (Group + Home Visit) | ||
|---|---|---|---|
| Session No. | Components Provided | Session No. | Components Provided |
| 1 | Introduction to child stimulation, WASH, and maternal and child nutrition | 1 (group) | Introduction to child stimulation, WASH, and maternal and child nutrition |
| 2 | Child stimulation, and maternal and child nutrition | 2 (home) | Child stimulation, and maternal and child nutrition |
| 3 | Child stimulation, WASH, and maternal and child nutrition | 3 (group) | Child stimulation, and maternal and child nutrition |
| 4 | Child stimulation, maternal mental health, and maternal and child nutrition | 4 (home) | Child stimulation, maternal mental health, and maternal and child nutrition |
| 5 | Lead, child stimulation, and maternal and child nutrition | 5 (group) | Lead, child stimulation, and WASH |
| 6 | Child stimulation, maternal mental health, and maternal and child nutrition | 6 (home) | Child stimulation, maternal mental health, and maternal and child nutrition |
| 7 | Child stimulation, and maternal and child nutrition | 7 (group) | Child stimulation, and maternal and child nutrition |
| 8 | Child stimulation, WASH, and maternal mental health | 8 (home) | Child stimulation, maternal mental health, and maternal and child nutrition |
| 9 | Child stimulation and WASH | 9 (group) | Child stimulation, WASH, and maternal and child nutrition |
| 10 | Child stimulation, maternal mental health, and maternal and child nutrition | 10 (home) | Child stimulation, maternal mental health, and maternal and child nutrition |
| 11 | Child stimulation and WASH | 11 (group) | Child stimulation and WASH |
| 12 | Child stimulation, maternal mental health, and maternal and child nutrition | 12 (home) | Child stimulation, WASH, and maternal mental health |
| 13 | Child stimulation and WASH | 13 (group) | Child stimulation |
| 14 | Child stimulation, WASH, maternal mental health, and maternal and child nutrition | 14 (home) | Child stimulation, maternal mental health, and maternal and child nutrition |
| 15 | Child stimulation, WASH, and maternal and child nutrition | 15 (group) | Child stimulation and WASH |
| 16 | Child stimulation, WASH, and maternal and child nutrition | 16 (home) | Child stimulation, maternal mental health, and maternal and child nutrition |
| 17 | Child stimulation, and maternal and child nutrition | 17 (group) | Child stimulation and maternal mental health |
| 18 | Child stimulation and summary on WASH, maternal mental health, and maternal and child nutrition | 18 (home) | Child stimulation and maternal and child nutrition |
| Group Arm No. of CHW N = 8 | Mixed Arm No. of CHW N = 8 | Total No. of CHW N = 16 | Total No. of Supervisor N = 4 | |
|---|---|---|---|---|
| Age in years | ||||
| 20–25 | 5 | 3 | 8 | |
| 31–35 | 3 | 4 | 7 | 2 |
| 36–40 | 0 | 1 | 1 | 2 |
| Education | ||||
| Higher secondary | 4 | 4 | 8 | |
| Secondary | 4 | 4 | 8 | |
| Postgraduate | 4 | |||
| Religion | ||||
| Muslim | 7 | 8 | 15 | 2 |
| Hindu | 1 | 0 | 1 | |
| Marital status | ||||
| Married | 6 | 7 | 13 | 4 |
| Unmarried | 2 | 1 | 3 | |
| Monthly family income (in USD) * | ||||
| <125 | 1 | 5 | 6 | |
| 126–185 | 4 | 2 | 6 | |
| 186–250 | 2 | 1 | 3 | |
| >250 | 1 | 0 | 1 | 4 |
| 1st Qualitative Assessment | |||
| Type of Participant | Focus Groups | Individual Interviews | Group Discussion |
| CHW | 2 (1 with 8 CHWs of group arm, 1 with 8 CHWs of combined arm) | N/A | N/A |
| Supervisors of CHWs | N/A | 4 (1 with each supervisor) | N/A |
| 2nd Qualitative Assessment | |||
| CHW | 3 (1 with 8 CHWs of group arm, 1 with 8 CHWs of combined arm and 1 with good and poorly performed CHWs) | N/A | N/A |
| Supervisors of CHWs | N/A | N/A | 1 (with all 4) |
| Type of Barriers | Description of the Barrier |
|---|---|
| Barriers related to attending training sessions | CHWs faced problems to arrive at training sessions on time due to distance and lack of vehicle. They also could not give proper attention during the lengthy in-house training sessions required, as they felt distracted and concerned about their prolonged absence from their families at home. |
| Difficulties related to session management | CHWs faced problems as they had to use different materials for different components in a single session and they failed to attract the mother’s attention due to noise. |
| Barriers related to achieving trust from the community | CHWs faced problems to achieve trust from the community due to targeting mothers for additional commodities depending on mid-upper arm circumference (MUAC) measurement and for “exclusive breastfeeding” mothers trusted doctors and other health professionals more than CHWs. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jahir, T.; Winch, P.J.; Leontsini, E.; Hwang, S.T.; Yeasmin, F.; Hossain, K.; Das, J.B.; Amin, R.; Nurul Huda, T.M.; Sultana, J.; et al. Success Factors for Community Health Workers in Implementing an Integrated Group-Based Child Development Intervention in Rural Bangladesh. Int. J. Environ. Res. Public Health 2021, 18, 7891. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18157891
Jahir T, Winch PJ, Leontsini E, Hwang ST, Yeasmin F, Hossain K, Das JB, Amin R, Nurul Huda TM, Sultana J, et al. Success Factors for Community Health Workers in Implementing an Integrated Group-Based Child Development Intervention in Rural Bangladesh. International Journal of Environmental Research and Public Health. 2021; 18(15):7891. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18157891
Chicago/Turabian StyleJahir, Tania, Peter J. Winch, Elli Leontsini, Sharon T. Hwang, Farzana Yeasmin, Khobair Hossain, Jyoti Bhushan Das, Ruhul Amin, Tarique Md. Nurul Huda, Jesmin Sultana, and et al. 2021. "Success Factors for Community Health Workers in Implementing an Integrated Group-Based Child Development Intervention in Rural Bangladesh" International Journal of Environmental Research and Public Health 18, no. 15: 7891. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18157891