
Association of Parental Socioeconomic Status and Physical Activity with Development of Arterial Stiffness in Prepubertal Children

 and
and
Abstract
:1. Introduction
2. Materials and Methods
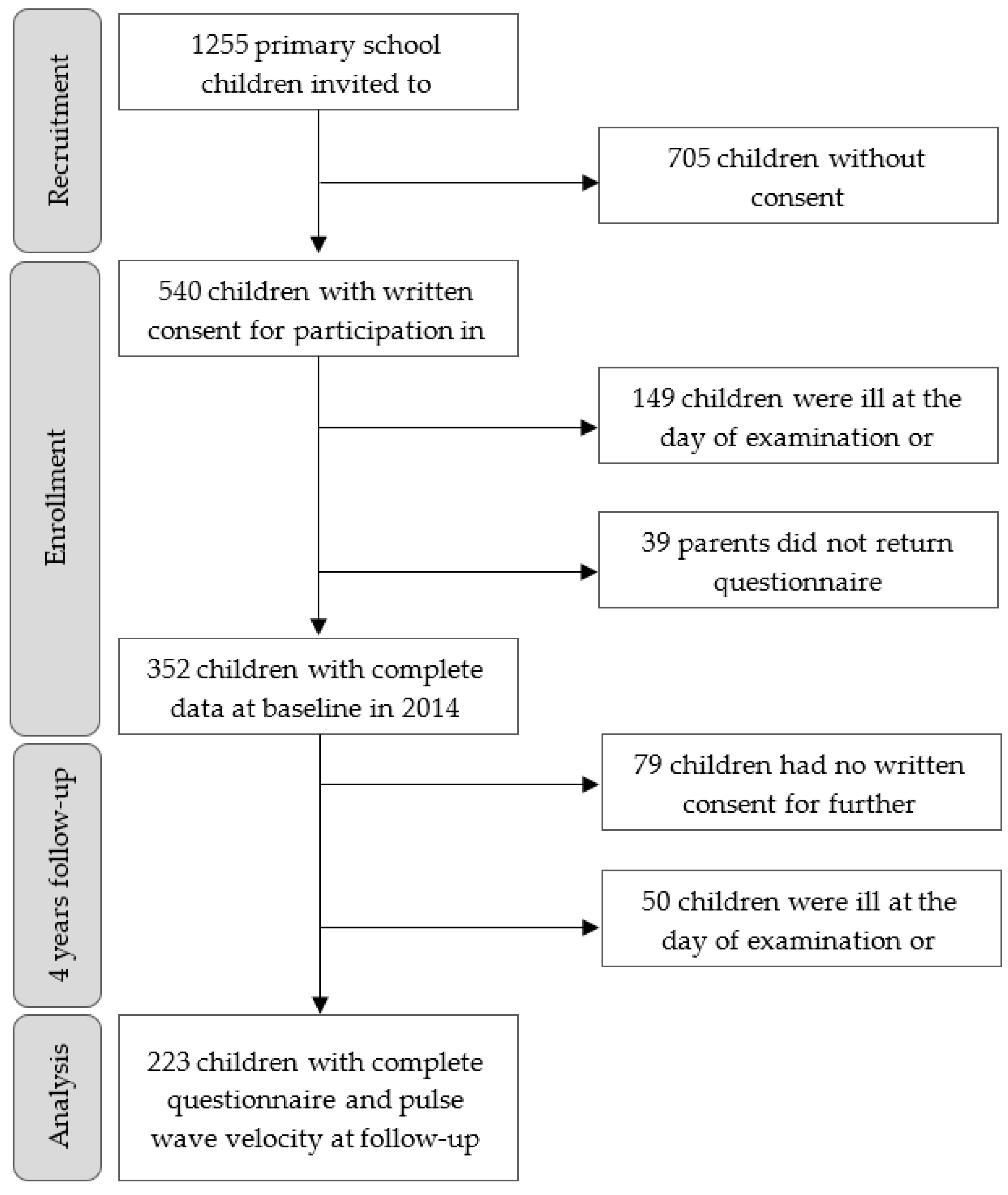
2.1. Study Design and Participants
2.2. Measurements
2.2.1. Central Arterial Stiffness
2.2.2. Anthropometric Parameters and Physical Fitness
2.2.3. Socioeconomic Status and Migration Background
2.2.4. Parental and Family Physical Activity Behavior
2.3. Statistical Analysis
3. Results
3.1. Population Characteristics
3.2. Association of Socioeconomic Status and Migration Background with Childhood Arterial Stiffness
3.3. Association of Parental and Familial Physical Activity Behavior with Childhood Arterial Stiffness
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roth, G.A.; Johnson, C.; Abajobir, A.; Abd-Allah, F.; Abera, S.F.; Abyu, G.; Ahmed, M.; Aksut, B.; Alam, T.; Alam, K.; et al. Global, Regional, and National Burden of Cardiovascular Diseases for 10 Causes, 1990 to 2015. J. Am. Coll. Cardiol. 2017, 70, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Havranek, E.P.; Mujahid, M.S.; Barr, D.A.; Blair, I.V.; Cohen, M.S.; Cruz-Flores, S.; Smith, G.D.; Himmelfarb, C.D.; Lauer, M.S.; Lockwood, D.W.; et al. Social Determinants of Risk and Outcomes for Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation 2015, 132, 873–898. [Google Scholar] [CrossRef] [Green Version]
- Veronesi, G.; Tunstall-Pedoe, H.; Ferrario, M.M.; Kee, F.; Kuulasmaa, K.; Chambless, L.E.; Amouyel, P.; Arveiler, D.; Bobak, M.; Ferrieres, J.; et al. Combined effect of educational status and cardiovascular risk factors on the incidence of coronary heart disease and stroke in European cohorts: Implications for prevention. Eur. J. Prev. Cardiol. 2016, 24, 437–445. [Google Scholar] [CrossRef] [PubMed]
- Winkleby, M.A.; Jatulis, D.E.; Frank, E.; Fortmann, S.P. Socioeconomic status and health: How education, income, and occupation contribute to risk factors for cardiovascular disease. Am. J. Public Health 1992, 82, 816–820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vazquez, C.E.; Cubbin, C. Socioeconomic Status and Childhood Obesity: A Review of Literature from the Past Decade to Inform Intervention Research. Curr. Obes. Rep. 2020, 9, 562–570. [Google Scholar] [CrossRef]
- Kivimäki, M.; Lawlor, D.A.; Smith, G.D.; Keltikangas-Järvinen, L.; Elovainio, M.; Vahtera, J.; Pulkki-Råback, L.; Taittonen, L.; Viikari, J.S.A.; Raitakari, O.T. Early Socioeconomic Position and Blood Pressure in Childhood and Adulthood. Hypertension 2006, 47, 39–44. [Google Scholar] [CrossRef] [Green Version]
- Pour, M.B.; Bergström, A.; Bottai, M.; Kull, I.; Wickman, M.; Håkansson, N.; Wolk, A.; Moradi, T. Effect of Parental Migration Background on Childhood Nutrition, Physical Activity, and Body Mass Index. J. Obes. 2014, 2014, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van den Berg, G.; Van Eijsden, M.; Galindo-Garre, F.; Vrijkotte, T.G.; Gemke, R.J. Explaining Socioeconomic Inequalities in Childhood Blood Pressure and Prehypertension. Hypertension 2013, 61, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Power, C.; Manor, O.; Matthews, S. Child to adult socioeconomic conditions and obesity in a national cohort. Int. J. Obes. 2003, 27, 1081–1086. [Google Scholar] [CrossRef] [Green Version]
- Ferreira, I.; van der Horst, K.; Wendel-Vos, W.; Kremers, S.; Van Lenthe, F.J.; Brug, J. Environmental correlates of physical activity in youth – a review and update. Obes. Rev. 2007, 8, 129–154. [Google Scholar] [CrossRef]
- Imhof, K.; Faude, O.; Donath, L.; Bean-Eisenhut, S.; Hanssen, H.; Zahner, L. The association of socio-economic factors with physical fitness and activity behaviours, spinal posture and retinal vessel parameters in first graders in urban Switzerland. J. Sports Sci. 2015, 34, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Lehto, E.; Ray, C.; Velde, S.T.; Petrova, S.; Duleva, V.; Krawinkel, M.; Behrendt, I.; Papadaki, A.; Kristjansdottir, A.; Thorsdottir, I.; et al. Mediation of parental educational level on fruit and vegetable intake among schoolchildren in ten European countries. Public Health Nutr. 2014, 18, 89–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolte, G.; Fromme, H.; For the GME Study Group. Socioeconomic determinants of children’s environmental tobacco smoke exposure and family’s home smoking policy. Eur. J. Public Health 2008, 19, 52–58. [Google Scholar] [CrossRef] [Green Version]
- Vlachopoulos, C.; Aznaouridis, K.; Stefanadis, C. Prediction of Cardiovascular Events and All-Cause Mortality with Arterial Stiffness: A Systematic Review and Meta-Analysis. J. Am. Coll. Cardiol. 2010, 55, 1318–1327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ben-Shlomo, Y.; Spears, M.; Boustred, C.; May, M.; Anderson, S.; Benjamin, E.; Boutouyrie, P.; Cameron, J.; Chen, C.-H.; Cruickshank, J.K.; et al. Aortic Pulse Wave Velocity Improves Cardiovascular Event Prediction. J. Am. Coll. Cardiol. 2014, 63, 636–646. [Google Scholar] [CrossRef] [PubMed]
- Zhong, Q.; Hu, M.-J.; Cui, Y.-J.; Liang, L.; Zhou, M.-M.; Yang, Y.-W.; Huang, F. Carotid–Femoral Pulse Wave Velocity in the Prediction of Cardiovascular Events and Mortality: An Updated Systematic Review and Meta-Analysis. Angiology 2017, 69, 617–629. [Google Scholar] [CrossRef]
- Lona, G.; Hauser, C.; Köchli, S.; Infanger, D.; Endes, K.; Schmidt-Trucksäss, A.; Hanssen, H. Association of blood pressure, obesity and physical activity with arterial stiffness in children: A systematic review and meta-analysis. Pediatr. Res. 2021, 1–11. [Google Scholar] [CrossRef]
- Proudfoot, N.A.; King-Dowling, S.; Cairney, J.; Bray, S.R.; Macdonald, M.J.; Timmons, B.W. Physical Activity and Trajectories of Cardiovascular Health Indicators During Early Childhood. Pediatrics 2019, 144, e20182242. [Google Scholar] [CrossRef]
- Lona, G.; Hauser, C.; Köchli, S.; Infanger, D.; Endes, K.; Faude, O.; Hanssen, H. Blood Pressure Increase and Microvascular Dysfunction Accelerate Arterial Stiffening in Children: Modulation by Physical Activity. Front. Physiol. 2020, 11, 613003. [Google Scholar] [CrossRef]
- Din-Dzietham, R.; Luao, D.; Diez-Roux, A.; Nieto, J.; Paton, C.; Howard, G.; Brown, A.; Carnethon, M.; Tyroler, H. Association of Educational Achievement with Pulsatile Arterial DiameterChange of the Common Carotid Artery. Am. J. Epidemiol. 2000, 152, 617–627. [Google Scholar] [CrossRef] [Green Version]
- Trudel, X.; Shipley, M.J.; McEniery, C.M.; Wilkinson, I.B.; Brunner, E.J. Socioeconomic status, education, and aortic stiffness progression over 5 years: The Whitehall II prospective cohort study. J. Hypertens. 2016, 34, 2038–2044. [Google Scholar] [CrossRef] [Green Version]
- Köchli, S.; Endes, K.; Grenacher, J.; Streese, L.; Lona, G.; Hauser, C.; Deiseroth, A.; Zahner, L.; Hanssen, H. Socioeconomic Status and Parental Lifestyle Are Associated With Vascular Phenotype in Children. Front. Public Health 2021, 9, 610268. [Google Scholar] [CrossRef]
- Bouthoorn, S.H.; Van Lenthe, F.J.; De Jonge, L.L.; Hofman, A.; Van Osch-Gevers, L.; Jaddoe, V.W.; Raat, H. Maternal Educational Level and Blood Pressure, Aortic Stiffness, Cardiovascular Structure and Functioning in Childhood: The Generation R Study. Am. J. Hypertens. 2013, 27, 89–98. [Google Scholar] [CrossRef] [Green Version]
- Lahelma, E. Pathways between socioeconomic determinants of health. J. Epidemiol. Community Health 2004, 58, 327–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imhof, K.; Zahner, L.; Schmidt-Trucksäss, A.; Hanssen, H. Association of body composition and blood pressure categories with retinal vessel diameters in primary school children. Hypertens. Res. 2016, 39, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Franssen, P.M.; Imholz, B.P. Evaluation of the Mobil-O-Graph new generation ABPM device using the ESH criteria. Blood Press. Monit. 2010, 15, 229–231. [Google Scholar] [CrossRef] [PubMed]
- Wassertheurer, S.; Kropf, J.; Weber, T.; Van Der Giet, M.; Baulmann, J.; Ammer, M.; Hametner, B.; Mayer, C.C.; Eber, B.; Magometschnigg, D. A new oscillometric method for pulse wave analysis: Comparison with a common tonometric method. J. Hum. Hypertens. 2010, 24, 498–504. [Google Scholar] [CrossRef]
- Weiss, W.; Gohlisch, C.; Harsch-Gladisch, C.; Tölle, M.; Zidek, W.; van der Giet, M. Oscillometric estimation of central blood pressure: Validation of the Mobil-O-Graph in comparison with the SphygmoCor device. Blood Press. Monit. 2012, 17, 128–131. [Google Scholar] [CrossRef] [Green Version]
- Elmenhorst, J.; Hulpke-Wette, M.; Barta, C.; Pozza, R.D.; Springer, S.; Oberhoffer, R. Percentiles for central blood pressure and pulse wave velocity in children and adolescents recorded with an oscillometric device. Atherosclerosis 2015, 238, 9–16. [Google Scholar] [CrossRef]
- Rosario, A.S.; Kurth, B.-M.; Stolzenberg, H.; Ellert, U.; Neuhauser, H. Body mass index percentiles for children and adolescents in Germany based on a nationally representative sample (KiGGS 2003–2006). Eur. J. Clin. Nutr. 2010, 64, 341–349. [Google Scholar] [CrossRef] [Green Version]
- National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents. Pediatrics 2004, 114, 555–576. [CrossRef]
- Flynn, J.T.; Kaelber, D.C.; Baker-Smith, C.M.; Blowey, D.; Carroll, A.E.; Daniels, S.R.; De Ferranti, S.D.; Dionne, J.M.; Falkner, B.; Flinn, S.K.; et al. Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and Adolescents. Pediatrics 2017, 140, e20171904. [Google Scholar] [CrossRef] [Green Version]
- Kriemler, S.; Zahner, L.; Schindler, C.; Meyer, U.; Hartmann, T.; Hebestreit, H.; Rocca, H.P.B.-L.; Van Mechelen, W.; Puder, J. Effect of school based physical activity programme (KISS) on fitness and adiposity in primary schoolchildren: Cluster randomised controlled trial. BMJ 2010, 340, c785. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neuhauser, H.K.; Thamm, M.; Ellert, U.; Hense, H.W.; Rosario, A.S. Blood Pressure Percentiles by Age and Height From Nonoverweight Children and Adolescents in Germany. Pediatrics 2011, 127, e978–e988. [Google Scholar] [CrossRef]
- van Mechelen, W.; Hlobil, H.; Kemper, H.C.G. Validation of two running tests as estimates of maximal aerobic power in children. Graefe’s Arch. Clin. Exp. Ophthalmol. 1986, 55, 503–506. [Google Scholar] [CrossRef]
- Léger, L.A.; Mercier, D.; Gadoury, C.; Lambert, J. The multistage 20 metre shuttle run test for aerobic fitness. J. Sports Sci. 1988, 6, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Artero, E.G.; Romero, V.E.; Castro-Piñero, J.; Ortega, F.B.; Suni, J.; Garzon, M.J.C.; Ruiz, J. Reliability of Field-Based Fitness Tests in Youth. Int. J. Sports Med. 2010, 32, 159–169. [Google Scholar] [CrossRef]
- Niederer, I.; Kriemler, S.; Zahner, L.; Bürgi, F.; Ebenegger, V.; Hartmann, T.; Meyer, U.; Schindler, C.; Nydegger, A.; Marques-Vidal, P.; et al. Influence of a lifestyle intervention in preschool children on physiological and psychological parameters (Ballabeina): Study design of a cluster randomized controlled trial. BMC Public Health 2009, 9, 94. [Google Scholar] [CrossRef] [Green Version]
- Lona, G.; Endes, K.; Köchli, S.; Infanger, D.; Zahner, L.; Hanssen, H. Retinal Vessel Diameters and Blood Pressure Progression in Children. Hypertension 2020, 76, 450–457. [Google Scholar] [CrossRef]
- Puolakka, E.; Pahkala, K.; Laitinen, T.T.; Magnussen, C.G.; Hutri-Kähönen, N.; Kähönen, M.; Lehtimäki, T.; Tossavainen, P.; Jokinen, E.; Sabin, M.A.; et al. Childhood Socioeconomic Status and Arterial Stiffness in Adulthood: The Cardiovascular Risk in Young Finns Study. Hypertension 2017, 70, 729–735. [Google Scholar] [CrossRef]
- Lam, P.H.; Chiang, J.J.; Chen, E.; Miller, G.E. Race, socioeconomic status, and low-grade inflammatory biomarkers across the lifecourse: A pooled analysis of seven studies. Psychoneuroendocrinology 2021, 123, 104917. [Google Scholar] [CrossRef] [PubMed]
- Moore, L.; Lombardi, D.A.; White, M.J.; Campbell, J.L.; Oliveria, S.A.; Ellison, R.C. Influence of parents’ physical activity levels on activity levels of young children. J. Pediatr. 1991, 118, 215–219. [Google Scholar] [CrossRef]
- Khanolkar, A.R.; Byberg, L.; Koupil, I. Parental influences on cardiovascular risk factors in Swedish children aged 5–14 years. Eur. J. Public Health 2011, 22, 840–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faith, M.S.; Van Horn, L.; Appel, L.J.; Burke, L.E.; Carson, J.A.S.; Franch, H.; Jakicic, J.M.; Kral, T.V.; Young, C.O.C.D.I.T.; Wansink, B.; et al. Evaluating Parents and Adult Caregivers as “Agents of Change” for Treating Obese Children: Evidence for Parent Behavior Change Strategies and Research Gaps. Circulation 2012, 125, 1186–1207. [Google Scholar] [CrossRef] [Green Version]
- Stoner, L.; Kucharska-Newton, A.; Meyer, M.L. Cardiometabolic Health and Carotid-Femoral Pulse Wave Velocity in Children: A Systematic Review and Meta-Regression. J. Pediatr. 2020, 218, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Juonala, M.; Magnussen, C.; Raitakari, O.T. Parental smoking produces long-term damage to vascular function in their children. Curr. Opin. Cardiol. 2013, 28, 569–574. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Baseline | 4 Years Follow-Up | Difference | ||||||
|---|---|---|---|---|---|---|---|---|
| n | Mean | SD | Mean | SD | Mean | SD | p-Value | |
| Sex (male, %) | 223 | 47 | ||||||
| Age (y) | 223 | 7.4 | 0.3 | 11.4 | 0.3 | |||
| Height (cm) | 210 | 125.9 | 5.1 | 149.0 | 6.6 | 23.0 | 3.6 | <0.001 |
| Weight (m) | 210 | 25.4 | 3.9 | 40.0 | 7.7 | 14.3 | 4.9 | <0.001 |
| BMI (kg/m2) Normal (%) Overweight (%) Obese (%) | 210 | 16.01 92 6 2 | 1.8 | 17.8 90 8 2 | 2.8 | 1.8 | 1.6 | <0.001 |
| Z-BMI * | 210 | -0.15 | 0.9 | -0.36 | 0.5 | 0.2 | 0.6 | <0.001 |
| Systolic BP (mmHg) Normal (%) Elevated (%) High (%) | 210 | 104.1 83 10 7 | 7.7 | 108.0 90 5 5 | 7.8 | 3.9 | 8.2 | <0.001 |
| Z-systolic BP * | 210 | 0.56 | 0.93 | 1.5 | 0.9 | 1.0 | 1.02 | <0.001 |
| Diastolic BP (mmHg) Normal (%) Elevated (%) High (%) | 210 | 65.2 76 10 14 | 7.2 | 67.0 81 9 10 | 6.5 | 1.8 | 7.6 | <0.001 |
| Z-diastolic BP | 210 | 0.56 | 1.1 | 1.3 | 0.9 | 0.74 | 1.1 | <0.001 |
| PWV (m/s) | 223 | 4.7 | 0.3 | |||||
| CRF (stages) | 202 | 4.7 | 1.7 | 6.5 | 2.1 | 1.9 | 1.8 | <0.001 |
| Parameter | Model | n | Pulse Wave Velocity at Follow-Up (Increase per 1 m/s) | |
|---|---|---|---|---|
| Mean (95% CI) | p-Value | |||
| Household income at baseline | ||||
| Low (<CHF 5000/month) | 1 | 40 | 4.56 (4.43 to 4.68) | 0.273 |
| Medium (CHF 5000–9000/month) | 70 | 4.66 (4.57 to 4.75) | ||
| High (>CHF 9000/month) | 95 | 4.69 (4.58 to 4.79) | ||
| Low (<CHF 5000/month) | 2 | 40 | 4.6 (4.51 to 4.69) | 0.382 |
| Medium (CHF 5000–9000/month) | 70 | 4.67 (4.6 to 4.73) | ||
| High (>CHF 9000/month) | 95 | 4.68 (4.62 to 4.74) | ||
| Education level at baseline | ||||
| Low (no vocational training) | 3 | 7 | 4.72 (4.52 to 4.93) | 0.544 |
| Medium (vocational training/high school education) | 74 | 4.68 (4.62 to 4.75) | ||
| High (college/university degree) | 141 | 4.64 (4.6 to 4.69) | ||
| Low (no vocational training) | 4 | 7 | 4.77 (4.54 to 5) | 0.466 |
| Medium (vocational training/high school education) | 74 | 4.68 (4.61 to 4.75) | ||
| High (college/university degree) | 141 | 4.64 (4.59 to 4.69) | ||
| Migration background at baseline | ||||
| European | 2 | 184 | 4.64 (4.6 to 4.68) | 0.445 |
| One-sided non-European | 25 | 4.71 (4.6 to 4.81) | ||
| Two-sided non-European | 9 | 4.72 (4.54 to 4.9) | ||
| European | 5 | 184 | 4.64 (4.6 to 4.68) | 0.198 |
| One-sided non-European | 25 | 4.72 (4.6 to 4.83) | ||
| Two-sided non-European | 9 | 4.79 (4.59 to 4.99) | ||
| Parameter | Pulse Wave Velocity at Follow-Up (Increase per 1 m/s) | |||
|---|---|---|---|---|
| Model | n | Mean (95% CI) | p-Value | |
| Maternal physical activity level at baseline | ||||
| Low (<1/week) | 1 | 67 | 4.7 (4.64 to 4.77) | 0.049 |
| Medium (1/week) | 73 | 4.69 (4.62 to 4.75) | ||
| High (>1/week) | 82 | 4.6 (4.54 to 4.66) | ||
| Paternal physical activity level at baseline | ||||
| Low (<1/week) | 1 | 62 | 4.69 (4.62 to 4.76) | 0.483 |
| Medium (1/week) | 59 | 4.64 (4.56 to 4.71) | ||
| High (>1/week) | 101 | 4.65 (4.6 to 4.71) | ||
| Familial physical activity level at baseline | ||||
| Low (<1/week) | 1 | 43 | 4.73 (4.65 to 4.82) | 0.108 |
| Medium (1/week) | 87 | 4.62 (4.57 to 4.68) | ||
| High (>1/week) | 91 | 4.66 (4.6 to 4.72) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lona, G.; Hauser, C.; Bade, S.; Köchli, S.; Infanger, D.; Endes, K.; Faude, O.; Hanssen, H. Association of Parental Socioeconomic Status and Physical Activity with Development of Arterial Stiffness in Prepubertal Children. Int. J. Environ. Res. Public Health 2021, 18, 8227. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18158227
Lona G, Hauser C, Bade S, Köchli S, Infanger D, Endes K, Faude O, Hanssen H. Association of Parental Socioeconomic Status and Physical Activity with Development of Arterial Stiffness in Prepubertal Children. International Journal of Environmental Research and Public Health. 2021; 18(15):8227. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18158227
Chicago/Turabian StyleLona, Giulia, Christoph Hauser, Svea Bade, Sabrina Köchli, Denis Infanger, Katharina Endes, Oliver Faude, and Henner Hanssen. 2021. "Association of Parental Socioeconomic Status and Physical Activity with Development of Arterial Stiffness in Prepubertal Children" International Journal of Environmental Research and Public Health 18, no. 15: 8227. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18158227