
Prevalence and Risk Factors of Sarcopenia among Older Adults Aged ≥65 Years Admitted to Daycare Centers of Taiwan: Using AWGS 2019 Guidelines

Abstract
:1. Introduction
2. Materials and Methods
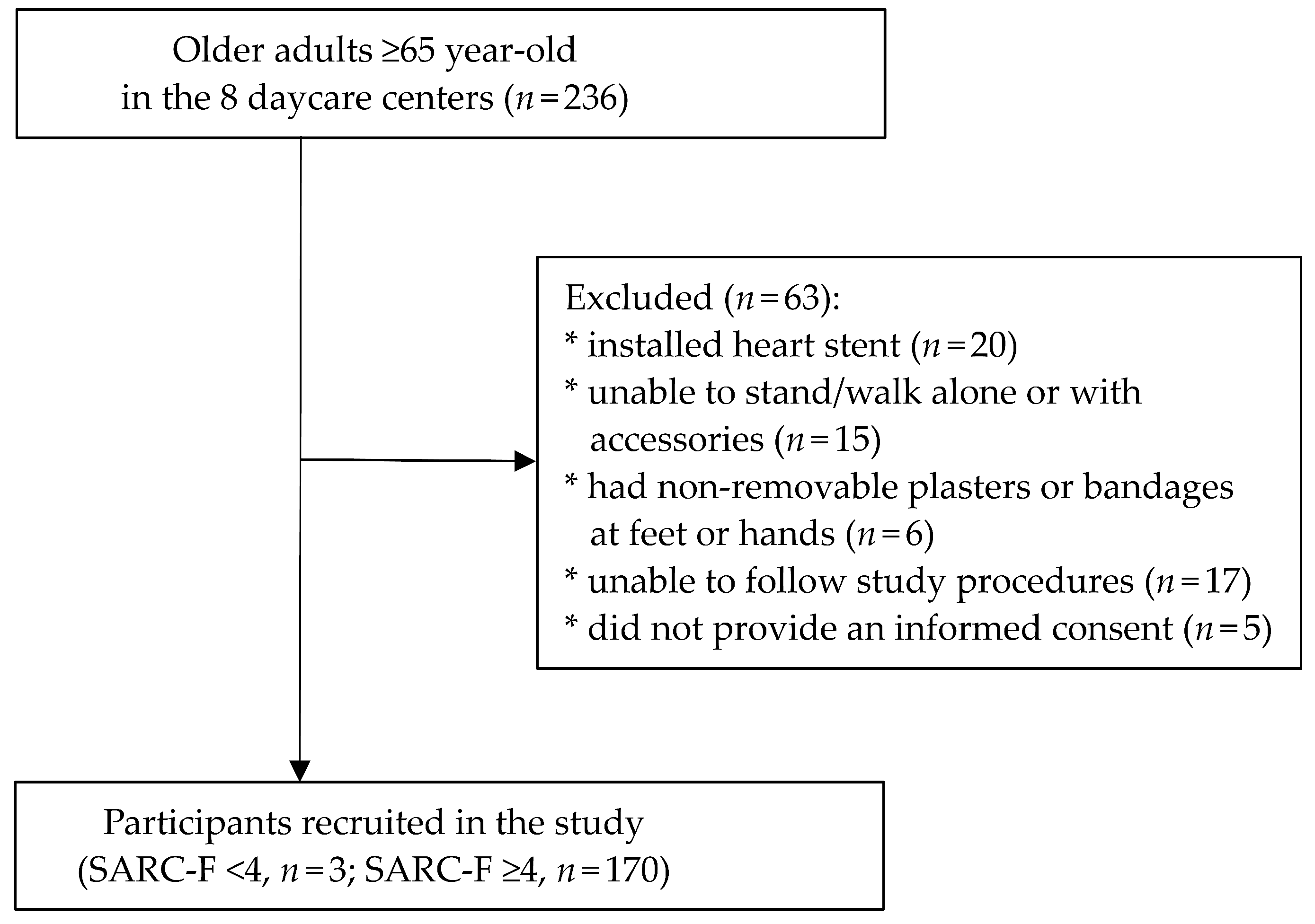
2.1. Study Design and Recruitment
2.2. Assessment of Sarcopenia
2.3. Assessment of Short Physical Performance Battery (SPPB) and Standing Balance
2.4. Assessment of Other Covariates Score
2.5. Statistical Analysis
3. Results
3.1. Demographic Characteristics
3.2. Prevalence of Possible and Confirmed Sarcopenia
3.3. Associated Parameters of Sarcopenia
3.4. Associated Parameters of Standing Balance
4. Discussion
4.1. Prevalence of Possible and Confirmed Sarcopenia
4.2. Associated Parameters of Confirmed Sarcopenia
4.3. Associated Parameters of Standing Balance
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sanchez-Rodriguez, D.; Hope, S.; Piotrowicz, K.; Benoit, F.; Czesak, J.; Dallmeier, D.; Decker, G.; De Spiegeleer, A.; Højmann, A.H.; Hrnciarikova, D.; et al. Sarcopenia in acute care patients: Protocol for the European collaboration of geriatric surveys: Sarcopenia 9+ EAMA Project. J. Am. Med. Dir. Assoc. 2019, 20, e1–e3. [Google Scholar] [CrossRef]
- Vrbova, P.; Smaha, J.; Stepan, J.; Tobias, D.; Kuzma, M.; Payer, J.; Koller, T. Prevalence of sarcopenia among hospitalized internal medicine patients: A cross-sectional single-center pilot study according to EWGSOP2 criteria. Bratisl. Lek. Listy. 2019, 120, 717–722. [Google Scholar] [CrossRef] [PubMed]
- Wu, C.H.; Chen, K.T.; Hou, M.T.; Chang, Y.F.; Chang, C.S.; Liu, P.Y.; Wu, S.J.; Chiu, C.J.; Jou, I.M.; Chen, C.Y. Prevalence and associated factors of sarcopenia and severe sarcopenia in older Taiwanese living in rural community: The Tianliao old people study 04. Geriatr. Gerontol. Int. 2014, 14, 69–75. [Google Scholar] [CrossRef] [Green Version]
- Moon, S.-S. Low skeletal muscle mass is associated with insulin resistance, diabetes, and metabolic syndrome in the Korean population: The Korea National Health and Nutrition Examination Survey (KNHANES) 2009–2010. Endocr. J. 2014, 61, 61–70. [Google Scholar] [CrossRef] [Green Version]
- Goodpaster, B.H.; Park, S.W.; Harris, T.B.; Kritchevsky, S.B.; Nevitt, M.; Schwartz, A.V.; Simonsick, E.M.; Tylavsky, F.A.; Visser, M.; Newman, A.B. The loss of skeletal muscle strength, mass, and quality in older adults: The health, aging and body composition study. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 1059–1064. [Google Scholar] [CrossRef] [PubMed]
- Patel, H.P.; Syddall, H.E.; Jameson, K.; Robinson, S.; Denison, H.; Roberts, H.C.; Edwards, M.; Dennison, E.; Cooper, C.; Aihie Sayer, A. Prevalence of sarcopenia in community-dwelling older people in the UK using the European Working Group on Sarcopenia in Older People (EWGSOP) definition: Findings from the Hertfordshire Cohort Study (HCS). Age Ageing 2013, 42, 378–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Magalhães, A.M.; Gomes, B.B.; Cerceau, D.M.; de Oliveira, G.V.; Parreiras de Menezes, K.K. Assessment of balance, gait, lower limb strength and functionality in sarcopenic and non-sarcopenic elderlies. MTP Rehabil. J. 2020, 18, 1–7. [Google Scholar] [CrossRef]
- Waters, D.L.; Baumgartner, R.N.; Garry, P.J.; Vellas, B. Advantages of dietary, exercise-related, and therapeutic interventions to prevent and treat sarcopenia in adult patients: An update. Clin. Interv. Aging 2010, 5, 259–270. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bertschi, D.; Kiss, C.M.; Beerli, N.; Kressig, R.W. Sarcopenia in hospitalized geriatric patients: Insights into prevalence and associated parameters using new EWGSOP2 guidelines. Eur. J. Clin. Nutr. 2021, 75, 653–660. [Google Scholar] [CrossRef]
- Baumgartner, R.N.; Koehler, K.M.; Gallagher, D.; Romero, L.; Heymsfield, S.B.; Ross, R.R.; Garry, P.J.; Lindeman, R.D. Epidemiology of sarcopenia among the elderly in New Mexico. Am. J. Epidemiol. 1998, 147, 755–763. [Google Scholar] [CrossRef] [PubMed]
- Senior, H.E.; Henwood, T.R.; Beller, E.M.; Mitchell, G.K.; Keogh, J.W. Prevalence and risk factors of sarcopenia among adults living in nursing homes. Maturitas 2015, 82, 418–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lovett, M.; Negm, A.; Ioannidis, G.; Petrucelli, D.; Winemaker, M.; Adachi, J.D.; Papaioannou, A. Identifying Patients with Osteoarthritis at Risk of Sarcopenia using the SARC-F. J. Geriatr. Cardiol. 2021, 24, 1–7. [Google Scholar] [CrossRef]
- Meng, N.H.; Li, C.I.; Liu, C.S.; Lin, C.H.; Lin, W.Y.; Chang, C.K.; Li, T.C.; Lin, C.C. Comparison of height- and weight-adjusted sarcopenia in a Taiwanese metropolitan older population. Geriatr. Gerontol. Int. 2015, 15, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Han, D.-S.; Chang, K.-V.; Li, C.-M.; Lin, Y.-H.; Kao, T.-W.; Tsai, K.-S.; Wang, T.-G.; Yang, W.-S. Skeletal muscle mass adjusted by height correlated better with muscular functions than that adjusted by body weight in defining sarcopenia. Sci. Rep. 2016, 6, 1–8. [Google Scholar] [CrossRef]
- Chen, Y.-P.; Wong, P.-K.; Tsai, M., Jr.; Chang, W.-C.; Hsieh, T.-S.; Leu, T.-H.; Jeff Lin, C.-F.; Lee, C.-H.; Kuo, Y.-J.; Lin, C.-Y. The high prevalence of sarcopenia and its associated outcomes following hip surgery in Taiwanese geriatric patients with a hip fracture. J. Formos. Med. Assoc. 2020, 119, 1807–1816. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307. [Google Scholar] [CrossRef]
- Office of Internal Affairs, Health, Welfare and Labor. Promote the 10-Year Long-Term Care Project 2.0. Available online: https://www.ey.gov.tw/Page/448DE008087A1971/aa69f5ba-4fc4-4825-9ba8-c93588dcbc86 (accessed on 29 September 2016).
- Fielding, R.A.; Vellas, B.; Evans, W.J.; Bhasin, S.; Morley, J.E.; Newman, A.B.; Abellan van Kan, G.; Andrieu, S.; Bauer, J.; Breuille, D.; et al. Sarcopenia: An undiagnosed condition in older adults. Current consensus definition: Prevalence, etiology, and consequences. International working group on sarcopenia. J. Am. Med. Dir. Assoc. 2011, 12, 249–256. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.; Park, K.S.; Yoo, J.I. Associations between the quality of life in sarcopenia measured with the SarQoL® and nutritional status. Health Qual. Life Outcomes 2021, 19, 1–7. [Google Scholar] [CrossRef]
- Casuso, R.A.; Huertas, J.R. The emerging role of skeletal muscle mitochondrial dynamics in exercise and ageing. Ageing Res. Rev. 2020, 58, 101025. [Google Scholar] [CrossRef]
- Kong, H.H.; Won, C.W.; Kim, W. Effect of sarcopenic obesity on deterioration of physical function in the elderly. Arch. Gerontol. Geriatr. 2020, 89, 104065. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.; Morley, J.E. Sarcopenia is recognized as an independent condition by an international classification of disease, Tenth Revision, Clinical Modification (ICD-10-CM) Code. J. Am. Med. Dir. Assoc. 2016, 17, 675–677. [Google Scholar] [CrossRef] [PubMed]
- Waite, S.J.; Maitland, S.; Thomas, A.; Yarnall, A.J. Sarcopenia and frailty in individuals with dementia: A systematic review. Arch. Gerontol. Geriatr. 2021, 92, 104268. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.-V.; Hsu, T.-H.; Wu, W.-T.; Huang, K.-C.; Han, D.-S. Is sarcopenia associated with depression? A systematic review and meta-analysis of observational studies. Age Ageing 2017, 46, 738–746. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnau, A.; Espaulella, J.; Méndez, T.; Serrarols, M.; Canudas, J.; Formiga, F.; Ferrer, M. Lower limb function and 10-year survival in population aged 75 years and older. Fam. Pract. 2016, 33, 10–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Treacy, D.; Hassett, L. The Short Physical Performance Battery. J. Physiother. 2018, 64, 61. [Google Scholar] [CrossRef]
- Guralnik, J.M.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef] [PubMed]
- National Health Service, Ministry of Health and Welfare. Taiwan Version Mini Nutritional Assessment Scale. Available online: https://dementiafc.tpech.gov.tw/Upload/Event/107091801%E9%A5%92%E6%9C%88%E5%A8%9F%E7%87%9F%E9%A4%8A%E5%B8%AB.pdf (accessed on 18 September 2018).
- Huang, C.-Y.; Hwang, A.-C.; Liu, L.-K.; Lee, W.-J.; Chen, L.-Y.; Peng, L.-N.; Lin, M.-H.; Chen, L.-K. Association of dynapenia, sarcopenia, and cognitive impairment among community-dwelling older Taiwanese. Rejuvenation Res. 2016, 19, 71–78. [Google Scholar] [CrossRef]
- Phu, S.; Kirk, B.; Bani Hassan, E.; Vogrin, S.; Zanker, J.; Bernardo, S.; Duque, G. The diagnostic value of the short physical performance battery for sarcopenia. BMC Geriatr. 2020, 20, 242. [Google Scholar] [CrossRef]
- Reiss, J.; Iglseder, B.; Alzner, R.; Mayr-Pirker, B.; Pirich, C.; Kässmann, H.; Kreutzer, M.; Dovjak, P.; Reiter, R. Consequences of applying the new EWGSOP2 guideline instead of the former EWGSOP guideline for sarcopenia case finding in older patients. Age Ageing 2019, 48, 719–724. [Google Scholar] [CrossRef]
- Ryu, M.; Jo, J.; Lee, Y.; Chung, Y.S.; Kim, K.M.; Baek, W.C. Association of physical activity with sarcopenia and sarcopenic obesity in community-dwelling older adults: The Fourth Korea National Health and Nutrition Examination Survey. Age Ageing 2013, 42, 734–740. [Google Scholar] [CrossRef] [Green Version]
- Flöter, A.; Nathorst-Böös, J.; Carlström, K.; Ohlsson, C.; Ringertz, H.; Schoultz, B. Effects of combined estrogen/testosterone therapy on bone and body composition in oophorectomized women. Gynecol. Endocrinol. 2005, 20, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Tu, S.; Chen, J. Sarcopenia. Fam. Med. Prim. Care 2017, 32, 154–159. [Google Scholar] [CrossRef]
- Maeda, K.; Koga, T.; Nasu, T.; Takaki, M.; Akagi, J. Predictiveaccuracy of calf circumference measurements to detect decreased skeletal muscle mass and European Society for clinical nutrition and metabolism-defined malnutrition in hospitalized older patients. Ann. Nutr. Metab. 2017, 71, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Ueshima, J.; Maeda, K.; Shimizu, A.; Inoue, T.; Murotani, K.; Mori, N.; Satake, S.; Matsui, Y.; Arai, H. Diagnostic accuracy of sarcopenia by “possible sarcopenia” premiered by the Asian Working Group for Sarcopenia 2019 definition. Arch. Gerontol. Geriatr. 2021, 97, 104484. [Google Scholar] [CrossRef]
- Landi, F.; Liperoti, R.; Fusco, D.; Mastropaolo, S.; Quattrociocchi, D.; Proia, A.; Russo, A.; Bernabei, R.; Onder, G. Prevalence and risk factors of sarcopenia among nursing home older residents. J. Gerontol. A 2011, 67, 48–55. [Google Scholar] [CrossRef] [Green Version]
- Zamboni, M.; Mazzali, G.; Fantin, F.; Rossi, A.; Di Francesco, V. Sarcopenic obesity: A new category of obesity in the elderly. Nutr. Metab. Cardiovasc. Dis. 2008, 18, 388–395. [Google Scholar] [CrossRef]
- Cheng, Q.; Zhu, X.; Zhang, X.; Li, H.; Du, Y.; Hong, W.; Xue, S.; Zhu, H. A cross-sectional study of loss of muscle mass corresponding to sarcopenia in healthy Chinese men and women: Reference values, prevalence, and association with bone mass. J. Bone. Miner. Metab. 2014, 32, 78–88. [Google Scholar] [CrossRef]
- De Cock, A.-M.; Perkisas, S.; Verhoeven, V.; Vandewoude, M.; Fransen, E.; Remmen, R. The impact of cognitive impairment on the physical ageing process. Aging Clin. Exp. Res. 2018, 30, 1297–1306. [Google Scholar] [CrossRef]
- Chang, K.-V.; Hsu, T.-H.; Wu, W.-T.; Huang, K.-C.; Han, D.-S. Association between sarcopenia and cognitive impairment: A systematic review and meta-analysis. J. Am. Med. Dir. Assoc. 2016, 17, 1164.e7–1164.e15. [Google Scholar] [CrossRef]
- Andrade-Moraes, C.H.; Oliveira-Pinto, A.V.; Castro-Fonseca, E.; da Silva, C.G.; Guimarães, D.M.; Szczupak, D.; Parente-Bruno, D.R.; Carvalho, L.R.; Polichiso, L.; Gomes, B.V.; et al. Cell number changes in Alzheimer’s disease relate to dementia, not to plaques and tangles. Brain 2013, 136, 3738–3752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maeda, K.; Akagi, J. Cognitive impairment is independently associated with definitive and possible sarcopenia in hospitalized older adults: The prevalence and impact of comorbidities. Geriatr. Gerontol. Int. 2017, 17, 1048–1056. [Google Scholar] [CrossRef]
- Herter, T.M.; Scott, S.H.; Dukelow, S.P. Systematic changes in position sense accompany normal aging across adulthood. J. Neuroeng. Rehabil. 2014, 11, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grönstedt, H.; Vikström, S.; Cederholm, T.; Franzén, E.; Seiger, Å.; Wimo, A.; Faxén-Irving, G.; Boström, A.-M. A study protocol of Older Person’s Exercise and Nutrition Study (OPEN)—a sit-to-stand activity combined with oral protein supplement—effects on physical function and independence: A cluster randomized clinical trial. BMC Geriatr. 2018, 18, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gadelha, A.B.; Neri, S.G.R.; Oliveira, R.J.; Bottaro, M.; David, A.C.; Vainshelboim, B.; Lima, R.M. Severity of sarcopenia is associated with postural balance and risk of falls in community-dwelling older women. Exp. Aging Res. 2018, 44, 258–269. [Google Scholar] [CrossRef]
- Yu, J. The etiology and exercise implications of sarcopenia in the elderly. Int. J. Nurs. Sci. 2015, 2, 199–203. [Google Scholar] [CrossRef] [Green Version]
- Viswanathan, A.; Sudarsky, L. Balance and gait problems in the elderly. Handb. Clin. Neurol. 2012, 103, 623–634. [Google Scholar] [CrossRef]
- Osoba, M.Y.; Rao, A.K.; Agrawal, S.K.; Lalwani, A.K. Balance and gait in the elderly: A contemporary review. Laryngoscope Investig. Otolaryngol. 2019, 4, 143–153. [Google Scholar] [CrossRef] [Green Version]
- Chronic Disease Prevention and Control Team, National Health Administration, Ministry of Health and Welfare. How serious is the problem of old adults falling? Available online: https://www.hpa.gov.tw/Pages/Detail.aspx?nodeid=807&pid=4326 (accessed on 14 November 2019).
- Figueiro, M.G.; Plitnick, B.; Rea, M.S.; Gras, L.Z.; Rea, M.S. Lighting and perceptual cues: Effects on gait measures of older adults at high and low risk for falls. BMC Geriatr. 2011, 11, 49. [Google Scholar] [CrossRef] [Green Version]
- Wolfson, L.; Judge, J.; Whipple, R.; King, M. Strength is a major factor in balance, gait, and the occurrence of falls. J. Gerontol. A Biol. Sci. Med. Sci. 1995, 50, 64–67. [Google Scholar] [CrossRef]
- Yang, M.; Hu, X.; Xie, L.; Zhang, L.; Zhou, J.; Lin, J.; Wang, Y.; Li, Y.; Han, Z.; Zhang, D.; et al. SARC-F for sarcopenia screening in community-dwelling older adults: Are 3 items enough? Medicine 2018, 97, e11726. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | All N = 170 | Male N = 42 (24.7%) | Female N = 128 (75.3%) | p-Value |
|---|---|---|---|---|
| General characteristic | ||||
| Age (years) | ||||
| 65–74 | 26 (15.3) | 10 (23.8) | 16 (12.5) | 0.005 |
| 75–84 | 77 (45.3) | 10 (23.8) | 67 (52.3) | |
| ≥85 | 67 (39.4) | 22 (52.4) | 45 (35.2) | |
| M ± SD | 81.6 ± 6.8 | 82 ± 7.7 | 81.4 ± 6.6 | 0.641 |
| BMI (kg/m2) | 48 (28.2) 55 (32.4) 67 (39.4) 23.3 ± 3.7 | 12 (28.6) 13 (31.0) 17 (40.5) 23.0 ± 3.0 | 36 (28.1) 42 (32.8) 50 (39.1) 23.4 ± 4.0 | |
| <21 | 0.974 | |||
| 21–24 | ||||
| ≥24 | ||||
| M ± SD | 0.564 | |||
| Calf circumference (cm) | 89 (52.4) 81 (47.6) 32.3 ± 3.2 | 22 (52.4) 20 (47.6) 33.2 ± 3.6 | 67 (52.3) 61 (47.7) 32.0 ± 3.0 | |
| <34 (33) for males (females) | 0.997 | |||
| ≥34 (33) for males (females) | ||||
| M ± SD | 0.036 | |||
| Duration of participation in daycare centers (m), M ± SD | 24.1 ± 17.8 | 21.2 ± 16.4 | 25.0 ± 18.2 | 0.228 |
| Comorbidities (n), M ± SD | 3.0 ± 1.7 | 3.2 ± 1.7 | 2.9 ± 1.7 | 0.303 |
| Hypertension | 89 (52.4) | 22 (52.4) | 67 (53.2) | 0.997 |
| Coronary heart disease | 50 (29.4) | 17 (40.5) | 33 (25.8) | 0.070 0.109 0.007 0.237 |
| Dementia | 95 (55.9) | 19 (45.2) | 76 (59.4) | |
| Stroke | 15 (8.9) | 8 (19.1) | 7 (5.5) | |
| Osteoporosis | 21 (12.5) | 3 (7.1) | 18 (14.1) | |
| Geriatric assessment parameters | ||||
| TW-MNA-SF(score) | ||||
| Normal (>11) | 134 (78.8) | 30 (71.4) | 104 (81.3) | 0.176 |
| At risk and malnutrition (≤11) | 36 (21.2) | 12 (28.6) | 24 (18.8) | |
| M ± SD | 12.5 ± 1.7 | 12.3 ± 1.6 | 12.6 ± 1.8 | 0.282 |
| SPPB | ||||
| Low SPPB score (≤9) | 163 (95.9) | 41 (97.6) | 122 (95.3) | 0.514 |
| Normal (>9) | 7 (4.1) | 1 (2.4) | 6 (4.7) | |
| M ± SD | 5.7 ± 2.2 | 5.4 ± 2.5 | 5.9± 2.1 | 0.300 |
| Balance (score), M ± SD | 2.6 ± 1.4 | 2.4 ± 1.6 | 2.7 ± 1.3 | 0.260 |
| 4 m GS, M ± SD | 13.0 ± 8.1 | 13.9 ± 10.2 | 12.7 ± 7.4 | 0.440 |
| 5-times sit to stand test (score) | ||||
| <12 | 5 (2.9) | 1 (2.4) | 4 (3.1) | 0.804 |
| ≥12 | 165 (97.1) | 41 (97.6) | 124 (96.9) | |
| M ± SD | 21.3± 11.3 | 23.8 ± 13.2 | 20.5 ± 10.5 | 0.104 |
| Sarcopenia index | 14.8 ± 6.5 0.4 ± 0.2 6.2 ±1.5 | 21.1 ± 6.4 0.4 ± 0.2 7.0 ± 1.7 | 12.7 ± 5.0 0.4 ± 0.2 5.9 ± 1.3 | |
| HGS (kg), M ± SD | <0.001 | |||
| GS (m/s), M ± SD | 0.905 | |||
| SMI (kg/m2), M ± SD | <0.001 |
| Prevalence of Sarcopenia | All N = 173 | Male N = 43 | Female N = 130 | p-Value |
|---|---|---|---|---|
| Sarcopenia Definition Criteria | ||||
| Low muscle strength, n (%) | 134 (77.5) | 34 (79.1) | 100 (76.9) | 0.770 |
| Low physical performance, n (%) | 168 (97.1) | 42 (97.7) | 126 (96.9) | 0.799 |
| Low muscle mass, n (%) | 88 (50.9) | 28 (65.1) | 60 (46.2) | 0.031 |
| Prevalence of sarcopenia | 0.025 0.031 0.145 | |||
| Possible sarcopenia, n (%) | 82 (47.4) | 14 (32.6) | 68 (52.3) | |
| 95% CI (%) | (40.1–54.8) | (4.9–13.1) | (32.3–46.7) | |
| Confirmed sarcopenia, n (%) | 88 (50.9) | 28 (65.1) | 60 (46.2) | |
| 95% CI (%) | (43.5–58.2) | (11.4–22.4) | (28.0–42.0) | |
| Severe sarcopenia 1, n (%) | 76 (43.9) | 23 (53.8) | 53 (40.8) | |
| 95% CI (%) | (36.8–51.4) | (9.0–19.2) | (24.3–37.9) |
| Parameter | n | OR | 95% CI | p-Value |
|---|---|---|---|---|
| Male | 43 | 3.09 | 1.19–7.98 | 0.020 |
| Age (year) | ||||
| 65–74 | 26 | 1.00 (ref) | - | - |
| 75–84 | 77 | 1.19 | 0.40–3.52 | 0.749 |
| ≥85 | 67 | 2.46 | 0.81–7.43 | 0.112 |
| BMI (kg/m2) | ||||
| <21 | 48 | 0.94 | 0.34–2.54 | 0.895 |
| 21–24 | 55 | 1.00 (ref) | - | - |
| ≥24 | 67 | 0.22 | 0.09–0.55 | 0.001 |
| Low c.c. 1 | 89 | 3.39 | 1.49–7.71 | 0.004 |
| At risk of malnutrition 2 | 36 | 5.65 | 1.96–16.31 | 0.001 |
| Low SPPB score (≤9) | 163 | 1.74 | 0.22–13.87 | 0.602 |
| Dementia | 97 | 2.31 | 1.05–5.04 | 0.036 |
| Parameter | n | B | 95% CI | p-Value |
|---|---|---|---|---|
| Male | 43 | −0.02 | −0.48 to 0.44 | 0.932 |
| Age (year) | ||||
| 65–74 | 26 | 1.00 (ref) | - | - |
| 75–84 | 77 | −0.05 | −0.62 to 0.52 | 0.856 |
| ≥85 | 67 | −0.08 | −0.67 to 0.51 | 0.792 |
| BMI (kg/m2) | ||||
| <21 | 48 | 0.03 | −0.48 to 0.54 | 0.909 |
| 21–24 | 55 | 1.00 (ref) | - | - |
| ≥24 | 67 | −0.78 | −1.26 to −0.30 | 0.002 |
| Low c.c.1 | 89 | −0.04 | −0.49 to 0.41 | 0.856 |
| At risk of malnutrition2 | 36 | 0.03 | −0.46 to 0.51 | 0.904 |
| 5-times sit to stand test (score) | 170 | −0.02 | −0.03 to 0.00 | 0.110 |
| 4m GS | 170 | −0.03 | −0.06 to −0.01 | 0.011 |
| Sarcopenia | 88 | −0.98 | −1.42 to −0.53 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, C.-F.; Yeh, Y.-L.; Chang, H.-Y.; Tsai, S.-H.; Wang, J.-Y. Prevalence and Risk Factors of Sarcopenia among Older Adults Aged ≥65 Years Admitted to Daycare Centers of Taiwan: Using AWGS 2019 Guidelines. Int. J. Environ. Res. Public Health 2021, 18, 8299. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168299
Chang C-F, Yeh Y-L, Chang H-Y, Tsai S-H, Wang J-Y. Prevalence and Risk Factors of Sarcopenia among Older Adults Aged ≥65 Years Admitted to Daycare Centers of Taiwan: Using AWGS 2019 Guidelines. International Journal of Environmental Research and Public Health. 2021; 18(16):8299. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168299
Chicago/Turabian StyleChang, Cheng-Fen, Yu-Lyu Yeh, Huang-Yu Chang, Sheng-Hua Tsai, and Jiun-Yi Wang. 2021. "Prevalence and Risk Factors of Sarcopenia among Older Adults Aged ≥65 Years Admitted to Daycare Centers of Taiwan: Using AWGS 2019 Guidelines" International Journal of Environmental Research and Public Health 18, no. 16: 8299. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18168299