
Eating Difficulties among Older Adults with Dementia in Long-Term Care Facilities: A Scoping Review

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Methodology
2.2. Research Question
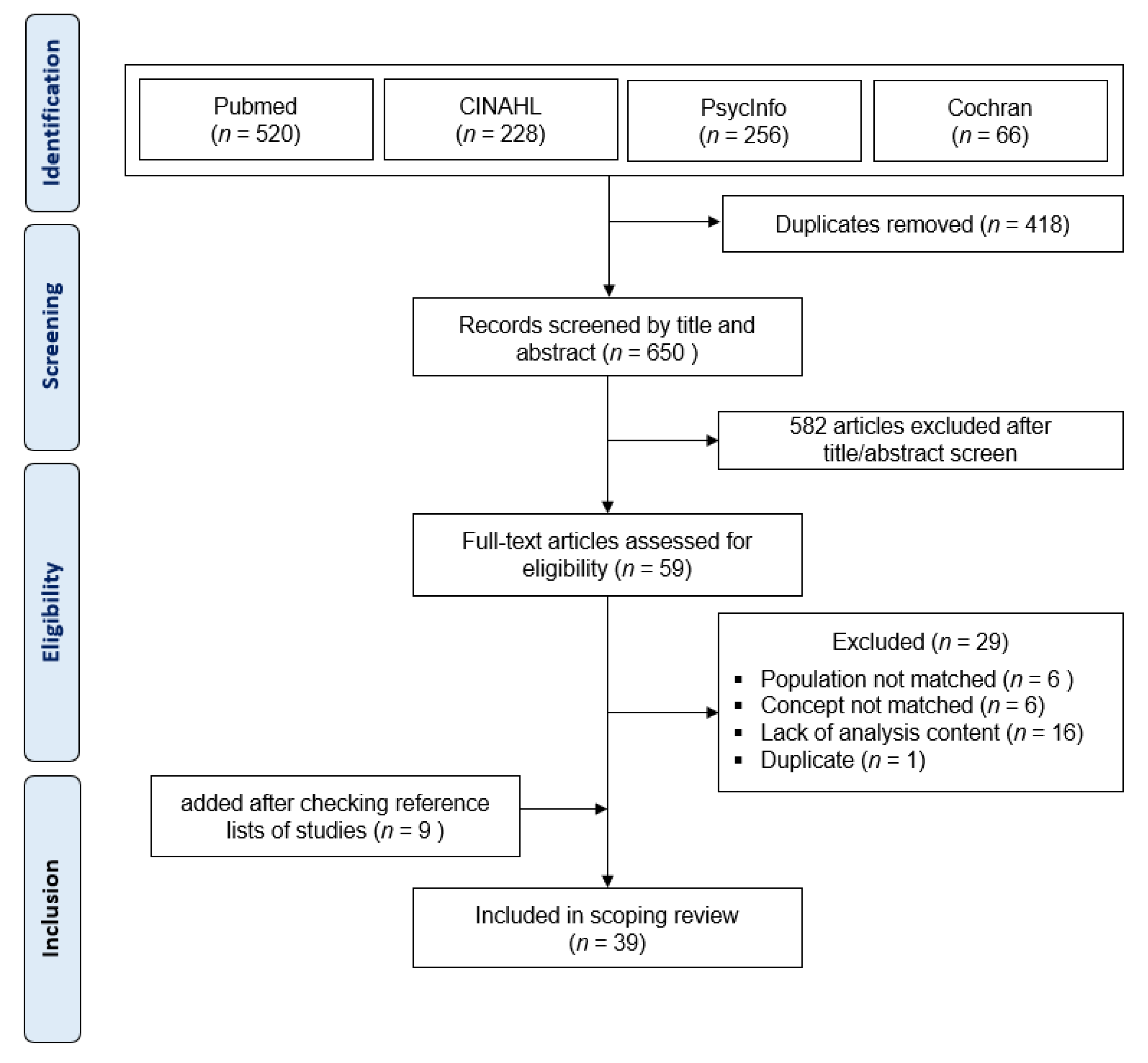
2.3. Search Strategy
2.4. Study Selection
- Incorporated contents were those related to the current research topic, including “eating disabilities”, “food intake difficulties”, “eating behavior difficulties”, “eating abnormality”, “eating disorder”, “eating difficulties”, “eating disturbance”, “mealtime behavioral challenges”, “poor food intake”, and “problem feeding behavior”;
- Participants were older adults (65 years or older) with dementia;
- Participants resided in long-term care facilities or nursing homes;
- Articles written in English.
2.5. Data Extraction
3. Results
3.1. Overview
3.2. Study Characteristics
3.3. The Concept of Feeding Difficulties
3.4. The Outcome Measurements
3.5. Interventions Related to Eating Behaviors in the Studies
3.6. Associated Factors
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization (WHO). Dementia. Available online: https://www.who.int/en/news-room/fact-sheets/detail/dementia (accessed on 23 December 2020).
- Arvanitakis, Z.; Shah, R.C.; Bennett, D.A. Diagnosis and Management of Dementia: Review. JAMA 2019, 322, 1589–1599. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Kim, K.H. Perceptions and Intention of Nurses in Using Physical Restraints for Dementia Patients in Geriatric Hospitals. J. Korean Gerontol. Nurs. 2016, 18, 159–171. [Google Scholar] [CrossRef]
- Health Insurance Review & Assessment Service. Analysis of Health Care Utilization of Dementia Patients. Available online: http://www.hira.or.kr/rc/icenter/study/getReportInfo.do?pgmid=HIRAA030095000000 (accessed on 7 December 2020).
- Houttekier, D.; Cohen, J.; Bilsen, J.; Addington-Hall, J.; Onwuteaka-Philipsen, B.D.; Deliens, L. Place of Death of Older Persons with Dementia: A Study in Five European Countries. J. Am. Geriatr. Soc. 2010, 58, 751–756. [Google Scholar] [CrossRef] [PubMed]
- Keller, H.H.; Carrier, N.; Slaughter, S.E.; Lengyel, C.; Steele, C.M.; Duizer, L.; Morrison, J.; Brown, K.S.; Chaudhury, H.; Yoon, M.N.; et al. Prevalence and Determinants of Poor Food Intake of Residents Living in Long-Term Care. J. Am. Med. Dir. Assoc. 2017, 18, 941–947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.M.; Song, J.A. Factors influencing the degree of eating ability among people with dementia. J. Clin. Nurs. 2015, 24, 1707–1717. [Google Scholar] [CrossRef]
- Liu, W.; Galik, E.; Boltz, M.; Nahm, E.S.; Lerner, N.; Resnick, B. Factors associated with eating performance for long-term care residents with moderate-to-severe cognitive impairment. J. Adv. Nurs. 2016, 72, 348–360. [Google Scholar] [CrossRef]
- Espinosa-Val, M.C.; Martín-Martínez, A.; Graupera, M.; Arias, O.; Elvira, A.; Cabré, M.; Palomera, E.; Bolívar-Prados, M.; Clavé, P.; Ortega, O. Prevalence, Risk Factors, and Complications of Oropharyngeal Dysphagia in Older Patients with Dementia. Nutrients 2020, 12, 863. [Google Scholar] [CrossRef] [Green Version]
- Murphy, J.L.; Holmes, J.; Brooks, C. Nutrition and dementia care: Developing an evidence-based model for nutritional care in nursing homes. BMC Geriatr. 2017, 17, 55. [Google Scholar] [CrossRef] [Green Version]
- Sakamoto, M.; Watanabe, Y.; Edahiro, A.; Motokawa, K.; Shirobe, M.; Hirano, H.; Ito, K.; Kanehisa, Y.; Yamada, R.; Yoshihara, A. Self-Feeding Ability as a Predictor of Mortality Japanese Nursing Home Residents: A Two-Year Longitudinal Study. J. Nutr. Health Aging 2019, 23, 157–164. [Google Scholar] [CrossRef]
- Batchelor-Murphy, M.; Kennerly, S.M.; Horn, S.D.; Barrett, R.; Bergstrom, N.; Boss, L.; Yap, T.L. Impact of Cognition and Handfeeding Assistance on Nutritional Intake for Nursing Home Residents. J. Nutr. Gerontol. Geriatr. 2019, 38, 262–276. [Google Scholar] [CrossRef]
- Cipriani, G.; Carlesi, C.; Lucetti, C.; Danti, S.; Nuti, A. Eating Behaviors and Dietary Changes in Patients with Dementia. Am. J. Alzheimers Dis. Other Demen. 2016, 31, 706–716. [Google Scholar] [CrossRef] [PubMed]
- Kai, K.; Hashimoto, M.; Amano, K.; Tanaka, H.; Fukuhara, R.; Ikeda, M. Relationship between Eating Disturbance and Dementia Severity in Patients with Alzheimer’s Disease. PLoS ONE 2015, 10, e0133666. [Google Scholar] [CrossRef] [PubMed]
- Batchelor-Murphy, M.; Amella, E.J.; Zapka, J.; Mueller, M.; Beck, C. Feasibility of a web-based dementia feeding skills training program for nursing home staff. Geriatr. Nurs. 2015, 36, 212–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, W.; Tripp-Reimer, T.; Williams, K.; Shaw, C. Facilitators and barriers to optimizing eating performance among cognitively impaired older adults: A qualitative study of nursing assistants’ perspectives. Dementia 2020, 19, 2090–2113. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef] [Green Version]
- Peters, M.D.J.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for conducting systematic scoping reviews. JBI Evid. Implement. 2015, 13, 141–146. [Google Scholar] [CrossRef] [Green Version]
- Colquhoun, H.L.; Levac, D.; O’Brien, K.K.; Straus, S.; Tricco, A.C.; Perrier, L.; Kastner, M.; Moher, D. Scoping reviews: Time for clarity in definition, methods, and reporting. J. Clin. Epidemiol. 2014, 67, 1291–1294. [Google Scholar] [CrossRef]
- Daudt, H.M.L.; van Mossel, C.; Scott, S.J. Enhancing the scoping study methodology: A large, inter-professional team’s experience with Arksey and O’Malley’s framework. BMC Med. Res. Methodol. 2013, 13, 48. [Google Scholar] [CrossRef] [Green Version]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated methodological guidance for the conduct of scoping reviews. JBI Evid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef]
- Chang, C.C.; Lin, L.C. Effects of a feeding skills training programme on nursing assistants and dementia patients. J. Clin. Nurs. 2005, 14, 1185–1192. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.C.; Wykle, M.L.; Madigan, E.A. The effect of a feeding skills training program for nursing assistants who feed dementia patients in Taiwanese nursing homes. Geriatr. Nurs. 2006, 27, 229–237. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.C.; Huang, Y.J.; Su, S.G.; Watson, R.; Tsai, B.W.J.; Wu, S.C. Using spaced retrieval and Montessori-based activities in improving eating ability for residents with dementia. Int. J. Geriatr. Psychiatry 2010, 25, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.C.; Huang, Y.J.; Watson, R.; Wu, S.C.; Lee, Y.C. Using a Montessori method to increase eating ability for institutionalised residents with dementia: A crossover design. J. Clin. Nurs. 2011, 20, 3092–3101. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.S.; Lin, L.C.; Su, S.C.; Wu, S.C. The effects of spaced retrieval combined with errorless learning in institutionalized elders with dementia: Recall performance, cognitive status, and food intake. Alzheimer Dis. Assoc. Disord. 2014, 28, 333–339. [Google Scholar] [CrossRef]
- Wu, H.S.; Lin, L.C.; Wu, S.C.; Lin, K.N.; Liu, H.C. The effectiveness of spaced retrieval combined with Montessori-based activities in improving the eating ability of residents with dementia. J. Adv. Nurs. 2014, 70, 1891–1901. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.N.; Lin, L.C.; Wu, S.C. The effects of spaced retrieval training in improving hyperphagia of people living with dementia in residential settings. J. Clin. Nurs. 2017, 26, 3224–3231. [Google Scholar] [CrossRef]
- Durnbaugh, T.; Haley, B.; Roberts, S. Assessing problem feeding behaviors in mid-stage Alzheimer’s disease: Clients with mid-stage Alzheimer’s disease may be eating far less than their caregivers believe. Geriatr. Nurs. 1996, 17, 63–67. [Google Scholar] [CrossRef]
- Berkhout, A.M.; Cools, H.J.; Van Houwelingen, H.C. The relationship between difficulties in feeding oneself and loss of weight in nursing-home patients with dementia. Age Ageing 1998, 27, 637–641. [Google Scholar] [CrossRef] [Green Version]
- Amelia, E.J. Factors influencing the proportion of food consumed by nursing home residents with dementia. J. Am. Geriatr. Soc. 1999, 47, 879–885. [Google Scholar] [CrossRef]
- Amella, E.J. Resistance at mealtimes for persons with dementia. J. Nutr. Health Aging 2002, 6, 117–122. [Google Scholar]
- Reed, P.S.; Zimmerman, S.; Sloane, P.D.; Williams, C.S.; Boustani, M. Characteristics associated with low food and fluid intake in long-term care residents with dementia. Gerontologist 2005, 45, 74–80. [Google Scholar] [CrossRef]
- Lin, L.C.; Watson, R.; Wu, S.C. What is associated with low food intake in older people with dementia? J. Clin. Nurs. 2010, 19, 53–59. [Google Scholar] [CrossRef]
- Slaughter, S.E.; Eliasziw, M.; Morgan, D.; Drummond, N. Incidence and predictors of eating disability among nursing home residents with middle-stage dementia. Clin. Nutr. 2011, 30, 172–177. [Google Scholar] [CrossRef]
- Chang, C.C. Prevalence and factors associated with feeding difficulty in institutionalized elderly with dementia in Taiwan. J. Nutr. Health Aging 2012, 16, 258–261. [Google Scholar] [CrossRef] [PubMed]
- Edahiro, A.; Hirano, H.; Yamada, R.; Chiba, Y.; Watanabe, Y.; Tonogi, M.; Yamane, G.Y. Factors affecting independence in eating among elderly with Alzheimer’s disease. Geriatr. Gerontol. Int. 2012, 12, 481–490. [Google Scholar] [CrossRef]
- Hanson, L.C.; Ersek, M.; Lin, F.C.; Carey, T.S. Outcomes of feeding problems in advanced dementia in a nursing home population. J. Am. Geriatr. Soc. 2013, 61, 1692–1697. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.S. Predictors of hyperphagia in institutionalized patients with dementia. J. Nurs. Res. 2014, 22, 250–258. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.-C.; Lin, Y.-F.; Chiu, C.-H.; Liao, Y.-M.; Ho, M.-H.; Lin, Y.-K.; Chou, K.-R.; Liu, M.F. Prevalence and factors associated with food intake difficulties among residents with dementia. PLoS ONE 2017, 12, 1–14. [Google Scholar] [CrossRef]
- Pérez-Sánchez, C.M.; Torres, D.N.; Morante, J.J.H. Altered eating attitudes in nursing home residents and its relationship with their cognitive and nutritional status. J. Nutr. Health Aging 2018, 22, 869–875. [Google Scholar] [CrossRef]
- Liu, W.; Jao, Y.L.; Williams, K. Factors influencing the pace of food intake for nursing home residents with dementia: Resident characteristics, staff mealtime assistance and environmental stimulation. Nurs. Open 2019, 6, 772–782. [Google Scholar] [CrossRef] [Green Version]
- Palese, A.; Gonella, S.; Grassetti, L.; Longobardi, M.; De Caro, A.; Achil, I.; Hayter, M.; Watson, R. What nursing home environment can maximise eating independence among residents with cognitive impairment? Findings from a secondary analysis. Geriatr. Nurs. 2020, 41, 709–716. [Google Scholar] [CrossRef] [PubMed]
- Athlin, E.; Norberg, A.; Asplund, K.; Jansson, L. Feeding problems in severely demented patients seen from task and relationship aspects. Scand. J. Caring Sci. 1989, 3, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.C.; Roberts, B.L. Cultural perspectives in feeding difficulty in Taiwanese elderly with dementia. J. Nurs. Sch. 2008, 40, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Shinagawa, S.; Honda, K.; Kashibayashi, T.; Shigenobu, K.; Nakayama, K.; Ikeda, M. Classifying eating-related problems among institutionalized people with dementia. Psychiatry Clin. Neurosci. 2016, 70, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Jung, D.; De Gagne, J.C.; Lee, M.; Lee, H.; Lee, K.; Choi, E.; Chung, J. Feasibility of a Mobile Meal Assistance Program for Direct Care Workers in Long-Term Care Facilities in South Korea. Clin. Interv. Aging 2020, 15, 2019–2029. [Google Scholar] [CrossRef] [PubMed]
- Keller, H.H.; Gibbs-Ward, A.; Randall-Simpson, J.; Bocock, M.A.; Dimou, E. Meal rounds: An essential aspect of quality nutrition services in long-term care. J. Am. Med. Dir. Assoc. 2006, 7, 40–45. [Google Scholar] [CrossRef]
- Cleary, S. Current approaches to managing feeding and swallowing disorders for residents with dementia. Can. Nurs. Home 2007, 18, 11–16. [Google Scholar]
- Aselage, M.B.; Amella, E.J.; Watson, R. State of the science: Alleviating mealtime difficulties in nursing home residents with dementia. Nurs. Outlook 2011, 59, 210–214. [Google Scholar] [CrossRef]
- Chang, C.C.; Roberts, B.L. Strategies for feeding patients with dementia. Am. J. Nurs. 2011, 111, 36–44. [Google Scholar] [CrossRef]
- Cole, D. Optimising nutrition for older people with dementia. Nurs. Stand. 2012, 26, 41–48. [Google Scholar] [CrossRef]
- Chang, C.C.; Roberts, B.L. Feeding difficulty in older adults with dementia. J. Clin. Nurs. 2008, 17, 2266–2274. [Google Scholar] [CrossRef]
- Liu, W.; Cheon, J.; Thomas, S.A. Interventions on mealtime difficulties in older adults with dementia: A systematic review. Int. J. Nurs. Stud. 2014, 51, 14–27. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Galik, E.; Boltz, M.; Nahm, E.S.; Resnick, B. Optimizing Eating Performance for Older Adults with Dementia Living in Long-term Care: A Systematic Review. Worldviews Evid. Based. Nurs. 2015, 12, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Fetherstonhaugh, D.; Haesler, E.; Bauer, M. Promoting mealtime function in people with dementia: A systematic review of studies undertaken in residential aged care. Int. J. Nurs. Stud. 2019, 96, 99–118. [Google Scholar] [CrossRef] [PubMed]
- Palese, A.; Bressan, V.; Hayter, M.; Watson, R. Enhancing independent eating among older adults with dementia: A scoping review of the state of the conceptual and research literature. BMC Nurs. 2020, 19, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Watson, R. Measuring feeding difficulty in patients with dementia: Replication and validation of the EdFED Scale #1. J. Adv. Nurs. 1994, 19, 850–855. [Google Scholar] [CrossRef]
- Watson, R. Measuring feeding difficulty in patients with dementia: Developing a scale. J. Adv. Nurs. 1994, 19, 257–263. [Google Scholar] [CrossRef]
- Watson, R. The Mokken scaling procedure (MSP) applied to the measurement of feeding difficulty in elderly people with dementia. Int. J. Nurs. Stud. 1996, 33, 385–393. [Google Scholar] [CrossRef]
- Watson, R.; Deary, I.J. Measuring feeding difficulty in patients with dementia: Multivariate analysis of feeding problems, nursing intervention and indicators of feeding difficulty. J. Adv. Nurs. 1994, 20, 283–287. [Google Scholar] [CrossRef]
- Watson, R.; Deary, I.J. Feeding difficulty in elderly patients with dementia: Confirmatory factor analysis. Int. J. Nurs. Stud. 1997, 34, 405–414. [Google Scholar] [CrossRef]
- Watson, R.; Green, S.M.; Legg, L. The Edinburgh Feeding Evaluation in Dementia Scale #2 (EdFED #2): Convergent and discriminant validity. Clin. Eff. Nurs. 2001, 5, 44–46. [Google Scholar] [CrossRef]
- Watson, R.; MacDonald, J.; McReady, T. The Edinburgh Feeding Evaluation in Dementia Scale #2 (EdFED #2): Inter- and intra-rater reliability. Clin. Eff. Nurs. 2001, 5, 184–186. [Google Scholar] [CrossRef]
- Lin, L.-C.; Chang, C.-C. A Chinese Translation of the EdFED-Q and Assessment of Equivalence. Alzheimer Dis. Assoc. Disord 2003, 17, 230–235. [Google Scholar] [CrossRef]
- Bagnasco, A.; Watson, R.; Zanini, M.; Rosa, F.; Rocco, G.; Sasso, L. Preliminary testing using Mokken scaling of an Italian translation of the Edinburgh Feeding Evaluation in Dementia (EdFED-I) scale. Appl. Nurs. Res. 2015, 28, 391–396. [Google Scholar] [CrossRef] [PubMed]
- Tully, M.W.; Matrakas, K.L.; Muir, J.; Musallam, K. The Eating Behavior Scale: A simple method of assessing functional ability in patients with alzheimer’s disease. J. Gerontol. Nurs. 1997, 23, 9. [Google Scholar] [CrossRef] [PubMed]
- Dox, I.G.; Melloni, B.J.; Eisner, G.M.; Melloni, J.L. Melloni’s Illustrated Medical Dictionary; CRC Press: Boca Raton, FL, USA, 2001. [Google Scholar]
- Watson, R. Measuring feeding difficulty in patients with dementia: Perspectives and problems. J. Adv. Nurs. 1993, 18, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Camp, C.J. From efficacy to effectiveness to diffusion: Making the transitions in dementia intervention research. Neuropsychol. Rehabil. 2001, 11, 495–517. [Google Scholar] [CrossRef]
- Baddeley, A.; Wilson, B.A. When implicit learning fails: Amnesia and the problem of error elimination. Neuropsychologia 1994, 32, 53–68. [Google Scholar] [CrossRef]
- Grandmaison, E.; Simard, M. A Critical Review of Memory Stimulation Programs in Alzheimer’s Disease. J. Neuropsych. Clin. Neurosci. 2003, 15, 130–144. [Google Scholar] [CrossRef]
- Cherid, C.; Baghdadli, A.; Wall, M.; Mayo, N.E.; Berry, G.; Harvey, E.J.; Albers, A.; Bergeron, S.G.; Morin, S.N. Current level of technology use, health and eHealth literacy in older Canadians with a recent fracture—A survey in orthopedic clinics. Osteoporos. Int. 2020, 31, 1333–1340. [Google Scholar] [CrossRef] [PubMed]
- Kong, E.-H.; Jeong, Y.-S. The effects of a dementia education program for the aged. J. Korean Acad. Commun. Health Nurs. 2011, 22, 252–261. [Google Scholar] [CrossRef]
- Mamary, E.M.; Charles, P. On-site to on-line: Barriers to the use of computers for continuing education. J. Contin. Educ. Health Prof. 2000, 20, 171–175. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.-L.; Li, H.; Lin, R.; Zheng, J.-H.; Wei, Y.-P.; Li, J.; Chen, P.; Chen, H.-Y. Effects of a feeding intervention in patients with Alzheimer’s disease and dysphagia. J. Clin. Nurs. 2016, 25, 699–707. [Google Scholar] [CrossRef] [PubMed]
- Bronfenbrenner, U. Ecological systems theory. In Six Theories of Child Development: Revised Formulations and Current issues; Jessica Kingsley Publishers: London, UK, 1992; pp. 187–249. [Google Scholar]
- Topo, P.; Kotilainen, H.; Eloniemi-Sulkava, U. Affordances of the Care Environment for People with Dementia—An Assessment Study. HERD 2012, 5, 118–138. [Google Scholar] [CrossRef]
- Liu, W.; Jao, Y.-L.; Williams, K. The association of eating performance and environmental stimulation among older adults with dementia in nursing homes: A secondary analysis. Int. J. Nurs. Stud. 2017, 71, 70–79. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.H.; Choi, G.Y.; Lee, J. Impact of Nurse Staffing, Skill Mix and Stability on Resident Health Outcomes in Korean Nursing Homes. J. Korean Gerontol. Nurs. 2020, 22, 29. [Google Scholar] [CrossRef]


{kind=link}
| Design | Author(s) (Reference Number) | Country | Aims | Population | Outcome Measurements |
|---|---|---|---|---|---|
| Batchelor-Murphy et al. [15] | USA | To evaluate the feasibility of a web-based dementia feeding skills training program for nursing home staff | ▪ 7 nursing assistant–dementia patient dyads -exp. (n = 4) -cont. (n = 3) | ▪ EdFED ▪ Time spent providing meal assistance ▪ Meal intake | |
| Intervention study | Chang et al. [23] | Taiwan | To evaluate the effectiveness of a feeding skills training program for nursing assistants | ▪ 67 nursing assistants -exp. (n = 31) -cont. (n = 36) ▪ 36 nursing assistant–dementia patient dyads -exp. (n = 20) -cont. (n = 16) | ▪ The Formal Caregivers’ Knowledge of Feeding Dementia Patient Questionnaire ▪ The Formal Caregivers’ Attitude toward Feeding Dementia Patient Questionnaire ▪ The Formal Caregivers’ Behaviors toward Feeding ▪ EdFED ▪ Total eating time ▪ Food intake |
| Chang et al. [24] | Taiwan | To evaluate the effectiveness of a feeding skills training program for nursing assistants | ▪ 67 nursing assistants -exp. (n = 31) -cont. (n = 36) ▪ 36 nursing assistant–dementia patient dyads -exp. (n = 20) -cont. (n = 16) | ▪ The Formal Caregivers’ Knowledge of Feeding Dementia Patients Questionnaire ▪ The Formal Caregivers’ Attitude toward Feeding Dementia Patients Questionnaire ▪ The Perceived Behavior Control Scale ▪ The Intention Scale ▪ The Formal Caregivers’ Behaviors in Feeding Dementia Patients Observation Checklist ▪ Feeding during mealtime was observed | |
| Lin et al. [25] | Taiwan | To evaluate the effectiveness of a training protocol (Spaced Retrieval and Montessori-based activities) in decreasing eating difficulty | ▪ 85 residents with dementia -exp. (SR) (n = 32) -exp. (Montessori) (n = 29) -cont. (n = 24) | ▪ Chinese version of EdFED ▪ MNA (Mini-nutritional assessment) ▪ Observation (Eating time, Eating amount, Residents fed by caregivers, Physical assistance, Verbal assistance) | |
| Lin et al. [26] | Taiwan | To evaluate the effectiveness of a Montessori intervention for improving eating ability and nutritional status | ▪ 29 residents with dementia -Montessori intervention sequence I (n = 15) -Montessori intervention sequence II (n = 14) | ▪ Chinese version of EdFED ▪ EBS ▪ MNA ▪ Observation (Self-feeding frequency, Self-feeding time, Verbal assistance, Physical assistance, Residents fed by caregivers) | |
| Wu et al. [27] | Taiwan | To evaluate the long-term effects of the standardized and individualized spaced retrieval combined with Montessori-based activities on eating ability | ▪ 61 residents with dementia -exp. (SR/EL group) (n = 32) -cont. (SR-only group) (n = 29) | ▪ The proportion of each meal consumed | |
| Wu et al. [28] | Taiwan | To evaluate the effects of using accumulating cues in a spaced retrieval paradigm on recall performance, cognitive status, and food intake | ▪ 90 residents with dementia -exp. (Montessori-based group) (n = 25) -exp. (Individualized group) (n = 38) -cont. (n = 27) | ▪ Chinese version of EdFED ▪ Eating amount ▪ Body weight | |
| Hsu et al. [29] | Taiwan | To evaluate the effectiveness of spaced retrieval for improving hyperphagia | ▪ 97 residents with dementia -exp. (n = 50) -cont. (n = 47) | ▪ Dementia Hyperphagic Behavior Scale ▪ Food intake ▪ BMI | |
| Observational study | Lee et al. [7] | Korea | To investigate factors associated with eating ability | ▪ 149 residents with dementia | ▪ MMSE-K ▪ Korean activities of daily living scale ▪ Eating Behavior Scale |
| Liu et al. [8] | USA | To investigate the association between specific personal and environmental factors and eating performance | ▪ 199 residents with dementia | ▪ Using the single self-care ‘feeding’ item in the Barthel Index ▪ MMSE ▪ Using the single ‘chair sit-sitting balance’ item in the Tinetti Gait and Balance scale ▪ Physical Capability Scale (PCS) ▪ Cornell Scale for Depression in Dementia (CSDD) ▪ Cohen-Mansfield Agitation Inventory-short form (CMAI) | |
| Durnbaugh et al. [30] | USA | To present the Feeding Behaviors Inventory, an instrument designed to identify common mealtime feeding behaviors | ▪ 20 residents with dementia | ▪ Feeding behaviors inventory | |
| Berkhout et al. [31] | Netherlands | To investigate the cause of weight loss in nursing-home patients with dementia | ▪ 514 residents above 65 years in nursing home -existing residents: (n = 250) -newly admitted: (n = 264) | ▪ Nurses recorded the most important difficulties in self-feeding (choosing food, bringing food to the mouth, chewing, and swallowing) | |
| Amella [32] | USA | To predict how the quality of the interaction between care giver and care receiver influenced the proportion of food consumed | ▪ 53 residents with late-stage dementia. | ▪ Proportion of food consumed (weighing) | |
| Amella [33] | USA | To investigate factors regarding resistance behavior at meals | ▪ 53 residents with dementia -resistors (n = 23) -acceptors (n = 30) | ▪ EdFED-Q ▪ BMI ▪ Proportion of food consumed (weighing) ▪ Time taken to assist with meals | |
| Reed et al. [34] | USA | To investigate factors associated with low food and fluid intake | ▪ 421 residents with dementia | ▪ The Structured Meal Observations (SMO) | |
| Lin et al. [35] | Taiwan | To investigate the risk factors of low food intake | ▪ 177 residents with dementia in LTC | ▪ Chinese version of EdFED ▪ BMI | |
| Slaughter et al. [36] | Canada | To estimate the incidence and identify the predictors of eating disability due to dementia | ▪ 120 nursing home residents | ▪ Researchers observed residents’ loss of eating ability during meals; eating disability was defined as receiving physical assistance to put food into the mouth or not eating at all | |
| Chang et al. [37] | Taiwan | To investigate factors associated with feeding difficulty of individuals with dementia | ▪ 93 residents with dementia | ▪ Chinese version of EdFED | |
| Edahiro et al. [38] | Japan | To investigate factors affecting self-feeding | ▪ 150 Alzheimer’s disease patients who were hospitalized in dementia ward | ▪ Feeding Cycle Recording ▪ Eating-related BPSD item | |
| Hanson et al. [39] | USA | To describe quality of care for feeding problems in residents with advanced dementia, and probability and predictors of weight loss and mortality. | ▪ 256 residents with dementia | ▪ Quality of feeding assistance provided by staff ▪ Body weight loss ▪ Mortality | |
| Wu [40] | Taiwan | To explore the prevalence and predictors of hyperphagic behaviors | ▪ 179 residents with dementia | ▪ Hyperphagia questionnaire ▪ Cognitive abilities screening instrument ▪ Cohen-Mansfield agitation inventory ▪ Demographic characteristics | |
| Chang et al. [41] | Taiwan | To identify the best cutoff point for the Chinese Feeding Difficulty Index (Ch-FDI) and factors associated with eating behaviors | ▪ 213 residents with dementia | ▪ Chinese Feeding Difficulty Index ▪ EdFED | |
| Maria Perez-Sanchez et al. [42] | Spain | To evaluate the relation between altered eating behaviors/attitudes and nutritional status | ▪ 139 residents with severe cognitive impairment | ▪ The Blanford’s Aversive Feeding Behaviors Inventory ▪ The 26-item Eating Attitudes Test ▪ Dietary intake ▪ MNA | |
| Liu et al. [43] | USA | To examine the association of resident characteristics, staff mealtime assistance, and environmental stimulation with the pace of food intake | ▪ 19 NA and 15 residents with dementia | ▪ The pace of food intake recorded on video ▪ Level of Eating Independence (LEI) scale ▪ Staff mealtime assistance recorded on video | |
| Palese et al. [44] | Italy | To explore the influence of nursing home environment on eating independence | ▪ 1027 residents with dementia | ▪ Italian-validated version of EdFED | |
| Qualitative study | Athlin et al. [45] | Sweden | To understand feeding problems in patients with severe dementia cared for in a task assignment system | ▪ 15 patients with severe dementia and 45 caregivers who fed the 15 patients during the study period | ▪ Researchers analyzed video-recorded meals for patients with severe dementia and interviews with caregivers who assist them. |
| Mixed methods | Chang et al. [46] | Taiwan | To investigate factors related to feeding difficulty that are shown in the interaction between nursing assistants and residents | ▪ 48 residents with dementia and 31 nursing assistants | ▪ Chinese version of EdFED ▪ Nursing assistant interview about feeding dementia residents |
| Shinagawa et al. [47] | Japan | To develop a possible classification of eating-related problems | ▪ 208 residents and patients | ▪ Semi-structured systematic interviews with nurses stationed on Eating and Swallowing ▪ Mini-Mental State Examination (MMSE) ▪ Clinical Dementia Rating (CDR) ▪ Neuropsychiatric Inventory (NPI) | |
| Jung et al. [48] | Korea | To assess the feasibility and examine the preliminary effectiveness of a mobile application-based meal assistant training program for use by direct care workers | ▪ 23 older adults with dementia-caregiver dyads | ▪ Eating behavior scale (EBS) | |
| Literature review | Keller et al. [49] | To present meal rounds as a potential intervention for identifying nutrition problems and specifically feeding, food texture, and mealtime behaviors. | ▪ A previously published study on 37 residents | N/A | |
| Cleary [50] | Canada | To review the current approaches to manage feeding and swallowing disorders | N/A | N/A | |
| Aselage et al. [51] | USA, UK, Australia | To explore the state of mealtime difficulties; characteristics, measurements, related factors, and interventions for alleviating mealtime difficulties | N/A | N/A | |
| Chang et al. [52] | Taiwan, USA | To propose strategies for feeding patients that caregivers can use | N/A | N/A | |
| Cole [53] | USA | To explore interventions that can be undertaken to establish and maintain adequate nutritional intake | ▪ 12 articles | N/A | |
| Systematic review | Chang et al. [54] | Taiwan | To use concept analysis to identify characteristics of feeding difficulty and its antecedents and consequences that provide direction for assessment and management | ▪ 71 articles | N/A |
| Liu et al. [55] | USA | To evaluate the effectiveness of interventions on mealtime difficulties | ▪ 22 intervention studies -2082 residents with dementia -95 professionals -85 long-term care facilities | N/A | |
| Liu et al. [56] | USA | To evaluate the effectiveness of interventions on eating performance | ▪ 11 articles | N/A | |
| Fetherstonhaugh et al. [57] | Australia | To review the literature on strategies for promoting mealtime function in people with dementia living in residential aged care facilities and assess their effectiveness | ▪ 20 articles | N/A | |
| Scoping review | Palese et al. [58] | Italy, UK | To map the state of the research designed to maintain and/or promote independent eating | ▪ 17 articles | N/A |
| Variables | Categories | n | Reference No. |
|---|---|---|---|
| Participants | Caregiver | 5 | [15,23,24,46,48] |
| Older adults with dementia | 5 | [15,25,26,27,28] | |
| Intervention type | Spaced retrieval (SR) training | 2 | [25] 1, [29] |
| Montessori | 2 | [25] 1, [26] | |
| Combined with SR | 2 | [27,28] | |
| Feeding skills training | 3 | [23,24,46] | |
| Online-based dementia feeding skills training (Web, Mobile) | 2 | [15,48] | |
| Sample size | ≤50 persons | 3 | [15,26,48] |
| 51−100 persons | 5 | [25,27,28,29,46] | |
| >100 persons | 2 | [23,24] | |
| Intervention length per session | ≤60 min | 5 | [15,25,26,27,28] |
| >60 min | 4 | [15,23,24,48] | |
| Intervention duration | <8 weeks | 4 | [23,24,29,48] |
| ≥8 weeks | 5 | [15,25,26,27,28] |
| Variable | Categories | n | Reference No. |
|---|---|---|---|
| Intrapersonal 1 | Age | 2 | [35] |
| Gender | 2 | [35,44] | |
| Comorbidities | 1 | [36] | |
| Duration of illness (dementia) | 1 | [7] | |
| Presence of dysphagia signs | 1 | [38] | |
| Number of medications | 1 | [37] | |
| Period of institutionalization | 2 | [7,40] | |
| Cognitive function | 7 | [7,8,36,37,38,39,42] | |
| Physical function | 4 | [7,8,35,37] | |
| Interpersonal 1 | Close relationship with family | 2 | [35,44] |
| Caregiver assistant | 1 | [43] | |
| Environmental 1 | Diet type | 1 | [7] |
| Eating place | 2 | [7,34] | |
| Presence of staff | 3 | [7,34,35] | |
| Length of the eating time | 1 | [41] | |
| Eating with other residents | 1 | [44] | |
| Physical (tablecloth, illuminance level, sound volume level, etc.) | 4 | [34,41,43,44] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, D.; Lee, K.; De Gagne, J.C.; Lee, M.; Lee, H.; Yoo, L.; Won, S.; Choi, E. Eating Difficulties among Older Adults with Dementia in Long-Term Care Facilities: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 10109. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910109
Jung D, Lee K, De Gagne JC, Lee M, Lee H, Yoo L, Won S, Choi E. Eating Difficulties among Older Adults with Dementia in Long-Term Care Facilities: A Scoping Review. International Journal of Environmental Research and Public Health. 2021; 18(19):10109. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910109
Chicago/Turabian StyleJung, Dukyoo, Kyuri Lee, Jennie C. De Gagne, Minkyung Lee, Hyesoon Lee, Leeho Yoo, Sarah Won, and Eunju Choi. 2021. "Eating Difficulties among Older Adults with Dementia in Long-Term Care Facilities: A Scoping Review" International Journal of Environmental Research and Public Health 18, no. 19: 10109. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910109