
The Relationship between Online and Offline Information-Seeking Behaviors for Healthy Nutrition

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sampling Procedure and Method of Data Recording
2.2. Sociodemographic Background of the Sample
2.3. Adapted Models
2.3.1. Importance of Online and Offline Sources of Information Related to Healthy Nutrition
2.3.2. Subjective Perception of Healthy Nutrition—Time Interval of Online and Offline Information-Seeking
2.3.3. Relative Perception of Healthy Nutrition—Transtheoretical Model (TTM) of Change in the Case of Transition to Health-Conscious Nutrition
2.3.4. Components of Attitudes towards Healthy Nutrition and of Electronic Health Literacy
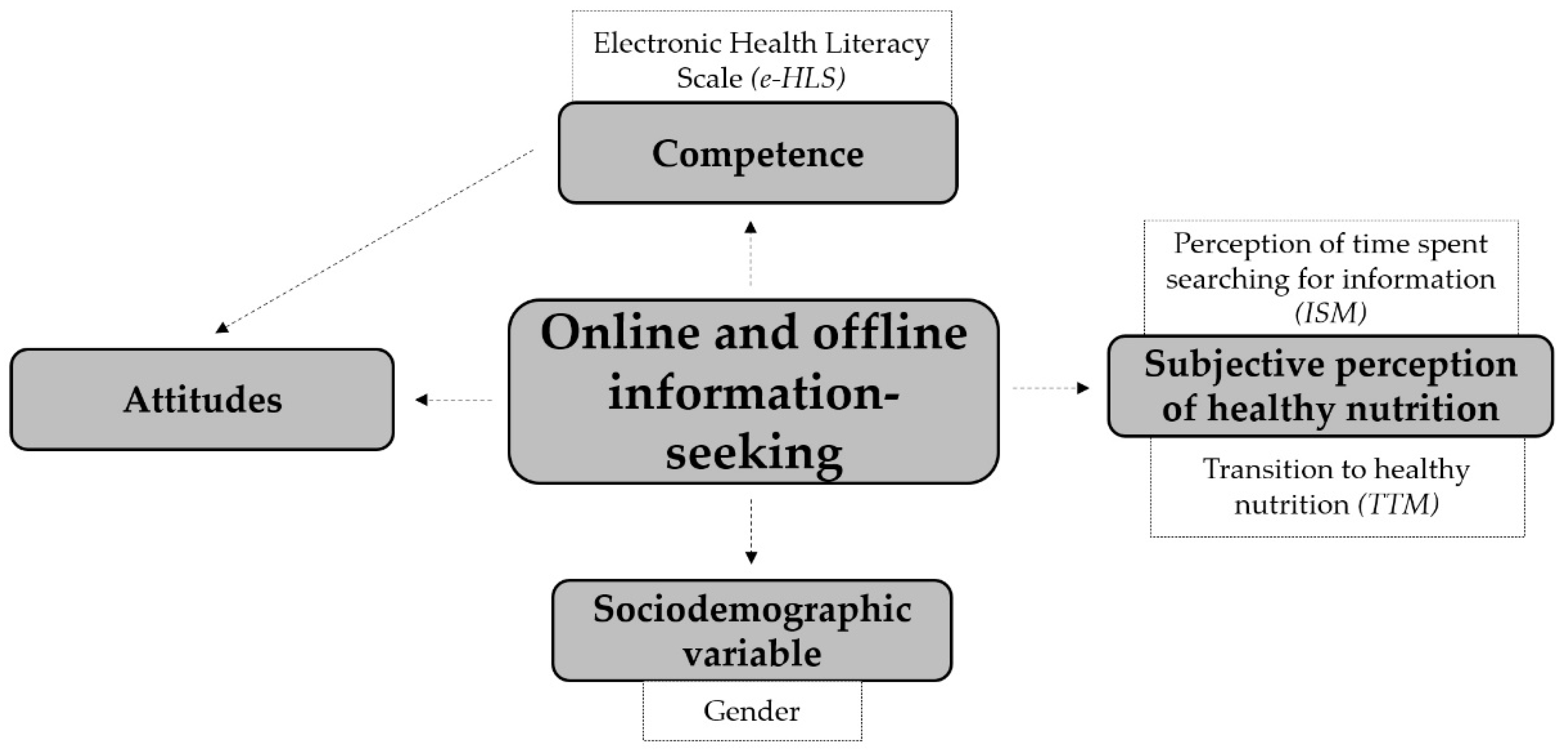
2.4. Preliminary Theoretical Concept of the Relationship between Online and Offline Information-Seeking Attitudes for Healthy Nutrition
2.5. Data Analysis
3. Results
3.1. Significance of Online and Offline Sources of Information
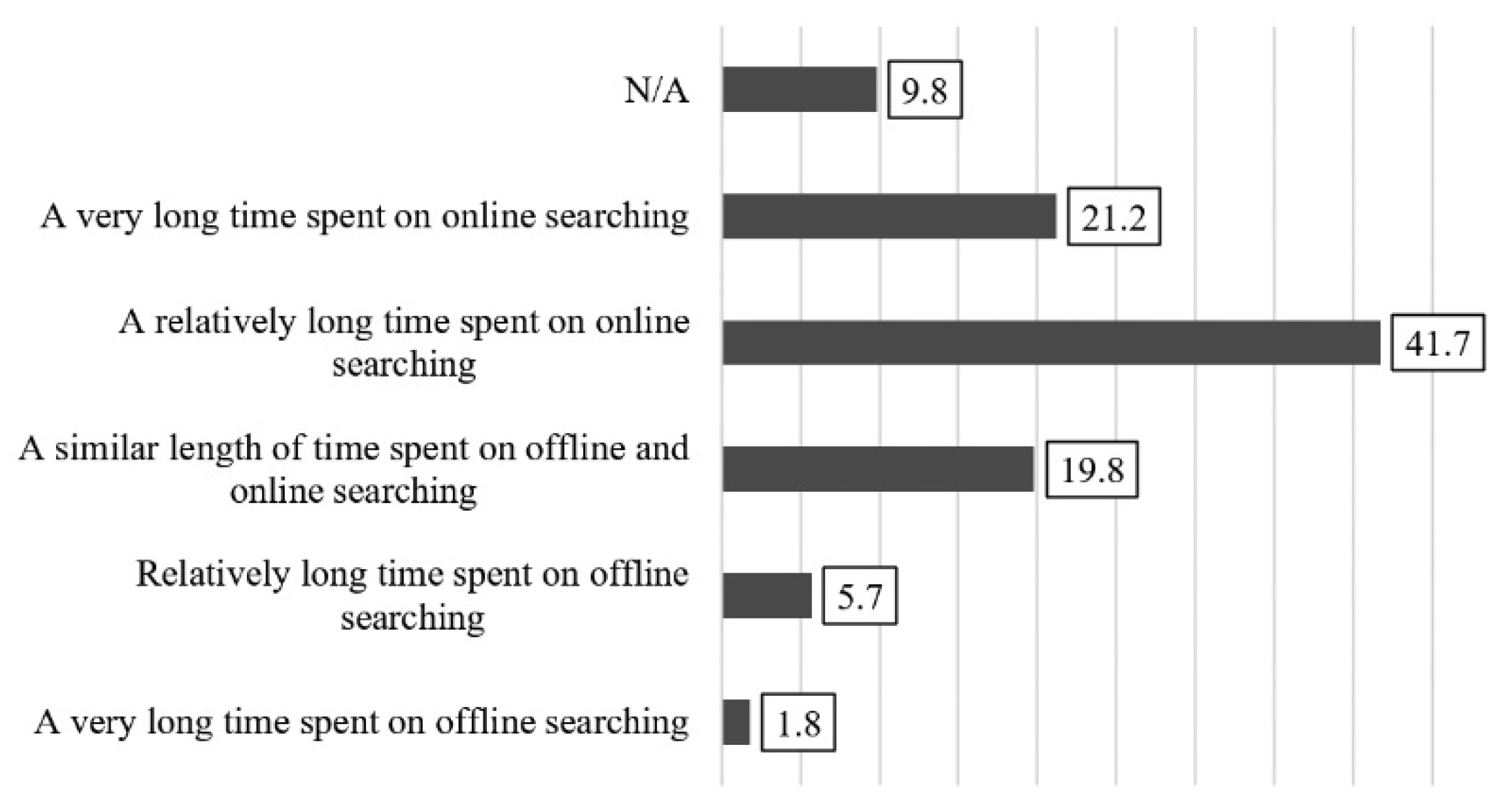
3.2. Time Interval of Online and Offline Information-Seeking
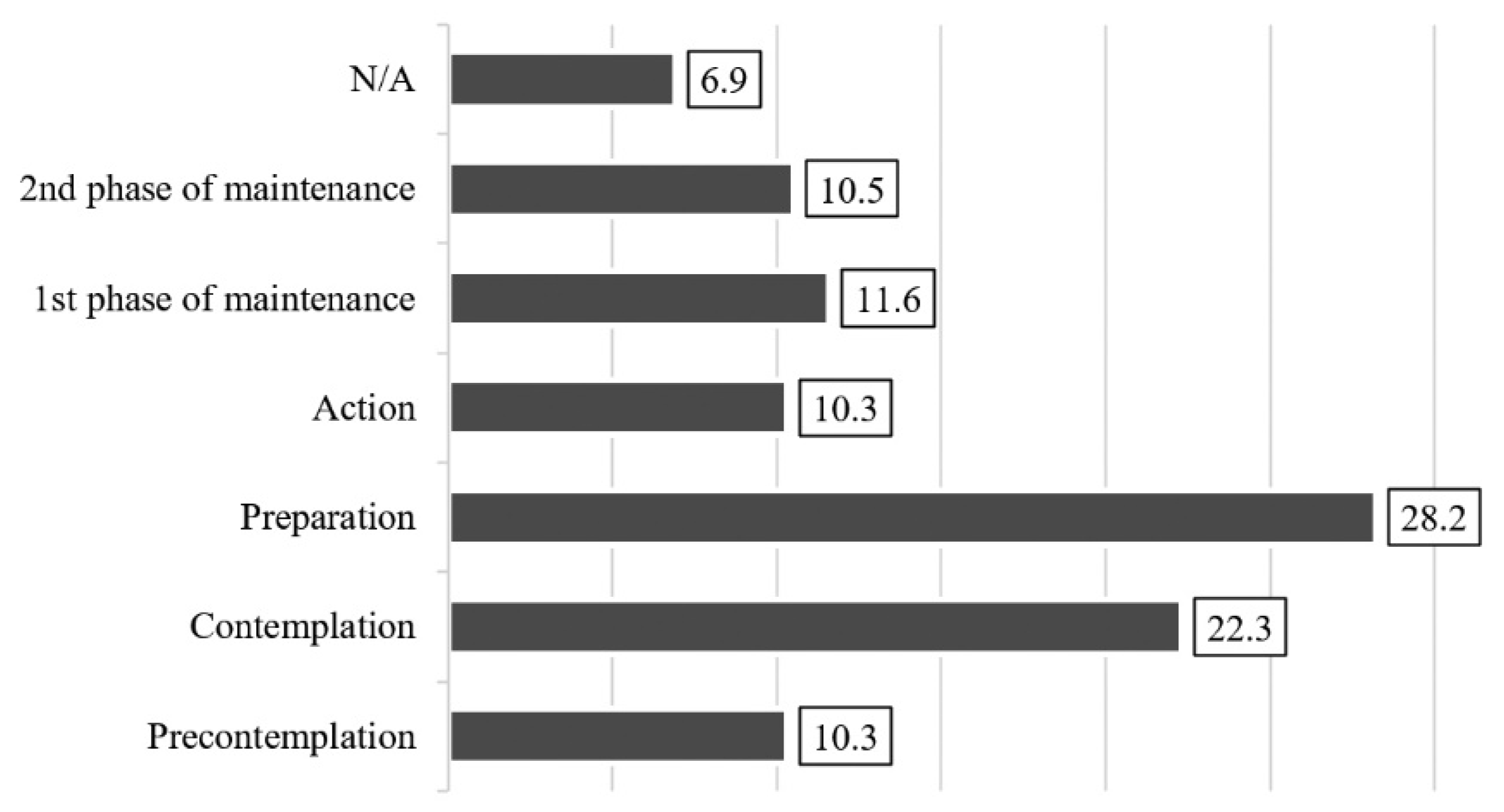
3.3. Transtheoretical Model (TTM) of Change for Transition to Health-Conscious Nutrition
3.4. Components of Attitudes towards Healthy Nutrition and of Electronic Health Literacy
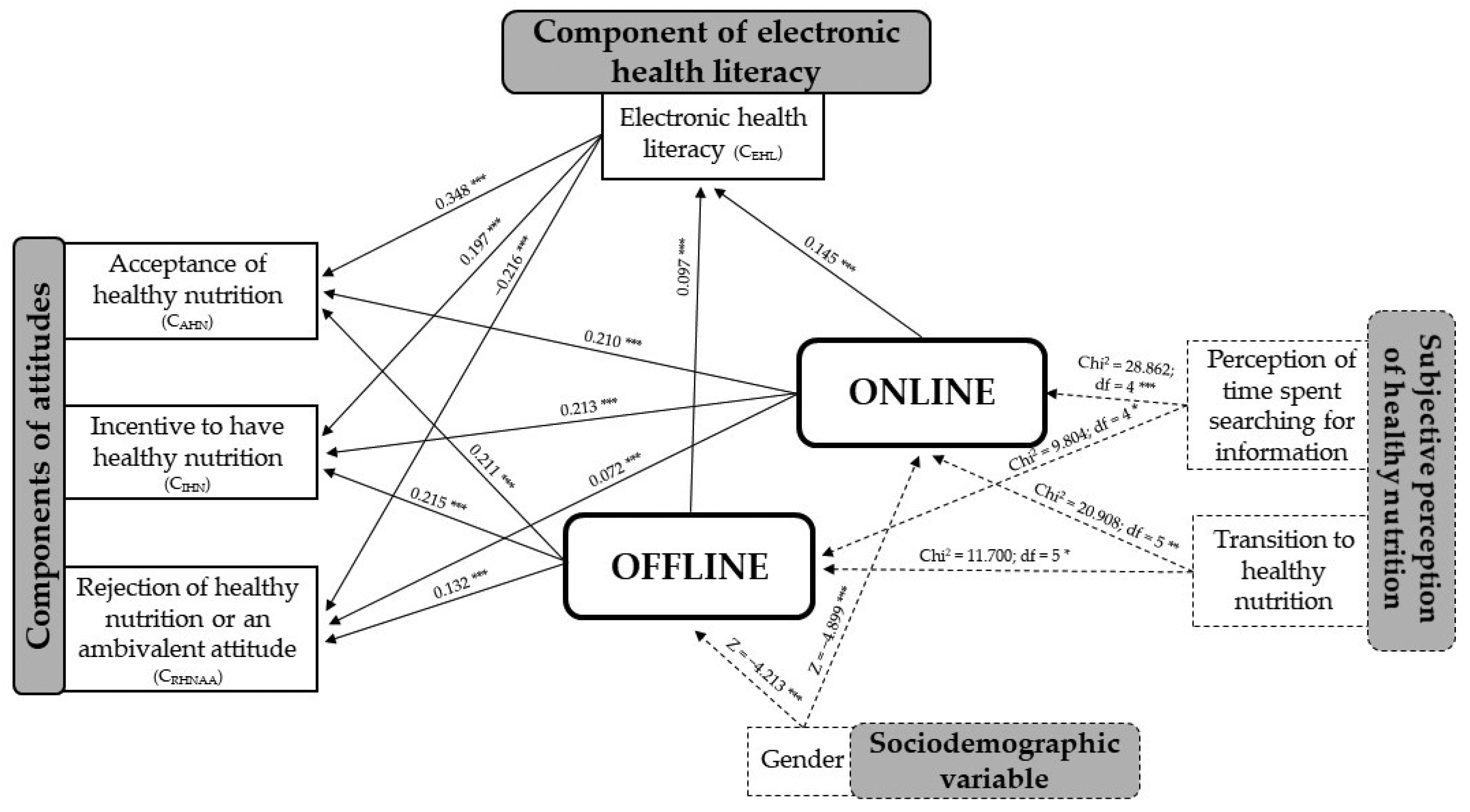
3.5. Theoretical Concept of the Relationship between Online and Offline Information-Seeking Attitudes Related to Healthy Nutrition
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Constitution. 2019. Available online: https://www.who.int/about/who-we-are/constitution (accessed on 11 April 2021).
- Felman, A. What is Good Health? Medical News Today. 2020. Available online: https://www.medicalnewstoday.com/articles/150999.php (accessed on 3 April 2021).
- Pagliaro, M. An industry in transition: The chemical industry and the megatrends driving its forthcoming transformation. Angew. Chem. Int. Edit. 2019, 58, 11154–11159. [Google Scholar] [CrossRef] [PubMed]
- Rohner, P. Water: A Megatrends Perspective. In Assessing Global Water Megatrends. Water Resources Development and Management; Biswas, A., Tortajada, C., Rohner, P., Eds.; Springer: Singapore, 2018. [Google Scholar] [CrossRef]
- Törőcsik, M. Az ételfogyasztás megatrend kapcsolódásai. The megatrend connections of food consumption. Táplálkozásmarketing 2014, 1, 19–27. [Google Scholar] [CrossRef]
- Zeyer, A. A win-win situation for health and science education: Seeing through the lens of a new framework model of health literacy. In Science, Environment, Health. Towards a Renewed Pedagogy for Science Education; Zeyer, A., Kyburz-Graber, R., Eds.; Springer: Dordrecht, Switzerland, 2012; ISBN 978-9048139484. [Google Scholar]
- Holly, B.; Stanulewicz, N.; Griffiths, K. Healthy lifestyle behaviors and health promotion attitudes in preregistered nurses: A questionnaire study. J. Nurs. Educ. 2017, 56, 94–103. [Google Scholar] [CrossRef] [Green Version]
- Von Bothmer, M.I.K.; Fridlund, B. Gender differences in health habits and in motivation for a healthy lifestyle among Swedish university students. Nurs. Health Sci. 2005, 7, 107–118. [Google Scholar] [CrossRef]
- Eurostat. Self-Perceived Health by Sex, Age and Groups of Country of Citizenship. 2019. Available online: https://appsso.eurostat.ec.europa.eu/nui/show.do?dataset=hlth_silc_24&lang=en (accessed on 1 April 2021).
- German, J.B.; Watzke, H.J. Personalizing foods for health and delight. Compr. Rev. Food Sci. Food Saf. 2004, 3, 145–151. [Google Scholar] [CrossRef]
- Kussmann, M.; Fay, L.B. Nutrigenomics and personalized nutrition. Pers. Med. 2008, 5, 447–455. [Google Scholar] [CrossRef]
- Szakály, Z.; Kiss, M.; Jasák, H. Funkcionális élelmiszerek, fogyasztói attitűdök és személyre szabott táplálkozás. Functional Foods, Consumer Attitudes and Personalized Nutrition. Táplálkozásmarketing 2014, 1–2, 3–17. [Google Scholar] [CrossRef]
- Szakály, Z.; Fehér, A.; Kiss, M. Chapter 9-Consumer Acceptance of Personalized Nutrition. In Trends in Personalized Nutrition; Galanakis, C.M., Ed.; Academic Press: London, UK, 2019; ISBN 978-0128164037. [Google Scholar]
- Eurobarometer. Health and Food. Special Eurobarometer No. 246. 2006, pp. 105–106. Available online: http://ec.europa.eu/health/ph_publication/eb_food_en.pdf (accessed on 8 April 2021).
- Gould, S.J. Health consciousness and health behavior: The application of a new health consciousness scale. Am. J. Prev. Med. 1990, 6, 228–237. [Google Scholar] [CrossRef]
- Larson, N.I.; Story, M.; Eisenberg, M.E.; Neumark-Sztainer, D. Food preparation and purchasing roles among adolescents: Associations with sociodemographic characteristics and diet quality. J. Am. Diet. Assoc. 2006, 106, 211–218. [Google Scholar] [CrossRef]
- Szakály, Z. Egészségmagatartás és funkcionális élelmiszerek: Hogyan vélekednek a hazai fogyasztók? Health behaviour and functional foods: What Hungarian consumers think of them? Élelmiszer Táplálkozás Mark. 2009, 6, 9–18. [Google Scholar]
- WHO. Obesity and Overweight. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 12 April 2021).
- Loef, M.; Walach, H. The combined effects of healthy lifestyle behaviors on all cause mortality: A systematic review and meta-analysis. Prev. Med. 2012, 55, 163–170. [Google Scholar] [CrossRef]
- WHO. Hungary. 2018. Available online: https://www.who.int/nmh/countries/hun_en.pdf?ua=1 (accessed on 11 April 2021).
- Ritchie, H.; Roser, M. Causes of Death. 2020. Available online: https://ourworldindata.org/causes-of-death (accessed on 6 April 2021).
- Karnai, L.; Szűcs, I. Táplálkozási szokások vizsgálata debreceni egyetemisták körében. Investigating the dietary practice of students at the University of Debrecen. Táplálkozásmarketing 2019, 6, 39–50. [Google Scholar] [CrossRef]
- McGinnis, J.M.; Appleton Gootman, J.; Kraak, V.I. (Eds.) Food marketing to children and youth. In Threat or Opportunity; The National Academies Press: Washington, DC, USA, 2006; ISBN 0-309-09713-4. [Google Scholar]
- Moreno, L.A.; Gottrand, F.; Huybrechts, I.; Ruiz, J.R.; González-Gross, M.; DeHenauw, S. Nutrition and lifestyle in European adolescents: The Helena (Healthy Lifestyle in Europe by Nutrition in Adolescence) Study. Adv. Nutr. 2014, 5, 615–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiss, V.Á.; Dombi, M.; Szakály, Z. Az egészség, a környezet és az étkezés kapcsolata–Szakirodalmi áttekintés. Analysis of the health–environment–nutrition nexus: A review. Táplálkozásmarketing 2019, 6, 3–24. [Google Scholar] [CrossRef]
- Cannella, C.; Savina, C.; Donini, L.M. Nutrition, longevity and behavior. Arch. Gerontol. Geriatr. 2009, 49 (Suppl. 1), 19–27. [Google Scholar] [CrossRef] [PubMed]
- Elmadfa, I. (Ed.) European Nutrition and Health Report. Forum of Nutrition; European Commission, Health and Consumer Protection, Directorate-Genera: Basel, Switzerland, 2009; ISBN 978-3805592963. [Google Scholar]
- Müller, A.; Gabnai, Z.; Pfau, C.S.; Pető, K. A magyarok táplálkozási szokásainak és tápláltsági állapotának jellemzői–Szakirodalmi áttekintés. Characteristics of eating habits and nutritional status among the Hungarian population–Literature review. Táplálkozásmarketing 2018, 5, 45–55. [Google Scholar] [CrossRef]
- Popkin, B.M. Commentary Global nutrition dynamics: The world is shifting rapidly toward a diet linked with noncommunicable diseases. Am. J. Clin. Nutr. 2006, 84, 289–298. [Google Scholar] [CrossRef]
- WHO. A Healthy Diet Sustainably Produced. Information Sheet. 2018. Available online: https://www.who.int/publications/i/item/WHO-NMH-NHD-18.12 (accessed on 7 April 2021).
- Yahia, N.; Wang, D.; Rapley, M.; Dey, R. Assessment of weight status, dietary habits and beliefs, physical activity, and nutritional knowledge among university students. Perspect. Public Health 2016, 136, 231–244. [Google Scholar] [CrossRef]
- El-Sabban, F.; Badr, H. Assessment of nutrition knowledge and related aspects among first-year Kuwait university students. Ecol. Food Nutr. 2011, 50, 181–195. [Google Scholar] [CrossRef]
- Tanvatanagul, W.; Uaphanthaseth, R. Statistical analysis of attitude and health care behavior of Chiang Mai University students (Thailand). J. Stat. Manag. Syst. 2005, 8, 659–679. [Google Scholar] [CrossRef]
- Önder, Ö.; Öztürk, M.; Yildiz, S.; Caylan, A. Evaluation of the attitudes of the students of the faculty of health sciences towards healthy nutrition and physical activity. Konuralp Med. J. 2020, 12, 400–405. [Google Scholar] [CrossRef]
- Racette, S.B.; Deusinger, S.S.; Strube, M.J.; Highstein, G.R.; Deusinger, R.H. Weight changes, exercise, and dietary patterns during freshman and sophomore years of college. J. Am. Coll. Health 2005, 53, 245–251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sira, N.; Pawlak, R. Prevalence of overweight and obesity, and dieting attitudes among Caucasian and African American college students in eastern North Carolina: A cross-sectional survey. Nutr. Res. Pract. 2010, 4, 36–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, X.; Pu, Y.; Sharma, M.; Rao, Y.; Cai, Y.; Zhao, Y. Predicting Physical Activity and Healthy Nutrition Behaviors Using Social Cognitive Theory: Cross-Sectional Survey among Undergraduate Students in Chongqing, China. Int. J. Environ. Res. Public Health 2017, 14, 1346. [Google Scholar] [CrossRef] [Green Version]
- Tavolacci, M.-P.; Déchelotte, P.; Ladner, J. Eating Disorders among College Students in France: Characteristics, Help-and Care-Seeking. Int. J. Environ. Res. Public Health 2020, 17, 5914. [Google Scholar] [CrossRef] [PubMed]
- Gergely, É.; Szabó, B.; Balázs, K. Az egészség- és környezettudatosság, valamint az értékrend hatása a bioélelmiszer-fogyasztásra. The effects of health and environmental consciousness and values on consuming bio foods. Mark. Menedzsment 2014, 48, 27–37. [Google Scholar]
- Kotler, L.A.; Cohen, P.; Davies, M.; Pine, D.S.; Walsh, B.T. Longitudinal relationships between childhood, adolescent, and adult eating disorders. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 1434–1440. [Google Scholar] [CrossRef]
- Nelson, M.; Story, M.; Larson, N.; Neumark-Sztainer, D.; Lytle, L. Emerging adulthood and college-aged youth: An overlooked age for weight-related behavior change. Obesity 2008, 16, 2205–2211. [Google Scholar] [CrossRef]
- Neumark-Sztainer, D.; Wall, M.; Larson, N.I.; Eisenberg, M.E.; Loth, K. Dieting and disordered eating behaviors from adolescence to young adulthood: Findings from a 10-year longitudinal study. J. Am. Diet Assoc. 2011, 111, 1004–1011. [Google Scholar] [CrossRef] [Green Version]
- Spinazze, P.A.; Kasteleyn, M.J.; Aardoom, J.J.; Car, J.; Chavannes, N.H. Cross-Sectional Analysis of University Students’ Health Using a Digitised Health Survey. Int. J. Environ. Res. Public Health 2020, 17, 3009. [Google Scholar] [CrossRef]
- Walter, W.C.; Skerrett, P.J. Eat, Drink, and Be Healthy: The Harvard Medical School Guide to Healthy Eating; Free Press: New York, NY, USA, 2017; ISBN 978-1501164774. [Google Scholar]
- Gál, T.; Soós, M.; Szakály, Z. Egészségtudatos táplálkozással kapcsolatos fogyasztói insight-ok feltárása netnográfiával. Exploring consumer insights related to health-conscious nutrition with netnography. Vezetéstudomány 2017, 48, 46–54. [Google Scholar] [CrossRef] [Green Version]
- Norman, C.D.; Skinner, H.A. eHEALS: The eHealth Literacy Scale. J. Med. Internet Res. 2006, 8, e27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blaylock, J.; Smallwood, D.; Kassel, K.; Variyam, J.; Aldrich, L. Economics, food choices, and nutrition. Food Policy 1999, 24, 269–286. [Google Scholar] [CrossRef] [Green Version]
- Szűcs, V.; Szabó, E.; Bánáti, D. Az egészséges táplálkozással kapcsolatos attitűdök feltárása kérdőíves megkérdezés alapján. Exploration of healthy nutrition attitudes using a questionnaire survey. Orv. Hetil. 2015, 156, 636–643. [Google Scholar] [CrossRef] [PubMed]
- Sørensen, K.; Van den Broucke, S.; Fullam, J.; Doyle, G.; Pelikan, J.; Slonska, Z.; Brand, H.; (HLS-EU) Consortium Health Literacy Project European. Health literacy and public health: A systematic review and integration of definitions and models. BMC Public Health 2012, 12, 80. [Google Scholar] [CrossRef] [Green Version]
- Behne, A.; Teuteberg, F. A healthy lifestyle and the adverse impact of its digitalization: The dark side of using eHealth Technologies. In Proceedings of the 15th International Conference on Wirtschaftsinformatik, Potsdam, Germany, 9–11 March 2020; Available online: https://0-doi-org.brum.beds.ac.uk/10.30844/wi_2020_f2-behne (accessed on 8 April 2021).
- AIPM. Problémás a Tudásunk az Egészségünkkel Kapcsolatosan–Felmérés Készült az Egészségértésről Magyarországon. [Our Knowledge about Our Health is Problematic–A Survey was Conducted on Health Perception in Hungary]. 2015. Available online: http://aipm.hu/hu/egeszsegertes/egeszsegertes-kutatas/ (accessed on 11 April 2021).
- Fehér, A.; Soós, M.; Szakály, Z. Az élelmiszer-fogyasztói magatartás vizsgálata online környezetben: Létezik-e hazánkban digitális élelmiszerfogyasztó? Analysis of the food consumer behavior in the online environment: Does digital food consumer exist in Hungary? Táplálkozásmarketing 2014, 1, 29–38. [Google Scholar] [CrossRef]
- Nomura, S.; Miyata, H. Digitization of the approach to food and nutrition respecting individual health values. Nutr. Rev. 2020, 78, 46–48. [Google Scholar] [CrossRef] [PubMed]
- IWS. World Internet Usage and Population Statistics. 2020. Available online: https://www.internetworldstats.com/stats.htm (accessed on 1 April 2021).
- Eurostat. Individuals Using the Internet for Seeking Health-Related Information. 2020. Available online: https://ec.europa.eu/eurostat/databrowser/view/tin00101/default/table?lang=en (accessed on 1 April 2021).
- Meskó, B.; Drobni, Z.; Bényei, É.; Gergely, B.; Győrffy, Z. Digital health is a cultural transformation of traditional healthcare. Mhealth 2017, 3, 38. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Lan, Y.-C.; Chang, Y.-W.; Chang, P.-Y. Exploring doctors’ willingness to provide online counseling services: The roles of motivations and costs. Int. J. Environ. Res. Public Health 2020, 17, 110. [Google Scholar] [CrossRef] [Green Version]
- Lupton, D. Better understanding about what’s going on: Young Australians’ use of digital technologies for health and fitness. Sport Educ. Soc. 2020, 25, 1–13. [Google Scholar] [CrossRef]
- Jacques, L.; Bussien, C.; Descloux, C.; Decorsaire, L.; Lovis, C.; Ehrler, F. Nutrikids a smartphone application to improve the quality of paediatrical dietary assessments: Feasability study. Stud. Health Technol. Inform. 2020, 270, 1016–1020. [Google Scholar] [CrossRef]
- Seung-Dae, K.; Myung-Gwan, K. The effect of university students’ approach to health information on improvement of health behavior. J. Korea Acad. Ind. Coop. Soc. 2015, 16, 3268–3275. [Google Scholar] [CrossRef]
- Achampong, E.K.; Azanga, T.M.; Agbeno, E.K. The influence of social media on the health seeking behaviour of university students. Appl. Med. Inform. 2020, 42, 200–205. [Google Scholar]
- Duffett, R.G. Influence of social media marketing communications on young consumers’ attitudes. Young Consum. 2017, 18, 19–39. [Google Scholar] [CrossRef]
- Field, A. Discovering Statistics Using IBM SPSS Statistics; SAGE Publications Ltd: London, UK, 2017; ISBN 978-1446249178. [Google Scholar]
- Jepsen, A.L. Factors affecting consumer use of the Internet for information search. J. Interact. Mark. 1997, 21, 21–34. [Google Scholar] [CrossRef] [Green Version]
- Prochaska, J.O.; Norcross, J.C.; DiClemente, C.C. Changing for Good: The Revolutionary Program that Explains the Six Stages of Change and Teaches You How to Free Yourself from Bad Habits; W. Morrow: New York, NY, USA, 1994; ISBN 978-0688112639. [Google Scholar]
- Ruggiero, L. Helping people with diabetes change behavior: From theory to practice. Diabetes Spectrum 2000, 13, 125. [Google Scholar]
- Szabó, S. The relationship of health-oriented nutritional habits and consumer behavior. Ph.D. Thesis, Kaposvári Egyetem, Gazdaságtudományi Kar, Kaposvár, Hungary, 2016. Available online: http://www.gtk.ke.hu/tartalom/doktori/Szabo-Sara-thesis-english.pdf (accessed on 8 April 2021).
- Britt, R.K.; Collins, W.B.; Wilson, K.; Linnermeier, G.; Englebert, A.M. eHealth Literacy and Health behaviors affecting modern college students: A pilot study of issues identified by the American College Health Association. J. Med. Internet Res. 2017, 19, e392. [Google Scholar] [CrossRef] [PubMed]
- Choi, N.G.; Dinitto, D.M. The digital divide among low-income homebound older adults: Internet use patterns, eHealth literacy, and attitudes toward computer/Internet use. J. Med. Internet Res. 2013, 15, e93. [Google Scholar] [CrossRef] [PubMed]
- Ghaddar, S.F.; Valerio, M.A.; Garcia, C.M.; Hansen, L. Adolescent health literacy: The importance of credible sources for online health information. J. Sch. Health 2012, 82, 28–36. [Google Scholar] [CrossRef] [Green Version]
- Mitsutake, S.; Shibata, A.; Ishii, K.; Okazaki, K.; Oka, K. Developing Japanese version of the eHealth Literacy Scale (eHEALS). Jpn. J. Health 2011, 58, 361–371. [Google Scholar] [PubMed]
- Reder, M.; Soellner, R. eHealth Literacy–German translation of the Self-reported Measure eHEALS and Development of a Skill-based Measure. In Proceedings of the 27th Conference of the European Health Psychology Society, Bordeaux, France, 16–20 July 2013. [Google Scholar]
- Szabó, K.; Pikó, B. A táplálkozással kapcsolatos attitűdök, magatartás és információkeresés vizsgálata és összefüggése szociodemográfiai és pszichológiai változókkal serdülők körében. Study of eating attitudes, behaviour and information-seeking in relation to sociodemographic and psychological factors among adolescents. Orv. Hetil. 2018, 159, 2183–2192. [Google Scholar] [CrossRef] [PubMed]
- Babby, E.R. (Ed.) The Basics of Social Research, 4th ed.; Thomson/Wadsworth: Belmont, CA, USA, 2007; ISBN 049-5094684. [Google Scholar]
- Pearson, K. Notes on regression and inheritance in the case of two parents. Proc. R. Soc. Lond. 1895, 58, 240–242. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Description | Distribution of the Sample | |
|---|---|---|
| Number | % | |
| By all students surveyed | ||
| Total | 612 | 100.0 |
| By gender | ||
| Female | 372 | 60.8 |
| Male | 240 | 39.2 |
| By type of residence | ||
| Capital | 50 | 8.2 |
| Municipality | 228 | 37.3 |
| Other towns | 182 | 29.7 |
| Village | 152 | 24.8 |
| Age distribution | ||
| 18–19 | 153 | 25.1 |
| 20–21 | 269 | 44.0 |
| Over 22 | 189 | 31.0 |
| Distribution by level of education | ||
| Bachelor program | 332 | 54.2 |
| Master’s program | 59 | 9.6 |
| University vocational program | 221 | 36.1 |
| Distribution by qualifications | ||
| University of Debrecen | 115 | 18.8 |
| University of Debrecen– Szolnok Campus | 81 | 13.2 |
| University of Kaposvár | 42 | 6.9 |
| Széchenyi István University | 94 | 15.4 |
| Budapest Business School | 98 | 16.0 |
| Szent István University | 14 | 2.3 |
| University of Nyírgyháza | 95 | 15.5 |
| University of Pécs | 9 | 1.5 |
| Perception of time spent using the Internet | ||
| Less than 30 min | 3 | 0.5 |
| Between 30 min and 1 h | 27 | 4.4 |
| Between 1 and 2 h | 121 | 19.8 |
| Between 3 and 5 h | 344 | 56.2 |
| Between 6 and 10 h | 93 | 15.2 |
| Over 10 h | 12 | 2.0 |
| Perception of subjective income position | ||
| Live very well off the income and can even save | 182 | 29.7 |
| Can live off the income but can save only a little | 290 | 47.4 |
| The income is barely sufficient to live on and the family cannot save any of it | 85 | 13.9 |
| Sometimes the income is not sufficient for the family | 7 | 1.1 |
| Family faces regular daily financial issues | 4 | 0.7 |
| Does not know / Does not answer | 44 | 7.2 |
| Subjective health consciousness | ||
| Not health conscious at all | 11 | 1.8 |
| Mostly not health conscious | 76 | 12.4 |
| Half health conscious, half not | 252 | 41.2 |
| Mostly health conscious | 232 | 37.9 |
| Very health conscious | 35 | 5.7 |
| By BMI index | ||
| Thinness (<18,5) | 54 | 9.1 |
| Normal (18.5–25) | 406 | 68.5 |
| Overweight (25–30) | 108 | 18.2 |
| Obesity (>30) | 25 | 4.2 |
| Mean | Median | Mode | Deviation | Skewness | |
|---|---|---|---|---|---|
| Homepage entries by dietitians/health science specialists related to healthy nutrition | 3.64 | 4 | 4 | 1.096 | −0.566 |
| Search engines (e.g., Google, Bing) | 3.10 | 3 | 3 | 1.052 | −0.121 |
| Blogs, forums | 3.02 | 3 | 3 | 1.015 | −0.086 |
| Internet news sites (e.g., BBC, CNN) | 2.99 | 3 | 3 | 1.067 | −0.079 |
| Social media (e.g., Facebook, Instagram) | 2.86 | 3 | 3 | 1.151 | −0.062 |
| Online video channels by influencers (e.g., YouTube channels) | 2.46 | 2 | 1 | 1.203 | 0.349 |
| Mean | Median | Mode | Deviation | Skewness | |
|---|---|---|---|---|---|
| Personal information received during health care (physician, dietitian, pharmacist, etc.) | 4.49 | 5 | 5 | 0.802 | −1.710 |
| Books, journals | 3.99 | 4 | 5 | 1.105 | −1.010 |
| Food labelling/marking, label information | 3.96 | 4 | 4 | 0.897 | −0.609 |
| Information provided by skilled shop assistants in specialized shops (e.g., organic shop, phyto-shop) | 3.96 | 4 | 4 | 0.916 | −0.786 |
| Discussion with neighbor, acquaintance, | 3.61 | 4 | 4 | 1.038 | −0.585 |
| Health booklets, health education handbooks | 3.60 | 4 | 4 | 1.068 | −0.491 |
| Knowledge learned in school | 3.43 | 3 | 3 | 0.937 | −0.295 |
| Articles in magazines about healthy lifestyle and healthy nutrition | 3.20 | 3 | 3 | 1.082 | −0.265 |
| Product information, leaflets | 2.83 | 3 | 3 | 1.027 | 0.057 |
| Relevant pieces of writing in free publications | 2.83 | 3 | 3 | 1.052 | −0.027 |
| Television programs | 2.48 | 3 | 3 | 1.008 | 0.141 |
| Television commercials | 2.32 | 2 | 2 | 0.984 | 0.462 |
| Advertisements in newspapers, on posters and billboards | 2.31 | 2 | 2 | 0.940 | 0.358 |
| Radio programs | 2.30 | 2 | 2 | 0.935 | 0.355 |
| Statements | CEHL |
|---|---|
| I know how to use the Internet to answer questions about healthy nutrition. | 0.756 |
| I know where to find helpful resources on the Internet in my daily searches. | 0.748 |
| I can tell high-quality health resources of healthy nutrition from low-quality health resources on the Internet. | 0.745 |
| I know how to use the health information related to healthy nutrition found on the Internet to help me. | 0.742 |
| I know where to find helpful resources on the Internet in my daily searches. | 0.731 |
| I have the skills I need to evaluate the health resources of healthy nutrition I find on the Internet. | 0.719 |
| I feel confident in using the information about healthy nutrition from the Internet to make health decisions. | 0.684 |
| I know what health resources are available on the Internet related to healthy nutrition. | 0.643 |
| Statements | CAHN | CIHN | CRHNAA |
|---|---|---|---|
| I pay close attention to healthy and balanced nutrition and choose my foods carefully. | 0.843 | ||
| I make a conscious effort to find foodstuffs with ingredients that I consider beneficial. | 0.760 | ||
| I pay attention to the effect of foods and foodstuffs on body weight. | 0.742 | ||
| I make a conscious effort to avoid foods that are energy-dense (oil, sugar). | 0.720 | ||
| I make a conscious effort to avoid foodstuffs with ingredients that I consider harmful. | 0.688 | ||
| I try to create a balanced diet. | 0.636 | ||
| When compiling my diet, I follow nutrition-related recommendations based on current medical knowledge. | 0.623 | ||
| I persuade others, too, to eat a healthier diet. | 0.879 | ||
| I find it important that the people around me should also have a healthier diet. | 0.879 | ||
| I have tried several times to eat healthily but, after temporary self-punishment, I have returned to my usual routine. | 0.693 | ||
| Healthy eating always reminds me of slimming cures. | 0.683 | ||
| What tastes good makes me really healthy. | 0.614 | ||
| Knowledge about healthy nutrition keeps changing and expanding, thus it is difficult to keep up with it. | 0.586 | ||
| Healthy nutrition is very costly. | 0.545 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fehér, A.; Véha, M.; Boros, H.M.; Kovács, B.; Kontor, E.; Szakály, Z. The Relationship between Online and Offline Information-Seeking Behaviors for Healthy Nutrition. Int. J. Environ. Res. Public Health 2021, 18, 10241. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910241
Fehér A, Véha M, Boros HM, Kovács B, Kontor E, Szakály Z. The Relationship between Online and Offline Information-Seeking Behaviors for Healthy Nutrition. International Journal of Environmental Research and Public Health. 2021; 18(19):10241. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910241
Chicago/Turabian StyleFehér, András, Miklós Véha, Henrietta Mónika Boros, Bence Kovács, Enikő Kontor, and Zoltán Szakály. 2021. "The Relationship between Online and Offline Information-Seeking Behaviors for Healthy Nutrition" International Journal of Environmental Research and Public Health 18, no. 19: 10241. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910241