
Evaluation of Stress Distribution and Force in External Hexagonal Implant: A 3-D Finite Element Analysis

 , , ,
, , , 
Abstract
:1. Introduction
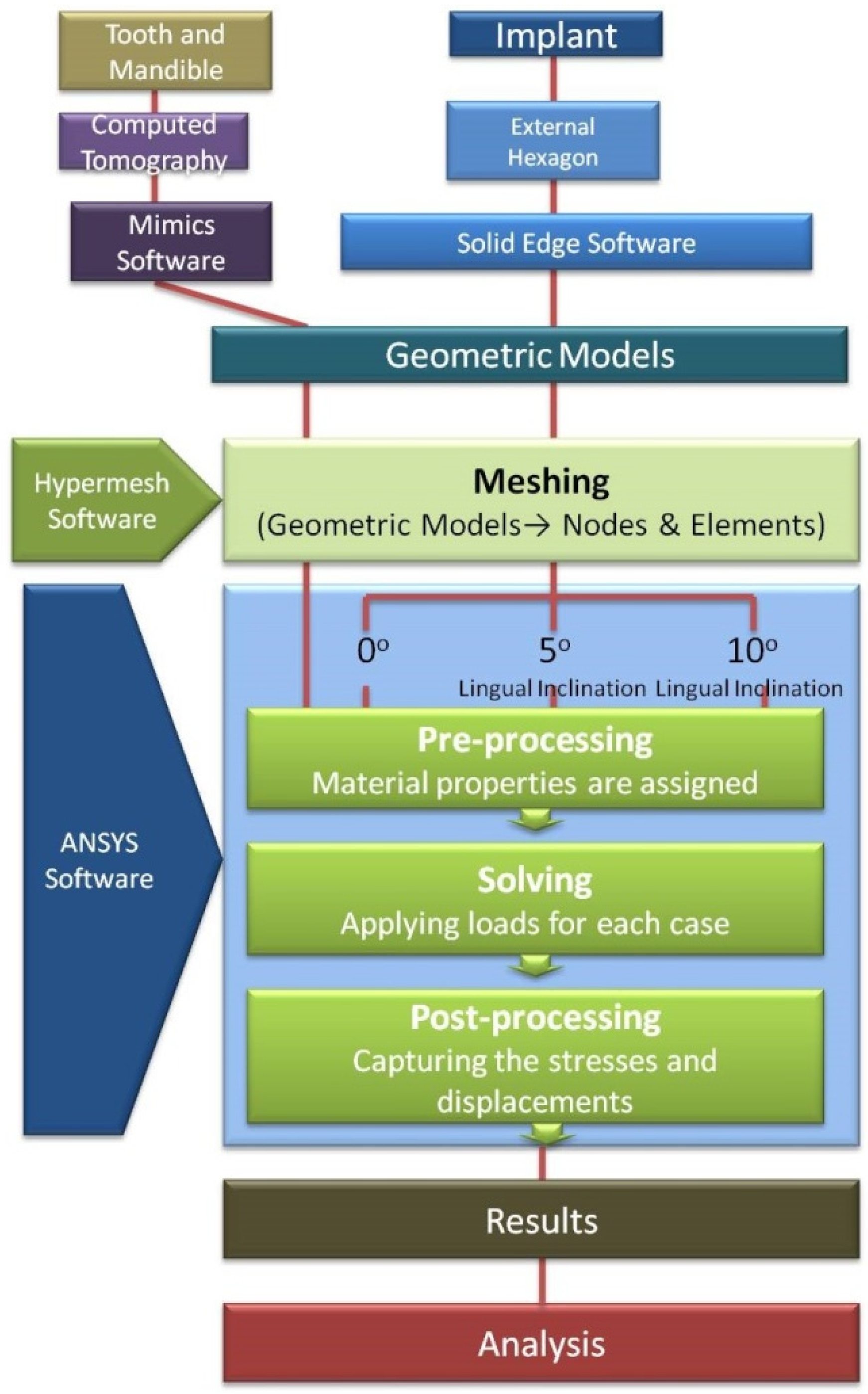
2. Materials and Methods
3. Results
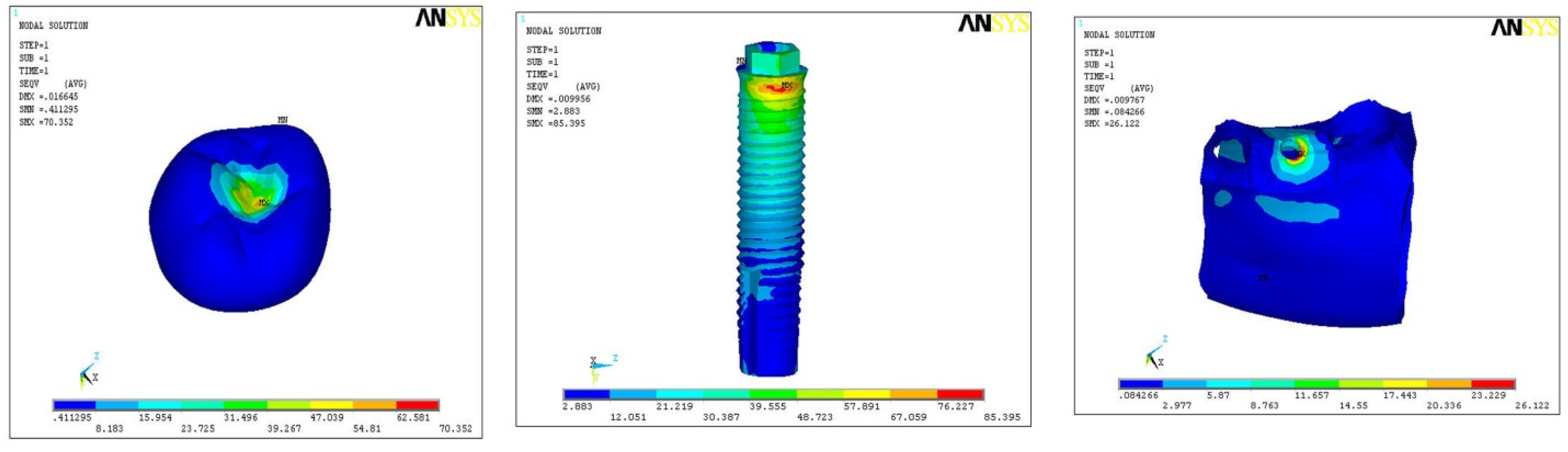
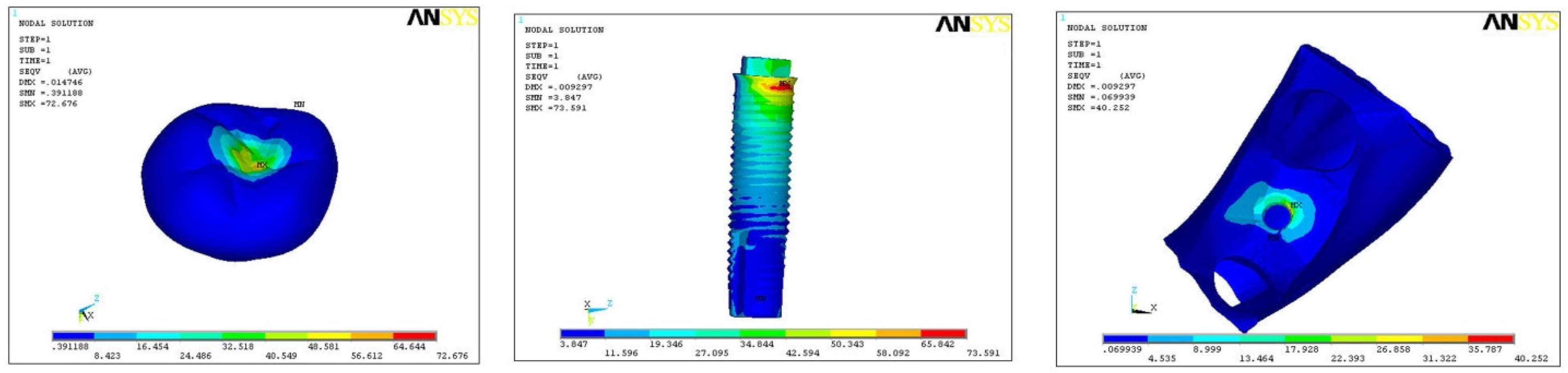
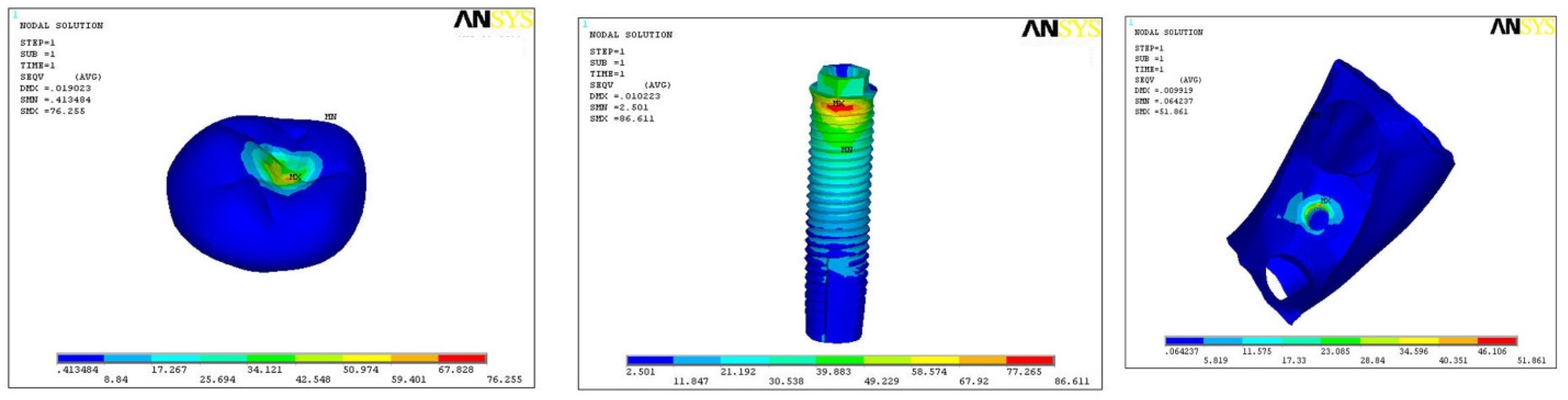
3.1. Von Mises Stress in Models A1, A2, and A3 (All Values in MPa)
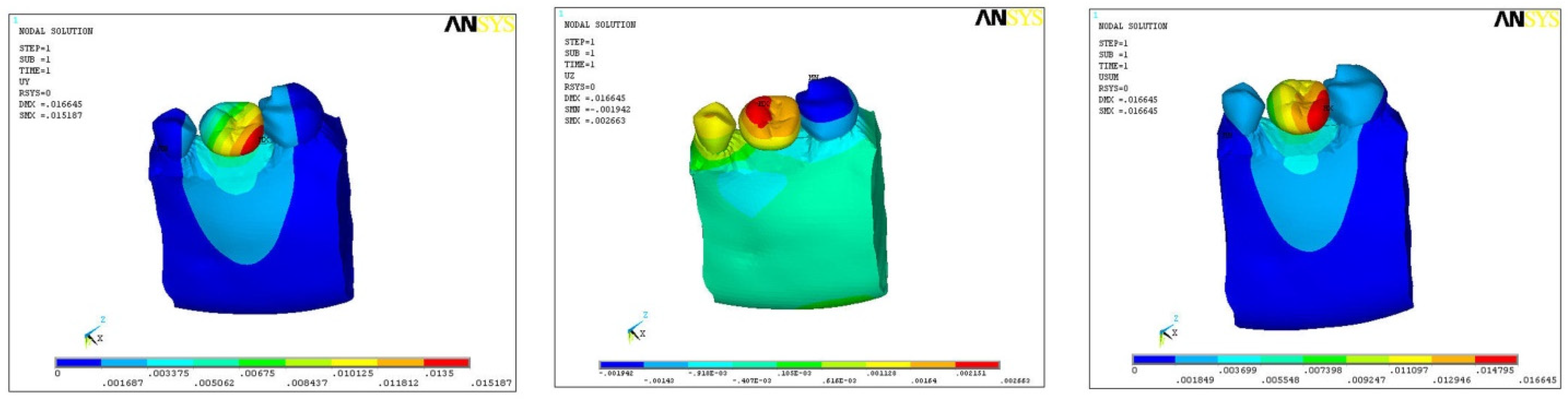
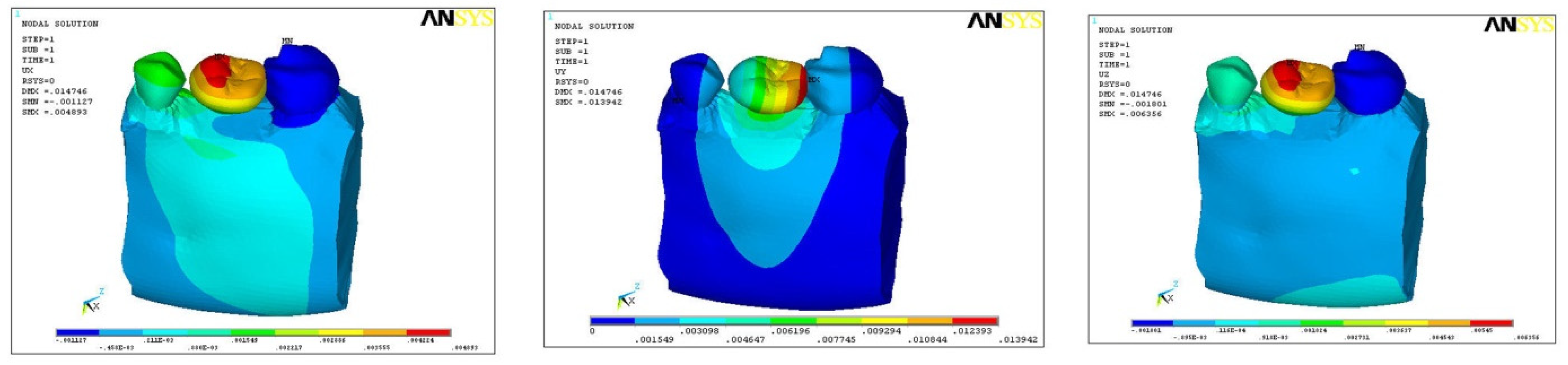
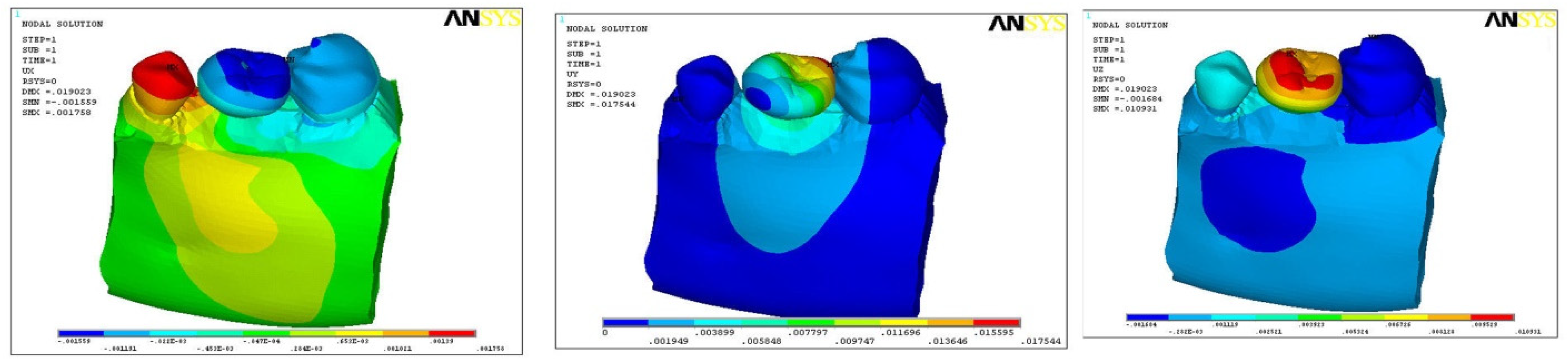
3.2. Direction of Force on Models B1, B2, and B3
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Raikar, S.; Talukdar, P.; Kumari, S.; Panda, S.K.; Oommen, V.M.; Prasad, A. Factors affecting the survival rate of dental implants: A retrospective study. J. Int. Soc. Prev. Community Dent. 2017, 7, 351–355. [Google Scholar] [CrossRef] [PubMed]
- Bandela, V.; Munagapati, B.; Komala, J.; Basany, R.B.; Patil, S.R.; Kanaparthi, S. Comparison of primary stability of implants installed by two different methods in D3 and D4 bone types: An in vitro study. J. Int. Soc. Prev. Community Dent. 2020, 10, 620–626. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, O.; Zafiropoulos, G.-G. Tooth-implant connection: A review. J. Oral Implantol. 2012, 38, 194–200. [Google Scholar] [CrossRef]
- Shafie, H.R. Clinical and Laboratory Manual of Dental Implant Abutments; John Wiley & Sons: Hoboken, NJ, USA, 2014. [Google Scholar]
- Gracis, S.; Michalakis, K.; Vigolo, P.; Vult von Steyern, P.; Zwahlen, M.; Sailer, I. Internal vs. external connections for abutments/reconstructions: A systematic review. Clin. Oral Implant. Res. 2012, 23, 202–216. [Google Scholar] [CrossRef]
- Yokoyama, S.; Wakabayashi, N.; Shiota, M.; Ohyama, T. The influence of implant location and length on stress distribution for three-unit implant-supported posterior cantilever fixed partial dentures. J. Prosthet. Dent. 2004, 91, 234–240. [Google Scholar] [CrossRef]
- Meijer, H.; Kuiper, J.; Starmans, F.; Bosman, F. Stress distribution around dental implants: Influence of superstructure, length of implants, and height of mandible. J. Prosthet. Dent. 1992, 68, 96–102. [Google Scholar] [CrossRef]
- Papavasiliou, G.; Kamposiora, P.; Bayne, S.C.; Felton, D.A. Three-dimensional finite element analysis of stress-distribution around single tooth implants as a function of bony support, prosthesis type, and loading during function. J. Prosthet. Dent. 1996, 76, 633–640. [Google Scholar] [CrossRef]
- Geramy, A.; Morgano, S.M. Finite element analysis of three designs of an implant-supported molar crown. J. Prosthet. Dent. 2004, 92, 434–440. [Google Scholar] [CrossRef]
- Misch, C. Dental Evaluation: Factors of Stress. In Contemporary Implant Dentistry, 2nd ed.; Mosby: St. Louis, MO, USA, 1999; pp. 123–129. [Google Scholar]
- Brunski, J.B.; Puleo, D.A.; Nanci, A. Biomaterials and biomechanics of oral and maxillofacial implants: Current status and future developments. Int. J. Oral Maxillofac. Implant. 2000, 15, 15–46. [Google Scholar]
- Ishigaki, S.; Nakano, T.; Yamada, S.; Nakamura, T.; Takashima, F. Biomechanical stress in bone surrounding an implant under simulated chewing. Clin. Oral Implant. Res. 2003, 14, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Imanishi, A.; Nakamura, T.; Ohyama, T. 3-D Finite element analysis of all-ceramic posterior crowns. J. Oral Rehabil. 2003, 30, 818–822. [Google Scholar] [CrossRef]
- Sato, Y.; Wadamoto, M.; Tsuga, K.; Teixeira, E. The effectiveness of element downsizing on a three-dimensional finite element model of bone trabeculae in implant biomechanics. J. Oral Rehabil. 1999, 26, 288–291. [Google Scholar] [CrossRef]
- De Jager, N.; de Kler, M.; van der Zel, J.M. The influence of different core material on the FEA-determined stress distribution in dental crowns. Dent. Mater. 2006, 22, 234–242. [Google Scholar] [CrossRef]
- Fütterling, S.; Klein, R.; Straßer, W.; Weber, H. Automated finite element modeling of a human mandible with dental implants. J. WSCG 1998, 6, 1–3. [Google Scholar]
- Hart, R.T.; Hennebel, V.V.; Thongpreda, N.; Van Buskirk, W.C.; Anderson, R.C. Modeling the biomechanics of the mandible: A three-dimensional finite element study. J. Biomech. 1992, 25, 261–286. [Google Scholar] [CrossRef]
- Okeson, J.P. Functional neuroanatomy and physiology of the masticatory system. In Management of Temporomandibular Dis-orders and Occlusion; Mosby: St. Louis, MO, USA, 1998; pp. 29–66. [Google Scholar]
- Levy, D.; Deporter, D.A.; Watson, P.A.; Pilliar, R.M. Periodontal parameters around porous-coated dental implants after 3 to 4 years supporting overdentures. J. Clin. Periodontol. 1996, 23, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Chandrupatla, T.R.; Belegundu, A.D.; Ramesh, T.; Ray, C. Introduction to Finite Elements in Engineering; Prentice Hall: Upper Saddle River, NJ, USA, 2002. [Google Scholar]
- Cruz, M.; Wassall, T.; Toledo, E.M.; da Silva Barra, L.P.; de Castro Lemonge, A.C. Three-dimensional finite element stress analysis of a cuneiform-geometry implant. Int. J. Oral Maxillofac. Implant. 2003, 18, 675–684. [Google Scholar]
- Geng, J.-P.; Tan, K.B.; Liu, G.-R. Application of finite element analysis in implant dentistry: A review of the literature. J. Prosthet. Dent. 2001, 85, 585–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meijer, H.; Starmans, F.; Steen, W.; Bosman, F. Loading conditions of endosseous implants in an edentulous human mandible: A three-dimensional, finite element study. J. Oral Rehabil. 1996, 23, 757–763. [Google Scholar] [CrossRef]
- Meijer, H.; Starmans, F.; Steen, W.; Bosman, F. A three-dimensional, finite-element analysis of bone around dental implants in an edentulous human mandible. Arch. Oral Biol. 1993, 38, 491–496. [Google Scholar] [CrossRef]
- Teixeira, E.; Sato, Y.; Akagawa, Y.; Shindoi, N. A comparative evaluation of mandibular finite element models with different lengths and elements for implant biomechanics. J. Oral Rehabil. 1998, 25, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Montemezzi, P.; Ferrini, F.; Pantaleo, G.; Gherlone, E.; Capparè, P. Dental Implants with Different Neck Design: A Prospective Clinical Comparative Study with 2-Year Follow-Up. Materials 2020, 13, 1029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zanardi, P.R.; Stegun, R.C.; Sesma, N.; Costa, B.; Shibli, J.A.; Laganá, D.C. Stress distribution around dental implants placed at different depths. J. Craniofac. Surg. 2015, 26, 2163–2166. [Google Scholar] [CrossRef] [PubMed]
- Cordeiro, B.Q.; Mourão, C.F.; Carvalho, W.R.; Fonseca, E.M.; Montemezzi, P.; Javid, K.; Martins, C.C.; Quinelato, V.; Moreno, M.D.; Casado, P.L. Vertical Discrepancy in Height of Morse Cone Abutments Submitted to Different Torque Forces. Materials 2021, 14, 4950. [Google Scholar] [CrossRef] [PubMed]
- Nelson, S.J. Wheeler’s Dental Anatomy, Physiology and Occlusion; Elsevier Health Sciences: St. Louis, MO, USA, 2014. [Google Scholar]
- Sertgöz, A.; Güvener, S. Finite element analysis of the effect of cantilever and implant length on stress distribution in an implant-supported fixed prosthesis. J. Prosthet. Dent. 1996, 76, 165–169. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Length of Implant | 13 mm |
|---|---|
| Diameter of implant | 5 mm |
| Length of abutment | 6.5 mm |
| Diameter of abutment | 5 mm |
| Yield strength | 760 MPa |
| Tensile strength | 860 MPa |
| Flexural strength of crown | 1120 MPa |
| Material | E (MPa) | Nu (ν) |
|---|---|---|
| Dentine | 18,600 | 0.31 |
| Hard bone | 15,000 | 0.33 |
| Soft bone | 1500 | 0.3 |
| Periodontal ligament | 50 | 0.45 |
| Implant | 110,000 | 0.35 |
| Abutment | 114,000 | 0.34 |
| Inner screw | 205,000 | 0.33 |
| Crown | 70,000 | 0.19 |
| n = 14 | Von Mises Stress (N/M2) | ANOVA | ||||
|---|---|---|---|---|---|---|
| Crown | Implant | Hard Bone | F-Value | p-Value | ||
| Model A 1 | 0 Degree | 70.35 (±14.85) | 85.39 (±22.65) | 26.12 (±8.95) | 25.8 | 0.00 * |
| Model A 2 | 5 Degree | 72.67 (±11.25) | 73.59 (±16.78) | 40.25 (±11.87) | 0.00 * | |
| Model A 3 | 10 Degree | 76.25 (±18.98) | 86.61 (±14.68) | 51.86 (±10.57) | 0.00 * | |
| n = 14 | Direction of Force (N) | ANOVA | ||||
|---|---|---|---|---|---|---|
| X-Axis | Y-Axis | Z-Axis | F-Value | p-Value | ||
| Model B 1 | 0 Degree | 0.01025 (±0.004) | 0.0151 (±0.003) | 0.002 (±0.003) | 0.001 | 0.012 |
| Model B 2 | 5 Degree | 0.0048 (±0.001) | 0.0139 (0.006) | 0.006 (±0.004) | 0.02 | |
| Model B 3 | 10 Degree | 0.0017 (±0.008) | 0.0175 (±0.005) | 0.0109 (±0.008) | 0.04 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bandela, V.; Basany, R.; Nagarajappa, A.K.; Basha, S.; Kanaparthi, S.; Ganji, K.K.; Patil, S.; Gudipaneni, R.K.; Mohammed, G.S.; Alam, M.K. Evaluation of Stress Distribution and Force in External Hexagonal Implant: A 3-D Finite Element Analysis. Int. J. Environ. Res. Public Health 2021, 18, 10266. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910266
Bandela V, Basany R, Nagarajappa AK, Basha S, Kanaparthi S, Ganji KK, Patil S, Gudipaneni RK, Mohammed GS, Alam MK. Evaluation of Stress Distribution and Force in External Hexagonal Implant: A 3-D Finite Element Analysis. International Journal of Environmental Research and Public Health. 2021; 18(19):10266. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910266
Chicago/Turabian StyleBandela, Vinod, Ram Basany, Anil Kumar Nagarajappa, Sakeenabi Basha, Saraswathi Kanaparthi, Kiran Kumar Ganji, Santosh Patil, Ravi Kumar Gudipaneni, Ghazi Sghaireen Mohammed, and Mohammad Khursheed Alam. 2021. "Evaluation of Stress Distribution and Force in External Hexagonal Implant: A 3-D Finite Element Analysis" International Journal of Environmental Research and Public Health 18, no. 19: 10266. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910266