
Obesogenic Clusters Associated with Weight Status in Brazilian Adolescents of the Movimente School-Base Intervention

 , , and
, , and
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Design and Population
2.2. Cluster Variables
2.2.1. Physical Activity
2.2.2. Sedentary Behavior
2.2.3. Dietary Patterns
2.3. Weight Status
2.4. Sociodemographic Variables
2.5. Statistical Analysis
3. Results
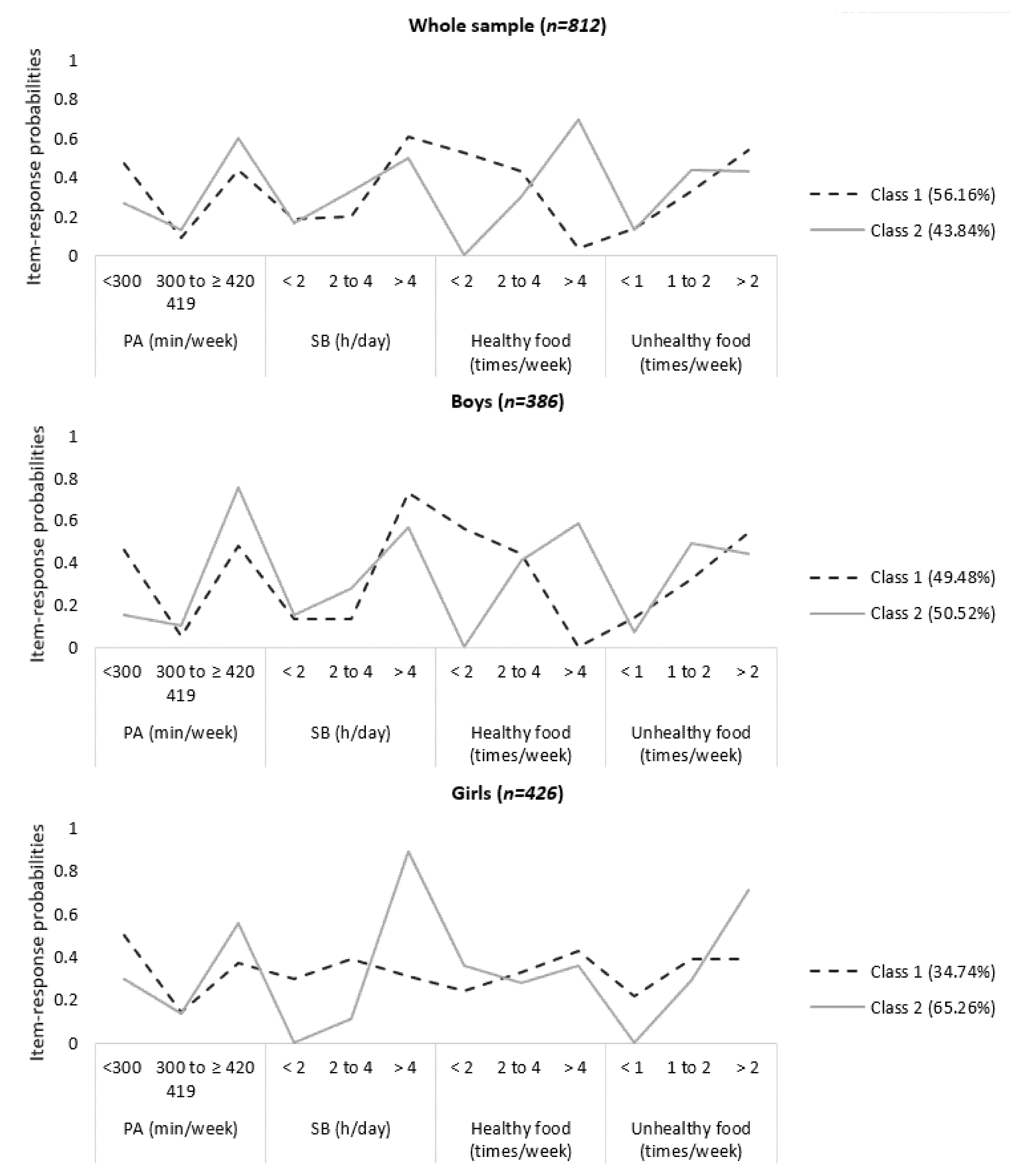
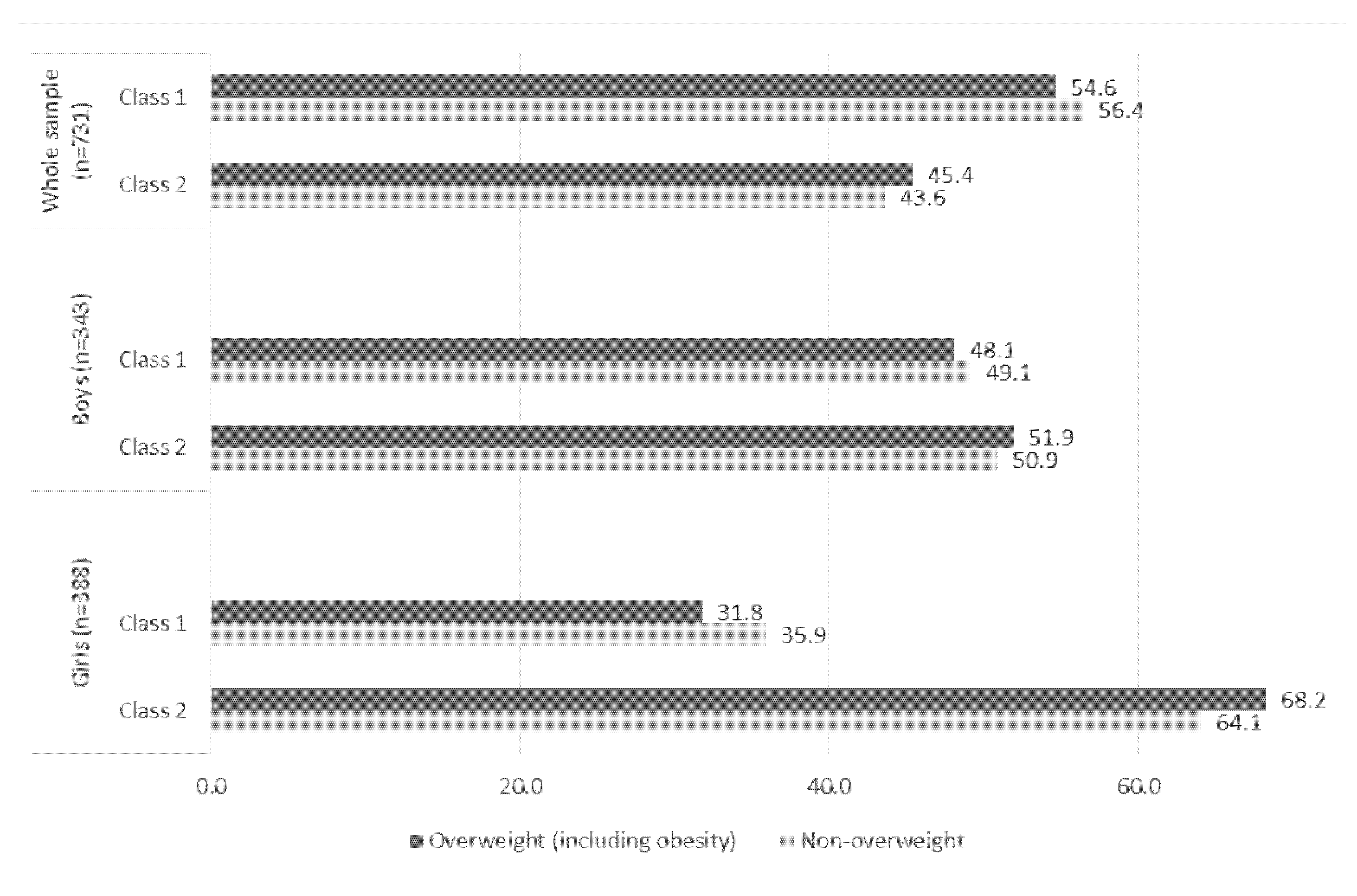
Latent Class Profiles
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The GBD 2015 Obesity Collaborators. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [CrossRef]
- Brazilian Institute of Geography and Statistics (Ed.) National School-Based Health Survey, 2015; IBGE: Rio de Janeiro, Brazil, 2016. [Google Scholar]
- Carlson, J.A.; Crespo, N.C.; Sallis, J.F.; Patterson, R.E.; Elder, J.P. Dietary-Related and Physical Activity-Related Predictors of Obesity in Children: A 2-Year Prospective Study. Child. Obes. 2012, 8, 110–115. [Google Scholar] [CrossRef] [Green Version]
- Leech, R.M.; McNaughton, S.A.; Timperio, A. The clustering of diet, physical activity and sedentary behavior in children and adolescents: A review. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 4. [Google Scholar] [CrossRef] [Green Version]
- Leis, R.; Jurado-Castro, J.M.; Llorente-Cantarero, F.J.; Anguita-Ruiz, A.; Rupérez, A.I.; Bedoya-Carpente, J.J.; Vázquez-Cobela, R.; Aguilera, C.M.; Bueno, G.; Gil-Campos, M. Cluster Analysis of Physical Activity Patterns, and Relationship with Sedentary Behavior and Healthy Lifestyles in Prepubertal Children: Genobox Cohort. Nutrients 2020, 12, 1288. [Google Scholar] [CrossRef] [PubMed]
- Dumuid, D.; Olds, T.; Lewis, L.K.; Martín-Fernández, J.A.; Katzmarzyk, P.; Barreira, T.; Broyles, S.T.; Chaput, J.-P.; Fogelholm, M.; Hu, G.; et al. Health-Related Quality of Life and Lifestyle Behavior Clusters in School-Aged Children from 12 Countries. J. Pediatr. 2017, 183, 178–183.e2. [Google Scholar] [CrossRef] [Green Version]
- Gubbels, J.S.; van Assema, P.; Kremers, S.P.J. Physical Activity, Sedentary Behavior, and Dietary Patterns among Children. Curr. Nutr. Rep. 2013, 2, 105–112. [Google Scholar] [CrossRef] [Green Version]
- Sanchez, A.; Norman, G.J.; Sallis, J.F.; Calfas, K.J.; Cella, J.; Patrick, K. Patterns and Correlates of Physical Activity and Nutrition Behaviors in Adolescents. Am. J. Prev. Med. 2007, 32, 124–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van den Bulck, J.; Hofman, A. The television-to-exercise ratio is a predictor of overweight in adolescents: Results from a prospective cohort study with a two year follow up. Prev. Med. 2009, 48, 368–371. [Google Scholar] [CrossRef] [PubMed]
- Ottevaere, C.; The HELENA Study Group; Huybrechts, I.; Benser, J.; De Bourdeaudhuij, I.; Cuenca-Garcia, M.; Dallongeville, J.; Zaccaria, M.; Gottrand, F.; Kersting, M.; et al. Clustering patterns of physical activity, sedentary and dietary behavior among European adolescents: The HELENA study. BMC Public Healh 2011, 11, 328. [Google Scholar] [CrossRef]
- Matias, T.S.; Silva, K.S.; Da Silva, J.A.; Mello, G.T.; Salmon, J. Clustering of diet, physical activity and sedentary behavior among Brazilian adolescents in the national school—Based health survey (PeNSE 2015). BMC Public Health 2018, 18, 1283. [Google Scholar] [CrossRef]
- Seghers, J.; Rutten, C. Clustering of multiple lifestyle behaviours and its relationship with weight status and cardiorespiratory fitness in a sample of Flemish 11- to 12-year-olds. Public Health Nutr. 2010, 13, 1838–1846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marshall, S.J.; Biddle, S.J.; Sallis, J.F.; McKenzie, T.L.; Conway, T.L. Clustering of Sedentary Behaviors and Physical Activity among Youth: A Cross-National Study. Pediatr. Exerc. Sci. 2002, 14, 401–417. [Google Scholar] [CrossRef]
- Sabbe, D.; De Bourdeaudhuij, I.; Legiest, E.; Maes, L. A cluster-analytical approach towards physical activity and eating habits among 10-year-old children. Health Educ. Res. 2007, 23, 753–762. [Google Scholar] [CrossRef]
- Boone-Heinonen, J.; Gordon-Larsen, P.; Adair, L.S. Obesogenic Clusters: Multidimensional Adolescent Obesity-related Behaviors in the U.S. Ann. Behav. Med. 2008, 36, 217–230. [Google Scholar] [CrossRef] [Green Version]
- Terzian, M.A. Preventing Multiple Risky Behaviors among Adolescents: Seven Strategies. Child Trends 2011, 24, 1–12. [Google Scholar]
- Community Preventive Services Task Force. Reducing Children’s Recreational Sedentary Screen Time. Am. J. Prev. Med. 2016, 50, 416–418. [Google Scholar] [CrossRef] [PubMed]
- Landsberg, B.; Plachta-Danielzik, S.; Lange, D.; Johannsen, M.; Seiberl, J.; Müller, M.J. Clustering of lifestyle factors and association with overweight in adolescents of the Kiel Obesity Prevention Study. Public Health Nutr. 2010, 13, 1708–1715. [Google Scholar] [CrossRef] [Green Version]
- van der Sluis, M.E.; Lien, N.; Twisk, J.W.; Steenhuis, I.H.; Bere, E.; Klepp, K.I.; Wind, M. Longitudinal associations of energy balance-related behaviours and cross-sectional associations of clusters and body mass index in Norwegian adolescents. Public Health Nutr. 2010, 13, 1716–1721. [Google Scholar] [CrossRef]
- Turner, K.; Dwyer, J.J.M.; Edwards, A.M.; Allison, K.R. Clustering of Specific Health-related Behaviours: Among Toronto Adolescents. Can. J. Diet. Pract. Res. 2011, 72, e155–e160. [Google Scholar] [CrossRef] [PubMed]
- Lobo, A.S.; de Assis, M.A.A.; Leal, D.B.; Borgatto, A.F.; Vieira, F.K.; Di Pietro, P.F.; Kupek, E. Empirically derived dietary patterns through latent profile analysis among Brazilian children and adolescents from Southern Brazil, 2013–2015. PLoS ONE 2019, 14, e0210425. [Google Scholar] [CrossRef]
- Silva, K.S.; da Silva, J.A.; Barbosa Filho, V.C.; Dos Santos, P.C.; da Silveira, P.M.; Lopes, M.V.; Salmon, J. Protocol paper for the Movimente school-based program: A cluster-randomized controlled trial targeting physical activity and sedentary behavior among Brazilian adolescents. Medicine (Baltimore) 2020, 99, e21233. [Google Scholar] [CrossRef]
- Farias Júnior JC, D.; Lopes AD, S.; Mota, J.; Santos, M.P.; Ribeiro, J.C.; Hallal, P.C. Validity and reproducibility of a physical activity questionnaire for adolescents: Adapting the SelfAdministered Physical Activity Checklist. Rev. Bras. Epidemiol. 2012, 15, 198–210. [Google Scholar]
- Costa, R.M.; Minatto, G.; Costa, B.G.G.; Silva, K.S. Clustering of 24-h movement behaviors associated with cardiorespiratory fitness among adolescents: A latent class analysis. Eur. J. Nucl. Med. Mol. Imaging 2021, 180, 109–117. [Google Scholar] [CrossRef]
- Silva, K.S.; Lopes, A.D.S.; Hoefelmann, L.P.; Cabral, L.G.D.A.; De Bem, M.F.L.; Barros, M.; Nahas, M.V. Projeto COMPAC (comportamentos dos adolescentes catarinenses): Aspectos. Braz. J. Kinanthropometry Hum. Perform. 2013, 15, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Silva, K.S.; Lopes, A.D.S.; Dumith, S.C.; Garcia, L.M.T.; Bezerra, J.; Nahas, M.V. Changes in television viewing and computers/videogames use among high school students in Southern Brazil between 2001 and 2011. Int. J. Public Health 2013, 59, 77–86. [Google Scholar] [CrossRef]
- Kaiser, H.F. An index of factor simplicity. Psychometrika 1974, 39, 31–36. [Google Scholar] [CrossRef]
- Lohman, T.G.; Roche, A.F.; Martorell, R. Anthropometric standardization reference manual. Cham. Human Kinet. 1992, 24. [Google Scholar] [CrossRef] [Green Version]
- de Onis, M. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ 2007, 85, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, J.B. Latent Class Analysis: An example for reporting results. Res. Soc. Adm. Pharm. 2017, 13, 1196–1201. [Google Scholar] [CrossRef]
- NCD Risk Factor Collaboration. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef] [Green Version]
- Monteiro, L.Z.; Varela, A.R.; Souza, P.D.; Maniçoba AC, M.; Braga Júnior, F. Hábitos alimentares, atividade física e comportamento sedentário entre escolares brasileiros: Pesquisa Nacional de Saúde do Escolar, 2015. Rev. Bras. Epidemiol. 2020, 23, e200034. [Google Scholar] [CrossRef]
- Platat, C.; Perrin, A.-E.; Oujaa, M.; Wagner, A.; Haan, M.-C.; Schlienger, J.-L.; Simon, C. Diet and physical activity profiles in French preadolescents. Br. J. Nutr. 2006, 96, 501–507. [Google Scholar] [PubMed]
- Kelishadi, R. Association of physical activity and dietary behaviours in relation to the body mass index in a national sample of Iranian children and adolescents: CASPIAN Study. Bull. World Health Organ. 2007, 85, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Pate, R.R.; Heath, G.W.; Dowda, M.; Trost, S. Associations between physical activity and other health behaviors in a representative sample of US adolescents. Am. J. Public Health 1996, 86, 1577–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moreno-Gómez, C.; Romaguera, D.; Tauler-Riera, P.; Bennasar-Veny, M.; Pericas-Beltran, J.; Martinez-Andreu, S.; Aguilo-Pons, A. Clustering of lifestyle factors in Spanish university students: The relationship between smoking, alcohol consumption, physical activity and diet quality. Public Health Nutr. 2012, 15, 2131–2139. [Google Scholar] [CrossRef] [Green Version]
- Parsons, T.J.; Power, C.; Manor, O. Longitudinal Physical Activity and Diet Patterns in the 1958 British Birth Cohort. Med. Sci. Sports Exerc. 2006, 38, 547–554. [Google Scholar] [CrossRef]
- Knäuper, B.; Rabiau, M.; Cohen, O.; Patriciu, N. Compensatory health beliefs: Scale development and psychometric properties. Psychol. Health 2004, 19, 607–624. [Google Scholar] [CrossRef]
- Ferrar, K.E.; Olds, T.S.; Walters, J.L. All the Stereotypes Confirmed: Differences in How Australian Boys and Girls Use Their Time. Health Educ. Behav. 2012, 39, 589–595. [Google Scholar] [CrossRef]
- Allender, S.; Cowburn, G.; Foster, C. Understanding participation in sport and physical activity among children and adults: A review of qualitative studies. Health Educ. Res. 2006, 21, 826–835. [Google Scholar] [CrossRef] [Green Version]
- Vance, V.A.; Woodruff, S.; McCargar, L.J.; Husted, J.; Hanning, R.M. Self-reported dietary energy intake of normal weight, overweight and obese adolescents. Public Health Nutr. 2009, 12, 222–227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberali, R.; Del Castanhel, F.; Kupek, E.; Assis, M.A.A. Latent Class Analysis of Lifestyle Risk Factors and Association with Overweight and/or Obesity in Children and Adolescents: Systematic Review. Child. Obes. 2021, 17, 2–15. [Google Scholar] [CrossRef] [PubMed]
- Sylvia, L.G.; Bernstein, E.E.; Hubbard, J.L.; Keating, L.; Anderson, E.J. Practical Guide to Measuring Physical Activity. J. Acad. Nutr. Diet. 2014, 114, 199–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Velde, G.T.; Plasqui, G.; Willeboordse, M.; Winkens, B.; Vreugdenhil, A. Associations between physical activity, sedentary time and cardiovascular risk factors among Dutch children. PLoS ONE 2021, 16, e0256448. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, S. Weekly patterns, diet quality and energy balance. Physiol. Behav. 2014, 134, 55–59. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variables | Total Sample (n = 731) | Boys (n = 343) | Girls (n = 388) | |||
|---|---|---|---|---|---|---|
| Age (Mean ± sd) | 13.0 ± 1.04 | 13.1 ± 1.06 | 13.1 ± 1.02 | |||
| % (95% CI) | ||||||
| Maternal level education | ||||||
| Low | 24.2 | (21.2, 27.4) | 21.8 | (17.7, 26.5) | 26.2 | (22.1, 30.9) |
| Medium | 27.6 | (24.5, 30.9) | 27.9 | (23.4, 33.0) | 27.3 | (23.0, 31.9) |
| High | 18.3 | (15.6, 21.3) | 19.2 | (15.3, 23.7) | 17.5 | (14.0, 21.6) |
| Unknown | 29.8 | (26.6, 32.2) | 30 | (26.2, 36.0) | 28.8 | (24.5, 33.5) |
| PA (min/week) | ||||||
| <300 | 38.6 | (35.4, 41.8) | 30.1 | (25.6, 34.8) | 43.9 | (39.2, 48.6) |
| 300 to 419 | 10.6 | (8.7, 12.7) | 7.5 | (5.2, 10.6) | 13.9 | (10.8, 17.4) |
| ≥420 | 50.8 | (47.5, 54.1) | 62.4 | (57.4, 67.1) | 42.3 | (37.6, 47.0) |
| SB (h/day) | ||||||
| <2 | 18.3 | (15.8, 20.9) | 14.3 | (11.0, 18.1) | 21.4 | (17.7, 25.5) |
| 2 to 4 | 25.8 | (23.0, 28.8) | 20.7 | (16.9, 25.0) | 31.0 | (26.7, 35.5) |
| >4 | 55.9 | (52.6, 59.1) | 65.0 | (60.1, 69.6) | 47.7 | (42.9, 52.4) |
| F&V (times/week) | ||||||
| <2 | 27.5 | (24.6, 30.4) | 26.9 | (22.7, 31.6) | 27.5 | (23.4, 31.9) |
| 2 to 4 | 36.3 | (33.1, 39.5) | 42.5 | (37.6, 47.4) | 31.9 | (27.6, 36.5) |
| >4 | 36.3 | (33.1, 39.5) | 30.6 | (26.1, 35.3) | 40.6 | (36.0, 45.3) |
| SSS (times/ week) | ||||||
| <1 | 12.9 | (10.8, 15.2) | 10.4 | (7.68, 13.8) | 15.5 | (12.3, 19.2) |
| 1 to 2 | 38.1 | (34.9, 41.3) | 40.9 | (36.1, 45.9) | 35.9 | (31.4, 40.6) |
| >2 | 49.0 | (45.7, 52.3) | 48.7 | (43.7, 53.7) | 48.6 | (43.8, 53.3) |
| Weight status | ||||||
| Non-overweight | 65.7 | (62.4, 68.7) | 63.1 | (58.3, 67.6) | 68.0 | (63.5, 72.2) |
| Overweight (including obesity) | 34.4 | (31.2, 37.5) | 36.9 | (32.3, 41.6) | 32.0 | (27.7, 36.4) |
| Classes | Overweight (Including Obesity) | |||
|---|---|---|---|---|
| Crude | Adjust | |||
| OR | 95% CI | OR | 95% CI | |
| Whole sample | ||||
| Class 1 | 1 | 1 | ||
| Class 2 | 1.11 | (0.82, 1.51) | 1.15 | (0.84, 1.57) |
| Boys | ||||
| Class 1 | 1 | 1 | ||
| Class 2 | 1.19 | (0.76, 1.86) | 1.24 | (0.78, 1.97) |
| Girls | ||||
| Class 1 | 1 | 1 | ||
| Class 2 | 1.27 | (0.80, 2.02) | 1.24 | (0.77, 1.99) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Mello, G.T.; Silva, K.S.; Matias, T.S.; de Assis, M.A.A.; Borgatto, A.F. Obesogenic Clusters Associated with Weight Status in Brazilian Adolescents of the Movimente School-Base Intervention. Int. J. Environ. Res. Public Health 2021, 18, 10350. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910350
de Mello GT, Silva KS, Matias TS, de Assis MAA, Borgatto AF. Obesogenic Clusters Associated with Weight Status in Brazilian Adolescents of the Movimente School-Base Intervention. International Journal of Environmental Research and Public Health. 2021; 18(19):10350. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910350
Chicago/Turabian Stylede Mello, Gabrielli Thais, Kelly Samara Silva, Thiago Sousa Matias, Maria Alice Altenburg de Assis, and Adriano Ferreti Borgatto. 2021. "Obesogenic Clusters Associated with Weight Status in Brazilian Adolescents of the Movimente School-Base Intervention" International Journal of Environmental Research and Public Health 18, no. 19: 10350. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph181910350