The Effect of Two Bed Bath Practices in Cost and Vital Signs of Critically Ill Patients


Abstract
:1. Introduction
2. Materials and Methods
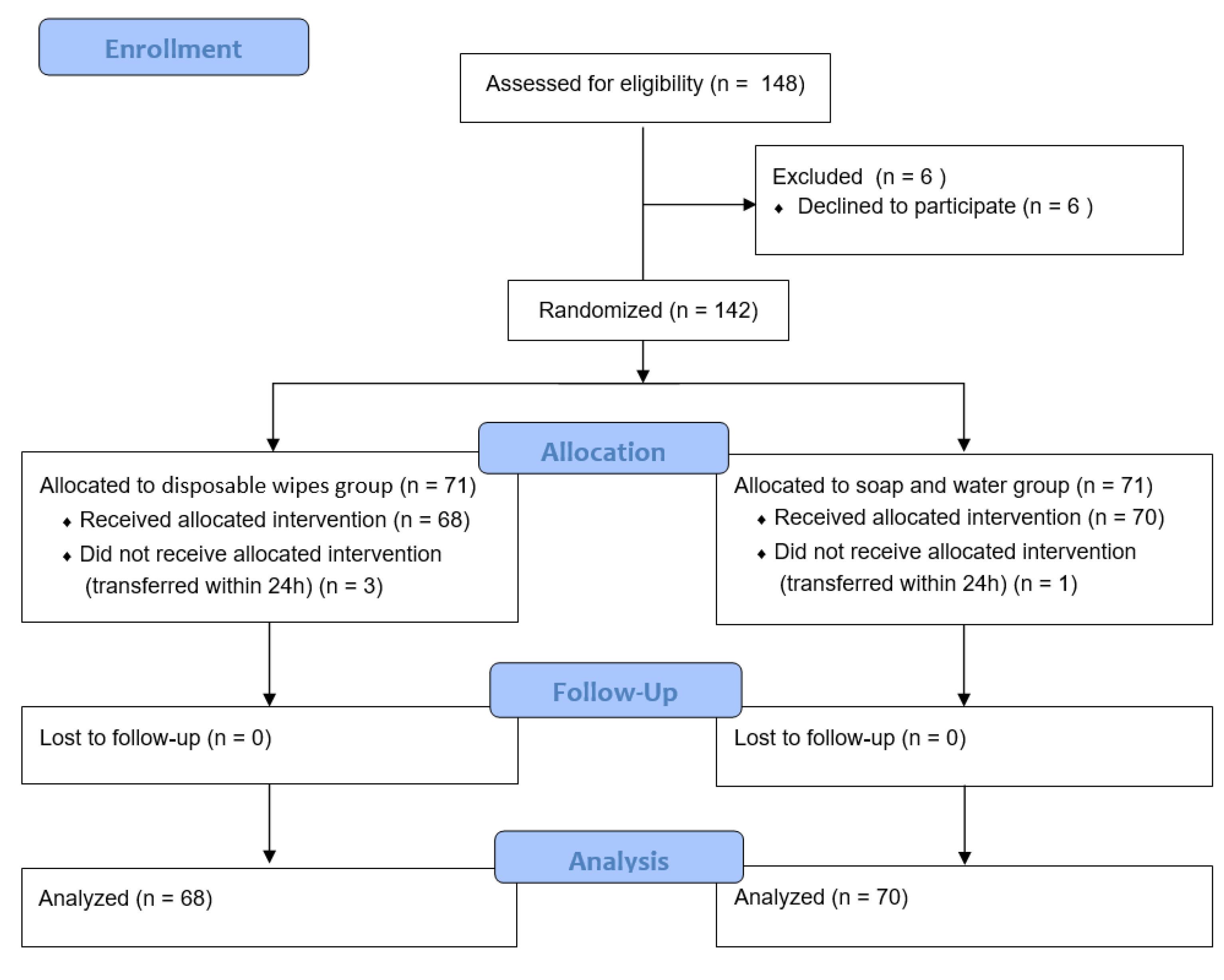
2.1. Study Design and Participants
2.2. Data Collection
2.3. Study Procedure
2.4. Statistical Analysis
3. Results
3.1. General Characteristics of the Participants
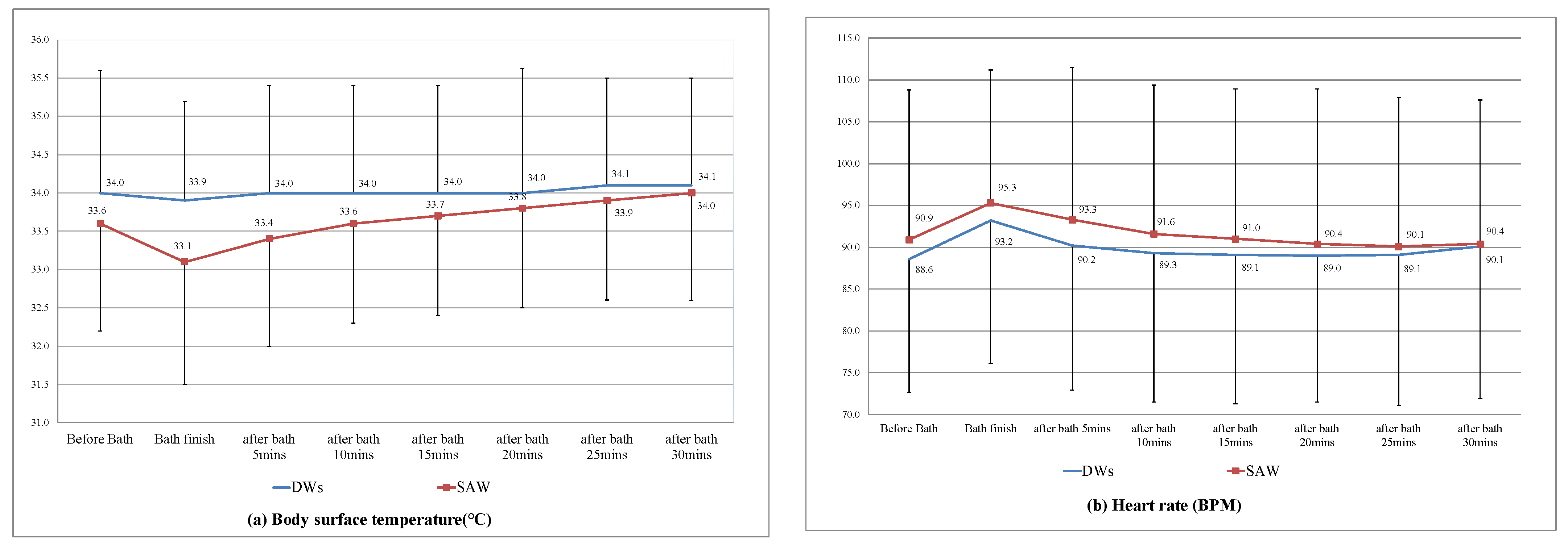
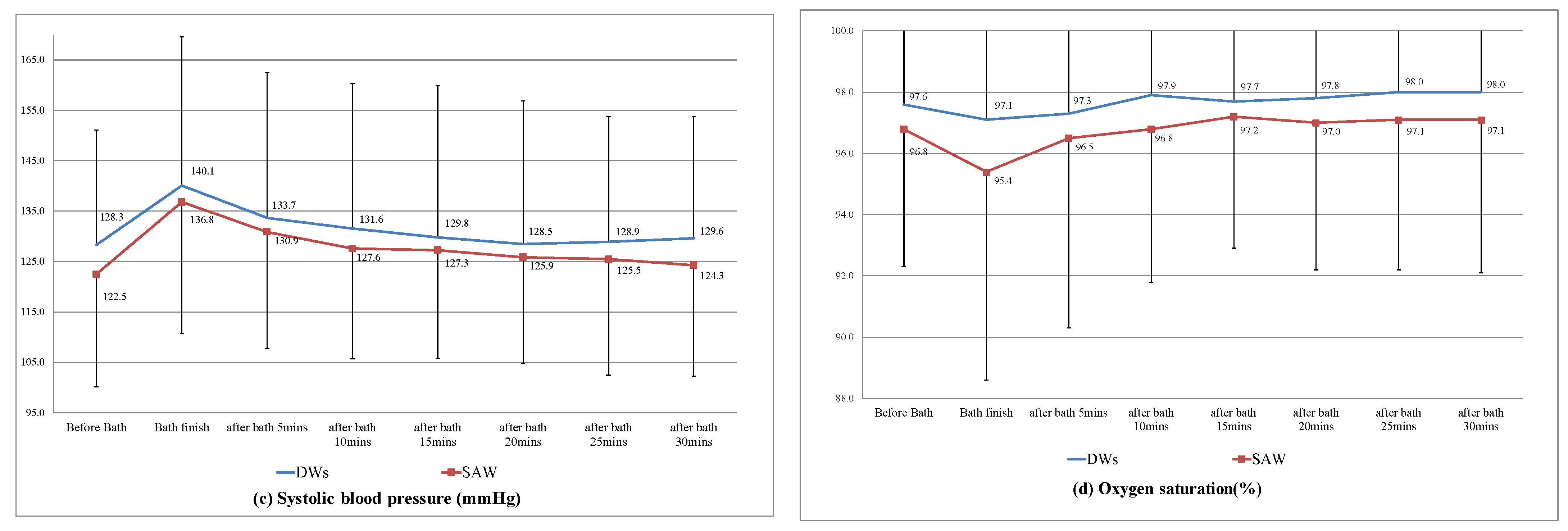
3.2. Bath Duration, Cost, and Vital Signs
3.3. Staff Satisfaction
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Haque, M.; McKimm, J.; Sartelli, M.; Dhingra, S.; Labricciosa, F.M.; Islam, S.; Jahan, D.; Nusrat, T.; Chowdhury, T.S.; Coccolini, F.; et al. Strategies to Prevent Healthcare-Associated Infections: A Narrative Overview. Risk Manag. Healthc. Policy 2020, 13, 1765–1780. [Google Scholar] [CrossRef] [PubMed]
- Kaye, K.S.; Marchaim, D.; Chen, Y.T.; Baures, T.; Anderson, D.J.; Choi, Y.; Sloane, R.; Schmader, K.E. Effect of nosocomial bloodstream infections on mortality, length of stay, and hospital costs in older adults. J. Am. Geriatr. Soc. 2014, 62, 306–311. [Google Scholar] [CrossRef] [PubMed]
- Lee, X.J.; Stewardson, A.J.; Worth, L.J.; Graves, N.; Wozniak, T.M. Attributable length of stay, mortality risk and costs of bacterial healthcare-associated infections in Australia: A retrospective case-cohort study. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef]
- Al-Tawfiq, J.A.; Tambyah, P.A. Healthcare associated infections (HAI) perspectives. J. Infect. Public Health 2014, 7, 339–344. [Google Scholar] [CrossRef] [Green Version]
- Lloyd Jones, M. Personal hygiene 3.4: Assisting with bathing. Br. J. Healthc. Assist. 2014, 8, 439–440. [Google Scholar] [CrossRef]
- Schoonhoven, L.; van Gaal, B.G.I.; Teerenstra, S.; Adang, E.; van der Vleuten, C.; van Achterberg, T. Cost-consequence analysis of “washing without water” for nursing home residents: A cluster randomized trial. Int. J. Nurs. Stud. 2015, 52, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Larson, E.L.; Ciliberti, T.; Chantler, C.; Abraham, J.; Lazaro, E.M.; Venturanza, M.; Pancholi, P. Comparison of traditional and disposable bed baths in critically ill patients. Am. J. Crit. Care 2004, 13, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Coyer, F.M.; O’Sullivan, J.; Cadman, N. The provision of patient personal hygiene in the intensive care unit: A descriptive exploratory study of bed-bathing practice. Aust. Crit. Care 2011, 24, 198–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marchaim, D.; Taylor, A.R.; Hayakawa, K.; Bheemreddy, S.; Sunkara, B.; Moshos, J.; Chopra, T.; Abreu-Lanfranco, O.; Martin, E.T.; Pogue, J.M.; et al. Hospital bath basins are frequently contaminated with multidrug-resistant human pathogens. Am. J. Infect. Control 2012, 40, 562–564. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.; Lineweaver, L.; Maze, L.M. Patients’ bath basins as potential sources of infection: A multicenter sampling study. Am. J. Crit. Care 2009, 18, 31–38, 41. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.-C.; Wang, Q.-J.; Lin, L.-G.; Liu, Y.-Y.; Liao, S.-C.; Tsou, Y.-C. Using Disposable Bathing Wipes to Improve Bathing for Critically Ill Patients. VGH Nurs. 2018, 35, 145–151. [Google Scholar]
- Groven, F.M.V.; Zwakhalen, S.M.G.; Odekerken-Schröder, G.; Joosten, E.J.T.; Hamers, J.P.H. How does washing without water perform compared to the traditional bed bath: A systematic review. BMC Geriatr. 2017, 17, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veje, P.L.; Chen, M.; Jensen, C.S.; Sørensen, J.; Primdahl, J. Bed bath with soap and water or disposable wet wipes: Patients’ experiences and preferences. J. Clin. Nurs. 2019. [Google Scholar] [CrossRef] [PubMed]
- de Lima Lopes, J.; Nogueira-Martins, L.A.; Gonçalves, M.A.B.; de Barros, A.L.B.L. Comparing levels of anxiety during bed and shower baths in patients with acute myocardial infarction. Rev. Lat. Am. Enferm. 2010, 18, 217–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noddeskou, L.H.; Hemmingsen, L.E.; Hordam, B. Elderly patients’ and nurses’ assessment of traditional bed bath compared to prepacked single units—Randomised controlled trial. Scand. J. Caring Sci. 2015, 29, 347–352. [Google Scholar] [CrossRef] [PubMed]
- Tai, C.-H.; Yu, L.-Y.; Hsu, H.-Y.; Lu, C.-W.; Chen, H.-L. Comparison of Body Temperature and Heart Rate Variations between Two Bed Bathing Practices for Critically Ill Patients: A Pilot Study. Tzu Chi Nurs. J. 2019, 18, 63–74. [Google Scholar]
- Veje, P.L.; Chen, M.; Jensen, C.S.; Sørensen, J.; Primdahl, J. Effectiveness of two bed bath methods in removing microorganisms from hospitalized patients: A prospective randomized crossover study. Am. J. Infect. Control 2020, 48, 638–643. [Google Scholar] [CrossRef] [PubMed]
- Lopes, J.L.; Nogueira-Martins, L.A.; de Barros, A.L. Bed and shower baths: Comparing the perceptions of patients with acute myocardial infarction. J. Clin. Nurs. 2013, 22, 733–740. [Google Scholar] [CrossRef] [PubMed]
- Frazier, S.K.; Moser, D.K.; Riegel, B.; McKinley, S.; Blakely, W.; An Kim, K.; Garvin, B.J. Critical care nurses’ assessment of patients’ anxiety: Reliance on physiological and behavioral parameters. Am. J. Crit. Care 2002, 11, 57–64. [Google Scholar] [CrossRef] [PubMed]
- El-Soussi, A.H.; Asfour, H.I. Examining bed-bath practices of critically ill patients. J. Nurs. Educ. Pract. 2016, 6. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | Total Participants (N = 138) | DWs Bath (n = 68) | SAW Bath (n = 70) | p-Value |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | ||
| Age [M (SD)] | 67.6 (15.3) | 65.4 (15.8) | 69.6 (14.6) | 0.11 |
| Sex | 0.88 | |||
| Female | 60 (43.5) | 30 (44.1) | 30 (42.9) | |
| Male | 78 (56.5) | 38 (55.9) | 40 (57.1) | |
| Diabetes History | 0.25 | |||
| Yes | 45 (32.6) | 19 (27.9) | 26 (37.1) | |
| No | 93 (67.4) | 49 (72.1) | 44 (62.9) | |
| Cardiovascular Disease History | 0.17 | |||
| Yes | 89 (64.5) | 40 (58.8) | 49 (70.0) | |
| No | 49 (35.5) | 28 (41.2) | 21 (30.0) | |
| Respiratory Disease History | 0.34 | |||
| Yes | 29 (21.0) | 12 (17.6) | 17 (24.3) | |
| No | 109 (79.0) | 56 (82.4) | 53 (75.7) | |
| Catheter Retention Status | ||||
| Endotracheal tube | 102 (73.9) | 50 (73.5) | 52 (74.3) | 0.92 |
| Central venous catheter | 88 (63.8) | 44 (64.7) | 44 (62.9) | 0.82 |
| Urinary catheter | 124 (89.9) | 61 (89.7) | 63 (90.0) | 0.95 |
| M (SD) | M (SD) | M (SD) | p-Value | |
| APACHE II | 23.8 (7.0) | 23.5 (8.0) | 24.0 (6.0) | 0.68 |
| BMI | 24.5 (5.9) | 23.8 (5.4) | 25.2 (6.4) | 0.18 |
| WBC (103/uL) | 13.0 (7.5) | 13.1 (7.7) | 13.0 (7.4) | 0.97 |
| Hb (g/dL) | 10.6 (2.6) | 10.6 (3.0) | 10.7 (2.2) | 0.79 |
| PT (sec) | 15.1 (11.4) | 15.3 (13.5) | 14.9 (9.1) | 0.87 |
| Na (mmol/L) | 139.1 (7.6) | 140.0 (8.8) | 138.3 (6.2) | 0.18 |
| K (mmol/L) | 4.2 (1.1) | 4.0 (1.1) | 4.3 (1.1) | 0.19 |
| BUN (mg/dL) | 46.2 (39.9) | 42.2 (41.1) | 50.2 (38.6) | 0.24 |
| Creatinine (mg/dL) | 2.4 (2.7) | 2.0 (1.9) | 2.8 (3.3) | 0.11 |
| Albumin (g/dL) | 3.1 (0.6) | 3.1 (0.5) | 3.1 (0.7) | 0.69 |
| CRP (mg/dL) | 9.9 (9.2) | 9.4 (8.7) | 10.3 (9.6) | 0.61 |
| Lactate (mg/dL) | 3.8 (3.9) | 4.1 (4.6) | 3.4 (2.8) | 0.31 |
| DWs Bath (n = 68) | SAW Bath (n = 70) | p-Value | |
|---|---|---|---|
| Variable | n (%) | n (%) | |
| Duration of bath [min (SD)] | 23.8 (7.5) | 34.4 (9.2) | <0.01 * |
| Bath cost [NTD/bath (SD)] | 237.9 (45.0) | 255.3 (31.5) | 0.01 * |
| Cost of bath consumables a | 124.9 (14.4) | 66.7 (14.0) | <0.01 * |
| Clothing cost | 33.7 (21.4) | 74.1 (9.3) | <0.01 * |
| Cost of nursing time | 79.2 (25.1) | 114.5 (30.7) | <0.01 * |
| Item | DWs Bath N (%) | SAW Bath N (%) | No Difference N (%) | p-Value |
|---|---|---|---|---|
| Convenient use | 32 (91.4) | 0 | 3 (8.6) | <0.001 * |
| Lower bath duration | 33 (94.3) | 0 | 2 (5.7) | <0.001 * |
| More comfortable for patients | 9 (25.8) | 20 (57.1) | 6 (17.1) | <0.001 * |
| Cleaner results | 6 (17.2) | 25 (71.4) | 4 (11.4) | <0.001 * |
| Overall preference for bath method | 22 (64.7) | 7 (20.6) | 5 (14.7) | <0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tai, C.-H.; Hsieh, T.-C.; Lee, R.-P. The Effect of Two Bed Bath Practices in Cost and Vital Signs of Critically Ill Patients. Int. J. Environ. Res. Public Health 2021, 18, 816. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020816
Tai C-H, Hsieh T-C, Lee R-P. The Effect of Two Bed Bath Practices in Cost and Vital Signs of Critically Ill Patients. International Journal of Environmental Research and Public Health. 2021; 18(2):816. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020816
Chicago/Turabian StyleTai, Chia-Hui, Tsung-Cheng Hsieh, and Ru-Ping Lee. 2021. "The Effect of Two Bed Bath Practices in Cost and Vital Signs of Critically Ill Patients" International Journal of Environmental Research and Public Health 18, no. 2: 816. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18020816