
Reliability of Repeated Trials Protocols for Body Composition Assessment by Air Displacement Plethysmography


 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. ADP Measurements
2.3. Repeated Trials Protocols
2.4. Statistical Analysis
3. Results
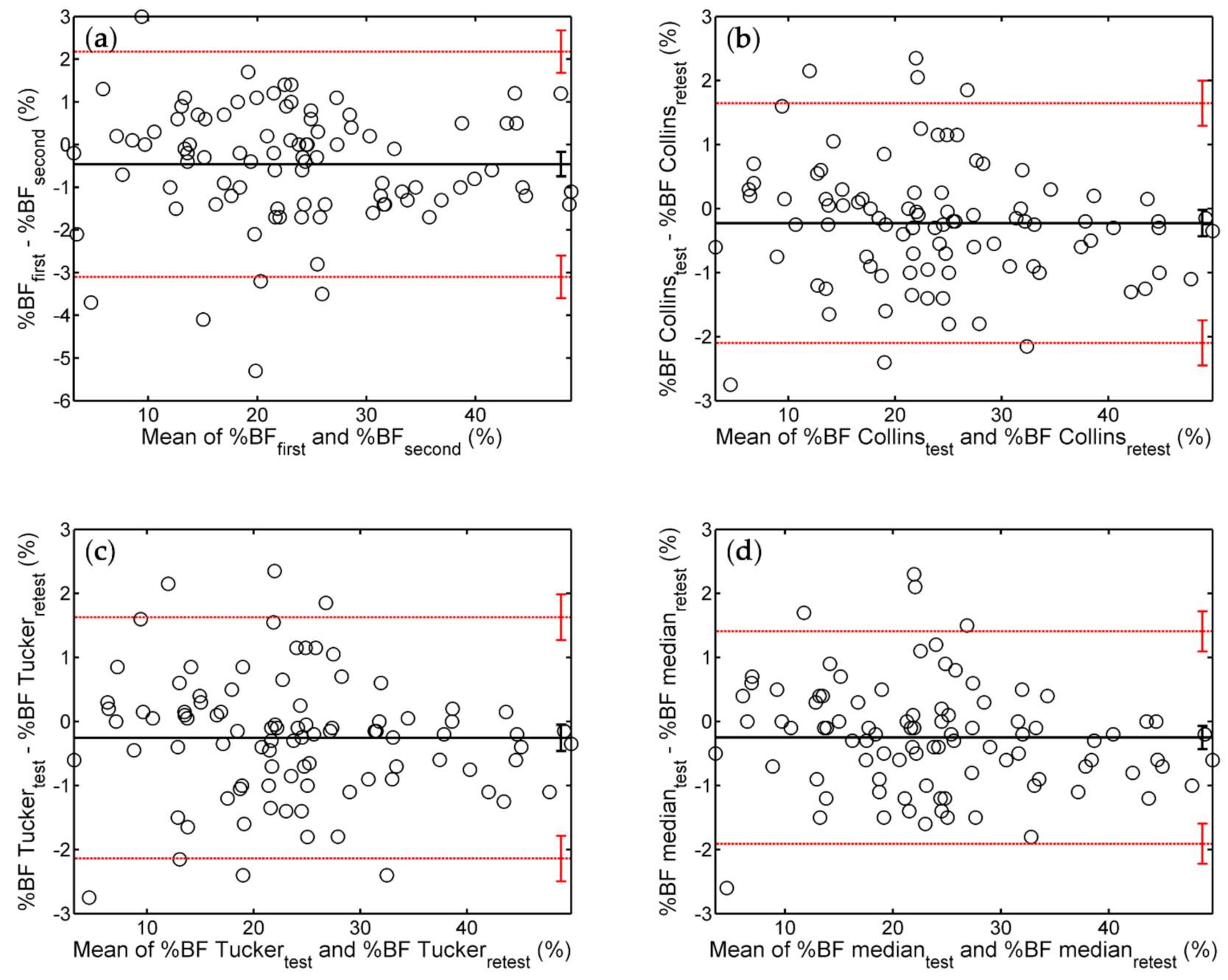
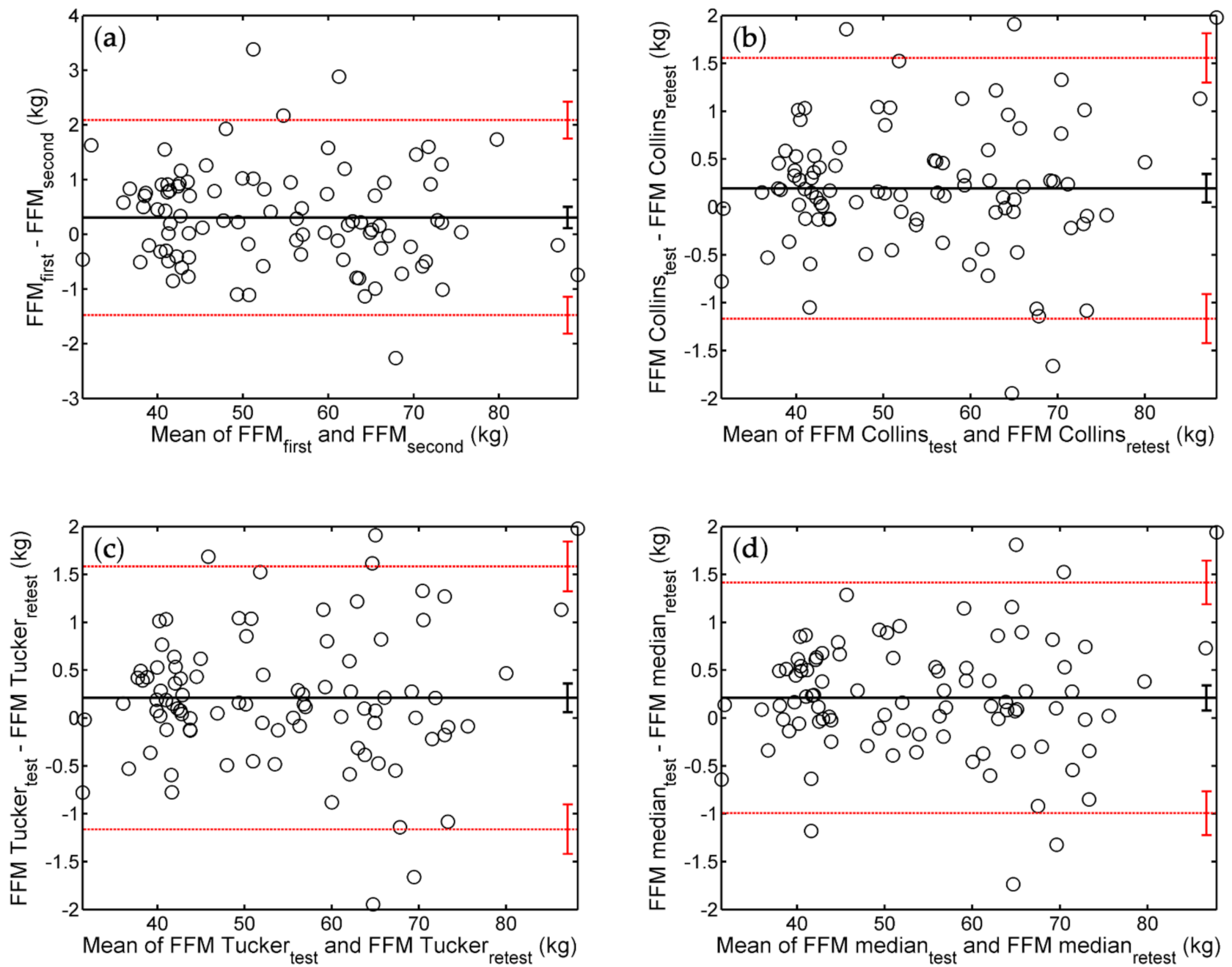
3.1. Bland–Altman Analysis of Repeatability
3.2. Absolute and Relative Measures of Reliability
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ackland, T.R.; Lohman, T.G.; Sundgot-Borgen, J.; Maughan, R.J.; Meyer, N.L.; Stewart, A.D.; Müller, W. Current status of body composition assessment in sport. Sports Med. 2012, 42, 227–249. [Google Scholar] [CrossRef]
- Muller, M.J.; Braun, W.; Enderle, J.; Bosy-Westphal, A. Beyond BMI: Conceptual Issues Related to Overweight and Obese Patients. Obes. Facts 2016, 9, 193–205. [Google Scholar] [CrossRef]
- Johnson, K.O.; Holliday, A.; Mistry, N.; Cunniffe, A.; Howard, K.; Stanger, N.; O’Mahoney, L.L.; Matu, J.; Ispoglou, T. An Increase in Fat-Free Mass is Associated with Higher Appetite and Energy Intake in Older Adults: A Randomised Control Trial. Nutrients 2021, 13, 141. [Google Scholar] [CrossRef]
- Barrientos, G.; Alves, J.; Toro, V.; Robles, M.C.; Muñoz, D.; Maynar, M. Association between Trace Elements and Body Composition Parameters in Endurance Runners. Int. J. Environ. Res. Public Health 2020, 17, 6563. [Google Scholar] [CrossRef] [PubMed]
- Müller, M.J.; Geisler, C.; Heymsfield, S.B.; Bosy-Westphal, A. Recent advances in understanding body weight homeostasis in humans. F1000Research 2018, 7, F1000 Faculty Rev-1025. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dempster, P.; Aitkens, S. A new air displacement method for the determination of human body composition. Med. Sci. Sports Exerc. 1995, 27, 1692–1697. [Google Scholar] [CrossRef] [PubMed]
- McCrory, M.A.; Gomez, T.D.; Bernauer, E.M.; Mole, P.A. Evaluation of a new air displacement plethysmograph for measuring human body composition. Med. Sci. Sports Exerc. 1995, 27, 1686–1691. [Google Scholar] [CrossRef] [Green Version]
- Fields, D.A.; Gunatilake, R.; Kalaitzoglou, E. Air displacement plethysmography: Cradle to grave. Nutr. Clin. Pract. 2015, 30, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Müller, M.J.; Geisler, C.; Hübers, M.; Pourhassan, M.; Bosy-Westphal, A. Body composition-related functions: A problem-oriented approach to phenotyping. Eur. J. Clin. Nutr. 2018, 73, 179–186. [Google Scholar] [CrossRef] [PubMed]
- Müller, M.J.; Bosy-Westphal, A. Effect of Over- and Underfeeding on Body Composition and Related Metabolic Functions in Humans. Curr. Diab. Rep. 2019, 19, 108. [Google Scholar] [CrossRef]
- Schubert, M.M.; Seay, R.F.; Spain, K.K.; Clarke, H.E.; Taylor, J.K. Reliability and validity of various laboratory methods of body composition assessment in young adults. Clin. Physiol. Funct. Imaging 2018, 39, 150–159. [Google Scholar] [CrossRef]
- Collins, A.L.; McCarthy, H.D. Evaluation of factors determining the precision of body composition measurements by air displacement plethysmography. Eur. J. Clin. Nutr. 2003, 57, 770–776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miyatake, N.; Nonaka, K.; Fujii, M. A new air displacement plethysmograph for the determination of Japanese body composition. Diabetes Obes. Metab. 1999, 1, 347–351. [Google Scholar] [CrossRef] [PubMed]
- Noreen, E.E.; Lemon, P.W.R. Reliability of air displacement plethysmography in a large, heterogeneous sample. Med. Sci. Sports Exerc. 2006, 38, 1505–1509. [Google Scholar] [CrossRef]
- Wells, J.C.; Fuller, N.J. Precision of measurement and body size in whole-body air-displacement plethysmography. Int. J. Obes. Relat. Metab. Disord. 2001, 25, 1161–1167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fields, D.A.; Goran, M.I.; McCrory, M.A. Body-composition assessment via air-displacement plethysmography in adults and children: A review. Am. J. Clin. Nutr. 2002, 75, 453–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tucker, L.A.; Lecheminant, J.D.; Bailey, B.W. Test-retest reliability of the Bod Pod: The effect of multiple assessments. Percept. Mot. Skills 2014, 118, 563–570. [Google Scholar] [CrossRef]
- Weir, J.P. Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. J. Strength Cond. Res. 2005, 19, 231–240. [Google Scholar] [CrossRef]
- Hopkins, W.G. Measures of reliability in sports medicine and science. Sports Med. 2000, 30, 1–15. [Google Scholar] [CrossRef] [Green Version]
- COSMED. BOD POD Gold Standard Body Composition Tracking System Operator’s Manual-P/N 210-2400 Rev. M-DCO 1765; COSMED USA, Inc.: Concord, CA, USA, 2015. [Google Scholar]
- Nelson, K.M.; Weinsier, R.L.; Long, C.L.; Schutz, Y. Prediction of resting energy expenditure from fat-free mass and fat mass. Am. J. Clin. Nutr. 1992, 56, 848–856. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef] [PubMed]
- Bland, M.J.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 327, 307–310. [Google Scholar] [CrossRef]
- Gerke, O. Reporting Standards for a Bland-Altman Agreement Analysis: A Review of Methodological Reviews. Diagnostics 2020, 10, 334. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-Y. Statistical notes for clinical researchers: Evaluation of measurement error 2: Dahlberg’s error, Bland-Altman method, and Kappa coefficient. Restor. Dent. Endod. 2013, 38, 182–185. [Google Scholar] [CrossRef]
- Eliasziw, M.; Young, S.L.; Woodbury, M.G.; Fryday-Field, K. Statistical Methodology for the Concurrent Assessment of Interrater and Intrarater Reliability: Using Goniometric Measurements as an Example. Phys. Ther. 1994, 74, 777–788. [Google Scholar] [CrossRef] [PubMed]
- Hollman, J.H.; Beckman, B.A.; Brandt, R.A.; Merriwether, E.N.; Williams, R.T.; Nordrum, J.T. Minimum Detectable Change in Gait Velocity during Acute Rehabilitation following Hip Fracture. J. Geriatr. Phys. Ther. 2008, 31, 53–56. [Google Scholar] [CrossRef]
- Peeters, M.W. Subject positioning in the BOD POD® only marginally affects measurement of body volume and estimation of percent body fat in young adult men. PLoS ONE 2012, 7, e32722. [Google Scholar] [CrossRef] [Green Version]
- Peeters, M.W.; Claessens, A.L. Effect of deviating clothing schemes on the accuracy of body composition measurements by air-displacement plethysmography. Int. J. Body Compos. Res. 2009, 7, 123–129. [Google Scholar]
- Anderson, D.E. Reliability of air displacement plethysmography. J. Strength Cond. Res. 2007, 21, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Gibson, A.L.; Roper, J.L.; Mermier, C.M. Intraindividual Variability in Test-Retest Air Displacement Plethysmography Measurements of Body Density for Men and Women. Int. J. Sport Nutr. Exerc. Metab. 2016, 26, 404–412. [Google Scholar] [CrossRef]
- Kasper, A.M.; Langan-Evans, C. Come Back Skinfolds, All Is Forgiven: A Narrative Review of the Efficacy of Common Body Composition Methods in Applied Sports Practice. Nutrients 2021, 13, 1075. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| All (n = 92) | Men (n = 46) | Women (n = 46) | |
|---|---|---|---|
| Age (y) | 30.4 ± 10.4 [20.0, 66.5] | 29.6 ± 7.7 [20.3, 54.9] | 31.2 ± 12.7 [20.0, 66.5] |
| Height (m) | 1.71 ± 0.10 [1.49, 1.92] | 1.79 ± 0.06 [1.69, 1.92] | 1.63 ± 0.06 [1.49, 1.77] |
| BM 1 (kg) | 71.6 ± 17.2 [38.0, 156.0] | 80.6 ± 17.1 [57.5, 156.0] | 62.6 ± 11.9 [38.0, 94.4] |
| BMI(kg/m2) | 24.3 ± 4.6 [16.7, 45.1] | 25.0 ± 4.6 [17.7, 45.1] | 23.6 ± 4.6 [16.7, 33.7] |
| BV (L) | 68.6 ± 17.1 [35.7, 155.4] | 76.4 ± 17.7 [53.0, 155.4] | 60.9 ± 12.5 [35.7, 94.9] |
| BSA (m2) | 1.83 ± 0.24 [1.28, 2.72] | 1.99 ± 0.20 [1.66, 2.72] | 1.67 ± 0.15 [1.28, 2.06] |
| %BF 2 (%) | 23.9 ± 10.8 [2.9, 49.6] | 18.1 ± 8.8 [2.9, 42.9] | 29.7 ± 9.5 [13.1, 49.6] |
| FFM 2 (kg) | 54.1 ± 13.2 [31.0, 89.2] | 65.0 ± 8.5 [50.6, 89.2] | 43.3 ± 6.3 [31.0, 68.6] |
| Protocol | %BF (%) | FFM (kg) | |||
|---|---|---|---|---|---|
| Bias [95% CI] | ULA [95% CI] | Bias [95% CI] | ULA [95% CI] | ||
| All | Single | −0.46 [−0.75, −0.17] | 2.18 [1.68, 2.68] | 0.305 [0.111, 0.499] | 2.089 [1.752, 2.425] |
| Collins | −0.23 [−0.43, −0.03] | 1.64 [1.29, 2.00] | 0.194 [0.046, 0.343] | 1.556 [1.299, 1.813] | |
| Tucker | −0.25 [−0.46, −0.05] | 1.63 [1.27, 1.98] | 0.211 [0.061, 0.360] | 1.583 [1.324, 1.842] | |
| Median | −0.25 [−0.43, −0.07] | 1.40 [1.09, 1.72] | 0.210 [0.079, 0.341] | 1.415 [1.188, 1.643] | |
| Men | Single | −0.30 [−0.68, 0.07] | 2.10 [1.45, 2.74] | 0.237 [−0.050, 0.524] | 2.093 [1.595, 2.591] |
| Collins | −0.17 [−0.45, 0.12] | 1.66 [1.17, 2.14] | 0.175 [−0.059, 0.409] | 1.683 [1.279, 2.088] | |
| Tucker | −0.20 [−0.50, 0.09] | 1.70 [1.19, 2.21] | 0.202 [−0.041, 0.444] | 1.766 [1.346, 2.186] | |
| Median | −0.19 [−0.45, 0.06] | 1.46 [1.01, 1.90] | 0.199 [−0.014, 0.412] | 1.574 [1.205, 1.943] | |
| Women | Single | −0.62 [−1.06, −0.18] | 2.23 [1.47, 2.99] | 0.373 [0.107, 0.639] | 2.092 [1.630, 2.553] |
| Collins | −0.29 [−0.58, 0.01] | 1.64 [1.12, 2.16] | 0.227 [0.041, 0.413] | 1.427 [1.105, 1.749] | |
| Tucker | −0.32 [−0.61, −0.03] | 1.57 [1.06, 2.08] | 0.220 [0.039, 0.401] | 1.387 [1.074, 1.700] | |
| Median | −0.31 [−0.57, −0.05] | 1.37 [0.92, 1.82] | 0.222 [0.063, 0.380] | 1.244 [0.970, 1.519] | |
| Protocol | BV (L) | RMR (Kcal/Day) | |||
|---|---|---|---|---|---|
| Bias [95% CI] | ULA [95% CI] | Bias [95% CI] | ULA [95% CI] | ||
| All | Single | −0.051 [−0.091, −0.012] | 0.312 [0.244, 0.381] | 6.728 [2.505, 10.952] | 45.489 [38.173, 52.805] |
| Collins | −0.014 [−0.043, 0.016] | 0.259 [0.207, 0.310] | 4.136 [0.959, 7.313] | 33.290 [27.787, 38.792] | |
| Tucker | −0.020 [−0.050, 0.011] | 0.260 [0.206, 0.312] | 4.739 [1.478, 8] | 34.663 [29.015, 40.311] | |
| Median | −0.019 [−0.045, 0.007] | 0.224 [0.178, 0.269] | 4.598 [1.750, 7.446] | 30.735 [25.802, 35.668] | |
| Men | Single | −0.036 [−0.094, 0.023] | 0.341 [0.240, 0.442] | 5.261 [−0.991, 11.513] | 45.619 [34.790, 56.447] |
| Collins | −0.005 [−0.053, 0.042] | 0.302 [0.219, 0.384] | 3.837 [−1.228, 8.902] | 36.532 [27.760, 45.304] | |
| Tucker | −0.012 [−0.061, 0.037] | 0.304 [0.219, 0.388] | 4.413 [−0.845, 9.671] | 38.358 [29.25, 47.465] | |
| Median | −0.014 [−0.057, 0.029] | 0.263 [0.189, 0.337] | 4.326 [−0.275, 8.927] | 34.025 [26.057, 41.994] | |
| Women | Single | −0.067 [−0.121, −0.012] | 0.284 [0.190, 0.379] | 8.196 [2.415, 13.976] | 45.512 [35.499, 55.524] |
| Collins | −0.022 [−0.059, 0.016] | 0.221 [0.156, 0.286] | 4.728 [0.638, 8.819] | 31.133 [24.048, 38.217] | |
| Tucker | −0.025 [−0.062, 0.011] | 0.212 [0.149, 0.276] | 5.065 [1.093, 9.038] | 30.710 [23.829, 37.591] | |
| Median | −0.023 [−0.055, 0.008] | 0.181 [0.126, 0.236] | 4.870 [1.410, 8.329] | 27.204 [21.212, 33.197] | |
| Protocol | %BF (%) | FFM (kg) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| TEM 1 | SEM | MDC | ICC(2,1) 2 | TEM | SEM | MDC | ICC(2,1) | ||
| All | Single | 1.00 | 1.00 | 2.77 | 0.9914 | 0.675 | 0.673 | 1.867 | 0.9974 |
| Collins | 0.69 | 0.69 | 1.91 | 0.9960 | 0.507 | 0.506 | 1.403 | 0.9985 | |
| Tucker | 0.70 | 0.70 | 1.93 | 0.9959 | 0.515 | 0.513 | 1.422 | 0.9985 | |
| Median | 0.62 | 0.62 | 1.72 | 0.9967 | 0.457 | 0.456 | 1.264 | 0.9988 | |
| Men | Single | 0.88 | 0.88 | 2.44 | 0.9898 | 0.683 | 0.679 | 1.883 | 0.9934 |
| Collins | 0.66 | 0.66 | 1.82 | 0.9944 | 0.552 | 0.549 | 1.522 | 0.9957 | |
| Tucker | 0.69 | 0.69 | 1.91 | 0.9938 | 0.576 | 0.573 | 1.588 | 0.9953 | |
| Median | 0.60 | 0.60 | 1.67 | 0.9953 | 0.510 | 0.508 | 1.407 | 0.9963 | |
| Women | Single | 1.11 | 1.10 | 3.05 | 0.9866 | 0.668 | 0.664 | 1.840 | 0.9885 |
| Collins | 0.72 | 0.71 | 1.98 | 0.9944 | 0.457 | 0.455 | 1.261 | 0.9948 | |
| Tucker | 0.71 | 0.71 | 1.96 | 0.9945 | 0.444 | 0.442 | 1.225 | 0.9951 | |
| Median | 0.64 | 0.63 | 1.76 | 0.9956 | 0.397 | 0.395 | 1.095 | 0.9961 | |
| Protocol | BV (L) | RMR (kcal/day) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| TEM | SEM | MDC | ICC(2,1) | TEM | SEM | MDC | ICC(2,1) | ||
| All | Single | 0.135 | 0.135 | 0.374 | 0.9999 | 14.7 | 14.7 | 40.6 | 0.9982 |
| Collins | 0.098 | 0.098 | 0.271 | 1.0000 | 10.9 | 10.8 | 30.0 | 0.9990 | |
| Tucker | 0.101 | 0.101 | 0.280 | 1.0000 | 11.2 | 11.2 | 31.1 | 0.9989 | |
| Median | 0.088 | 0.088 | 0.243 | 1.0000 | 9.9 | 9.9 | 27.4 | 0.9992 | |
| Men | Single | 0.137 | 0.136 | 0.377 | 0.9999 | 14.9 | 14.8 | 41.0 | 0.9962 |
| Collins | 0.110 | 0.109 | 0.302 | 1.0000 | 12.0 | 11.9 | 33.0 | 0.9975 | |
| Tucker | 0.113 | 0.112 | 0.311 | 1.0000 | 12.5 | 12.4 | 34.5 | 0.9973 | |
| Median | 0.099 | 0.099 | 0.274 | 1.0000 | 11.0 | 11.0 | 30.4 | 0.9979 | |
| Women | Single | 0.134 | 0.133 | 0.369 | 0.9999 | 14.5 | 14.4 | 40.0 | 0.9926 |
| Collins | 0.088 | 0.088 | 0.243 | 1.0000 | 10.0 | 9.9 | 27.6 | 0.9966 | |
| Tucker | 0.087 | 0.086 | 0.239 | 1.0000 | 9.8 | 9.8 | 27.1 | 0.9967 | |
| Median | 0.075 | 0.074 | 0.206 | 1.0000 | 8.7 | 8.6 | 23.9 | 0.9974 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muntean, P.; Micloș-Balica, M.; Popa, A.; Neagu, A.; Neagu, M. Reliability of Repeated Trials Protocols for Body Composition Assessment by Air Displacement Plethysmography. Int. J. Environ. Res. Public Health 2021, 18, 10693. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010693
Muntean P, Micloș-Balica M, Popa A, Neagu A, Neagu M. Reliability of Repeated Trials Protocols for Body Composition Assessment by Air Displacement Plethysmography. International Journal of Environmental Research and Public Health. 2021; 18(20):10693. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010693
Chicago/Turabian StyleMuntean, Paul, Monica Micloș-Balica, Anca Popa, Adrian Neagu, and Monica Neagu. 2021. "Reliability of Repeated Trials Protocols for Body Composition Assessment by Air Displacement Plethysmography" International Journal of Environmental Research and Public Health 18, no. 20: 10693. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010693