
Exploring the Environment behind In-Patient Falls and Their Relation to Hospital Overcrowdedness—A Register-Based Observational Study



Abstract
:1. Introduction
2. Materials and Methods
3. Results
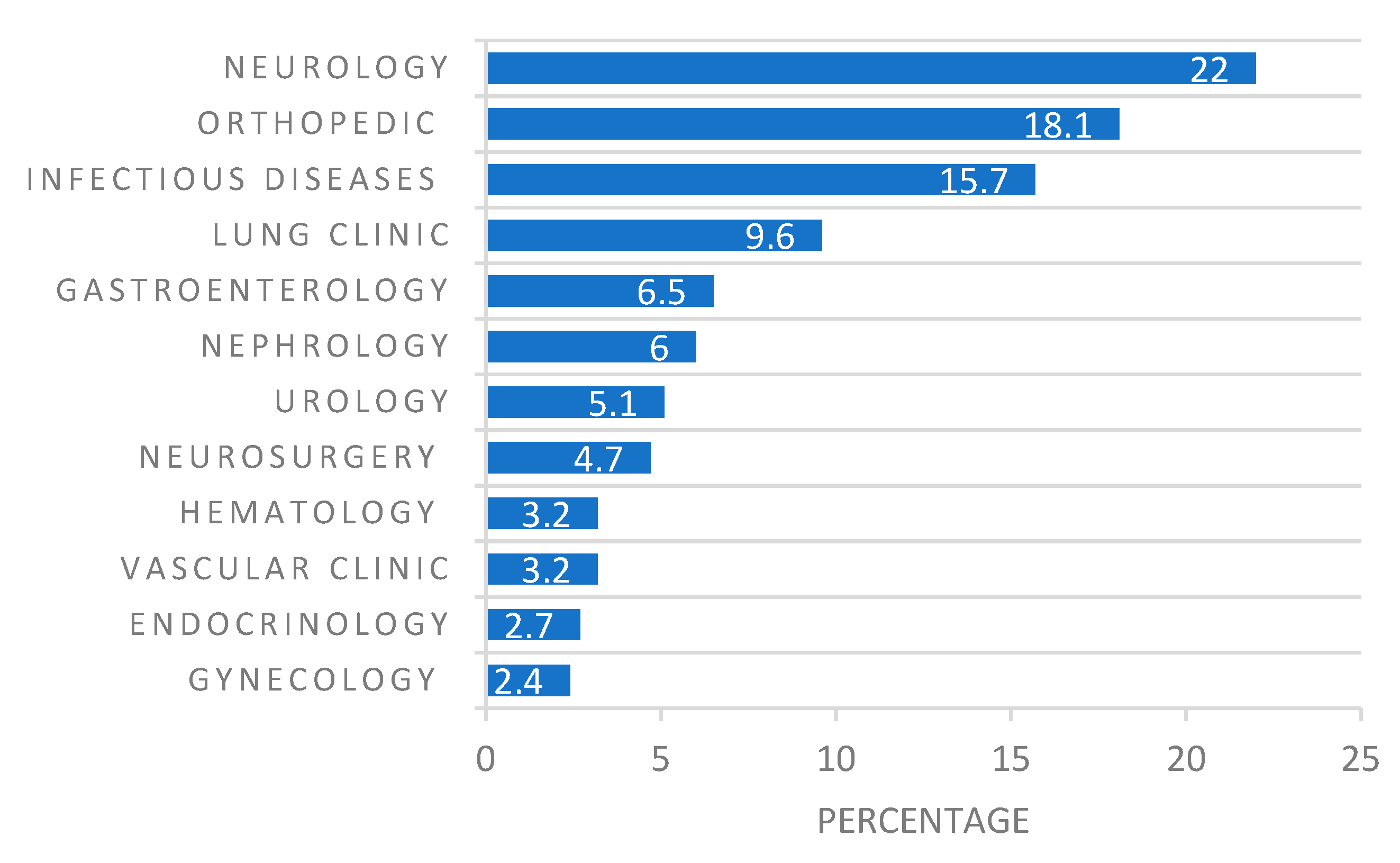
3.1. Inpatient Falls and Their Characteristics
3.2. Correlation between the Inpatient Overcrowdedness and the Total Amount of Inpatient Falls
3.3. Statistical Association of Total Number of Inpatient Falls with the Inpatient Overcrowdedness
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO|Falls; WHO: Geneva, Switzerland, 2014; Available online: https://www.who.int/violence_injury_prevention/other_injury/falls/en/ (accessed on 22 April 2019).
- Fall Injuries—Patient Safety. Fallskador—Patientsäkerhet. Available online: https://patientsakerhet.socialstyrelsen.se/risker-och-vardskador/vardskador/fallskador/ (accessed on 8 May 2020).
- Agneta, A. Fall and Fall Injuries—SKL. Sveriges Kommuner och Regioner. 2017. Available online: https://skl.se/halsasjukvard/patientsakerhet/riskomradenatgardspaket/riskomraden/fallochfallskador.618.html (accessed on 24 April 2019).
- National Board of Health and Welfare. Socialstyrelsen. Statistics on Fall Accidents in Your Region. Available online: https://www.socialstyrelsen.se/fallolyckor/statistikomfallolyckor (accessed on 25 April 2019).
- Abreu, C.; Mendes, A.; Monteiro, J.; Santos, F.R. Falls in hospital settings: A longitudinal study. Rev. Lat. Am. Enferm. 2012, 20, 597–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, D.; Hodgkinson, B.; Lambert, L.; Wood, J. Falls risk factors in the hospital setting: A systematic review. Int. J. Nurs. Pract. 2001, 7, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Hitcho, E.B.; Krauss, M.J.; Birge, S.; Claiborne Dunagan, W.; Fischer, I.; Johnson, S.; Nast, P.A.; Costantinou, E.; Fraser, V.J. Characteristics and circumstances of falls in a hospital setting: A prospective analysis. J. Gen. Intern. Med. 2004, 19, 732–739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Severo, I.M.; Almeida, M.d.A.; Kuchenbecker, R.; Vieira, D.F.V.B.; Weschenfelder, M.E.; Pinto, L.R.C.; Klein, C.; Siqueira, A.P.d.O.; Panato, B.P. Risk factors for falls in hospitalized adult patients: An integrative review. Rev. Esc. Enferm. USP 2014, 48, 540–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Udén, G.; Ehnfors, M.; Sjöström, K. Use of initial risk assessment and recording as the main nursing intervention in identifying risk of falls. J. Adv. Nurs. 1999, 29, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Healey, F.; Scobie, S.; Oliver, D.; Pryce, A.; Thomson, R.; Glampson, B. Falls in English and Welsh hospitals: A national observational study based on retrospective analysis of 12 months of patient safety incident reports. Qual. Saf. Health Care 2008, 17, 424–430. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, T. The National Patient Safety Agency. Arch. Dis. Child. 2005, 90, 226–228. [Google Scholar] [CrossRef] [Green Version]
- Bates, D.W.; Pruess, K.; Souney, P.; Platt, R. Serious falls in hospitalized patients: Correlates and resource utilization. Am. J. Med. 1995, 99, 137–143. [Google Scholar] [CrossRef]
- Liddle, J.; Gilleard, C. The emotional consequences of falls for older people and their families. Clin. Rehabil. 1995, 9, 110–114. [Google Scholar] [CrossRef]
- Oliver, D. Bed falls and bedrails—What should we do? Age Ageing 2002, 31, 415–418. [Google Scholar] [CrossRef] [Green Version]
- de Freitas Luzia, M.; de Goes Victor, M.A.; de Fátima Lucena, A. Diagnóstico de enfermagem Risco de quedas: Prevalência e perfil clínico de pacientes hospitalizados. Rev. Lat. Am. Enferm. 2014, 22, 262–268. [Google Scholar]
- Tsur, A.; Shakeer, N.; Segal, Z.; Itah, D.; Eluz, D. Extrinsic and intrinsic factors for falls that caused hip fracture. Harefuah 2017, 156, 294–297. [Google Scholar] [PubMed]
- Harlein, J.; Dassen, T.; Halfens, R.J.G.; Heinze, C. Fall risk factors in older people with dementia or cognitive impairment: A systematic review. J. Adv. Nurs. 2009, 65, 922–933. [Google Scholar] [CrossRef] [PubMed]
- Bird, M.-L.; Cheney, M.J.; Williams, A.D. Accidental Fall Rates in Community-Dwelling Adults Compared to Cancer Survivors During and Post-Treatment: A Systematic Review With Meta-Analysis. Oncol. Nurs. Forum. 2016, 43, E64–E72. [Google Scholar] [CrossRef]
- Pfortmueller, C.A.; Lindner, G.; Exadaktylos, A.K. Reducing fall risk in the elderly: Risk factors and fall prevention, a systematic review. Minerva Med. 2014, 105, 275–281. [Google Scholar]
- Hempel, S.; Newberry, S.; Wang, Z.; Booth, M.; Shanman, R.; Johnsen, B.; Shier, V.; Saliba, D.; Spector, W.D.; Ganz, D.A. Hospital fall prevention: A systematic review of implementation, components, adherence, and effectiveness. J. Am. Geriatr. Soc. 2013, 61, 483–494. [Google Scholar] [CrossRef]
- Carpenter, C.R.; Avidan, M.S.; Wildes, T.; Stark, S.; Fowler, S.A.; Lo, A.X. Predicting geriatric falls following an episode of emergency department care: A systematic review. Acad. Emerg. Med. 2014, 21, 1069–1082. [Google Scholar] [CrossRef] [Green Version]
- Oliver, D.; Connelly, J.B.; Victor, C.R.; Shaw, F.E.; Whitehead, A.; Genc, Y.; Vanoli, A.; Martin, F.C.; Gosney, M.A. Strategies to prevent falls and fractures in hospitals and care homes and effect of cognitive impairment: Systematic review and meta-analyses. BMJ 2007, 334, 82. [Google Scholar] [CrossRef] [Green Version]
- Vieira, E.R.; Freund-Heritage, R.; da Costa, B.R. Risk factors for geriatric patient falls in rehabilitation hospital settings: A systematic review. Clin. Rehabil. 2011, 25, 788–799. [Google Scholar] [CrossRef] [PubMed]
- Oliver, D.; Hopper, A.; Seed, P. Do hospital fall prevention programs work? A systematic review. J. Am. Geriatr. Soc. 2000, 48, 1679–1689. [Google Scholar] [CrossRef]
- Deandrea, S.; Bravi, F.; Turati, F.; Lucenteforte, E.; La Vecchia, C.; Negri, E. Risk factors for falls in older people in nursing homes and hospitals. A systematic review and meta-analysis. Arch. Gerontol. Geriatr. 2013, 56, 407–415. [Google Scholar] [CrossRef]
- de Vries, M.; Seppala, L.J.; Daams, J.G.; van de Glind, E.M.M.; Masud, T.; van der Velde, N. Fall-Risk-Increasing Drugs: A Systematic Review and Meta-Analysis: I. Cardiovascular Drugs. J. Am. Med. Dir. Assoc. 2018, 19, 371.e1–371.e9. [Google Scholar] [CrossRef] [Green Version]
- Sousa, L.M.M.; Marques-Vieira, C.M.A.; Caldevilla, M.N.G.N.; de Henriques, C.M.A.D.; Severino, S.S.P.; Caldeira, S.M.A. Risk for falls among community-dwelling older people: Systematic literature review. Rev. Gauch. Enferm. 2017, 37, e55030. [Google Scholar]
- Lusardi, M.M.; Fritz, S.; Middleton, A.; Allison, L.; Wingood, M.; Phillips, E.; Criss, M.; Verma, S.; Osborne, J.; Chui, K.K. Determining Risk of Falls in Community Dwelling Older Adults: A Systematic Review and Meta-analysis Using Posttest Probability. J. Geriatr Phys. Ther. 2017, 40, 1–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliver, D.; Daly, F.; Martin, F.C.; McMurdo, M.E.T. Risk factors and risk assessment tools for falls in hospital in-patients: A systematic review. Age Ageing 2004, 33, 122–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collis, J. Adverse effects of overcrowding on patient experience and care. Emerg. Nurse 2010, 18, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Sveriges Kommuner och Landsting. Väntetider i Vården—En Webbplats Från Sveriges Kommuner och Landsting. 2018. Available online: https://www.vantetider.se/Kontaktkort/Skanes/Overbelaggning/ (accessed on 1 April 2020).
- European Commission. Statistics|Eurostat. Eurostat. 2019. Available online: https://ec.europa.eu/eurostat/databrowser/view/tps00046/default/table?lang=en (accessed on 16 April 2020).
- Mizzi, M. Overcrowding Rises as Winter Looms. Available online: https://healthcare-in-europe.com/en/news/overcrowding-rises-as-winter-looms.html (accessed on 27 April 2020).
- Pedroja, A.T. The tipping point: The relationship between volume and patient harm. Am. J. Med. Qual. 2008, 23, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Hillier, D.F.; Parry, G.J.; Shannon, M.W.; Stack, A.M. The Effect of Hospital Bed Occupancy on Throughput in the Pediatric Emergency Department. Ann. Emerg. Med. 2009, 53, 767–776.e3. [Google Scholar] [CrossRef]
- Lorch, S.A.; Millman, A.M.; Zhang, X.; Even-Shoshan, O.; Silber, J.H. Impact of admission-day crowding on the length of stay of pediatric Hospitalizations. Pediatrics 2008, 121, e718–e730. [Google Scholar] [CrossRef]
- Schilling, P.L.; Campbell, D.A.; Englesbe, M.J.; Davis, M.M. A comparison of in-hospital mortality risk conferred by high hospital occupancy, differences in nurse staffing levels, weekend admission, and seasonal influenza. Med. Care 2010, 48, 224–232. [Google Scholar] [CrossRef]
- Chen, L.C.; Lin, C.C.; Han, C.Y.; Hsieh, C.L.; Wu, C.J.J.; Liang, H.F. An Interpretative Study on Nurses’ Perspectives of Working in an Overcrowded Emergency Department in Taiwan. Asian Nurs. Res. (Korean Soc. Nurs. Sci.) 2018, 12, 62–68. [Google Scholar] [CrossRef] [Green Version]
- Eriksson, J.; Gellerstedt, L.; Hillerås, P.; Craftman, Å.G.G. Registered nurses’ perceptions of safe care in overcrowded emergency departments. J. Clin. Nurs. 2018, 27, e1061–e1067. [Google Scholar] [CrossRef]
- Vasli, P.; Dehghan-Nayeri, N. Emergency nurses’ experience of crisis: A qualitative study. Jpn. J. Nurs. Sci. 2016, 13, 55–64. [Google Scholar] [CrossRef]
- Teitelbaum, A.; Lahad, A.; Calfon, N.; Gun-Usishkin, M.; Lubin, G.; Tsur, A. Overcrowding in psychiatric wards is associated with increased risk of adverse incidents. Med. Care 2016, 54, 296–302. [Google Scholar] [CrossRef]
- IBM. IBM SPSS Statistics 26. Available online: https://www.ibm.com/support/pages/downloading-ibm-spss-statistics-26 (accessed on 7 April 2020).
- Mukaka, M.M. Statistics corner: A guide to appropriate use of correlation coefficient in medical research. Malawi Med. J. 2012, 24, 69–71. [Google Scholar]
- Chan, Y.H. Biostatistics104: Correlational Analysis. Singap. Med. J. 2003, 44, 614–649. [Google Scholar]
- Schneider, A.; Hommel, G.; Blettner, M. Linear regression analysis: Part 14 of a series on evaluation of scientific publications. Dtsch. Arztebl. Int. 2010, 107, 776–782. [Google Scholar] [PubMed]
- McDonald, J.H. Handbook of Biological Statistics; Sparky House Publishing: Baltimore, MD, USA, 2009. [Google Scholar]
- Halfon, P.; Eggli, Y.; Van Melle, G.; Vagnair, A. Risk of falls for hospitalized patients: A predictive model based on routinely available data. J. Clin. Epidemiol. 2001, 54, 1258–1266. [Google Scholar] [CrossRef]
- Morello, R. School of Public Health and Preventive Medicine In-Hospital Fall Injuries: Where, When and How Do They Occur? When and How Do They Occur? Available online: http://www.med.monash.edu.au/assets/docs/creps/2012/2012preventingfalls-renatamorello.pdf (accessed on 22 April 2020).
- Gurlek Kisacik, O.; Professor, A.; Cigerci, Y. Characteristics of Ιnpatient Falls in a Hospital Setting: A Retrospective Study from Turkey. Int. J. Caring Sci. 2019, 12, 2. [Google Scholar]
- Currie, L. Advances in Patient Safety Fall and Injury Prevention. In Patient Safety and Quality: An Evidence-Based Handbook for Nurses; Hughes, R.G., Ed.; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2008. [Google Scholar]
- Virtanen, M.; Pentti, J.; Vahtera, J.; Ferrie, J.E.; Stansfeld, S.A.; Helenius, H.; Elovainio, M.; Honkonen, T.; Terho, K.; Oksanen, T.; et al. Overcrowding in hospital wards as a predictor of antidepressant treatment among hospital staff. Am. J. Psychiatry 2008, 165, 1482–1486. [Google Scholar] [CrossRef] [PubMed]
- Santibáñez, P.; Chow, V.S.; French, J.; Puterman, M.L.; Tyldesley, S. Reducing patient wait times and improving resource utilization at British Columbia Cancer Agency’s ambulatory care unit through simulation. Health Care Manag. Sci. 2009, 12, 392–407. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Clinic | Falls | Severe | Location | Time of Day | Staff | ||||
|---|---|---|---|---|---|---|---|---|---|
| Falls | Toilet | Dayroom | Room | Corridor | Day | Night | Present | ||
| n | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |
| Gynecology | 21 | 1 (4.8) | 11 (52.4) | 1 (4.8) | 7 (33.3) | 2 (9.5) | 12 (57.1) | 9 (42.9) | 3 (14.3) |
| Endocrinology | 24 | 2 (8.3) | 6 (25) | 0 (0) | 18 (75) | 0 (0) | 9 (37.5) | 15 (62.5) | 1 (4.2) |
| Vascular | 28 | 6 (21.4) | 2 (7.1) | 2 (7.1) | 22 (78.6) | 2 (7.1) | 13 (46.4) | 15 (53.6) | 3 (10.7) |
| Hematology | 33 | 3 (9.1) | 8 (24.2) | 1 (3) | 23 (69.8) | 1 (3) | 13 (39.4) | 20 (60.6) | 5 (15.2) |
| Neurosurgery | 41 | 1 (2.4) | 7 (17.1) | 1 (2.4) | 28 (68.3) | 5 (12.2) | 24 (58.5) | 17 (41.5) | 4 (9.8) |
| Urology | 45 | 1 (2.2) | 8 (17.8) | 3 (6.7) | 30 (66.7) | 4 (8.9) | 28 (62.2) | 17 (37.8) | 4 (8.9) |
| Nephrology | 52 | 3 (5.8) | 9 (17.3) | 6 (11.5) | 34 (65.,4) | 3 (5.8) | 24 (46.2) | 28 (53.8) | 5 (9.6) |
| Gastroenterology | 57 | 1 (1.8) | 20 (35.1) | 0 (0) | 35 (61.4) | 2 (3.5) | 30 (52.6) | 27 (47.4) | 11 (19.3) |
| Lung | 84 | 3 (3.6) | 20 (23.8) | 3 (3.6) | 58 (69) | 3 (3.6) | 31 (36.9) | 53 (63.1) | 7 (8.3) |
| Infectious diseases | 137 | 3 (2.2) | 34 (24.8) | 1 (0.7) | 96 (70.1) | 6 (4.4) | 64 (46.7) | 73 (53.3) | 13 (9.5) |
| Orthopedic | 158 | 5 (3.2) | 28 (17.7) | 8 (5.1) | 116 (73.4) | 6 (3.8) | 68 (43) | 90 (57) | 11 (7) |
| Neurology | 190 | 6 (3.2) | 32 (16.8) | 12 (6.3) | 123 (64.7) | 23 (12.1) | 90 (47.4) | 100 (52.6) | 26 (13.7) |
| TOTAL | 870 | 35 (4.2) | 185 (21.3) | 38 (4.4) | 590 (67.8) | 57 (6.5) | 406 (46.7) | 464 (53.3) | 93 (10.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stathopoulos, D.; Ekvall Hansson, E.; Stigmar, K. Exploring the Environment behind In-Patient Falls and Their Relation to Hospital Overcrowdedness—A Register-Based Observational Study. Int. J. Environ. Res. Public Health 2021, 18, 10742. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010742
Stathopoulos D, Ekvall Hansson E, Stigmar K. Exploring the Environment behind In-Patient Falls and Their Relation to Hospital Overcrowdedness—A Register-Based Observational Study. International Journal of Environmental Research and Public Health. 2021; 18(20):10742. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010742
Chicago/Turabian StyleStathopoulos, Dimitrios, Eva Ekvall Hansson, and Kjerstin Stigmar. 2021. "Exploring the Environment behind In-Patient Falls and Their Relation to Hospital Overcrowdedness—A Register-Based Observational Study" International Journal of Environmental Research and Public Health 18, no. 20: 10742. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182010742