
Status of Constipation and Its Association with Sarcopenia in Older Adults: A Population-Based Cohort Study

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Assessments of Constipation
2.2.1. No Constipation
2.2.2. Self-Reported Constipation Only
2.2.3. Clinically Diagnosed Constipation
2.3. Measurement of Sarcopenia
2.3.1. Muscle Mass
2.3.2. Grip Strength
2.3.3. Gait Speed
2.3.4. Definition of Sarcopenia
2.4. Other Geriatric Parameters
2.5. Statistical Analysis
3. Results
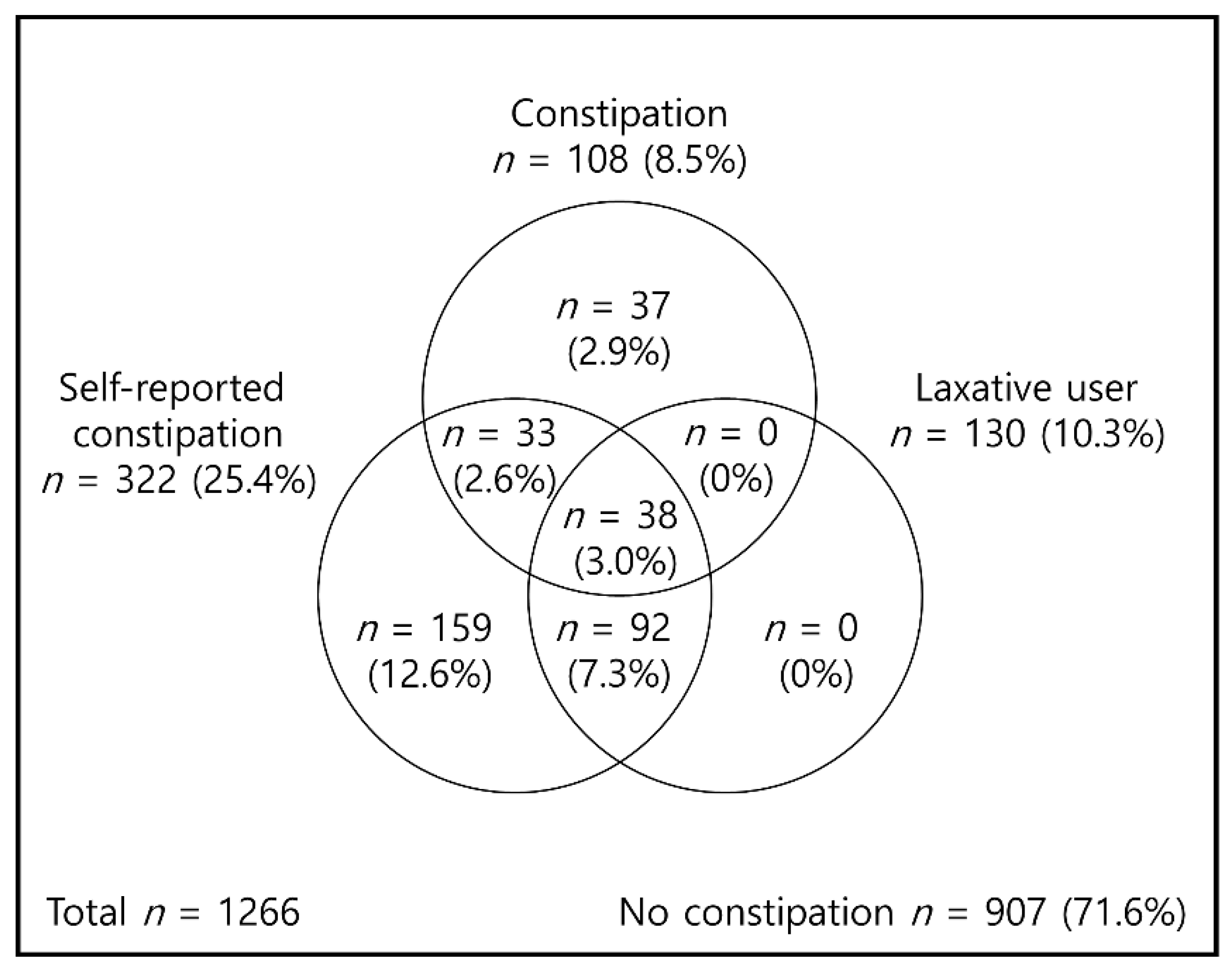
3.1. Prevalence of Constipation and Associated Characteristics
3.2. Association of Sarcopenia with Constipation Status
3.3. Association of Sarcopenia Parameters with Constipation Status
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bouras, E.P.; Tangalos, E.G. Chronic constipation in the elderly. Gastroenterol. Clin. N. Am. 2009, 38, 463–480. [Google Scholar] [CrossRef] [PubMed]
- Suares, N.C.; Ford, A.C. Prevalence of, and risk factors for, chronic idiopathic constipation in the community: Systematic review and meta-analysis. Am. J. Gastroenterol. 2011, 106, 1582–1591. [Google Scholar] [CrossRef]
- Wald, A.; Scarpignato, C.; Mueller-Lissner, S.; Kamm, M.A.; Hinkel, U.; Helfrich, I.; Schuijt, C.; Mandel, K.G. A multinational survey of prevalence and patterns of laxative use among adults with self-defined constipation. Aliment. Pharmacol. Ther. 2008, 28, 917–930. [Google Scholar] [CrossRef] [PubMed]
- Wald, A.; Mueller-Lissner, S.; Kamm, M.A.; Hinkel, U.; Richter, E.; Schuijt, C.; Mandel, K.G. Survey of laxative use by adults with self-defined constipation in South America and Asia: A comparison of six countries. Aliment. Pharmacol. Ther. 2010, 31, 274–284. [Google Scholar] [CrossRef]
- Jun, D.W.; Park, H.Y.; Lee, O.Y.; Lee, H.L.; Yoon, B.C.; Choi, H.S.; Hahm, J.S.; Lee, M.H.; Lee, D.H.; Kee, C.S. A population-based study on bowel habits in a Korean community: Prevalence of functional constipation and self-reported constipation. Dig. Dis. Sci. 2006, 51, 1471–1477. [Google Scholar] [CrossRef] [PubMed]
- Glia, A.; Lindberg, G. Quality of life in patients with different types of functional constipation. Scand. J. Gastroenterol. 1997, 32, 1083–1089. [Google Scholar] [CrossRef]
- Koloski, N.A.; Jones, M.; Wai, R.; Gill, R.S.; Byles, J.; Talley, N.J. Impact of persistent constipation on health-related quality of life and mortality in older community-dwelling women. Am. J. Gastroenterol. 2013, 108, 1152–1158. [Google Scholar] [CrossRef]
- Sommers, T.; Corban, C.; Sengupta, N.; Jones, M.; Cheng, V.; Bollom, A.; Nurko, S.; Kelley, J.; Lembo, A. Emergency department burden of constipation in the United States from 2006 to 2011. Am. J. Gastroenterol. 2015, 110, 572–579. [Google Scholar] [CrossRef] [PubMed]
- Yu, Q.J.; Yu, S.Y.; Zuo, L.J.; Lian, T.H.; Hu, Y.; Wang, R.D.; Piao, Y.S.; Guo, P.; Liu, L.; Jin, Z.; et al. Parkinson disease with constipation: Clinical features and relevant factors. Sci. Rep. 2018, 8, 567. [Google Scholar] [CrossRef] [Green Version]
- Song, E.M.; Lee, H.J.; Jung, K.W.; Kim, M.J.; Hwang, S.W.; Park, S.H.; Yang, D.H.; Ye, B.D.; Byeon, J.S.; Choe, J.; et al. Long-Term Risks of Parkinson’s Disease, Surgery, and Colorectal Cancer in Patients With Slow-Transit Constipation. Clin. Gastroenterol. Hepatol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Sumida, K.; Yamagata, K.; Kovesdy, C.P. Constipation in CKD. Kidney Int. Rep. 2019, 5, 121–134. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e302. [Google Scholar] [CrossRef]
- Jang, I.Y.; Lee, E.; Lee, H.; Park, H.; Kim, S.; Kim, K.I.; Jung, H.W.; Kim, D.H. Characteristics of sarcopenia by European consensuses and a phenotype score. J. Cachexia Sarcopenia Muscle 2020, 11, 497–504. [Google Scholar] [CrossRef] [Green Version]
- Jung, H.W.; Kim, S.; Jang, I.Y.; Shin, D.W.; Lee, J.E.; Won, C.W. Screening Value of Timed Up and Go Test for Frailty and Low Physical Performance in Korean Older Population: The Korean Frailty and Aging Cohort Study (KFACS). Ann. Geriatr. Med. Res. 2020, 24, 259–266. [Google Scholar] [CrossRef]
- Jung, H.W.; Kim, S.W.; Kim, I.Y.; Lim, J.Y.; Park, H.S.; Song, W.; Yoo, H.J.; Jang, H.C.; Kim, K.; Park, Y.; et al. Protein Intake Recommendation for Korean Older Adults to Prevent Sarcopenia: Expert Consensus by the Korean Geriatric Society and the Korean Nutrition Society. Ann. Geriatr. Med. Res. 2018, 22, 167–175. [Google Scholar] [CrossRef] [Green Version]
- Jung, H.W.; Jang, I.Y.; Lee, Y.S.; Lee, C.K.; Cho, E.I.; Kang, W.Y.; Chae, J.H.; Lee, E.J.; Kim, D.H. Prevalence of Frailty and Aging-Related Health Conditions in Older Koreans in Rural Communities: A Cross-Sectional Analysis of the Aging Study of Pyeongchang Rural Area. J. Korean Med. Sci. 2016, 31, 345–352. [Google Scholar] [CrossRef]
- Jang, I.Y.; Jung, H.W.; Lee, C.K.; Lee, Y.S.; Kim, K.I.; Kim, K.W.; Oh, H.; Ji, M.Y.; Lee, E.; Kim, D.H. Rural and Urban Disparities in Frailty and Aging-Related Health Conditions in Korea. J. Am. Geriatr. Soc. 2016, 64, 908–911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, M.; Shinkai, S.; Murayama, H.; Mori, S. Comparison of segmental multifrequency bioelectrical impedance analysis with dual-energy X-ray absorptiometry for the assessment of body composition in a community-dwelling older population. Geriatr. Gerontol. Int. 2015, 15, 1013–1022. [Google Scholar] [CrossRef] [PubMed]
- Hachiya, M.; Murata, S.; Otao, H.; Kamijou, K.; Mizota, K.; Asami, T. Reproducibility and validity of the 50-meter walking test in community-dwelling elderly. J. Phys. Ther. Sci. 2015, 27, 1511–1514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mathiowetz, V.; Rennells, C.; Donahoe, L. Effect of elbow position on grip and key pinch strength. J. Hand. Surg. Am. 1985, 10, 694–697. [Google Scholar] [CrossRef]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef]
- Peters, D.M.; Fritz, S.L.; Krotish, D.E. Assessing the reliability and validity of a shorter walk test compared with the 10-Meter Walk Test for measurements of gait speed in healthy, older adults. J. Geriatr. Phys. Ther. 2013, 36, 24–30. [Google Scholar] [CrossRef]
- Jang, I.Y.; Jung, H.W.; Lee, C.K.; Yu, S.S.; Lee, Y.S.; Lee, E. Comparisons of predictive values of sarcopenia with different muscle mass indices in Korean rural older adults: A longitudinal analysis of the Aging Study of PyeongChang Rural Area. Clin. Interv. Aging 2018, 13, 91–99. [Google Scholar] [CrossRef] [Green Version]
- Won, C.W.; Yang, K.Y.; Rho, Y.G.; Kim, S.Y.; Lee, E.J.; Yoon, J.L.; Cho, K.H.; Shin, H.C.; Cho, B.R.; Oh, J.R.; et al. The Development of Korean Activities of Daily Living(K-ADL) and Korean Instrumental Activities of Daily Living(K-IADL) Scale. J. Korean Geriatr. Soc. 2002, 6, 107–120. [Google Scholar]
- Kang, Y.W.; Na, D.L.; Hahn, S.H. A validity study on the korean mini-mental state examination (K-MMSE) in dementia patients. J. Korean Neurol. Assoc. 1997, 15, 300–308. [Google Scholar]
- Radloff, L.S. The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Rubenstein, L.Z.; Harker, J.O.; Salvà, A.; Guigoz, Y.; Vellas, B. Screening for undernutrition in geriatric practice: Developing the short-form mini-nutritional assessment (MNA-SF). J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M366–M372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, J.E.; Jung, H.K.; Lee, T.H.; Jo, Y.; Lee, H.; Song, K.H.; Hong, S.N.; Lim, H.C.; Lee, S.J.; Chung, S.S.; et al. Guidelines for the Diagnosis and Treatment of Chronic Functional Constipation in Korea, 2015 Revised Edition. J. Neurogastroenterol. Motil. 2016, 22, 383–411. [Google Scholar] [CrossRef] [PubMed]
- Gallegos-Orozco, J.F.; Foxx-Orenstein, A.E.; Sterler, S.M.; Stoa, J.M. Chronic constipation in the elderly. Am. J. Gastroenterol. 2012, 107, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Wiskur, B.; Greenwood-Van Meerveld, B. The Aging Colon: The Role of Enteric Neurodegeneration in Constipation. Curr. Gastroenterol. Rep. 2010, 12, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Delmonico, M.J.; Harris, T.B.; Visser, M.; Park, S.W.; Conroy, M.B.; Velasquez-Mieyer, P.; Boudreau, R.; Manini, T.M.; Nevitt, M.; Newman, A.B.; et al. Longitudinal study of muscle strength, quality, and adipose tissue infiltration. Am. J. Clin. Nutr. 2009, 90, 1579–1585. [Google Scholar] [PubMed]
- Beaudart, C.; Biver, E.; Reginster, J.-Y.; Rizzoli, R.; Rolland, Y.; Bautmans, I.; Petermans, J.; Gillain, S.; Buckinx, F.; Dardenne, N.; et al. Validation of the SarQoL®, a specific health-related quality of life questionnaire for Sarcopenia. J. Cachexia Sarcopenia Muscle 2017, 8, 238–244. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Filtering out of Irritable Bowel Syndrome |
| Must fulfill the following criteria for the past 3 months: |
| 1. Recurrent abdominal pain occurring on average at least 1 day per week |
| 2. Pain is associated with two or more of the following criteria: a. Related to defecation b. Associated with a change in frequency of stool c. Associated with a change in form (appearance) of stool |
| 3. Symptom onset at least 6 months prior to diagnosis |
| Diagnosis of Functional Constipation |
| 1. Presence of ≥2 of the following features within the last 3 months: a. Straining during >25% of defecations b. Lumpy or hard stools in >25% of defecations c. Sensation of incomplete evacuation in >25% of defecations d. Sensation of anorectal obstruction or blockage in >25% of defecations e. Need for manual maneuvers to facilitate >25% of defecations f. <3 spontaneous bowel movements per week. |
| 2. Loose stools are rarely present without the use of laxatives |
| 3. Insufficient criteria for irritable bowel syndrome |
| 4. Symptom onset at least 6 months prior to diagnosis |
| Assessment of Sarcopenia Parameters |
| 1. Muscle strength Decreased handgrip strength < 26 kg for men and < 18 kg for women |
| 2. Physical performance Slow gait speed <1 m/s |
| 3. Appendicular skeletal mass (ASM) Decreased muscle mass: sex-specific lowest quintile of ASM/ht2 |
| Diagnosis of Sarcopenia |
| 1. Sarcopenia: Low ASM + low muscle strength OR Low physical performance |
| 2. Severe Sarcopenia: Low ASM + low muscle strength AND Low physical performance |
| No Constipation | Self-Reported Constipation Only | Clinically Defined Constipation | p-Value | |
|---|---|---|---|---|
| (N = 907) | (N = 251) | (N = 108) | ||
| Age | 74.7 ± 6.1 | 76.5 ± 6.2 (1) | 77.4 ± 6.5 (2) | <0.001 |
| Female | 493 (54.4%) | 186 (74.1%) (1) | 69 (63.9%) | <0.001 |
| Living alone | 219 (24.1%) | 84 (33.5%) (1) | 27 (25.0%) | 0.011 |
| No formal education | 359 (39.6%) | 142 (56.6%) (1) | 65 (60.2%) (2) | <0.001 |
| Multimorbidity | 412 (45.4%) | 157 (62.5%) (1) | 69 (63.9%) (2) | <0.001 |
| Polypharmacy | 183 (20.2%) | 67 (26.7%) | 32 (29.6%) (2) | 0.014 |
| BMI (Kg/m2) | 25.2 ± 3.5 | 25.1 ± 3.5 | 25.0 ± 3.7 | 0.648 |
| Cognitive impairment | 205 (22.7%) | 88 (35.1%) (1) | 37 (34.3%) (2) | <0.001 |
| Depressed mood | 44 (4.9%) | 33 (13.1%) (1) | 9 (8.3%) | <0.001 |
| Sarcopenia | 415 (45.8%) | 158 (62.9%) (1) | 68 (63.0%) (2) | <0.001 |
| Muscle mass (ASM/ht2) | 6.6 ± 1.0 | 6.4 ± 2.3 | 6.3 ± 1.0 (2) | 0.003 |
| Decreased muscle mass | 285 (31.4%) | 97 (38.6%) | 43 (39.8%) | 0.036 |
| Grip strength (kg) | 23.1 ± 9.0 | 19.4 ± 7.3 (1) | 20.4 ± 9.2 (2) | <0.001 |
| Decreased grip strength | 407 (44.9%) | 143 (57.0%) (1) | 61 (56.5%) (2) | 0.001 |
| Gait speed (m/s) | 1.0 ± 0.3 | 0.9 ± 0.3 (1) | 0.8 ± 0.5 (2) | <0.001 |
| Slow gait speed | 497 (54.8%) | 170 (67.7%) (1) | 83 (76.9%) (2) | <0.001 |
| Malnutrition | 16 (1.8%) | 10 (4.0%) (1) | 7 (6.5%) (2) | <0.001 |
| ADL disability | 219 (24.1%) | 97 (38.6%) (1) | 35 (32.4%) | <0.001 |
| IADL disability | 163 (18.0%) | 62 (24.7%) (1) | 32 (29.6%) (2) | 0.003 |
| Fall history | 96 (10.6%) | 34 (13.5%) | 14 (13.0%) | 0.367 |
| EQ-5D index | 0.86 ± 0.10 | 0.82 ± 0.12 (1) | 0.79 ± 0.11 (2) | <0.001 |
| Model 1 | Model 2 | Model 3 | ||||
|---|---|---|---|---|---|---|
| Variable | OR | 95% CI | OR | 95% CI | OR | 95% CI |
| Self-reported constipation | ||||||
| No sarcopenia | (ref) | |||||
| Sarcopenia | 2.01 | 1.51–2.69 | 1.44 | 1.03–2.01 | 1.29 | 0.90–1.83 |
| p value | <0.001 | 0.034 | 0.161 | |||
| Clinically defined constipation | ||||||
| No sarcopenia | (ref) | |||||
| Sarcopenia | 2.02 | 1.34–3.04 | 1.36 | 0.75–2.20 | 1.17 | 0.71–1.93 |
| p value | <0.001 | 0.201 | 0.526 | |||
| General constipation | ||||||
| No sarcopenia | (ref) | |||||
| Sarcopenia | 2.01 | 1.56–2.59 | 1.4 | 1.05–1.88 | 1.24 | 0.91–1.68 |
| p value | <0.001 | 0.024 | 0.169 | |||
| Model 1 | Model 2 | Model 3 | ||||
|---|---|---|---|---|---|---|
| Variable | OR | 95% CI | OR | 95% CI | OR | 95% CI |
| Self-reported constipation | ||||||
| Normal muscle mass | (ref) | |||||
| Decreased muscle mass | 1.13 | 0.83–1.53 | 1.08 | 0.79–1.49 | 1.07 | 0.77–1.48 |
| p value | 0.44 | 0.619 | 0.674 | |||
| Normal grip strength | (ref) | |||||
| Decreased grip strength | 1.37 | 1.01–1.85 | 1.05 | 0.76–1.46 | 1.00 | 0.71–1.39 |
| p value | 0.04 | 0.752 | 0.978 | |||
| Normal gait speed | (ref) | |||||
| Slow gait speed | 1.43 | 1.06–1.94 | 1.25 | 0.71–1.72 | 1.19 | 0.86–1.64 |
| p value | 0.02 | 0.16 | 0.299 | |||
| Clinically defined constipation | ||||||
| Normal muscle mass | (ref) | |||||
| Decreased muscle mass | 1.16 | 0.89–1.53 | 1.07 | 0.80–1.42 | 1.06 | 0.79–1.42 |
| p value | 0.269 | 0.657 | 0.686 | |||
| Normal grip strength | (ref) | |||||
| decreased grip strength | 1.35 | 1.03–1.76 | 1.02 | 0.76–1.36 | 0.95 | 0.71–1.28 |
| p value | 0.029 | 0.901 | 0.747 | |||
| Normal gait speed | (ref) | |||||
| Slow gait speed | 1.79 | 1.37–2.35 | 1.54 | 1.16–2.04 | 1.46 | 1.10–1.94 |
| p value | <0.001 | 0.003 | 0.009 | |||
| General constipation | ||||||
| Normal muscle mass | (ref) | |||||
| Decreased muscle mass | 1.17 | 0.89–1.53 | 1.07 | 0.80–1.42 | 1.06 | 0.79–1.42 |
| p value | 0.269 | 0.657 | 0.686 | |||
| Normal grip strength | (ref) | |||||
| Decreased grip strength | 1.35 | 1.03–1.76 | 1.02 | 0.76–1.36 | 0.95 | 0.71–1.28 |
| p value | 0.029 | 0.901 | 0.747 | |||
| Normal gait speed | (ref) | |||||
| Slow gait speed | 1.79 | 1.37–2.35 | 1.54 | 1.16–2.04 | 1.46 | 1.10–1.94 |
| p value | ☐ | <0.001 | ☐ | 0.003 | ☐ | 0.009 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, H.; Lim, J.; Baek, J.Y.; Lee, E.; Jung, H.-W.; Jang, I.-Y. Status of Constipation and Its Association with Sarcopenia in Older Adults: A Population-Based Cohort Study. Int. J. Environ. Res. Public Health 2021, 18, 11083. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111083
Park H, Lim J, Baek JY, Lee E, Jung H-W, Jang I-Y. Status of Constipation and Its Association with Sarcopenia in Older Adults: A Population-Based Cohort Study. International Journal of Environmental Research and Public Health. 2021; 18(21):11083. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111083
Chicago/Turabian StylePark, Hyungchul, Jihye Lim, Ji Yeon Baek, Eunju Lee, Hee-Won Jung, and Il-Young Jang. 2021. "Status of Constipation and Its Association with Sarcopenia in Older Adults: A Population-Based Cohort Study" International Journal of Environmental Research and Public Health 18, no. 21: 11083. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111083