
Effect of Heart Rate Reserve on Prefrontal Cortical Activation While Dual-Task Walking in Older Adults


Abstract
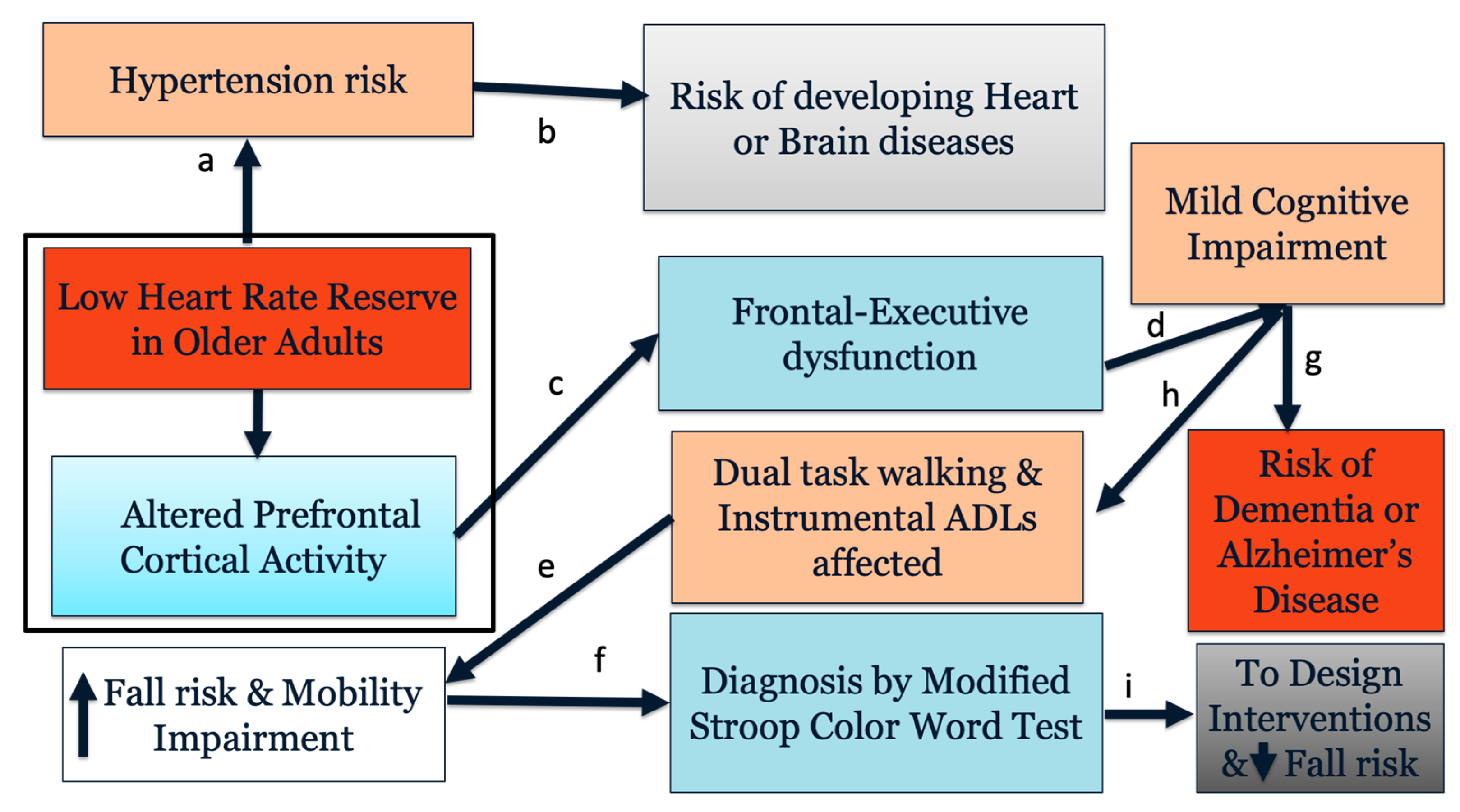
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Physical and Cognitive Assessments
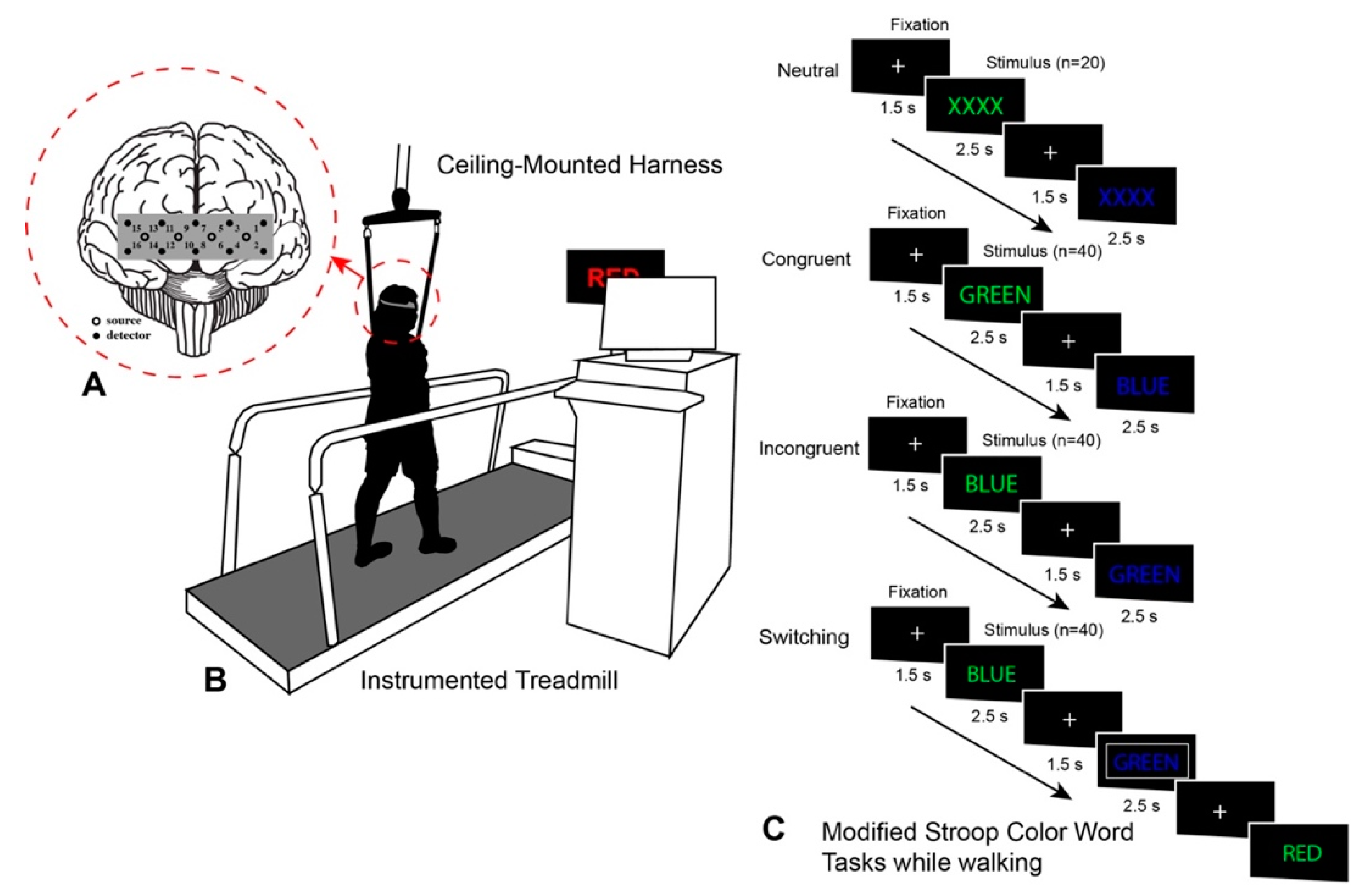
2.4. Dual-Task Paradigm
2.5. Functional Near-Infrared Spectroscopy
2.6. Data Analysis
2.7. Statistical Analysis
3. Results
3.1. Physical and Cognitive Performance
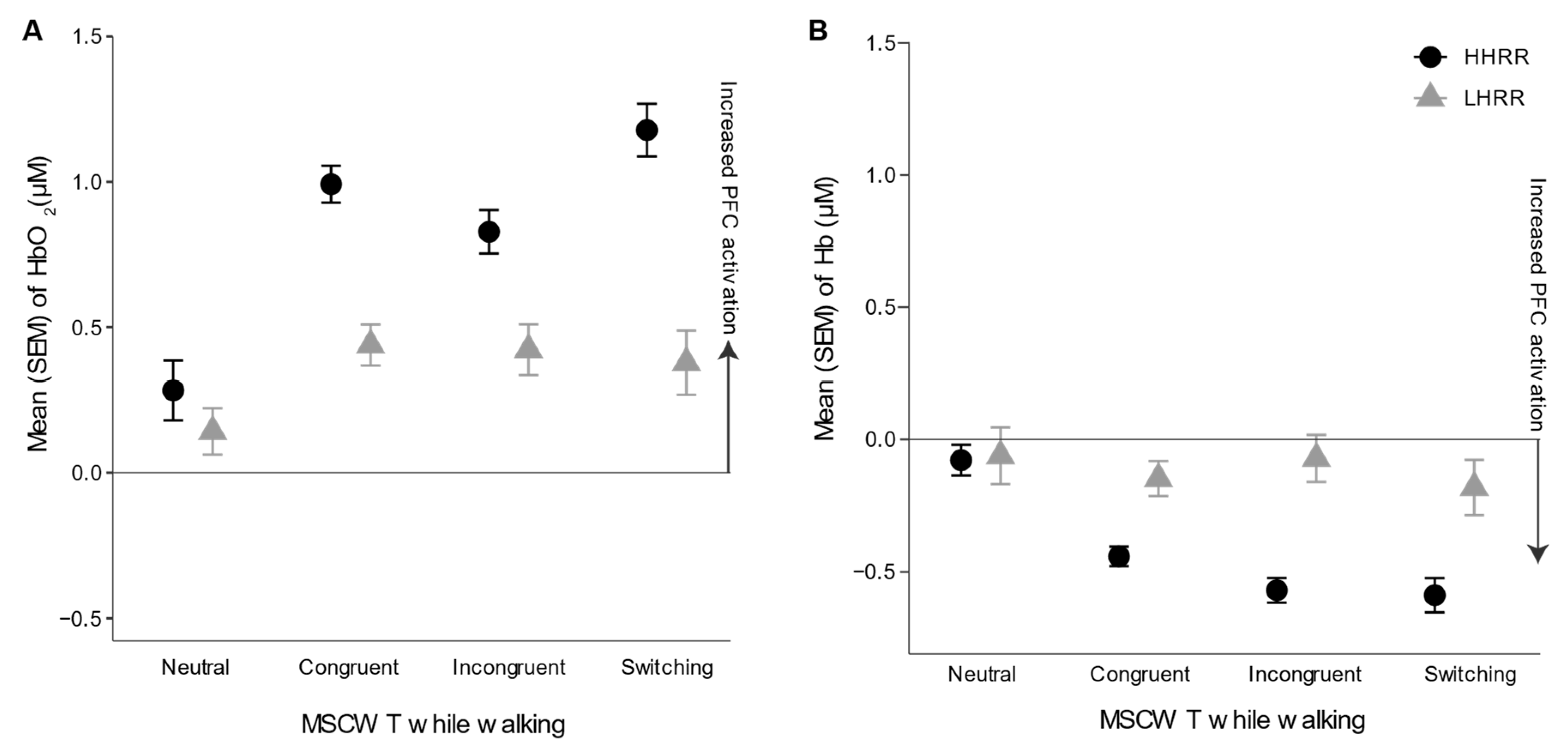
3.2. Prefrontal Cortical Activation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. Heart Disease and Stroke Statistics—2018 Update: A Report From the American Heart Association. Circulation 2018, 137, e67–e492. [Google Scholar] [CrossRef] [PubMed]
- Ferrucci, L.; Giallauria, F.; Guralnik, J.M. Epidemiology of Aging. Radiol. Clin. N. Am. 2008, 46, 643–652. [Google Scholar] [CrossRef]
- Kivipelto, M.; Helkala, E.L.; Hänninen, T.; Laakso, M.P.; Hallikainen, M.; Alhainen, K.; Soininen, H.; Tuomilehto, J.; Nissinen, A. Midlife Vascular Risk Factors and Late-Life Mild Cognitive Impairment: A Population-Based Study. Neurology 2001, 56, 1683–1689. [Google Scholar] [CrossRef] [PubMed]
- McGrath, E.R.; Beiser, A.S.; DeCarli, C.; Plourde, K.L.; Vasan, R.S.; Greenberg, S.M.; Seshadri, S. Blood Pressure from Mid-to Late Life and Risk of Incident Dementia. Neurology 2017, 89, 2447–2454. [Google Scholar] [CrossRef] [PubMed]
- Skoog, I. The Relationship between Blood Pressure and Dementia: A Review. Biomed. Pharmacother. 1997, 51, 367–375. [Google Scholar] [CrossRef]
- Whitmer, R.A.; Sidney, S.; Selby, J.; Johnston, S.C.; Yaffe, K. Midlife Cardiovascular Risk Factors and Risk of Dementia in Late Life. Neurology 2005, 64, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Prasad, V.; Hand, G.; Sui, X.; Shrestha, D.; Lee, D.-C.; Lavie, C.; Jaggers, J.; Blair, S. Association of Exercise Heart Rate Response and Incidence of Hypertension in Men. Mayo Clin. Proc. 2014, 89, 1101–1107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeCarli, C.; Miller, B.L.; Swan, G.E.; Reed, T.; Wolf, P.A.; Carmelli, D. Cerebrovascular and Brain Morphologic Correlates of Mild Cognitive Impairment in the National Heart, Lung, and Blood Institute Twin Study. Arch. Neurol. 2001, 58, 643–647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brubaker, P.H.; Kitzman, D.W. Chronotropic Incompetence: Causes, Consequences, and Management. Circulation 2011, 123, 1010–1020. [Google Scholar] [CrossRef] [Green Version]
- Law, L.L.; Schultz, S.A.; Boots, E.A.; Einerson, J.A.; Dougherty, R.J.; Oh, J.M.; Korcarz, C.E.; Edwards, D.F.; Koscik, R.L.; Dowling, N.M.; et al. Chronotropic Response and Cognitive Function in a Cohort at Risk for Alzheimer’s Disease. J. Alzheimer’s Dis. 2017, 56, 351–359. [Google Scholar] [CrossRef] [Green Version]
- Rosano, C.; Studenski, S.A.; Aizenstein, H.J.; Boudreau, R.M.; Longstreth, W.T.; Newman, A.B. Slower Gait, Slower Information Processing and Smaller Prefrontal Area in Older Adults. Age Ageing 2012, 41, 58–64. [Google Scholar] [CrossRef] [Green Version]
- Holtzer, R.; Mahoney, J.R.; Izzetoglu, M.; Izzetoglu, K.; Onaral, B.; Verghese, J. FNIRS Study of Walking and Walking While Talking in Young and Old Individuals. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2011, 66, 879–887. [Google Scholar] [CrossRef] [Green Version]
- Sheridan, P.H. The Role of Higher-Level Cognitive Function in Gait: Executive Dysfunction Contributes to Fall Risk in Alzherimer´s Disease. Dement. Geriatr. Cogn. Disord. 2011, 24, 125–137. [Google Scholar] [CrossRef] [Green Version]
- Miyai, I.; Tanabe, H.C.; Sase, I.; Eda, H.; Oda, I.; Konishi, I.; Tsunazawa, Y.; Suzuki, T.; Yanagida, T.; Kubota, K. Cortical Mapping of Gait in Humans: A near-Infrared Spectroscopic Topography Study. Neuroimage 2001, 14, 1186–1192. [Google Scholar] [CrossRef] [PubMed]
- Hamacher, D.; Herold, F.; Wiegel, P.; Hamacher, D.; Schega, L. Brain Activity during Walking: A Systematic Review. Neurosci. Biobehav. Rev. 2015, 57, 310–327. [Google Scholar] [CrossRef] [PubMed]
- Holtzer, R.; Mahoney, J.R.; Izzetoglu, M.; Wang, C.; England, S.; Verghese, J. Online Fronto-Cortical Control of Simple and Attention-Demanding Locomotion in Humans. Neuroimage 2015, 112, 152–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menant, J.C.; Maidan, I.; Alcock, L.; Al-Yahya, E.; Cerasa, A.; Clark, D.J.; de Bruin, E.; Fraser, S.; Gramigna, V.; Hamacher, D.; et al. A Consensus Guide to Using Functional Near-Infrared Spectroscopy in Posture and Gait Research. Gait Posture 2020, 82, 254–265. [Google Scholar] [CrossRef]
- Prakash, R.S.; Snook, E.M.; Erickson, K.I.; Colcombe, S.J.; Voss, M.W.; Motl, R.W.; Kramer, A.F. Cardiorespiratory Fitness: A Predictor of Cortical Plasticity in Multiple Sclerosis. Neuroimage 2007, 34, 1238–1244. [Google Scholar] [CrossRef] [PubMed]
- Dupuy, O.; Gauthier, C.J.; Fraser, S.A.; Desjardins-Crèpeau, L.; Desjardins, M.; Mekary, S.; Lesage, F.; Hoge, R.D.; Pouliot, P.; Bherer, L. Higher Levels of Cardiovascular Fitness Are Associated with Better Executive Function and Prefrontal Oxygenation in Younger and Older Women. Front. Hum. Neurosci. 2015, 9, 66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mirelman, A.; Maidan, I.; Bernad-Elazari, H.; Shustack, S.; Giladi, N.; Hausdorff, J.M. Effects of Aging on Prefrontal Brain Activation during Challenging Walking Conditions. Brain Cogn. 2017, 115, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Beurskens, R.; Helmich, I.; Rein, R.; Bock, O. Age-Related Changes in Prefrontal Activity during Walking in Dual-Task Situations: A FNIRS Study. Int. J. Psychophysiol. 2014, 92, 122–128. [Google Scholar] [CrossRef]
- Hawkins, K.A.; Fox, E.J.; Daly, J.J.; Rose, D.K.; Christou, E.A.; McGuirk, T.E.; Otzel, D.M.; Butera, K.A.; Chatterjee, S.A.; Clark, D.J. Prefrontal Over-Activation during Walking in People with Mobility Deficits: Interpretation and Functional Implications. Hum. Mov. Sci. 2018, 59, 46–55. [Google Scholar] [CrossRef] [PubMed]
- Perrochon, A.; Kemoun, G.; Watelain, E.; Dugué, B.; Berthoz, A. The “Stroop Walking Task”: An Innovative Dual-Task for the Early Detection of Executive Function Impairment. Neurophysiol. Clin. 2015, 45, 181–190. [Google Scholar] [CrossRef]
- Chaparro, G.N.; Stine-Morrow, E.A.L.; Hernandez, M.E. Effects of Aerobic Fitness on Cognitive Performance as a Function of Dual-Task Demands in Older Adults. Exp. Gerontol. 2019, 118, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Woollacott, M.; Shumway-Cook, A. Attention and the Control of Posture and Gait: A Review of an Emerging Area of Research. Gait Posture 2002, 16, 1–14. [Google Scholar] [CrossRef]
- Al-Yahya, E.; Dawes, H.; Smith, L.; Dennis, A.; Howells, K.; Cockburn, J. Cognitive Motor Interference While Walking: A Systematic Review and Meta-Analysis. Neurosci. Biobehav. Rev. 2011, 35, 715–728. [Google Scholar] [CrossRef] [PubMed]
- Montero-Odasso, M.; Oteng-Amoako, A.; Speechley, M.; Gopaul, K.; Beauchet, O.; Annweiler, C.; Muir-Hunter, S.W. The Motor Signature of Mild Cognitive Impairment: Results from the Gait and Brain Study. J. Gerontol.-Ser. A Biol. Sci. Med. Sci. 2014, 69, 1415–1421. [Google Scholar] [CrossRef]
- Huang, C.; Mattis, P.; Julin, P. Identifying Functional Imaging Markers of Mild Cognitive Impairment in Early Alzheimer’s and Parkinson’s Disease Using Multivariate Analysis. Clin. Neurosci. Res. 2007, 6, 367–373. [Google Scholar] [CrossRef]
- Cocchini, G.; Sala, S.D.; Logie, R.H.; Pagani, R.; Sacco, L.; Spinnler, H. Dual Task Effects of Walking When Talking in Alzheimer’s Disease. Rev. Neurol. 2004, 160, 74–80. [Google Scholar] [CrossRef]
- Makizako, H.; Doi, T.; Shimada, H.; Yoshida, D.; Tsutsumimoto, K.; Uemura, K.; Suzuki, T. Does a Multicomponent Exercise Program Improve Dual-Task Performance in Amnestic Mild Cognitive Impairment? A Randomized Controlled Trial. Aging Clin. Exp. Res. 2012, 24, 640–646. [Google Scholar] [CrossRef] [PubMed]
- Welsh, K.A.; Breitner, J.C.S.; Magruder-Habib, K.M. Detection of Dementia in the Elderly Using Telephone Screening of Cognitive Status. Neuropsychiatry Neuropsychol. Behav. Neurol. 1993, 6, 103–110. [Google Scholar]
- Kurlowicz, L.; Greenberg, S.A. The Geriatric Depression Scale (GDS) Validation of a Geriatric Depression Screening Scale: A Preliminary Report. AJN Am. J. Nurs. 2007, 107, 67–68. [Google Scholar] [CrossRef]
- Colblindor. Ishihara 38 Plates CVD test. Available online: https://www.color-blindness.com/ishihara-38-plates-cvd-test/ (accessed on 20 November 2021).
- Canadian Society for Exercise Physiology. The Rockport One Mile Walking Test. In The Canadian Physical Activity, Fitness and Lifestyle Approach, 3rd ed.; Canadian Society for Exercise Physiology: Ottawa, ON, Canada, 2010; pp. s9–s15. [Google Scholar]
- Randolph, C.; Tierney, M.C.; Mohr, E.; Chase, T.N. The Repeatable Battery for the Assessment of Neuropsychological Status (RBANS): Preliminary Clinical Validity. J. Clin. Exp. Neuropsychol. 1998, 20, 310–319. [Google Scholar] [CrossRef] [PubMed]
- Bright, P.; Jaldow, E.; Kopelman, M.D. The National Adult Reading Test as a Measure of Premorbid Intelligence: A Comparison with Estimates Derived from Demographic Variables. J. Int. Neuropsychol. Soc. 2002, 8, 847–854. [Google Scholar] [CrossRef] [Green Version]
- Kline, G.M.; Porcari, J.P.; Hintermeister, R.; Freedson, P.S.; Ward, A.; McCarron, R.F.; Ross, J.; Rippe, J.M. Estimation of VO2max from a One-Mile Track Walk, Gender, Age, and Body Weight. Med. Sci. Sports Exerc. 1987, 19, 253–259. [Google Scholar] [CrossRef]
- Tanaka, H.; Monahan, K.D.; Seals, D.R. Age-Predicted Maximal Heart Rate Revisited. J. Am. Coll. Cardiol. 2001, 37, 153–156. [Google Scholar] [CrossRef] [Green Version]
- Benes, J.; Kotrc, M.; Borlaug, B.A.; Lefflerova, K.; Jarolim, P.; Bendlova, B.; Jabor, A.; Kautzner, J.; Melenovsky, V. Resting Heart Rate and Heart Rate Reserve in Advanced Heart Failure Have Distinct Pathophysiologic Correlates and Prognostic Impact. JACC Hear. Fail. 2013, 1, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Chaparro, G.N.; Sosnoff, J.J.; Hernandez, M.E. Effects of Aerobic Fitness on Cognitive Motor Interference during Self-Paced Treadmill Walking in Older Adults. Aging Clin. Exp. Res. 2020, 32, 2539–2547. [Google Scholar] [CrossRef]
- León-Carrion, J.; Damas-López, J.; Martín-Rodríguez, J.F.; Domínguez-Roldán, J.M.; Murillo-Cabezas, F.; Barroso y Martin, J.M.; Domínguez-Morales, M.R. The Hemodynamics of Cognitive Control: The Level of Concentration of Oxygenated Hemoglobin in the Superior Prefrontal Cortex Varies as a Function of Performance in a Modified Stroop Task. Behav. Brain Res. 2008, 193, 248–256. [Google Scholar] [CrossRef]
- Izzetoglu, M.; Chitrapu, P.; Bunce, S.; Onaral, B. Motion Artifact Cancellation in NIR Spectroscopy Using Discrete Kalman Filtering. Biomed. Eng. Online 2010, 9, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huppert, T.; Angela Franceschini, M.; Boas, D. Noninvasive Imaging of Cerebral Activation with Diffuse Optical Tomography. In In Vivo Optical Imaging of Brain Function, 2nd ed.; Frosting, R.D., Ed.; CRC Press LLC: Boca Raton, FL, USA, 2009; pp. 393–433. [Google Scholar]
- Seidler, R.D.; Bernard, J.A.; Burutolu, T.B.; Fling, B.W.; Gordon, M.T.; Gwin, J.T.; Kwak, Y.; Lipps, D.B. Motor Control and Aging: Links to Age-Related Brain Structural, Functional, and Biochemical Effects. Neurosci. Biobehav. Rev. 2010, 34, 721–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stern, Y. Cognitive Reserve. Neuropsychologia 2009, 47, 2015–2028. [Google Scholar] [CrossRef]
- Reuter-Lorenz, P.A.; Cappell, K.A. Neurocognitive Aging and the Compensation Hypothesis. Curr. Dir. Psychol. Sci. 2008, 17, 177–182. [Google Scholar] [CrossRef]
- Bishnoi, A.; Holtzer, R.; Hernandez, M.E. Brain Activation Changes While Walking in Adults with and without Neurological Disease: Systematic Review and Meta-Analysis of Functional near-Infrared Spectroscopy Studies. Brain Sci. 2021, 11, 291. [Google Scholar] [CrossRef] [PubMed]
- Chaparro, G.; Balto, J.M.; Sandroff, B.M.; Holtzer, R.; Izzetoglu, M.; Motl, R.W.; Hernandez, M.E. Frontal Brain Activation Changes Due to Dual-Tasking under Partial Body Weight Support Conditions in Older Adults with Multiple Sclerosis. J. Neuroeng. Rehabil. 2017, 14, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Tombu, M.; Jolicoæur, P. A Central Capacity Sharing Model of Dual-Task Performance. J. Exp. Psychol. Hum. Percept. Perform. 2003, 29, 3. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, S. The Ecological Approach to Cognitive–motor Dual-Tasking: Findings on the Effects of Expertise and Age. Front. Psychol. 2014, 5, 1167. [Google Scholar] [CrossRef] [Green Version]
- Chaparro, G.N.; Singh, D.; Hernandez, M.E. Effects of Aerobic Fitness on Prefrontal Brain Activation While Dual-Task Walking in Older Adults: A Pilot Study. J. Phys. Med. Rehabil. 2021, 3, 1–6. [Google Scholar] [CrossRef]
- Talamonti, D.; Vincent, T.; Fraser, S.; Nigam, A.; Lesage, F.; Bherer, L. The Benefits of Physical Activity in Individuals with Cardiovascular Risk Factors: A Longitudinal Investigation Using FNIRS and Dual-Task Walking. J. Clin. Med. 2021, 10, 579. [Google Scholar] [CrossRef]
- Cabeza, R. Hemispheric Asymmetry Reduction in Older Adults: The HAROLD Model. Psychol. Aging 2002, 17, 85. [Google Scholar] [CrossRef] [PubMed]
- Vermeij, A.; van Beek, A.H.E.A.; Olde Rikkert, M.G.M.; Claassen, J.A.H.R.; Kessels, R.P.C. Effects of Aging on Cerebral Oxygenation during Working-Memory Performance: A Functional Near-Infrared Spectroscopy Study. PLoS ONE 2012, 7, e46210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reuter-Lorenz, P.A.; Jonides, J.; Smith, E.E.; Hartley, A.; Miller, A.; Marshuetz, C.; Koeppe, R.A. Age Differences in the Frontal Lateralization of Verbal and Spatial Working Memory Revealed by PET. J. Cogn. Neurosci. 2000, 12, 174–187. [Google Scholar] [CrossRef]
- Huppert, T.; Barker, J.; Schmidt, B.; Walls, S.; Ghuman, A. Comparison of Group-Level, Source Localized Activity for Simultaneous Functional near-Infrared Spectroscopy-Magnetoencephalography and Simultaneous FNIRS-FMRI during Parametric Median Nerve Stimulation. Neurophotonics 2017, 4, 015001. [Google Scholar] [CrossRef] [PubMed]
- Sato, H.; Yahata, N.; Funane, T.; Takizawa, R.; Katura, T.; Atsumori, H.; Nishimura, Y.; Kinoshita, A.; Kiguchi, M.; Koizumi, H.; et al. A NIRS-FMRI Investigation of Prefrontal Cortex Activity during a Working Memory Task. Neuroimage 2013, 83, 158–173. [Google Scholar] [CrossRef]
- Scarapicchia, V.; Brown, C.; Mayo, C.; Gawryluk, J.R. Functional Magnetic Resonance Imaging and Functional Near-Infrared Spectroscopy: Insights from Combined Recording Studies. Front. Hum. Neurosci. 2017, 11, 419. [Google Scholar] [CrossRef]
- Bhambhani, Y.; Maikala, R.; Farag, M.; Rowland, G. Reliability of Near-Infrared Spectroscopy Measures of Cerebral Oxygenation and Blood Volume during Handgrip Exercise in Nondisabled and Traumatic Brain-Injured Subjects. J. Rehabil. Res. Dev. 2006, 43, 845. [Google Scholar] [CrossRef]
- Dravida, S.; Noah, J.A.; Zhang, X.; Hirsch, J. Comparison of Oxyhemoglobin and Deoxyhemoglobin Signal Reliability with and without Global Mean Removal for Digit Manipulation Motor Tasks. Neurophotonics 2017, 5, 011006. [Google Scholar] [CrossRef]
- Stuart, S.; Belluscio, V.; Quinn, J.F.; Mancini, M. Pre-Frontal Cortical Activity during Walking and Turning Is Reliable and Differentiates across Young, Older Adults and People with Parkinson’s Disease. Front. Neurol. 2019, 10, 536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hernandez, M.E.; O’Donnell, E.; Chaparro, G.; Holtzer, R.; Izzetoglu, M.; Sandroff, B.M.; Motl, R.W. Brain Activation Changes during Balance- And Attention-Demanding Tasks in Middle- And Older-Aged Adults with Multiple Sclerosis. Mot. Control 2019, 23, 498–517. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, M.E.; Holtzer, R.; Chaparro, G.; Jean, K.; Balto, J.M.; Sandroff, B.M.; Izzetoglu, M.; Motl, R.W. Brain Activation Changes during Locomotion in Middle-Aged to Older Adults with Multiple Sclerosis. J. Neurol. Sci. 2016, 370, 277–283. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | LHRR (n = 14) | HHRR (n = 14) | p-Value |
|---|---|---|---|
| Males/females | 4/10 | 6/8 | 0.693 |
| Age (years) | 73.8 ± 7.0 | 61.8 ± 8.0 | 0.0002 *** |
| Aerobic capacity (estimated VO2 max) | 25.6 ± 8.6 | 33.2 ± 6.4 | 0.019 * |
| Education (years) | 7.3 ± 4.5 | 7.5 ± 6.6 | 0.949 |
| Heart rate reserve (bpm) | 57.5 ± 12.5 | 85.3 ± 8.7 | <0.0001 *** |
| NART | 113.4 ± 6.9 | 110.5 ± 7.1 | 0.335 |
| RBANS | 96.4 ± 9.1 | 98.8 ± 8.6 | 0.498 |
| Rockport gait speed (m/s) | 1.8 ± 0.2 | 2.0 ± 0.3 | 0.030 * |
| LHRR (n = 14) | HHRR (n = 14) | |
|---|---|---|
| Gait speed (m/s) | ||
| Neutral | 0.97 ± 0.27 | 0.93 ± 0.32 |
| Congruent | 0.94 ± 0.29 | 1.03 ± 0.28 |
| Incongruent | 1.01 ± 0.27 | 1.06 ± 0.26 |
| Switching | 1.08 ± 0.27 | 1.07 ± 0.28 |
| Accuracy (%) | ||
| Neutral | 99.6 ± 1.3 | 100.0 ± 0.0 |
| Congruent | 99.8 ± 0.7 | 99.8 ± 0.8 |
| Incongruent | 95.7 ± 3.1 | 96.3 ± 2.4 |
| Switching *** | 70.4 ± 24.0 | 92.8 ± 5.1 |
| β | SE | p-Value | |
|---|---|---|---|
| Age | 0.015 | 0.006 | 0.021 * |
| Aerobic capacity | 0.022 | 0.006 | <0.001 *** |
| Task: congruent vs. neutral | 0.439 | 0.090 | <0.001 *** |
| Task: incongruent vs. neutral | 0.301 | 0.090 | <0.001 *** |
| Task: switching vs. neutral | 0.459 | 0.090 | <0.001 *** |
| HRR level: HHRR vs. LHRR | 0.062 | 0.151 | 0.682 |
| Channel 12 vs. Channel 1 | 0.594 | 0.266 | 0.026 * |
| Channel 14 vs. Channel 1 | 0.650 | 0.269 | 0.016 * |
| HHRR × congruent | 0.271 | 0.116 | 0.020 * |
| HHRR × incongruent | 0.245 | 0.116 | 0.035 * |
| HHRR × switching | 0.437 | 0.116 | <0.001 *** |
| β | SE | p Value | |
|---|---|---|---|
| Age | 0.105 | 0.004 | 0.008 ** |
| Aerobic capacity | −0.007 | 0.004 | 0.045 * |
| Task: congruent vs. neutral | −0.193 | 0.085 | 0.023 * |
| Task: incongruent vs. neutral | −0.220 | 0.085 | <0.010 ** |
| Task: switching vs. neutral | −0.314 | 0.085 | <0.001 *** |
| HRR level: HHRR vs. LHRR | −0.216 | 0.105 | 0.039 * |
| Channel 8 vs. Channel 1 | 0.582 | 0.164 | <0.001 *** |
| Channel 10 vs. Channel 1 | 0.422 | 0.164 | 0.010 * |
| Channel 12 vs. Channel 1 | 0.461 | 0.160 | 0.004 ** |
| Channel 14 vs. Channel 1 | 0.319 | 0.162 | <0.050 * |
| HHRR × congruent | −0.171 | 0.109 | 0.118 |
| HHRR × incongruent | −0.272 | 0.109 | 0.013 * |
| HHRR × switching | −0.196 | 0.109 | 0.072 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bishnoi, A.; Chaparro, G.N.; Hernandez, M.E. Effect of Heart Rate Reserve on Prefrontal Cortical Activation While Dual-Task Walking in Older Adults. Int. J. Environ. Res. Public Health 2022, 19, 47. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010047
Bishnoi A, Chaparro GN, Hernandez ME. Effect of Heart Rate Reserve on Prefrontal Cortical Activation While Dual-Task Walking in Older Adults. International Journal of Environmental Research and Public Health. 2022; 19(1):47. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010047
Chicago/Turabian StyleBishnoi, Alka, Gioella N. Chaparro, and Manuel E. Hernandez. 2022. "Effect of Heart Rate Reserve on Prefrontal Cortical Activation While Dual-Task Walking in Older Adults" International Journal of Environmental Research and Public Health 19, no. 1: 47. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph19010047