
Factors Associated with Smoke-Free Pregnancy among Aboriginal and Torres Strait Women and Their Experience of Quitting Smoking in Pregnancy: A Mixed Method Cross-Sectional Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sampling
2.2. Data Analysis
3. Results
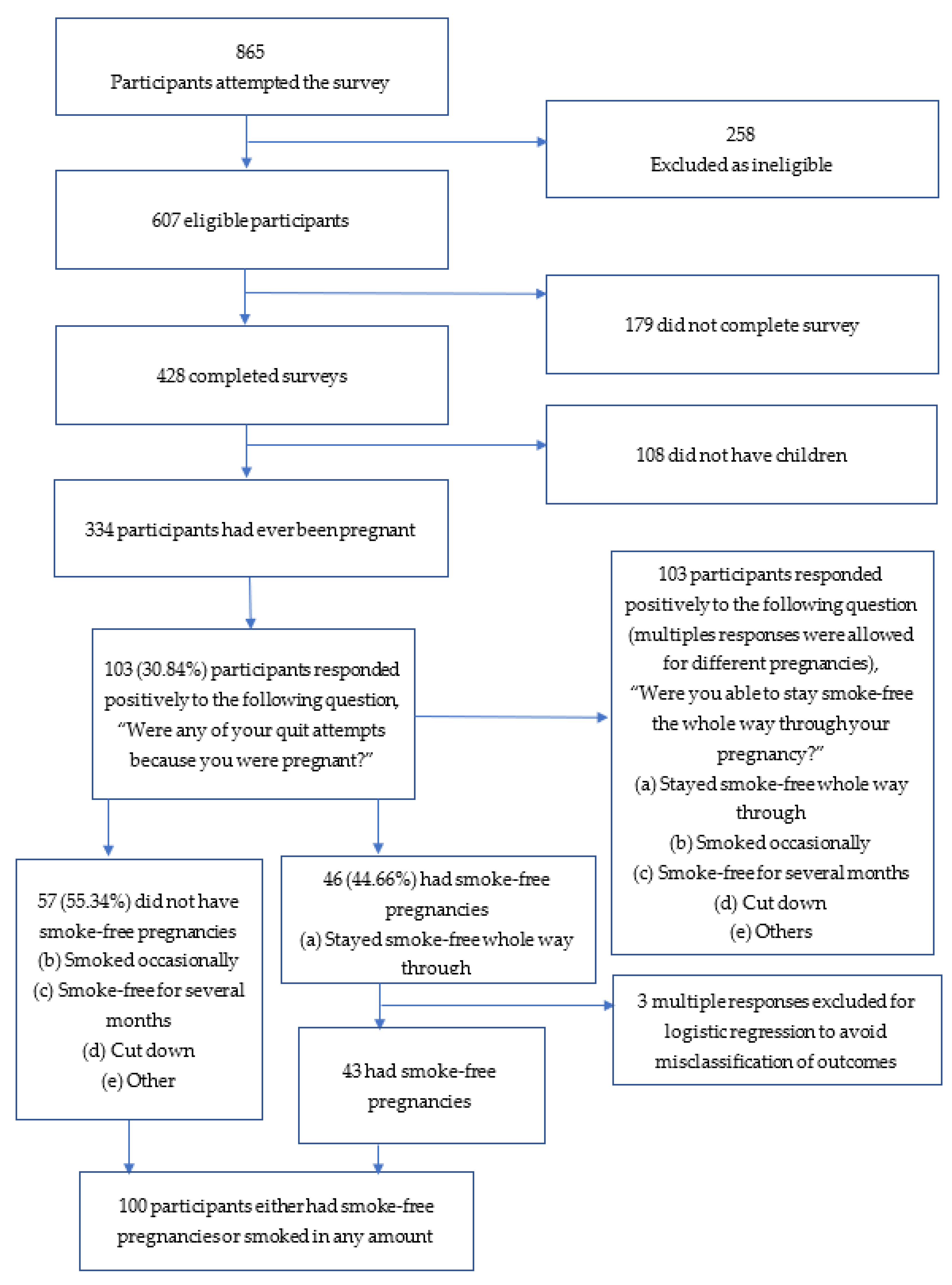
3.1. Participation Description
3.2. Factors Associated with Smoke-Free Pregnancy
3.3. Women’s Experiences of Smoking Cessation during Pregnnacy
3.3.1. Motivations for Quitting Smoking
“As soon as I heard the baby’s heart beat I quit.”37 year old, stayed smoke-free
“My morning sickness was aggravated by the smell of smoke so I didn’t smoke and couldn’t be around smokers.”33 year old, smoked occasionally
3.3.2. The Levels of Behavioural Change May Vary
“I was too stressed and decided it would be better for me to cut down instead.”42 year old, cut down
“It was hard at first so I cut down in the beginning until I finally quit. It made it easier to quit knowing I was growing a bub.”19 year old, stayed smoke-free
“I quit as soon as I found out [I was pregnant] with my first and didn’t start again until my 3rd child was 3.”35 year old, stayed smoke-free
3.3.3. The Experience of Change Is Diverse, either Difficult or Easy
“It was hard at first but stopped after 3–4 months into pregnancy and only smoked when I was stressing out.”17 year old, smoked occasionally and remained smoke-free for months
“With my first I was advised to continue to smoke as trying to quit was putting too much stress on my body and could cause loss of baby, I was told to cut down, which I did. Second pregnancy I quit altogether and lost my twins at 18 weeks, 3rd and 4th I quit in the last few months of pregnancy.”33 year old, remained smoke-free for months and cut down
“Quitting while pregnant was easy, just wanted to give my child the best start to life.”23 year old, stayed smoke-free
3.3.4. Experience of Change Evolves over Time and in Different Pregnancies
“I quit for the first few months, I started stressing at work midway through my pregnancy and started smoking again.”22 year old, smoked occasionally
“Its hard to do whilst pregnant. First and second I smoked most the way through cutting down. Third I gave up for months but not all. Last I gave up before getting pregnant.”35 year old, stayed smoke-free, remained smoke-free for months, and cut down
4. Discussion
4.1. Strength and Limitations of the Study
4.2. Implications for Policy and Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gould, G.S.; Patten, C.; Glover, M.; Kira, A.; Jayasinghe, H. Smoking in pregnancy among Indigenous women in high-income countries: A narrative review. Nicotine Tob. Res. 2017, 19, 506–517. [Google Scholar] [CrossRef]
- Rahman, T.; Eftekhari, P.; Bovill, M.; Baker, A.; Gould, G. Socioecological mapping of barriers and enablers to smoking cessation in Indigenous Australian women during pregnancy and postpartum: A systematic review. Nicotine Tob. Res. 2021, 23, 888–899. [Google Scholar] [CrossRef]
- Small, S.; Porr, C.; Swab, M.; Murray, C. Experiences and cessation needs of Indigenous women who smoke during pregnancy: A systematic review of qualitative evidence. JBI Database Syst. Rev. Implement. Rep. 2018, 16, 385–452. [Google Scholar] [CrossRef]
- Cnattingius, S. The epidemiology of smoking during pregnancy: Smoking prevalence, maternal characteristics, and pregnancy outcomes. Nicotine Tob. Res. 2004, 6, S125–S140. [Google Scholar] [CrossRef]
- Banderali, G.; Martelli, A.; Landi, M.; Moretti, F.; Betti, F.; Radaelli, G.; Lassandro, C.; Verduci, E. Short and long term health effects of parental tobacco smoking during pregnancy and lactation: A descriptive review. J. Transl. Med. 2015, 13, 327. [Google Scholar] [CrossRef]
- Bovill, M. What ngidhi yinaaru nhal yayi (this woman told me) about smoking during pregnancy. Med. J. Aust. 2020, 212, 358–359.e351. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. Smoking. Available online: https://www.abs.gov.au/statistics/health/health-conditions-and-risks/smoking/latest-release (accessed on 4 October 2021).
- Australian Institute of Health and Welfare. Austrlia’s Mothers and Babies 2017—In Brief; AIHW: Canberra, Australia, 2019.
- Wood, L.; France, K.; Hunt, K.; Eades, S.; Slack-Smith, L. Indigenous women and smoking during pregnancy: Knowledge, cultural contexts and barriers to cessation. Soc. Sci. Med. 2008, 66, 2378–2389. [Google Scholar] [CrossRef] [PubMed]
- Passey, M.E.; Gale, J.T.; Sanson-Fisher, R.W. “It’s almost expected”: Rural Australian aboriginal women’s reflections on smoking initiation and maintenance: A qualitative study. BMC Womens Health 2011, 11, 12. [Google Scholar] [CrossRef] [PubMed]
- Gould, G.S.; Bovill, M.; Clarke, M.J.; Gruppetta, M.; Cadet-James, Y.; Bonevski, B. Chronological narratives from smoking initiation through to pregnancy of Indigenous Australian women: A qualitative study. Midwifery 2017, 52, 27–33. [Google Scholar] [CrossRef]
- Bovill, M.; Gruppetta, M.; Cadet-James, Y.; Clarke, M.; Bonevski, B.; Gould, G.S. Wula (Voices) of Aboriginal women on barriers to accepting smoking cessation support during pregnancy: Findings from a qualitative study. Women Birth 2018, 31, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Bovill, M.; Bar-Zeev, Y.; Bonevski, B.; Gruppetta, M.; Oldmeadow, C.; Hall, A.; Reath, J.; Gould, G.S. Aboriginal Wingadhan Birrang (woman’s journey) of smoking cessation during pregnancy as they participate in the ICAN QUIT in pregnancy pilot step-wedge trial. Women Birth 2020, 33, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Gould, G.S.; Munn, J.; Avuri, S.; Hoff, S.; Cadet-James, Y.; McEwen, A.; Clough, A.R. “Nobody smokes in the house if there’s a new baby in it”: Aboriginal perspectives on tobacco smoking in pregnancy and in the household in regional NSW Australia. Women Birth 2013, 26, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Mendelsohn, C.; Gould, G.S.; Oncken, C. Management of smoking in pregnant women. Aust. Fam. Physician 2014, 43, 46. [Google Scholar] [PubMed]
- Heil, S.H.; Higgins, S.T.; Bernstein, I.M.; Solomon, L.J.; Rogers, R.E.; Thomas, C.S.; Badger, G.J.; Lynch, M.E. Effects of voucher-based incentives on abstinence from cigarette smoking and fetal growth among pregnant women. Addiction 2008, 103, 1009–1018. [Google Scholar] [CrossRef] [PubMed]
- Pearson, J.L.; Waa, A.; Siddiqi, K.; Edwards, R.; Nez Henderson, P.; Webb Hooper, M. Naming racism, not race, as a determinant of tobacco-related health disparities. Nicotine Tob. Res. 2021, 23, 885–887. [Google Scholar] [CrossRef] [PubMed]
- Gilligan, C.; Sanson-Fisher, R.W.; D’Este, C.; Eades, S.; Wenitong, M. Knowledge and attitudes regarding smoking during pregnancy among Aboriginal and Torres Strait Islander women. Med. J. Aust. 2009, 190, 557–561. [Google Scholar] [CrossRef] [PubMed]
- Johnston, V.; Thomas, D.P.; McDonnell, J.; Andrews, R.M. Maternal smoking and smoking in the household during pregnancy and postpartum: Findings from an indigenous cohort in the Northern Territory. Med. J. Aust. 2011, 194, 556–559. [Google Scholar] [CrossRef]
- Bovill, M.; Chamberlain, C.; Bennett, J.; Longbottom, H.; Bacon, S.; Field, B.; Hussein, P.; Berwick, R.; Gould, G.; O’Mara, P. Building an indigenous-led evidence base for smoking cessation care among Aboriginal and Torres Strait Islander women during pregnancy and beyond: Research protocol for the which way? project. Int. J. Environ. Res. Public Health 2021, 18, 1342. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Panaretto, K.S.; Wenitong, M.; Button, S.; Ring, I.T. Aboriginal community controlled health services: Leading the way in primary care. Med. J. Aust. 2014, 200, 649–652. [Google Scholar] [CrossRef]
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Rickert, W.; Robinson, J. Measuring the heaviness of smoking: Using self-reported time to the first cigarette of the day and number of cigarettes smoked per day. Br. J. Addict. 1989, 84, 791–800. [Google Scholar] [CrossRef]
- Thomas, D.P.; Panaretto, K.S.; Stevens, M.; Borland, R. Dependence in a national sample of Aboriginal and Torres Strait Islander daily smokers. Med. J. Aust. 2015, 202, S39–S44. [Google Scholar] [CrossRef] [PubMed]
- Gould, G.S.; Chiu, S.; Oldmeadow, C.; Bar-Zeev, Y.; Bovill, M. Pregnant Aboriginal women self-assess health risks from smoking and efficacy to quit over time using an adapted Risk Behaviour Diagnosis (RBD) Scale. J. Smok. Cessat. 2020, 15, 198–205. [Google Scholar] [CrossRef]
- Riaz, M.; Lewis, S.; Coleman, T.; Aveyard, P.; West, R.; Naughton, F.; Ussher, M. Which measures of cigarette dependence are predictors of smoking cessation during pregnancy? Analysis of data from a randomized controlled trial. Addiction 2016, 111, 1656–1665. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. 1270.0.55.005—Australian Statistical Geography Standard (ASGS): Volume 5—Remoteness Structure, July 2016. Available online: https://www.abs.gov.au/AUSSTATS/[email protected]/DetailsPage/1270.0.55.005July%202016?OpenDocument (accessed on 24 May 2021).
- Ogundimu, E.O.; Altman, D.G.; Collins, G.S. Adequate sample size for developing prediction models is not simply related to events per variable. J. Clin. Epidemiol. 2016, 76, 175–182. [Google Scholar] [CrossRef]
- StataCorp. Stata Statistical Software: Release 15; StataCorp LLC: College Station, TX, USA, 2017. [Google Scholar]
- Walsh, R.A.; Redman, S.; Brinsmead, M.W.; Fryer, J.L. Predictors of smoking in pregnancy and attitudes and knowledge of risks of pregnant smokers. Drug Alcohol Rev. 1997, 16, 41–67. [Google Scholar] [CrossRef] [PubMed]
- Australia’s Health 2018. Available online: https://www.aihw.gov.au/reports/australias-health/australias-health-2018/contents/table-of-contents (accessed on 10 October 2021).
- NVivo Qualitative Data Analysis Software; Version 12; QSR International Pty Ltd.: Melbourne, Australia, 2018.
- Australian Institute of Health and Welfare. Indigenous Australians’ Use of Health Services. Available online: https://www.aihw.gov.au/reports/australias-health/indigenous-australians-use-of-health-services (accessed on 25 June 2021).
- Marley, J.V.; Atkinson, D.; Kitaura, T.; Nelson, C.; Gray, D.; Metcalf, S.; Maguire, G.P. The be our ally beat smoking (BOABS) study, a randomised controlled trial of an intensive smoking cessation intervention in a remote aboriginal Australian health care setting. BMC Public Health 2014, 14, 32. [Google Scholar] [CrossRef] [PubMed]
- DiGiacomo, M.; Davidson, P.; Abbott, P.; Davison, J.; Moore, L.; Thompson, S. Smoking cessation in indigenous populations of Australia, New Zealand, Canada, and the United States: Elements of effective interventions. Int. J. Environ. Res. Public Health 2011, 8, 388–410. [Google Scholar] [CrossRef]
- Bond, C.; Brough, M.; Spurling, G.; Hayman, N. ‘It had to be my choice’Indigenous smoking cessation and negotiations of risk, resistance and resilience. Health Risk Soc. 2012, 14, 565–581. [Google Scholar] [CrossRef]
- Chamberlain, C.; Perlen, S.; Brennan, S.; Rychetnik, L.; Thomas, D.; Maddox, R.; Alam, N.; Banks, E.; Wilson, A.; Eades, S. Evidence for a comprehensive approach to Aboriginal tobacco control to maintain the decline in smoking: An overview of reviews among Indigenous peoples. Syst. Rev. 2017, 6, 135. [Google Scholar] [CrossRef] [PubMed]
- Australian Institute of Health and Welfare. National Core Maternity Indicators. Available online: https://www.aihw.gov.au/reports/mothers-babies/ncmi-data-visualisations/contents/antenatal-period-indicators/smoking-during-pregnancy (accessed on 28 July 2021).
- Bar-Zeev, Y.; Bonevski, B.; Twyman, L.; Watt, K.; Atkins, L.; Palazzi, K.; Oldmeadow, C.; Gould, G.S. Opportunities missed: A cross-sectional survey of the provision of smoking cessation care to pregnant women by Australian general practitioners and obstetricians. Nicotine Tob. Res. 2017, 19, 636–641. [Google Scholar] [CrossRef] [PubMed]
- Askew, D.A.; Guy, J.; Lyall, V.; Egert, S.; Rogers, L.; Pokino, L.-a.; Manton-Williams, P.; Schluter, P.J. A mixed methods exploratory study tackling smoking during pregnancy in an urban aboriginal and torres strait islander primary health care service. BMC Public Health 2019, 19, 343. [Google Scholar] [CrossRef] [PubMed]
- Gould, G.S.; Bovill, M.; Pollock, L.; Bonevski, B.; Gruppetta, M.; Atkins, L.; Carson-Chahhoud, K.; Boydell, K.M.; Gribbin, G.R.; Oldmeadow, C. Feasibility and acceptability of Indigenous Counselling and Nicotine (ICAN) QUIT in Pregnancy multicomponent implementation intervention and study design for Australian Indigenous pregnant women: A pilot cluster randomised step-wedge trial. Addict. Behav. 2019, 90, 176–190. [Google Scholar] [CrossRef]
- Lyall, V.; Guy, J.; Egert, S.; Pokino, L.-A.; Rogers, L.; Askew, D. “They Were Willing to Work with Me and Not Pressure Me”: A qualitative investigation into the features of value of a smoking cessation in pregnancy program for aboriginal and torres strait islander women. Int. J. Environ. Res. Public Health 2021, 18, 49. [Google Scholar] [CrossRef] [PubMed]
- Gould, G.S.; Chiu, S.; Oldmeadow, C.; Bar-Zeev, Y. General practitioner and obstetrician views on system changes to improve smoking cessation care in pregnancy in Australia: A cross-sectional survey. J. Smok. Cessat. 2020, 15, 136–142. [Google Scholar] [CrossRef]
- Doogan, N.; Roberts, M.; Wewers, M.; Stanton, C.; Keith, D.; Gaalema, D.; Kurti, A.; Redner, R.; Cepeda-Benito, A.; Bunn, J. A growing geographic disparity: Rural and urban cigarette smoking trends in the United States. Prev. Med. 2017, 104, 79–85. [Google Scholar] [CrossRef]
- Mitchel, E.; Bandara, P.; Smith, V. Tackling Indigenous Smoking Program: Final Evaluation Report Prepared for the Australian Government Department of Health; The Cultural and Indigenous Research Centre Australia (CIRCA): Canberra, Australia, 2018. [Google Scholar]
- Social Inequality in Cigarette Consumption, Cigarette Dependence, and Intention to Quit among Norwegian Smokers. Available online: https://downloads.hindawi.com/journals/bmri/2015/835080.pdf (accessed on 10 October 2021).
- Siahpush, M.; McNeill, A.; Borland, R.; Fong, G. Socioeconomic variations in nicotine dependence, self-efficacy, and intention to quit across four countries: Findings from the International Tobacco Control (ITC) four country survey. Tob. Control. 2006, 15, iii71–iii75. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, Y.-L.; Gamst, A.C.; Cummins, S.E.; Wolfson, T.; Zhu, S.-H. Comparison of smoking cessation between education groups: Findings from 2 US National Surveys over 2 decades. Am. J. Public Health 2015, 105, 373–379. [Google Scholar] [CrossRef]
- Baxter, S.; Everson-Hock, E.; Messina, J.; Guillaume, L.; Burrows, J.; Goyder, E. Factors relating to the uptake of interventions for smoking cessation among pregnant women: A systematic review and qualitative synthesis. Nicotine Tob. Res. 2010, 12, 685–694. [Google Scholar] [CrossRef] [PubMed]
- McNair Ingenuity Research. Media Use Amongst Aboriginal and Torres Strait Islander People. 2014. Available online: https://mcnair.com.au/wp-content/uploads/Media-Usage-amongst-Aboriginal-and-Torres-Strait-Islander-People-McNai....pdf (accessed on 16 July 2021).
- Colonna, E.; Maddox, R.; Cohen, R.; Marmor, A.; Doery, K.; Thurber, K.; Thomas, D.; Guthrie, J.; Wells, S.; Lovett, R. Review of Tobacco Use among Aboriginal and Torres Strait Islander Peoples; Australian Indigenous HealthInfoNet: Perth, WA, Australia, 2020. [Google Scholar]
- Australian Bureau of Statistics. Estimates of Aboriginal and Torres Strait Islander Australians. Available online: https://www.abs.gov.au/statistics/people/aboriginal-and-torres-strait-islander-peoples/estimates-aboriginal-and-torres-strait-islander-australians/jun-2016 (accessed on 8 October 2021).
- Wright, A.; Thurber, K.A.; Yap, M.; Du, W.; Banks, E.; Walker, J.; Irwin, F.; Sanders, W.; Lovett, R. Who responds? An examination of response rates to a national postal survey of Aboriginal and Torres Strait Islander adults, 2018–2019. BMC Med. Res. Methodol. 2020, 20, 149. [Google Scholar] [CrossRef] [PubMed]
- Australian Government Department of Health. Indigenous Australians’ Health Programme. Available online: https://www.health.gov.au/initiatives-and-programs/indigenous-australians-health-programme (accessed on 30 July 2021).
- Australian Government Department of Health. Indigenous Smoking and Pregnancy Roundtable–Summary Report; Australian Government Department of Health: Canberra, Australia, 2020.


{kind=link}
| Variables | Counts (Column %) |
|---|---|
| Are you Aboriginal and/or Torres Strait Islander? * | |
| Aboriginal | 98 (95.15) |
| Aboriginal and Torres Strait Islander | 5 (4.85) |
| What is your age? | |
| Mean and Standard Deviation (sd) (mean 32.13, sd ± 7.47) | |
| 16–25 | 21 (20.39) |
| 26–35 | 45 (43.69) |
| 36 and above | 37 (35.92) |
| What education level have you completed? | |
| Up to Year 11 | 35 (33.98) |
| Year 12 | 20 (19.42) |
| Current student at university/TAFE/Apprentice | 20 (19.42) |
| Trade certificate/University degree | 28 (27.18) |
| What state do you live in? | |
| NSW | 47 (45.63) |
| QLD | 29 (28.16) |
| VIC | 12 (11.56) |
| Rest of Australia | 15 (14.56) |
| Do you use an Aboriginal Health Service(s)? | |
| Yes | 79 (76.70) |
| No | 24 (23.30) |
| What is your post code? (Remoteness) | |
| Urban | 58 (56.31) |
| Regional/remote | 45 (43.69) |
| How many children currently live in your household? | |
| None | 3 (2.91) |
| 1–2 | 53 (51.46) |
| 3 or more | 44 (42.72) |
| Pregnant | 6 (5.83) |
| How long ago was your latest quit attempt | |
| Days | 11 (10.68) |
| Weeks | 13 (12.62) |
| Months | 79 (76.70) |
| Of all the times you tried to quit smoking, what was the longest period you stayed completely of the smokes for? | |
| Hours | 2 (1.94) |
| Days | 7 (6.80) |
| Weeks | 13 (12.62) |
| Months | 33 (32.04) |
| Years | 46 (44.66) |
| Don’t know | 2 (1.94) |
| On your most recent quit attempt, did you stop smoking suddenly or did you gradually cut down your smokes? | |
| Stopped suddenly | 59 (57.28) |
| Reduced gradually | 44 (42.72) |
| Have you ever used any type stop-smoking medications? | |
| Yes | 40 (38.83) |
| No | 63 (61.17) |
| Would you say you are | |
| Current smokers | 59 (57.28) |
| Ex-smokers | 44 (42.72) |
| In the last month, have you tried to cut down the number of smokes you have each day? ** | |
| Yes | 40 (67.80) |
| No | 19 (32.20) |
| Heaviness of Smoking Index ** | |
| Low | 40 (67.80) |
| Moderate | 18 (30.51) |
| High | 1 (1.69) |
| How much of the time have you felt the urge to smoke in the last 24 h? (FUTS) ** | |
| Not at all | 5 (8.47) |
| A little of the time | 5 (8.47) |
| Some of the time | 17 (28.81) |
| A lot of the time | 20 (33.90) |
| Almost all the time | 4 (6.78) |
| All the time | 8(13.56) |
| FUTS (low vs. high) ** | |
| Low | 27 (45.76) |
| High | 32 (54.24 |
| In general how strong are your urges to smoke (in the last 24 h)? (SUTS) * | |
| No urges | 3 (5.08) |
| Slight | 5 (8.47) |
| Moderate | 21 (35.59) |
| Strong | 17 (28.81) |
| Very strong | 6 (10.17) |
| Extremely strong | 7 (11.86) |
| SUTS (low vs high) ** | |
| Low | 29 (49.15) |
| High | 30 (50.85) |
| Variables | Stayed Smoke-Free Whole Way through Pregnancy (n = 43) | Did Not Stay Smoke-Free Whole Way through Pregnancy (n = 57) | Pearson’s Chi-Square Test | ||||
|---|---|---|---|---|---|---|---|
| n | Column % | n | Column % * | χ2 | df | p-Value | |
| What is your age? | |||||||
| Mean and Standard Deviation (sd) | 33.02 (7.52) | 31.49 (7.67) | 0.318 | ||||
| 16–25 | 8 | 18.60 | 13 | 22.81 | |||
| 26–35 | 17 | 39.53 | 25 | 43.86 | |||
| 36 and above | 18 | 41.86 | 19 | 33.33 | 0.80 | 2 | 0.671 |
| What education level have you completed? | |||||||
| Up to Year 11 | 15 | 34.88 | 20 | 35.09 | |||
| Year 12 | 7 | 16.28 | 13 | 22.81 | |||
| Current student at university/TAFE/Apprentice | 8 | 18.60 | 11 | 19.30 | |||
| Trade certificate/University degree | 13 | 30.23 | 13 | 22.81 | 1.05 | 3 | 0.790 |
| Do you use an Aboriginal Health Service(s)? | |||||||
| Yes | 39 | 90.70 | 38 | 66.67 | |||
| No | 4 | 9.30 | 19 | 33.33 | 7.99 | 1 | 0.005 |
| What is your post code? (Remoteness) | |||||||
| Urban | 17 | 39.53 | 38 | 66.67 | |||
| Regional/Remote | 26 | 60.47 | 19 | 33.33 | 7.29 | 1 | 0.007 |
| How long ago was your latest quit attempt ∆ | |||||||
| Days | 4 | 9.30 | 7 | 12.28 | |||
| Weeks | 4 | 9.30 | 9 | 15.79 | |||
| Months | 35 | 81.40 | 41 | 71.93 | 0.583 | ||
| Of all the times you tried to quit smoking, what was the longest period you stayed completely of the smokes for? ∆ | |||||||
| Hours | 0 | 0.00 | 2 | 3.51 | |||
| Days | 1 | 2.33 | 6 | 10.53 | |||
| Weeks | 0 | 0.00 | 13 | 22.81 | |||
| Months | 9 | 20.93 | 23 | 40.35 | |||
| Years | 32 | 74.42 | 12 | 21.05 | |||
| Don’t know | 1 | 2.33 | 1 | 2.33 | <0.001 | ||
| On your most recent quit attempt, did you stop smoking suddenly or did you gradually cut down your smokes? | |||||||
| Stopped suddenly | 27 | 62.79 | 27 | 47.37 | |||
| Reduced gradually | 16 | 37.21 | 30 | 52.63 | 1.03 | 1 | 0.310 |
| Have you ever used any type stop-smoking medications? | |||||||
| Yes | 13 | 30.23 | 24 | 42.11 | |||
| No | 30 | 69.77 | 33 | 57.89 | 1.48 | 1 | 0.223 |
| In the last month, have you tried to cut down the number of smokes you have each day? *,∆ | |||||||
| Yes | 9 | 69.23 | 31 | 67.39 | |||
| No | 4 | 30.77 | 15 | 32.61 | 1.000 | ||
| How many cigarettes do you usually smoke per day (on the days you smoke)? † | |||||||
| Number of cigarettes smoked per day; Median and (Q1–Q3) | 6 (4–10) | 10 (6–15) | 0.134 | ||||
| Heaviness of Smoking Index *,∆ | |||||||
| Low | 11 | 84.62 | 29 | 63.04 | |||
| Moderate | 2 | 15.38 | 16 | 34.78 | |||
| High | 0 | 0.00 | 1 | 2.17 | 0.460 | ||
| How much of the time have you felt the urge to smoke in the last 24 h? (FUTS) * | |||||||
| Low | 8 | 61.54 | 19 | 41.30 | |||
| High | 5 | 38.46 | 27 | 58.70 | 1.67 | 1 | 0.196 |
| In general how strong are your urges to smoke (in the last 24 h)? (SUTS) * | |||||||
| Low | 8 | 61.54 | 21 | 45.65 | |||
| High | 5 | 38.46 | 25 | 54.35 | 1.02 | 1 | 0.312 |
| Variables | Multivariable Analysis | ||||
|---|---|---|---|---|---|
| n | % | AOR † | 95% CI ∆ for OR | p-Value | |
| What is your age? | |||||
| 16–25 | 21 | 21 | Ref | ||
| 26–35 | 42 | 42 | 1.73 | 0.46–6.48 | 0.418 |
| 36 and above | 37 | 34 | 2.10 | 0.55–8.09 | 0.280 |
| What education level have you completed? | |||||
| Up to Year 11 | 35 | 35 | Ref | ||
| Year 12 | 20 | 20 | 0.85 | 0.23–3.07 | 0.800 |
| Current student at university/TAFE/Appr | 19 | 19 | 1.76 | 0.47–6.56 | 0.401 |
| Trade certificate/University degree | 26 | 26 | 1.45 | 0.46–4.58 | 0.530 |
| Have you ever used any type stop-smoking medications? | |||||
| No | 63 | 63 | Ref | ||
| Yes | 37 | 37 | 0.56 | 0.21–1.47 | 0.235 |
| Do you use an Aboriginal Health Service(s)? | |||||
| No | 23 | 23 | Ref | ||
| Yes | 77 | 73 | 4.54 | 1.29–15.95 | 0.018 |
| What is your post code? (Remoteness) | |||||
| Regional/remote | 45 | 45 | Ref | ||
| Urban | 55 | 55 | 0.33 | 0.13–0.84 | 0.020 |
| Sl | Major Themes | Subthemes | Counts |
|---|---|---|---|
| 1 | Motivations for changes in the smoking behaviour | Quitting soon after becoming aware of pregnancy with strong intent to protect unborn child | 9 |
| Health of unborn child | 17 | ||
| Morning sickness making smoking not pleasurable and even difficult | 16 | ||
| 2 | The level of behavioural change may vary | Reduction in consumption | 18 |
| Complete cessation through to term | 28 | ||
| 3 | The experience of change is diverse, either difficult or easy | Giving up smoking can be either difficult or stressful for some Aboriginal women during pregnancy | 34 |
| Some Aboriginal women may find quitting smoking easy during pregnancy | 18 | ||
| 4 | Experience of change evolves over time and in different pregnancies | Change in smoking behaviour over the course of a pregnancy | 13 |
| Smoking and quitting experience may vary in different pregnancies | 12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rahman, T.; Baker, A.L.; Gould, G.S.; Palazzi, K.; Lambkin, D.; Kennedy, M. Factors Associated with Smoke-Free Pregnancy among Aboriginal and Torres Strait Women and Their Experience of Quitting Smoking in Pregnancy: A Mixed Method Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 11240. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111240
Rahman T, Baker AL, Gould GS, Palazzi K, Lambkin D, Kennedy M. Factors Associated with Smoke-Free Pregnancy among Aboriginal and Torres Strait Women and Their Experience of Quitting Smoking in Pregnancy: A Mixed Method Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(21):11240. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111240
Chicago/Turabian StyleRahman, Tabassum, Amanda L. Baker, Gillian S. Gould, Kerrin Palazzi, David Lambkin, and Michelle Kennedy. 2021. "Factors Associated with Smoke-Free Pregnancy among Aboriginal and Torres Strait Women and Their Experience of Quitting Smoking in Pregnancy: A Mixed Method Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 21: 11240. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph182111240