A Clinical-Epidemiological and Geospatial Study of Tuberculosis in a Neglected Area in the Amazonian Region Highlights the Urgent Need for Control Measures

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
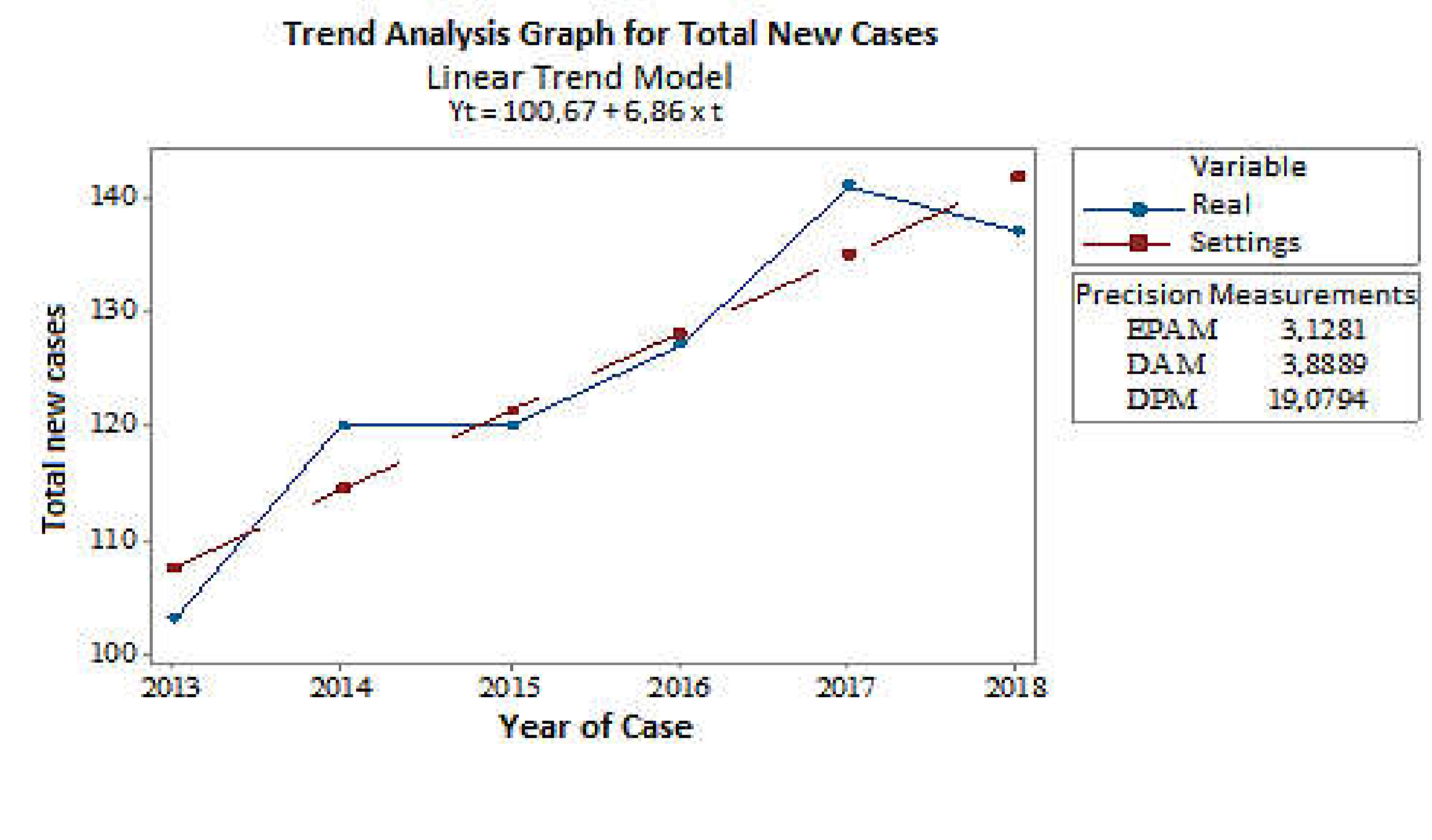
3.1. Analysis of the Trend of New Cases
3.2. Description of Clinical and Epidemiological Data
3.3. Description of New Tuberculosis Cases According to the Tuberculosis Culture Results, HIV Diagnosis, and Closure Situation
3.4. Analysis of MDR-TB Cases: Relapse and Re-Admission
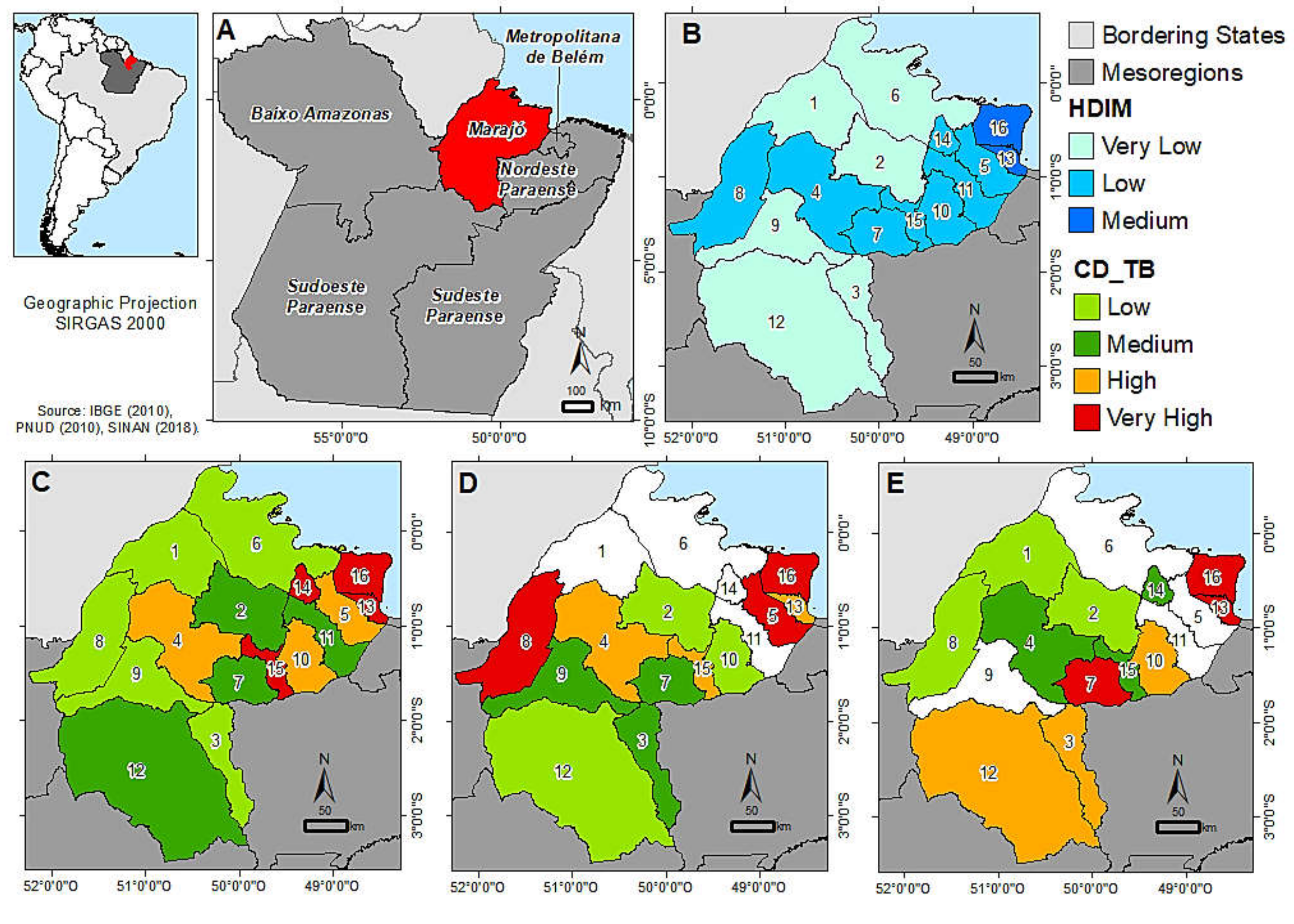
3.5. Geospatial Distribution of Cases by Municipality
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report 2019; World Health Organization: Geneva, Switzerland, 2019; Available online: https://www.who.int/tb/publications/global_report/en/ (accessed on 24 June 2020).
- Crispim, J.A.; Touso, M.M.; Yamamura, M.; Popolin, M.P.; Garcia, M.C.C.; Santos, C.B.; Palha, P.F.; Arcênio, R.A. Cultural adaptation of the Tuberculosis-related stigma scale to Brazil. Cienc. Saude Colet. 2016, 21, 2233. Available online: https://www.scielo.br/pdf/csc/v21n7/en_1413-8123-csc-21-07-2233.pdf (accessed on 24 June 2020). [CrossRef] [Green Version]
- Ministry of Health, Brazil. Manual de Recomendações Para o Controle da Tuberculose no Brasil; Ministry of Health: Brasilia, Brazil, 2011. Available online: http://www.saude.gov.br/images/pdf/2015/junho/30/MANUAL-DE-RECOMENDACOES-PARA-O-CONTROLE-DA-TUBERCULOSE-NO-BRASIL.pdf (accessed on 23 June 2020).
- Barreira, D. The challenges to eliminating tuberculosis in Brazil. Epidemiol. Serv. Saude 2018, 27, e00100009. Available online: https://www.scielo.br/pdf/ress/v27n1/en_2237-9622-ress-27-01-e00100009.pdf (accessed on 23 June 2020).
- Malik, A.A.; Safdar, N.; Chandir, S.; Khan, U.; Khowaja, S.; Riaz, N.; Manjar, R.; Jaswal, M.; Khan, A.J.; Hussain, H. Tuberculosis control and care in the era of COVID-19. Health Policy Plan. 2020, 1130. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health, Brazil. Health Surveillance Secretariat. Panorama da Tuberculose no Brasil: A Mortalidade em Números; Ministério da Saúde: Brasilia, Brazil, 2016. Available online: http://bvsms.saude.gov.br/bvs/publicacoes/panorama_tuberculose_brasil_mortalidade.pdf (accessed on 25 June 2020).
- World Health Organization. The End TB Strategy; World Health Organization: Geneva, Switzerland, 2015; p. 20. Available online: https://www.who.int/tb/End_TB_brochure.pdf?ua=1 (accessed on 23 June 2020).
- World Health Organization. The Paradigm: Global Plan to End TB: 2018–2022; World Health Organization: Geneva, Switzerland, 2019; Available online: http://www.stoptb.org/assets/documents/global/plan/GPR_2018-2022_Digital.pdf (accessed on 24 June 2020).
- Ministry of Health, Brazil. Health Surveillance Secretariat. Brasil Livre da Tuberculose: Plano Nacional pelo Fim da Tuberculose como Problema de Saúde Pública 2017. Available online: http://saude.pi.gov.br/uploads/warning_document/file/403/Plano_Nacional_Pelo_Fim_da_Tuberculose__1_.pdf (accessed on 23 June 2020).
- Solovic, I.; Abubakar, I.; Sotgiu, G.; Dara, M.; Goletti, D.; Duarte, R.; Aliberti, S.; Benedictis, F.M.; Ward, B.; Teixeira, V; et al. Standard operating procedures for tuberculosis care. Eur. Respir. J. 2017, 49, 1. Available online: https://erj.ersjournals.com/content/49/6 (accessed on 25 June 2020). [CrossRef] [PubMed] [Green Version]
- Ministry of Health, Brazil, Health Surveillance Secretariat. Boletim Epidemiológico da Tuberculose. 2020. Available online: https://www.saude.gov.br/images/pdf/2020/marco/24/Boletim-tuberculose-2020-marcas--1-.pdf (accessed on 20 June 2020).
- Ministry of Health, Brazil. Boletim Epdeimiológico-Brasil Livre da Tuberculose: Evolução dos Cenários Epidemiológicos e Operacionais da Doença. 2019; 50. Available online: https://portalarquivos2.saude.gov.br/images/pdf/2019/marco/22/2019-009.pdf (accessed on 20 June 2020).
- State Secretariat of Health of Pará—SESPA. Plano Estadual de Saúde 2016–2019; Secretaria do Estado do Pará: Belem, Brazil, 2016; Available online: https://www.conass.org.br/pdf/planos-estaduais-de-saude/PA_Plano-estadual-saude-2016-2019.pdf (accessed on 23 June 2020).
- Brazilian Institute of Geography and Statistics—IBGE. Cidades. 2010. Available online: https://cidades.ibge.gov.br/ (accessed on 26 June 2020).
- Amazon Foundation for Support to Studies and Research—FAPESPA. Relatório sobre a Vulnerabilidade Social no Estado do Pará; Amazon Foundation for Support to Studies and Research—FAPESPA: Belem, Brazil, 2015. [Google Scholar]
- Boulhosa, M.S. Turismo, desenvolvimento e sustentabilidade na ilha do Marajó. Pap. NAEA 2019, 28, 454. [Google Scholar] [CrossRef]
- Sanches, P.M.A.; Campos, J.A.D.B. Geoprocessing as a tool of Health in Brazil. Rev. UNINGÁ 2010, 26, 189–197. Available online: http://revista.uninga.br/index.php/uninga/article/view/920 (accessed on 27 June 2020).
- PNUD, Programa das Nações Unidas para o Desenvolvimento. Ranking IDHM e IDH. 2010. Available online: https://www.br.undp.org/content/brazil/pt/home/idh0/rankings/idhm-uf-2010.html (accessed on 3 July 2020).
- Santos, M.L.; Coeli, C.M.; Batista, J.D.L.; Braga, M.C.; Albuquerque, M.F.P.M. Factors associated with underreporting of tuberculosis based on data from Sinan Aids and Sinan TB. Rev. Bras. Epidemiol. 2018, 21, e180019. Available online: https://www.scielo.br/pdf/rbepid/v21/en_1980-5497-rbepid-21-e180019.pdf (accessed on 1 July 2020).
- Carvalho, C.N.; Dourado, I.; Bierrenbach, A.L. Underreporting of the tuberculosis and AIDS comorbidity: An application of the linkage method. Rev. Saúde Pública 2011, 45, 548–555. Available online: https://www.scielo.br/pdf/rsp/v45n3/en_2326.pdf (accessed on 28 June 2020). [CrossRef] [Green Version]
- MacNeil, A.; Glaziou, P.; Sismanidis, C.; Maloney, S.; Floyd, K. Global Epidemiology of Tuberculosis and Progress Toward Achieving Global Targets—2017. Morb. Mortal. Wkly. Rep. 2019, 68, 263. Available online: https://www.cdc.gov/mmwr/volumes/68/wr/mm6811a3.htm (accessed on 29 June 2020). [CrossRef] [Green Version]
- Pinto, P.F.P.S.; Silveira, C.; Rujula, M.J.P.; Neto, F.C.; Ribeiro, M.C.S.A. Epidemiological profile of tuberculosis in São Paulo municipality from 2006 to 2013. Rev. Bras. Epidemiol. 2017, 20, 549. Available online: https://www.scielo.br/pdf/rbepid/v20n3/en_1980-5497-rbepid-20-03-549.pdf (accessed on 5 July 2020). [CrossRef] [Green Version]
- Santos, A.N.; Santos, M.R.; Gonçalves, L.V.P. Epidemiological profile of tuberculosis in a Bahia MicroRegion (2008–2018). Rev. Bras. Saúde Func. 2020, 10, 29. Available online: http://www.seer-adventista.com.br/ojs3/index.php/RBSF/article/view/1234 (accessed on 10 July 2020).
- Conceição, E.M.; Guimarães, A.E.S.; Lopes, M.L.; Furlaneto, I.P.; Rodrigues, Y.C.R.; Conceição, M.L.; Barros, W.A.; Cardoso, N.C.; Sharma, A.; Lima, L.N.G.C.; et al. Analysis of potential household transmission events of tuberculosis in the city of Belem, Brazil. Tuberculosis 2018, 133, 125. Available online: https://0-www-sciencedirect-com.brum.beds.ac.uk/science/article/abs/pii/S1472979218300271 (accessed on 6 July 2020).
- Macedo, J.L.; Oliveira, A.S.S.S.; Pereira, I.C.; Assunção, M.J.S.M. Epidemiological profile of tuberculosis in a Municipality of Maranhão. ReonFacema 2017, 3, 699. Available online: https://pdfs.semanticscholar.org/8cf5/cfafcfa9c3eb15ede06abd7f857ead65783b.pdf (accessed on 28 June 2020).
- Pereira, F.A.; Zanin, L.; Flório, F.M. Clinical and epidemiological profile of patients with tuberculosis cared at a municipal health center in Belém, Pará State, Brazil. Res. Soc. Dev. 2020, 9, e908986212. Available online: https://rsdjournal.org/index.php/rsd/article/view/6212 (accessed on 24 June 2020). [CrossRef]
- Freitas, W.M.T.M.; Santos, C.C.; Silva, M.M.; Rocha, G.A. Perfil clínico-epidemiológico de pacientes portadores de tuberculose atendidos em uma unidade municipal de saúde de Belém, Estado do Pará, Brasil. Rev. Pan-Amaz. Saude 2016, 7, 45. Available online: http://scielo.iec.gov.br/scielo.php?script=sci_arttext&pid=S2176-62232016000200045&lng=pt&nrm=iso (accessed on 24 June 2020).
- Suarez, I.; Fünger, S.M.; Kröger, S.; Rademacher, J.; Fätkenheuer, G.; Rybniker, J. The Diagnosis and Treatment of Tuberculosis. Dtsch. Ärzteblatt Int. 2019, 116, 729. Available online: https://www.aerzteblatt.de/int/archive/article/210460/The-diagnosis-and-treatment-of-tuberculosis (accessed on 27 June 2020).
- Brazil, Ministry of Health, Health Surveillance Secretariat. Recomendações para o Manejo da Coinfecção TB-HIV em Serviços de Atenção Especializada a Pessoas Vivendo com HIV/AIDS; Ministério da Saúde: Brasilia, Brazil, 2013. Available online: http://bvsms.saude.gov.br/bvs/publicacoes/recomendacoes_manejo_coinfeccao_tb_hiv.pdf (accessed on 23 June 2020).
- Ruffino-Neto, A. Recurrence of tuberculosis. J. Bras. Pneumol. 2007, 33, xxvii. Available online: https://cdn.publisher.gn1.link/jornaldepneumologia.com.br/pdf/2007_33_5_1_english.pdf (accessed on 28 June 2020).
- Rodrigues, I.C.; Vendramini, S.H.F.; Ponce, M.A.Z.; Ruffino-Neto, A.; Souza, N.G.; Chiarvalloti-Neto, F.; Santos, M.L.S.G.; Wysocki, A.D. Recidiva da Tuberculose: Fatores associados em um Grupo de Vigilância Epidemiológica de São Paulo. Rev. Eletronica Enferm. 2017, 19, 1. Available online: https://www.revistas.ufg.br/fen/article/view/42694/22902 (accessed on 29 June 2020). [CrossRef] [Green Version]
- Costa, R.R.; Silva, M.R.; Gonçalves, I.C. Laboratory diagnosis of tuberculosis: Literature review. Rev. Med. Minas Gerais 2018, 28, e-S280525. [Google Scholar] [CrossRef]
- Mendes, A.M.; Bastos, J.L.; Bresan, D.; Leite, M.S. Epidemiologic situation of tuberculosis in Rio Grande do Sul: An analysis about Sinan’s data between 2003 and 2012 focusing on indigenous peoples. Rev. Bras. Epidemiol. 2016, 19, 658. Available online: https://www.scielo.br/pdf/rbepid/v19n3/en_1980-5497-rbepid-19-03-00658.pdf (accessed on 27 June 2020). [CrossRef] [Green Version]
- World Health Organization. Tuberculosis; World Health Organization: Geneva, 2010; Available online: https://www.who.int/tb/features_archive/new_rapid_test/en/ (accessed on 20 June 2020).
- Ministry of Health, Brazil. Health Surveillance Secretariat. Ofício Circular Nº 6/2019/CGDR/.DCCI/SVS/MS. In Revogação da Nota Técnica Nº 22/2018—CGPNCT/DEVIT/MS sobre a Indisponibilidade Temporária da Rifampicina 300 mg Cápsula e Rifampicina Suspensão Oral 20 mg/ml para o Tratamento da Infecção Latente Pelo Mycobacterium tuberculosis.; 2019. Available online: https://central3.to.gov.br/arquivo/472141/ (accessed on 20 August 2020).
- Furlaneto, I.P.; Conceição, L.M.; Conceição, E.C.; Lopes, M.L.; Rodrigues, Y.C.; Macelino, B.R.; Gomes, H.M.; Suffys, P.N.; Guimaraes, R.J.P.S.; Silva, M.G.; et al. Molecular epidemiology of mycobacteria among herds in Marajó Island, Brazil, reveals strains genetically related and potential zoonotic risk of clinical relevance. Infect. Genet. Evol. 2020, 77, 104044. Available online: https://pubmed.ncbi.nlm.nih.gov/31634644/ (accessed on 20 August 2020). [CrossRef] [PubMed]
- Conceição, L.M.; Conceição, E.C.; Furlaneto, I.P.; Silva, S.P.; Guimarães, A.E.S.; Gomes, P.; Boschiroli, M.L.; Michelet, L.; Kohl, T.A.; Kranzer, K.; et al. Phylogenomic Perspective on a Unique Mycobacterium bovis Clade Dominating Bovine Tuberculosis Infections among Cattle and Buffalos in Northern Brazil. Sci. Rep. 2020, 10, 1747. Available online: https://pubmed.ncbi.nlm.nih.gov/32019968/ (accessed on 20 August 2020).
- Lima, V.M.; Costa, S.M.F.; Mendes, J.A.; Montóia, G.R.M. The Public Health Challenge in Small Cities of the Amazon Region: A Study of Ponta De Pedras, Marajó Island—Para. Rev. Univap 2012, 18. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Epidemiological Characterization (New Cases) | Number | % | p-Value (1) |
|---|---|---|---|
| Age Range (year) | |||
| From <1 | 09 | 1% | <0.001 * |
| From 1 to 19 | 106 | 14% | |
| From 20 to 39 | 334 | 45% | |
| From 40 to 59 | 190 | 25% | |
| From ≥60 | 110 | 15% | |
| Total | 749 | 100% | |
| Sex | |||
| Female | 262 | 35% | <0.001 * |
| Male | 487 | 65% | |
| Total | 749 | 100% | |
| Total | 749 | 100% | <0.001 * |
| Race/Skin Color | |||
| White | 65 | 9% | <0.001 * |
| Black | 57 | 8% | |
| “Brown” (“Parda”) | 611 | 82% | |
| Yellow | 5 | 1% | |
| Indigenous | 1 | 0% | |
| Ignored | 10 | 1% | |
| Total | 749 | 100% | |
| Education | |||
| Illiterate | 76 | 10% | 0.021 * |
| Incomplete elementary school (1th to 4th series) | 201 | 27% | |
| Complete elementary school (old “1 degree”)—4th Series | 36 | 5% | |
| Incomplete elementary school (old “1 degree”)—5th to 8th Series | 124 | 17% | |
| Complete elementary school (old “1 degree”) | 35 | 5% | |
| Incomplete high school (old “2 degree”) | 59 | 8% | |
| Complete high school (old “2 degree”) | 53 | 7% | |
| Incomplete higher education | 7 | 1% | |
| Complete higher education | 12 | 2% | |
| Ignored | 123 | 16% | |
| Not applicable ** | 23 | 3% | |
| Total | 749 | 100% | |
| Clinical Characteristics | |||
| Pulmonary | 686 | 92% | |
| Extrapulmonary | 43 | 5.8% | |
| Pulmonary + Extrapulmonary | 19 | 2% | <0.001 * |
| Ignored | 1 | 0.2% | |
| Total | 749 | 100% | |
| Diseases (New Cases) | Number | % | p-Value (1) | |
|---|---|---|---|---|
| Diseases and Associated Grievances (Mental Disease) | 1. Yes | 16 | 2.1% | 0.001 * |
| 2. No | 664 | 88.8% | ||
| 9. Ignored | 32 | 4.3% | ||
| No information | 36 | 4.8% | ||
| Diseases and Associated Grievances (Others) | 1. Yes | 42 | 5.6% | 0.031 * |
| 2. No | 503 | 67.2% | ||
| 9. Ignored | 104 | 13.9% | ||
| No information | 99 | 13.2% | ||
| Diseases and Associated Grievances | Not applied (2) | 707 | 94.5% | 0.031 * |
| Asma | 1 | 0.1% | ||
| Amygdala Cancer | 1 | 0.1% | ||
| Breast cancer | 1 | 0.1% | ||
| Cardiopathy | 2 | 0.3% | ||
| TB contact | 1 | 0.1% | ||
| Insanity | 1 | 0.1% | ||
| Depression | 1 | 0.1% | ||
| Illicit drugs | 3 | 0.4% | ||
| Epilepsy | 1 | 0.1% | ||
| Ex-Smoker | 1 | 0.1% | ||
| Pulmonary Fibrosis | 1 | 0.1% | ||
| Smoking | 1 | 0.1% | ||
| HAS | 13 | 1.7% | ||
| Hepatitis | 3 | 0.4% | ||
| LTA | 1 | 0.1% | ||
| Pneumonia | 1 | 0.1% | ||
| Chronic Kidney | 1 | 0.1% | ||
| Syphilis | 2 | 0.3% | ||
| Down Syndrome | 2 | 0.3% | ||
| Smoking | 2 | 0.3% | ||
| VDRL+ | 1 | 0.1% | ||
| Culture/HIV/Closing (New Cases) | Number | % | p-Value (1) | |
|---|---|---|---|---|
| Culture | 1. Positive | 64 | 8.6% | 0.006 * |
| 2. Negative | 17 | 2.3% | ||
| 3. Waiting result | 15 | 2.0% | ||
| 4. No performed | 652 | 87.2% | ||
| HIV | 1. Positive | 40 | 5.3% | 0.001 * |
| 2. Negative | 384 | 51.3% | ||
| 3. Waiting result | 29 | 3.9% | ||
| 4. No performed | 295 | 39.4% | ||
| Closing Situation | 1. Cure | 499 | 66.7% | <0.001 * |
| 10. Primary Abandonment | 2 | 0.3% | ||
| 2. Abandonment | 86 | 11.5% | ||
| 3. Death by TB | 23 | 3.1% | ||
| 4. Death from other causes | 27 | 3.6% | ||
| 5. Transferred | 64 | 8.5% | ||
| 6. Diagnostic Change | 3 | 0.4% | ||
| 7. Tuberculosis drug resistance | 8 | 1.1% | ||
| 8. Scheme Change | 3 | 0.4% | ||
| 9. Failure | 2 | 0.3% | ||
| No information | 31 | 4.1% | ||
| Start Date of Treatment | Sex | Age | Municipality of Residence | Drug Resistance Profile | Type of Resistance | Pulmonary Type | Outcome | HIV Status |
|---|---|---|---|---|---|---|---|---|
| 30 January 2013 | M | 47 | Portel | MDR | Acquired | Bilateral cavity | Cured | No |
| 6 August 2013 | M | 45 | Santa Cruz do Arari | MDR | Acquired | Bilateral cavity | Failure | Yes |
| 21 March 2016 | F | 24 | Breves | MDR | Acquired | Unilateral c cavity | Failure | No |
| 30 December 2016 | M | 29 | Ponta de Pedras | MDR | Primary | Unilateral non-cavitary | Abandon | Yes |
| 4 January 2017 | F | 25 | Breves | MDR | Acquired | Unilateral cavity | Cured | No |
| 1 December 2017 | M | 28 | Cachoeira do Arari | Rifampicin | Acquired | Unilateral c cavity | Failure | No |
| 29 March 2018 | M | 20 | Soure | MDR | Acquired | Bilateral non-cavity | Cured | No |
| 28 May 2018 | M | 28 | Cachoeira do Arari | MDR | Acquired | Unilateral cavity | In treatment | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mesquita, C.R.; Conceição, E.C.; Monteiro, L.H.M.T.; da Silva, O.M.; Lima, L.N.G.C.; de Oliveira, R.A.C.; de Brito, A.C.; Guimarães, R.J.d.P.S.e.; Lima, K.V.B. A Clinical-Epidemiological and Geospatial Study of Tuberculosis in a Neglected Area in the Amazonian Region Highlights the Urgent Need for Control Measures. Int. J. Environ. Res. Public Health 2021, 18, 1335. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031335
Mesquita CR, Conceição EC, Monteiro LHMT, da Silva OM, Lima LNGC, de Oliveira RAC, de Brito AC, Guimarães RJdPSe, Lima KVB. A Clinical-Epidemiological and Geospatial Study of Tuberculosis in a Neglected Area in the Amazonian Region Highlights the Urgent Need for Control Measures. International Journal of Environmental Research and Public Health. 2021; 18(3):1335. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031335
Chicago/Turabian StyleMesquita, Cristal Ribeiro, Emilyn Costa Conceição, Lúcia Helena Martins Tavares Monteiro, Odinea Maria da Silva, Luana Nepomuceno Gondim Costa Lima, Rafael Aleixo Coelho de Oliveira, Artemir Coelho de Brito, Ricardo José de Paula Souza e Guimarães, and Karla Valéria Batista Lima. 2021. "A Clinical-Epidemiological and Geospatial Study of Tuberculosis in a Neglected Area in the Amazonian Region Highlights the Urgent Need for Control Measures" International Journal of Environmental Research and Public Health 18, no. 3: 1335. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18031335