
Irregular Work Hours and the Risk of Sleep Disturbance Among Korean Service Workers Required to Suppress Emotion


Abstract
:1. Introduction
2. Materials and Methods
2.1. Work Regularity
2.2. Emotion Suppression
2.3. Sleep Disturbance
2.4. Covariates
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Costa, G. Shift work and occupational medicine: An overview. Occup. Med. 2003, 53, 83–88. [Google Scholar] [CrossRef] [Green Version]
- Horowitz, T.S.; Tanigawa, T. Circadian-based new technologies for night workers. Ind. Health 2002, 40, 223–236. [Google Scholar] [CrossRef]
- Kim, W.; Kim, T.H.; Lee, T.H.; Choi, J.W.; Park, E.C. The impact of shift and night work on health related quality of life of working women: Findings from the korea health panel. Health Qual. Life Outcomes 2016, 14, 162. [Google Scholar] [CrossRef] [Green Version]
- Books, C.; Coody, L.C.; Kauffman, R.; Abraham, S. Night shift work and its health effects on nurses. Health Care Manag. 2020, 39, 122–127. [Google Scholar] [CrossRef]
- Schernhammer, E.S.; Laden, F.; Speizer, F.E.; Willett, W.C.; Hunter, D.J.; Kawachi, I.; Fuchs, C.S.; Colditz, G.A. Night-shift work and risk of colorectal cancer in the nurses’ health study. J. Natl. Cancer Inst. 2003, 95, 825–828. [Google Scholar] [CrossRef] [Green Version]
- Pan, A.; Schernhammer, E.S.; Sun, Q.; Hu, F.B. Rotating night shift work and risk of type 2 diabetes: Two prospective cohort studies in women. PLoS Med. 2011, 8, e1001141. [Google Scholar] [CrossRef] [Green Version]
- Fukuda, S.; Koyama, H.; Kondo, K.; Fujii, H.; Hirayama, Y.; Tabata, T.; Okamura, M.; Yamakawa, T.; Okada, S.; Hirata, S.; et al. Effects of nutritional supplementation on fatigue, and autonomic and immune dysfunction in patients with end-stage renal disease: A randomized, double-blind, placebo-controlled, multicenter trial. PLoS ONE 2015, 10, e0119578. [Google Scholar] [CrossRef] [Green Version]
- Kecklund, G.; Axelsson, J. Health consequences of shift work and insufficient sleep. BMJ 2016, 355, i5210. [Google Scholar] [CrossRef]
- Frost, P.; Kolstad, H.A.; Bonde, J.P. Shift work and the risk of ischemic heart disease—A systematic review of the epidemiologic evidence. Scand. J. Work Environ. Health 2009, 35, 163–179. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.S.; Armstrong, M.E.; Cairns, B.J.; Key, T.J.; Travis, R.C. Shift work and chronic disease: The epidemiological evidence. Occup. Med. 2011, 61, 78–89. [Google Scholar] [CrossRef] [Green Version]
- Wang, A.; Arah, O.A.; Kauhanen, J.; Krause, N. Work schedules and 11-year progression of carotid atherosclerosis in middle-aged finnish men. Am. J. Ind. Med. 2015, 58, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ye, H.H.; Jeong, J.U.; Jeon, M.J.; Sakong, J. The association between shift work and the metabolic syndrome in female workers. Ann. Occup. Environ. Med. 2013, 25, 33. [Google Scholar] [CrossRef] [Green Version]
- Magrini, A.; Pietroiusti, A.; Coppeta, L.; Babbucci, A.; Barnaba, E.; Papadia, C.; Iannaccone, U.; Boscolo, P.; Bergamaschi, E.; Bergamaschi, A. Shift work and autoimmune thyroid disorders. Int. J. Immunopathol. Pharmacol. 2006, 19, 31–36. [Google Scholar]
- Vallieres, A.; Azaiez, A.; Moreau, V.; LeBlanc, M.; Morin, C.M. Insomnia in shift work. Sleep Med. 2014, 15, 1440–1448. [Google Scholar] [CrossRef] [PubMed]
- Ganesan, S.; Magee, M.; Stone, J.E.; Mulhall, M.D.; Collins, A.; Howard, M.E.; Lockley, S.W.; Rajaratnam, S.M.W.; Sletten, T.L. The impact of shift work on sleep, alertness and performance in healthcare workers. Sci. Rep. 2019, 9, 4635. [Google Scholar] [CrossRef]
- Rajaratnam, S.M.; Howard, M.E.; Grunstein, R.R. Sleep loss and circadian disruption in shift work: Health burden and management. Med. J. Aust. 2013, 199, S11–S15. [Google Scholar] [CrossRef]
- Utsugi, M.; Saijo, Y.; Yoshioka, E.; Horikawa, N.; Sato, T.; Gong, Y.; Kishi, R. Relationships of occupational stress to insomnia and short sleep in japanese workers. Sleep 2005, 28, 728–735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.C.; Kim, B.K.; Min, K.B.; Min, J.Y.; Hwang, S.H.; Park, S.G. Association between job stress and insomnia in korean workers. J. Occup. Health 2011, 53, 164–174. [Google Scholar] [CrossRef] [Green Version]
- Lim, S.S.; Lee, W.; Hong, K.; Jeung, D.; Chang, S.J.; Yoon, J.H. Facing complaining customer and suppressed emotion at worksite related to sleep disturbance in korea. J. Korean Med. Sci. 2016, 31, 1696–1702. [Google Scholar] [CrossRef] [Green Version]
- Yun, S.; Lim, S.S.; Kim, J.; Kim, Y.K.; Won, J.U.; Yoon, J.H. The role of customer service manual on workplace emotional burden in nationwide cross sectional study. Ann. Occup. Environ. Med. 2019, 31, 5. [Google Scholar] [CrossRef] [PubMed]
- Iacovides, A.; Fountoulakis, K.N.; Kaprinis, S.; Kaprinis, G. The relationship between job stress, burnout and clinical depression. J. Affect. Disord. 2003, 75, 209–221. [Google Scholar] [CrossRef]
- Lee, W.T.; Lim, S.S.; Kim, J.; Yun, S.; Yoon, J.H.; Won, J.U. Work schedule irregularity and the risk of work-related injury among korean manual workers. Int. J. Environ. Res. Public Health 2020, 17, 7617. [Google Scholar] [CrossRef] [PubMed]
- Ohayon, M.M.; Hong, S.C. Prevalence of insomnia and associated factors in south korea. J. Psychosom. Res. 2002, 53, 593–600. [Google Scholar] [CrossRef]
- Cho, Y.W.; Shin, W.C.; Yun, C.H.; Hong, S.B.; Kim, J.; Earley, C.J. Epidemiology of insomnia in korean adults: Prevalence and associated factors. J. Clin. Neurol. 2009, 5, 20–23. [Google Scholar] [CrossRef] [Green Version]
- Nomura, K.; Yamaoka, K.; Nakao, M.; Yano, E. Social determinants of self-reported sleep problems in South Korea and Taiwan. J. Psychosom. Res. 2010, 69, 435–440. [Google Scholar] [CrossRef]
- Smagula, S.F.; Stone, K.L.; Fabio, A.; Cauley, J.A. Risk factors for sleep disturbances in older adults: Evidence from prospective studies. Sleep Med. Rev. 2016, 25, 21–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saper, C.B.; Scammell, T.E.; Lu, J. Hypothalamic regulation of sleep and circadian rhythms. Nature 2005, 437, 1257–1263. [Google Scholar] [CrossRef] [PubMed]
- Deboer, T. Sleep homeostasis and the circadian clock: Do the circadian pacemaker and the sleep homeostat influence each others’ functioning? Neurobiol. Sleep Circadian Rhythm. 2018, 5, 68–77. [Google Scholar] [CrossRef]
- Weibel, L.; Brandenberger, G. Disturbances in hormonal profiles of night workers during their usual sleep and work times. J. Biol. Rhythm. 1998, 13, 202–208. [Google Scholar] [CrossRef]
- Morgan, E.; Schumm, L.P.; McClintock, M.; Waite, L.; Lauderdale, D.S. Sleep characteristics and daytime cortisol levels in older adults. Sleep 2017, 40, zsx043. [Google Scholar] [CrossRef] [Green Version]
- Boivin, D.B.; James, F.O. Light treatment and circadian adaptation to shift work. Ind. Health 2005, 43, 34–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewy, A.J.; Wehr, T.A.; Goodwin, F.K.; Newsome, D.A.; Markey, S.P. Light suppresses melatonin secretion in humans. Science 1980, 210, 1267–1269. [Google Scholar] [CrossRef]
- Boivin, D.B.; Tremblay, G.M.; James, F.O. Working on atypical schedules. Sleep Med. 2007, 8, 578–589. [Google Scholar] [CrossRef] [PubMed]
- Drake, C.L.; Roehrs, T.; Richardson, G.; Walsh, J.K.; Roth, T. Shift work sleep disorder: Prevalence and consequences beyond that of symptomatic day workers. Sleep 2004, 27, 1453–1462. [Google Scholar] [CrossRef] [PubMed]
- Nakashima, M.; Morikawa, Y.; Sakurai, M.; Nakamura, K.; Miura, K.; Ishizaki, M.; Kido, T.; Naruse, Y.; Suwazono, Y.; Nakagawa, H. Association between long working hours and sleep problems in white-collar workers. J. Sleep Res. 2011, 20, 110–116. [Google Scholar] [CrossRef]
- Bannai, A.; Ukawa, S.; Tamakoshi, A. Long working hours and sleep problems among public junior high school teachers in japan. J. Occup. Health 2015, 57, 457–464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hori, D.; Sasahara, S.; Oi, Y.; Doki, S.; Andrea, C.S.; Takahashi, T.; Shiraki, N.; Ikeda, T.; Ikeda, Y.; Kambayashi, T.; et al. Relationships between insomnia, long working hours, and long commuting time among public school teachers in japan: A nationwide cross-sectional diary study. Sleep Med. 2020, 75, 62–72. [Google Scholar] [CrossRef]
- Akerstedt, T.; Ingre, M.; Broman, J.E.; Kecklund, G. Disturbed sleep in shift workers, day workers, and insomniacs. Chronobiol. Int. 2008, 25, 333–348. [Google Scholar] [CrossRef]
- Jansen, N.W.; Kant, I.J.; van den Brandt, P.A. Need for recovery in the working population: Description and associations with fatigue and psychological distress. Int. J. Behav. Med. 2002, 9, 322–340. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, K.H.; Diestel, S. Differential effects of decision latitude and control on the job demands-strain relationship: A cross-sectional survey study among elderly care nursing staff. Int. J. Nurs. Stud. 2011, 48, 307–317. [Google Scholar] [CrossRef] [PubMed]
- Grandey, A.; Foo, S.C.; Groth, M.; Goodwin, R.E. Free to be you and me: A climate of authenticity alleviates burnout from emotional labor. J. Occup. Health Psychol. 2012, 17, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Plotsky, P.M.; Cunningham, E.T., Jr.; Widmaier, E.P. Catecholaminergic modulation of corticotropin-releasing factor and adrenocorticotropin secretion. Endocr. Rev. 1989, 10, 437–458. [Google Scholar] [CrossRef] [PubMed]
- Buckley, T.M.; Schatzberg, A.F. Review: On the interactions of the hypothalamic-pituitary-adrenal (hpa) axis and sleep: Normal hpa axis activity and circadian rhythm, exemplary sleep disorders. J. Clin. Endocr. Metab. 2005, 90, 3106–3114. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Parameters | Total | Moderate Sleep Disturbance, No. (%) | Severe Sleep Disturbance, No. (%) | ||||
|---|---|---|---|---|---|---|---|
| Yes | No | p-Value | Yes | No | p-Value | ||
| Gender | <0.001 | <0.001 | |||||
| Male | 6804 | 636 (9.3) | 6168 (90.7) | 193 (2.8) | 6611 (97.2) | ||
| Female | 11,042 | 1281 (11.6) | 9761 (88.4) | 419 (3.8) | 10,623 (96.2) | ||
| Age (years) | 0.0019 | 0.0966 | |||||
| <25 | 958 | 93 (9.7) | 865 (90.3) | 31 (3.2) | 927 (96.8) | ||
| 25–34 | 4029 | 419 (10.4) | 3610 (89.6) | 137 (3.4) | 3892 (96.6) | ||
| 35–44 | 5300 | 509 (9.6) | 4791 (90.4) | 156 (2.9) | 5144 (97.1) | ||
| 45–54 | 5041 | 573 (11.4) | 4468 (88.6) | 186 (3.7) | 4855 (96.3) | ||
| ≥55 | 2518 | 323 (12.8) | 2195 (87.2) | 102 (4.1) | 2416 (95.9) | ||
| Education Level | <0.001 | <0.001 | |||||
| <High school | 498 | 66 (13.1) | 432 (86.7) | 35 (7.0) | 463 (93.0) | ||
| <College | 9196 | 1081 (11.8) | 8115 (88.2) | 348 (3.8) | 8848 (96.2) | ||
| ≥College | 8152 | 770 (9.4) | 7382 (90.6) | 229 (2.8) | 7923 (97.2) | ||
| Weekly working hours | 0.0295 | <0.001 | |||||
| <40 | 2128 | 258 (12.1) | 1870 (87.9) | 121 (5.7) | 2007 (94.3) | ||
| 40–52 | 13,731 | 1430 (10.4) | 12,301 (89.6) | 428 (3.1) | 13,303 (96.9) | ||
| >52 | 1987 | 229 (11.5) | 1758 (88.5) | 63 (3.2) | 1924 (96.8) | ||
| Work size | 0.1655 | 0.1394 | |||||
| Small | 12,096 | 1336 (11.0) | 10,760 (89.0) | 456 (3.8) | 11,640 (96.2) | ||
| Medium | 2418 | 244 (10.1) | 2174 (89.9) | 65 (2.7) | 2353 (97.3) | ||
| Large | 3332 | 337 (10.1) | 2995 (89.9) | 91 (2.7) | 3241 (97.3) | ||
| Emotion suppression at work | <0.001 | <0.001 | |||||
| Rarely | 3023 | 209 (6.9) | 2814 (93.1) | 57 (1.9) | 2966 (98.1) | ||
| Sometimes | 6739 | 686 (10.2) | 6053 (89.8) | 197 (2.9) | 6542 (97.1) | ||
| Always | 8084 | 1022 (12.6) | 7062 (87.4) | 358 (4.4) | 7726 (95.6) | ||
| Work schedule * | <0.001 | <0.001 | |||||
| Regular | 14,225 | 1282 (9.0) | 12,943 (91.0) | 347 (2.4) | 13,878 (97.6) | ||
| Irregular | 3621 | 635 (17.5) | 2986 (82.5) | 265 (7.3) | 3356 (92.7) | ||
| Daily working hours | <0.001 | <0.001 | |||||
| Fixed | 15,189 | 1403 (9.2) | 13,786 (90.8) | 374 (2.5) | 14,815 (97.5) | ||
| Not fixed | 2657 | 514 (19.3) | 2143 (80.7) | 238 (9.0) | 2419 (91.0) | ||
| Weekly working days | <0.001 | <0.001 | |||||
| Fixed | 16,397 | 1576 (9.6) | 14,821 (90.4) | 432 (2.6) | 15,965 (97.4) | ||
| Not fixed | 1449 | 341 (23.5) | 1108 (76.5) | 180 (12.4) | 1269 (87.6) | ||
| Weekly work shift | <0.001 | <0.001 | |||||
| Fixed | 15,514 | 1493 (9.6) | 14,021 (90.4) | 418 (2.7) | 15,096 (97.3) | ||
| Not fixed | 2332 | 424 (18.2) | 1908 (81.8) | 194 (8.3) | 2138 (91.7) | ||
| Start and end time of each shift | <0.001 | <0.001 | |||||
| Fixed | 16,948 | 1677 (9.9) | 15,271 (90.1) | 482 (2.8) | 16,466 (97.2) | ||
| Not fixed | 898 | 240 (26.7) | 658 (73.3) | 130 (14.5) | 768 (85.5) | ||
| Total | 17,846 | 1917 (10.7) | 15,929 (89.3) | 612 (3.4) | 17,134 | ||
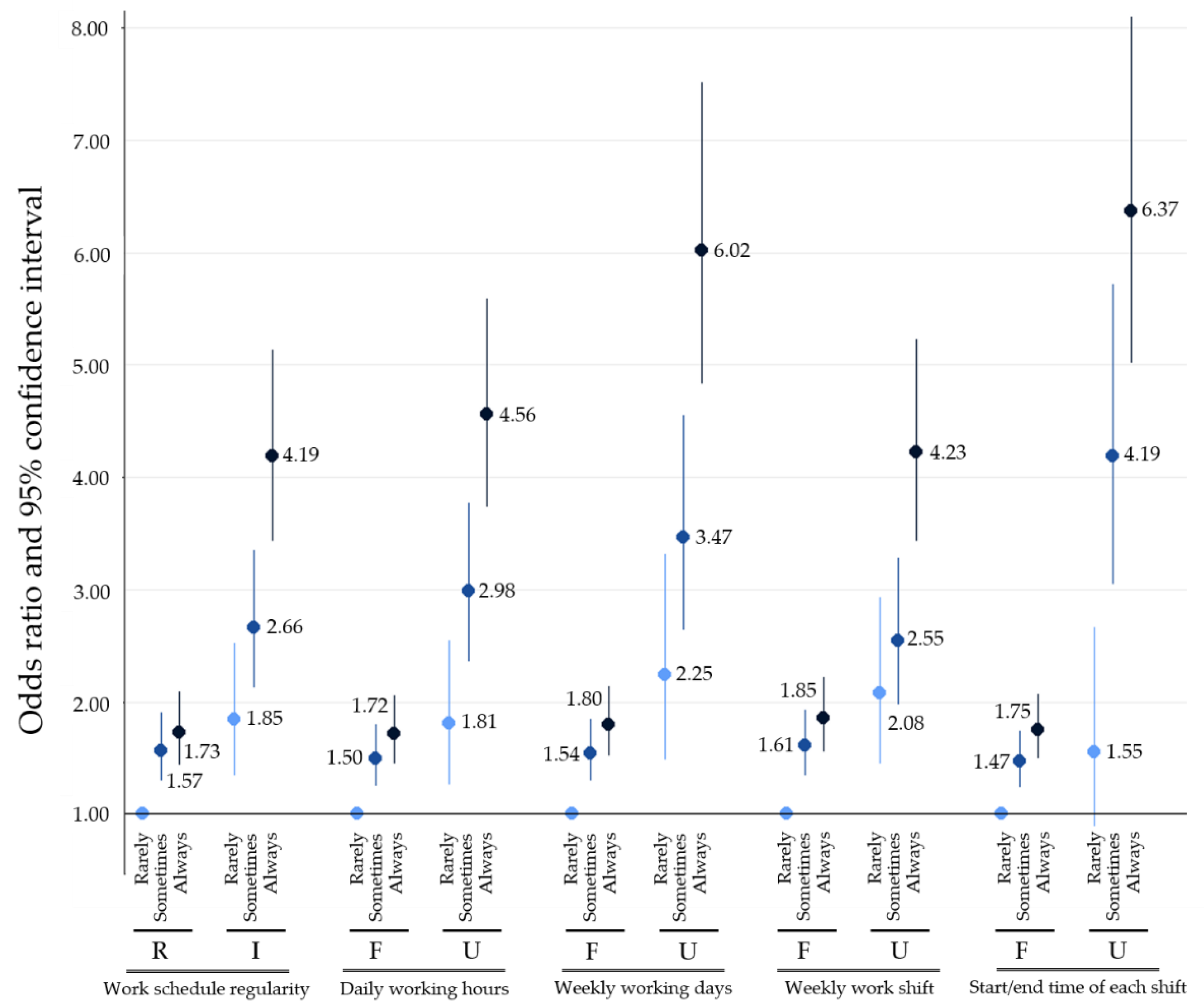
| Variables | Model A | Model B | Model C | |||
|---|---|---|---|---|---|---|
| ORs | 95% CIs | ORs | 95% CIs | ORs | 95% CIs | |
| Work schedule * | ||||||
| Regular | 1.00 | 1.00 | 1.00 | |||
| Irregular | 2.15 | 1.94–2.38 | 2.11 | 1.90–2.34 | 2.11 | 1.90–2.33 |
| Daily working hours | ||||||
| Fixed | 1.00 | 1.00 | 1.00 | |||
| Not fixed | 2.36 | 2.11–2.63 | 2.35 | 2.10–2.62 | 2.35 | 2.10–2.62 |
| Weekly working days | ||||||
| Fixed | 1.00 | 1.00 | 1.00 | |||
| Not fixed | 2.89 | 2.53–3.30 | 2.83 | 2.49–3.23 | 2.82 | 2.48–3.22 |
| Weekly work shift | ||||||
| Fixed | 1.00 | 1.00 | 1.00 | |||
| Not fixed | 2.09 | 1.85–2.35 | 2.04 | 1.81–2.30 | 2.03 | 1.80–2.29 |
| Start and end time of each shift | ||||||
| Fixed | 1.00 | 1.00 | 1.00 | |||
| Not fixed | 3.32 | 2.84–3.88 | 3.18 | 2.71–3.72 | 3.18 | 2.71–3.71 |
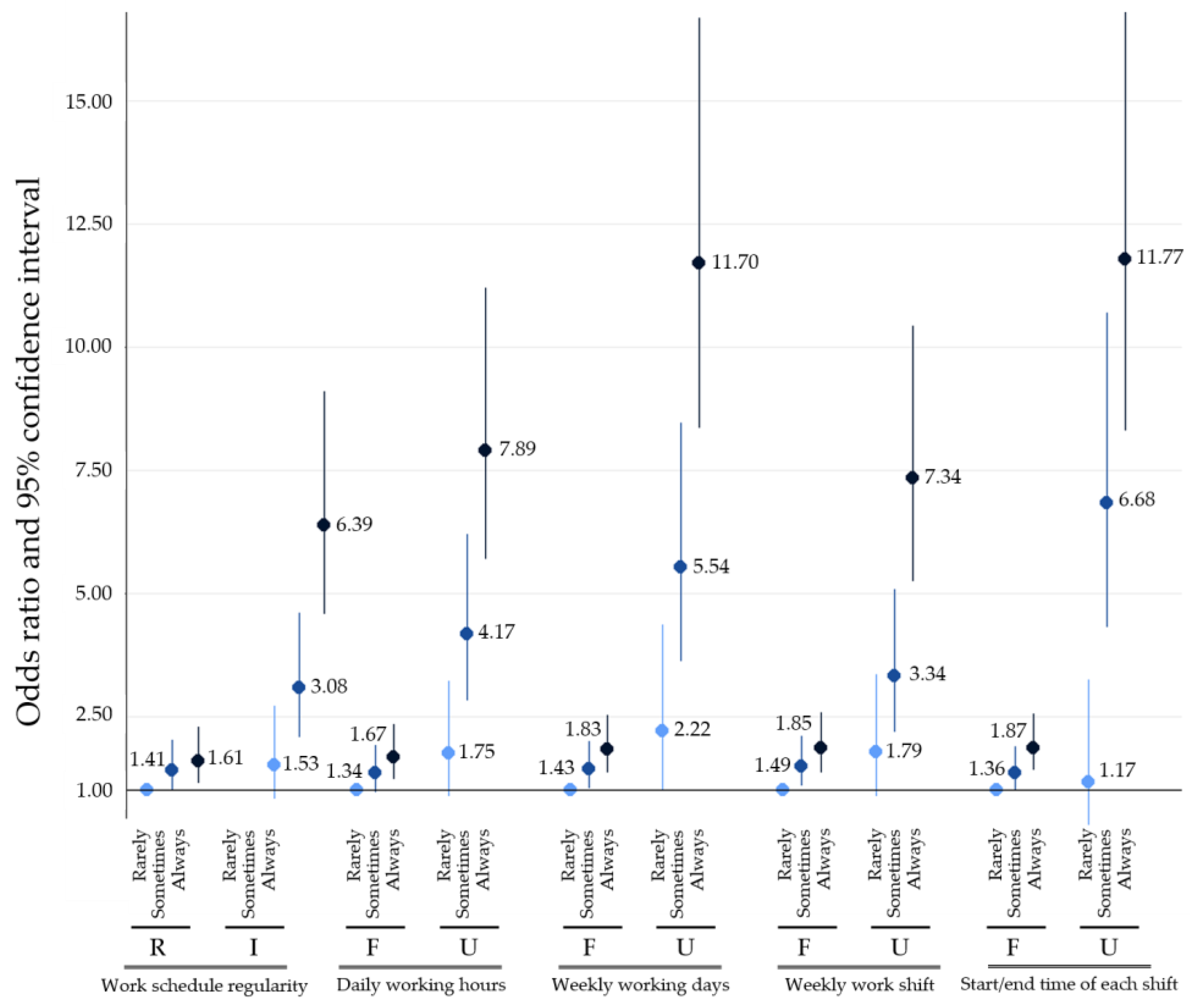
| Variables | Model A | Model B | Model C | |||
|---|---|---|---|---|---|---|
| ORs | 95% CIs | ORs | 95% CIs | ORs | 95% CIs | |
| Work schedule * | ||||||
| Regular | 1.00 | 1.00 | 1.00 | |||
| Irregular | 3.15 | 2.68–3.72 | 3.10 | 2.63–3.65 | 3.10 | 2.62–3.66 |
| Daily working hours | ||||||
| Fixed | 1.00 | 1.00 | 1.00 | |||
| Not fixed | 3.90 | 3.29–4.61 | 3.90 | 3.29–4.61 | 3.86 | 3.25–4.57 |
| Weekly working days | ||||||
| Fixed | 1.00 | 1.00 | 1.00 | |||
| Not fixed | 5.24 | 4.36–6.28 | 5.13 | 4.26–6.16 | 4.96 | 4.11–5.98 |
| Weekly work shift | ||||||
| Fixed | 1.00 | 1.00 | 1.00 | |||
| Not fixed | 3.28 | 2.74–3.90 | 3.21 | 2.69–3.83 | 3.21 | 2.68–3.83 |
| Start and end time of each shift | ||||||
| Fixed | 1.00 | 1.00 | 1.00 | |||
| Not fixed | 5.78 | 4.69–7.09 | 5.52 | 4.46–6.78 | 5.28 | 4.25–6.52 |
| Variables | Working Hours ≤52 h/Week | Working Hours >52 h/Week | ||
|---|---|---|---|---|
| ORs | 95% CIs | ORs | 95% CIs | |
| Work schedule * | ||||
| Regular | 1.00 | 1.00 | ||
| Irregular | 2.20 | 1.97–2.46 | 1.76 | 1.28–2.38 |
| Daily working hours | ||||
| Fixed | 1.00 | 1.00 | ||
| Not fixed | 2.40 | 2.13–2.70 | 2.04 | 1.45–2.83 |
| Weekly working days | ||||
| Fixed | 1.00 | 1.00 | ||
| Not fixed | 2.99 | 2.60–3.43 | 2.22 | 1.43–3.34 |
| Weekly work shift | ||||
| Fixed | 1.00 | 1.00 | ||
| Not fixed | 2.21 | 1.96–2.51 | 1.25 | 0.84–1.83 |
| Start and end time of each shift | ||||
| Fixed | 1.00 | 1.00 | ||
| Not fixed | 3.37 | 2.85–3.97 | 2.95 | 1.78–4.75 |
| Variables | Working Hours ≤52 h/Week | Working Hours >52 h/Week | ||
|---|---|---|---|---|
| ORs | 95% CIs | ORs | 95% CIs | |
| Work schedule * | ||||
| Regular | 1.00 | 1.00 | ||
| Irregular | 3.22 | 2.71–3.83 | 2.64 | 1.56–4.40 |
| Daily working hours | ||||
| Fixed | 1.00 | 1.00 | ||
| Not fixed | 3.96 | 3.31–4.72 | 3.39 | 1.96–5.72 |
| Weekly working days | ||||
| Fixed | 1.00 | 1.00 | ||
| Not fixed | 5.51 | 4.54–6.66 | 3.12 | 1.55–5.80 |
| Weekly work shift | ||||
| Fixed | 1.00 | 1.00 | ||
| Not fixed | 3.51 | 2.92–4.22 | 1.62 | 0.81–2.98 |
| Start and end time of each shift | ||||
| Fixed | 1.00 | 1.00 | ||
| Not fixed | 5.95 | 4.78–7.37 | 4.29 | 2.00–8.41 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yun, S.; Kim, M.; Lee, W.-T.; Yoon, J.-H.; Won, J.-U. Irregular Work Hours and the Risk of Sleep Disturbance Among Korean Service Workers Required to Suppress Emotion. Int. J. Environ. Res. Public Health 2021, 18, 1517. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041517
Yun S, Kim M, Lee W-T, Yoon J-H, Won J-U. Irregular Work Hours and the Risk of Sleep Disturbance Among Korean Service Workers Required to Suppress Emotion. International Journal of Environmental Research and Public Health. 2021; 18(4):1517. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041517
Chicago/Turabian StyleYun, Sehyun, Minsuk Kim, Won-Tae Lee, Jin-Ha Yoon, and Jong-Uk Won. 2021. "Irregular Work Hours and the Risk of Sleep Disturbance Among Korean Service Workers Required to Suppress Emotion" International Journal of Environmental Research and Public Health 18, no. 4: 1517. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041517