
Dose-Response Relationship between Night Work and the Prevalence of Impaired Fasting Glucose: The Korean Worker’s Special Health Examination for Night Workers Cohort


Abstract
:1. Introduction
2. Materials and Methods
2.1. SHEW for Night Work
2.2. Study Population and Data Collection
2.3. Ethics
2.4. Definition of Covariates
2.5. Statistical Analyses
3. Results
4. Discussion
4.1. Limitations
4.2. Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes Atlas, 9th ed.; International Diabetes Federation: Brussels, Belgium, 2019; Available online: https://www.diabetesatlas.org (accessed on 23 November 2020).
- GBD 2017 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1923–1994. [Google Scholar] [CrossRef] [Green Version]
- Ng, Y.C.; Jacobs, P.; Johnson, J. Productivity losses associated with diabetes in the US. Diabetes Care 2001, 24, 257–261. [Google Scholar] [CrossRef] [Green Version]
- Pedron, S.; Emmert-Fees, K.; Laxy, M.; Schwettmann, L. The impact of diabetes on labour market participation: A systematic review of results and methods. BMC Public Health 2019, 19, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeFronzo, R.A.; Ferrannini, E.; Groop, L.; Henry, R.R.; Herman, W.H.; Holst, J.J.; Hu, F.B.; Kahn, C.R.; Raz, I.; Shulman, G.I.; et al. Type 2 diabetes mellitus. Nat. Rev. Dis. Prim. 2015, 1, 15019. [Google Scholar] [CrossRef] [PubMed]
- Morikawa, Y.; Nakagawa, H.; Miura, K.; Soyama, Y.; Ishizaki, M.; Kido, T.; Naruse, Y.; Suwazono, Y.; Nogawa, K. Shift work and the risk of diabetes mellitus among Japanese male factory workers. Scand. J. Work. Environ. Health 2005, 31, 179–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suwazono, Y.; Sakata, K.; Okubo, Y.; Harada, H.; Oishi, M.; Kobayashi, E.; Uetani, M.; Kido, T.; Nogawa, K. Long-Term Longitudinal Study on the Relationship Between Alternating Shift Work and the Onset of Diabetes Mellitus in Male Japanese Workers. J. Occup. Environ. Med. 2006, 48, 455–461. [Google Scholar] [CrossRef]
- Zoto, E.; Cenko, F.; Doci, P.; Rizza, S. Effect of night shift work on risk of diabetes in healthy nurses in Albania. Acta Diabetol. 2019, 56, 811–813. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Government Legislation. Article 130 of Occupational Safety and Health Act. Available online: http://www.law.go.kr/LSW//lsInfoP.do?lsiSeq=219125&efYd=20200609&ancYnChk=0#0000 (accessed on 23 November 2020).
- Ministry of Government Legislation. Attached Table 22 of Enforcemnt rule of Occupational Safety and Health Act. Available online: http://www.law.go.kr/%EB%B2%95%EB%A0%B9/%EC%82%B0%EC%97%85%EC%95%88%EC%A0%84%EB%B3%B4%EA%B1%B4%EB%B2%95%EC%8B%9C%ED%96%89%EA%B7%9C%EC%B9%99 (accessed on 23 November 2020).
- Ministry of Government Legislation. Attached Table 24 of Enforcemnt rule of Occupational Safety and Health. Available online: http://www.law.go.kr/%EB%B2%95%EB%A0%B9/%EC%82%B0%EC%97%85%EC%95%88%EC%A0%84%EB%B3%B4%EA%B1%B4%EB%B2%95%EC%8B%9C%ED%96%89%EA%B7%9C%EC%B9%99 (accessed on 23 November 2020).
- Ministry of Health and Welfare. The Physical Activity Guide for Koreans. Available online: http://www.mohw.go.kr/react/jb/sjb030301vw.jsp?PAR_MENU_ID=03&MENU_ID=032901&CONT_SEQ=337139 (accessed on 23 November 2020).
- Kim, J.S. Management of drinking patients in primary care. Korean J. Fam. Pract. 2012, 2, 280–288. [Google Scholar]
- World Health Organization. Regional Office for the Western Pacific. The Asia-Pacific perspective: Redefining obesity and its treatment [Internet]. Sydney: Health Communications Australia. Available online: https://apps.who.int/iris/handle/10665/206936 (accessed on 23 November 2020).
- Hu, G.; Lindström, J.; Valle, T.T.; Eriksson, J.G.; Jousilahti, P.; Silventoinen, K.; Qiao, Q.; Tuomilehto, J. Physical Activity, Body Mass Index, and Risk of Type 2 Diabetes in Patients with Normal or Impaired Glucose Regulation. Arch. Intern. Med. 2004, 164, 892–896. [Google Scholar] [CrossRef] [Green Version]
- Biggs, M.L. Association Between Adiposity in Midlife and Older Age and Risk of Diabetes in Older Adults. JAMA 2010, 303, 2504–2512. [Google Scholar] [CrossRef] [Green Version]
- Qian, J.; Scheer, F.A. Circadian System and Glucose Metabolism: Implications for Physiology and Disease. Trends Endocrinol. Metab. 2016, 27, 282–293. [Google Scholar] [CrossRef] [Green Version]
- Scheer, F.A.J.L.; Hilton, M.F.; Mantzoros, C.S.; Shea, S.A. Adverse metabolic and cardiovascular consequences of circadian misalignment. Proc. Natl. Acad. Sci. USA 2009, 106, 4453–4458. [Google Scholar] [CrossRef] [Green Version]
- Gale, J.E.; Cox, H.I.; Qian, J.; Block, G.D.; Colwell, C.S.; Matveyenko, A.V. Disruption of Circadian Rhythms Accelerates Development of Diabetes through Pancreatic Beta-Cell Loss and Dysfunction. J. Biol. Rhythm. 2011, 26, 423–433. [Google Scholar] [CrossRef] [Green Version]
- Rakshit, K.; Thomas, A.P.; Matveyenko, A.V. Does disruption of circadian rhythms contribute to beta-cell failure in type 2 diabetes? Curr. Diabetes Rep. 2014, 14, 474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.; Schernhammer, E.; Schwarzschild, M.A.; Ascherio, A. A Prospective Study of Night Shift Work, Sleep Duration, and Risk of Parkinson’s Disease. Am. J. Epidemiol. 2006, 163, 726–730. [Google Scholar] [CrossRef] [Green Version]
- Sallinen, M.; Kecklund, G. Shift work, sleep, and sleepiness—Differences between shift schedules and systems. Scand. J. Work. Environ. Health 2010, 36, 121–133. [Google Scholar] [CrossRef]
- Mansukhani, M.P.; Kolla, B.P.; Surani, S.; Varon, J.; Ramar, K. Sleep Deprivation in Resident Physicians, Work Hour Limitations, and Related Outcomes: A Systematic Review of the Literature. Postgrad. Med. 2012, 124, 241–249. [Google Scholar] [CrossRef]
- Spiegel, K.; Knutson, K.; Leproult, R.; Tasali, E.; Van Cauter, E. Sleep loss: A novel risk factor for insulin resistance and Type 2 diabetes. J. Appl. Physiol. 2005, 99, 2008–2019. [Google Scholar] [CrossRef] [PubMed]
- Ayas, N.T.; White, D.P.; Al-Delaimy, W.K.; Manson, J.E.; Stampfer, M.J.; Speizer, F.E.; Patel, S.; Hu, F.B. A Prospective Study of Self-Reported Sleep Duration and Incident Diabetes in Women. Diabetes Care 2003, 26, 380–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knutsson, A.; Kempe, A. Shift work and diabetes—A systematic review. Chronobiol. Int. 2014, 31, 1146–1151. [Google Scholar] [CrossRef] [PubMed]
- Pan, A.; Schernhammer, E.S.; Sun, Q.; Hu, F.B. Rotating Night Shift Work and Risk of Type 2 Diabetes: Two Prospective Cohort Studies in Women. PLoS Med. 2011, 8, e1001141. [Google Scholar] [CrossRef] [Green Version]
- Antunes, L.C.; Levandovski, R.; Dantas, G.; Caumo, W.; Hidalgo, M.P. Obesity and shift work: Chronobiological aspects. Nutr. Res. Rev. 2010, 23, 155–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Drongelen, A.; Boot, C.R.L.; Merkus, S.L.; Smid, T.; Van Der Beek, A.J. The effects of shift work on body weight change—A systematic review of longitudinal studies. Scand. J. Work. Environ. Health 2011, 37, 263–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spiegel, K.; Tasali, E.; Penev, P.; Van Cauter, E. Brief Communication: Sleep Curtailment in Healthy Young Men Is Associated with Decreased Leptin Levels, Elevated Ghrelin Levels, and Increased Hunger and Appetite. Ann. Intern. Med. 2004, 141, 846–850. [Google Scholar] [CrossRef]
- Hargens, T.A.; Kaleth, A.S.; Edwards, E.S.; Butner, K.L. Association between sleep disorders, obesity, and exercise: A review. Nat. Sci. Sleep 2013, 5, 27–35. [Google Scholar] [CrossRef] [Green Version]
- Toshihiro, M.; Saito, K.; Takikawa, S.; Takebe, N.; Onoda, T.; Satoh, J. Psychosocial factors are independent risk factors for the development of Type 2 diabetes in Japanese workers with impaired fasting glucose and/or impaired glucose tolerance1. Diabet. Med. 2008, 25, 1211–1217. [Google Scholar] [CrossRef] [Green Version]
- Pippitt, K.; Li, M.; Gurgle, H.E. Diabetes Mellitus: Screening and Diagnosis. Am. Fam. Physician 2016, 93, 103–109. [Google Scholar]
- Yan, H.; Yang, W.; Zhou, F.; Li, X.; Pan, Q.; Shen, Z.; Han, G.; Newell-Fugate, A.; Tian, Y.; Majeti, R.; et al. Estrogen Improves Insulin Sensitivity and Suppresses Gluconeogenesis via the Transcription Factor Foxo1. Diabetes 2019, 68, 291–304. [Google Scholar] [CrossRef] [Green Version]
- Hoshuyama, T.; Hino, Y.; Kayashima, K.; Morita, T.; Goto, H.; Minami, M.; Sakuragi, S.; Tanaka, C.; Takahashi, K. Inequality in the health status of workers in small-scale enterprises. Occup. Med. 2006, 57, 126–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, A.B.; Stayner, L.; Hansen, J.; Andersen, Z.J. Night shift work and incidence of diabetes in the Danish Nurse Cohort. Occup. Environ. Med. 2016, 73, 262–268. [Google Scholar] [CrossRef]
- Gommans, F.; Jansen, N.; Stynen, D.; De Grip, A.; Kant, I. The ageing shift worker: A prospective cohort study on need for recovery, disability, and retirement intentions. Scand. J. Work. Environ. Health 2015, 41, 356–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, W.; Chen, Z.; Ruan, W.; Yi, G.; Wang, D.; Lu, Z. A meta-analysis of cohort studies including dose-response relationship between shift work and the risk of diabetes mellitus. Eur. J. Epidemiol. 2019, 34, 1013–1024. [Google Scholar] [CrossRef] [PubMed]
- Gan, Y.; Yang, C.; Tong, X.; Sun, H.; Cong, Y.; Yin, X.; Li, L.; Cao, S.; Dong, X.; Gong, Y.; et al. Shift work and diabetes mellitus: A meta-analysis of observational studies. Occup. Environ. Med. 2015, 72, 72–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Normal, N (%) (N = 78,900) | IFG, N (%) (N = 1177) | p-Value | |
|---|---|---|---|
| Age | |||
| 38.8 ± 11.8 (years) | 38.6 ± 11.8 | 47.7 ± 10.4 | <0.0001 |
| <20 s | 21,608 (27.39) | 55 (4.67) | <0.0001 |
| 30 s | 22,403 (28.39) | 215 (18.27) | |
| 40 s | 18,617 (23.60) | 361 (30.67) | |
| ≥50 s | 16,272 (20.62) | 546 (46.39) | |
| Sex | <0.0001 | ||
| Male | 59,422 (75.31) | 1045 (88.79) | |
| Female | 19,478 (24.69) | 132 (11.21) | |
| Exercise | 0.0027 | ||
| Adequate | 35,557 (45.07) | 582 (49.45) | |
| Lack of exercise | 43,343 (54.93) | 595 (50.55) | |
| Alcohol drinking | 0.1569 | ||
| Adequate | 56,383 (71.46) | 819 (69.58) | |
| Heavy | 22,517 (28.54) | 358 (30.42) | |
| Smoking | <0.0001 | ||
| Non-smoker | 34,684 (43.96) | 390 (33.14) | |
| Ex-smoker | 16,218 (20.56) | 396 (33.64) | |
| Current-smoker | 27,998 (35.49) | 391 (33.22) | |
| Duration of night work | |||
| 6.1 ± 7.7 (years) | 6.0 ± 7.7 | 10.5 ± 10.0 | <0.0001 |
| <2 years | 16,757 (21.24) | 146 (12.40) | <0.0001 |
| 2–5 years | 27,823 (35.26) | 281 (23.87) | |
| 5–12 years | 17,452 (22.12) | 270 (22.94) | |
| ≥12 years | 16,868 (21.38) | 480 (40.78) | |
| History of hypertension | <0.0001 | ||
| No | 73,870 (93.62) | 952 (80.88) | |
| Yes | 5030 (6.38) | 225 (19.12) | |
| History of dyslipidemia | 0.0046 | ||
| No | 77,698 (98.48) | 1147 (97.45) | |
| Yes | 1202 (1.52) | 30 (2.55) | |
| BMI | <0.0001 | ||
| <23 kg/m2 | 32,371 (41.03) | 250 (21.24) | |
| 23–24.9 kg/m2 | 18,912 (23.97) | 278 (23.62) | |
| 25–29.9 kg/m2 | 23,343 (29.59) | 535 (45.45) | |
| ≥30 kg/m2 | 4274 (5.42) | 114 (9.69) | |
| Abdominal obesity | * < 0.0001 | ||
| No | 65,123 (82.54) | 814 (69.16) | |
| Yes | 13,777 (17.46) | 363 (30.84) |
| Crude | Model 1 † | Model 2 ‡ | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | |
| Duration of night work | ||||||
| <2 years | 1.00 | 1.00 | 1.00 | |||
| 2~5 years | 1.16 | 0.95–1.42 | 1.14 | 0.93–1.40 | 1.12 | 0.92–1.38 |
| 5~12years | 1.78 * | 1.45–2.18 | 1.51 * | 1.23–1.86 | 1.49 * | 1.21–1.84 |
| ≥12 years | 3.27 * | 2.72–3.95 | 1.75 * | 1.44–2.12 | 1.74 * | 1.44–2.12 |
| Age | ||||||
| ≤20 s | 1.00 | 1.00 | 1.00 | |||
| 30 s | 3.77 * | 2.83–5.12 | 2.67 * | 1.99–3.65 | 2.77 * | 2.06–3.79 |
| 40 s | 7.62 * | 5.79–10.23 | 4.91 * | 3.67–6.68 | 4.96 * | 3.72–6.75 |
| ≥50 s | 13.18 * | 10.08–17.60 | 9.14 * | 6.87–12.38 | 8.81 * | 6.64–11.92 |
| Sex | ||||||
| Male | 1.00 | 1.00 | 1.00 | |||
| Female | 0.39 * | 0.32–-0.46 | 0.53 * | 0.43–0.65 | 0.50 * | 0.40–0.61 |
| Exercise | ||||||
| Adequate | 1.00 | 1.00 | 1.00 | |||
| Lack of exercise | 0.84 * | 0.75–0.94 | 1.15 * | 1.03–1.30 | 1.12 | 0.99–1.26 |
| Drinking | ||||||
| Adequate | 1.00 | 1.00 | 1.00 | |||
| Heavy | 1.10 | 0.97–1.24 | 1.14 | 1.00–1.30 | 1.16 | 1.02–1.32 |
| Smoking | ||||||
| Non-smoker | 1.00 | 1.00 | 1.00 | |||
| Ex-smoker | 2.17 * | 1.89–2.50 | 1.09 | 0.93–1.28 | 1.10 | 0.94–1.29 |
| Current-smoker | 1.24 * | 1.08–1.43 | 0.96 | 0.82–1.13 | 0.95 | 0.81–1.11 |
| History of hypertension | ||||||
| Normal | 1.00 | 1.00 | 1.00 | |||
| Hypertension | 3.47 * | 2.99–4.02 | 1.58 * | 1.34–1.84 | 1.67 * | 1.42–1.95 |
| History of dyslipidemia | ||||||
| Normal | 1.00 | 1.00 | 1.00 | |||
| Dyslipidemia | 1.69 * | 1.15–2.39 | 0.84 | 0.57–1.20 | 0.84 | 0.57–1.20 |
| BMI | ||||||
| Normal | 1.00 | 1.00 | ||||
| Overweight | 1.90 * | 1.60–2.26 | 1.37 * | 1.15–1.63 | ||
| Obesity | 2.97 * | 2.56–3.46 | 2.10 * | 1.80–2.45 | ||
| Severe obesity | 3.45 * | 2.75–4.31 | 3.62 * | 2.87–4.54 | ||
| Abdominal obesity | ||||||
| Normal | 1.00 | 1.00 | ||||
| Abdominal obesity | 2.11 * | 1.86–2.39 | 1.79 * | 1.57–2.04 | ||
| Normal, N (%) | IFG, N (%) | Crude | Model 1 † | Model 2 ‡ | ||||
|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | OR | 95% CI | |||
| Duration of night work * | ||||||||
| 9.5 ± 9.6 (years) | 9.5 ± 9.6 | 12.0 ± 10.6 | ||||||
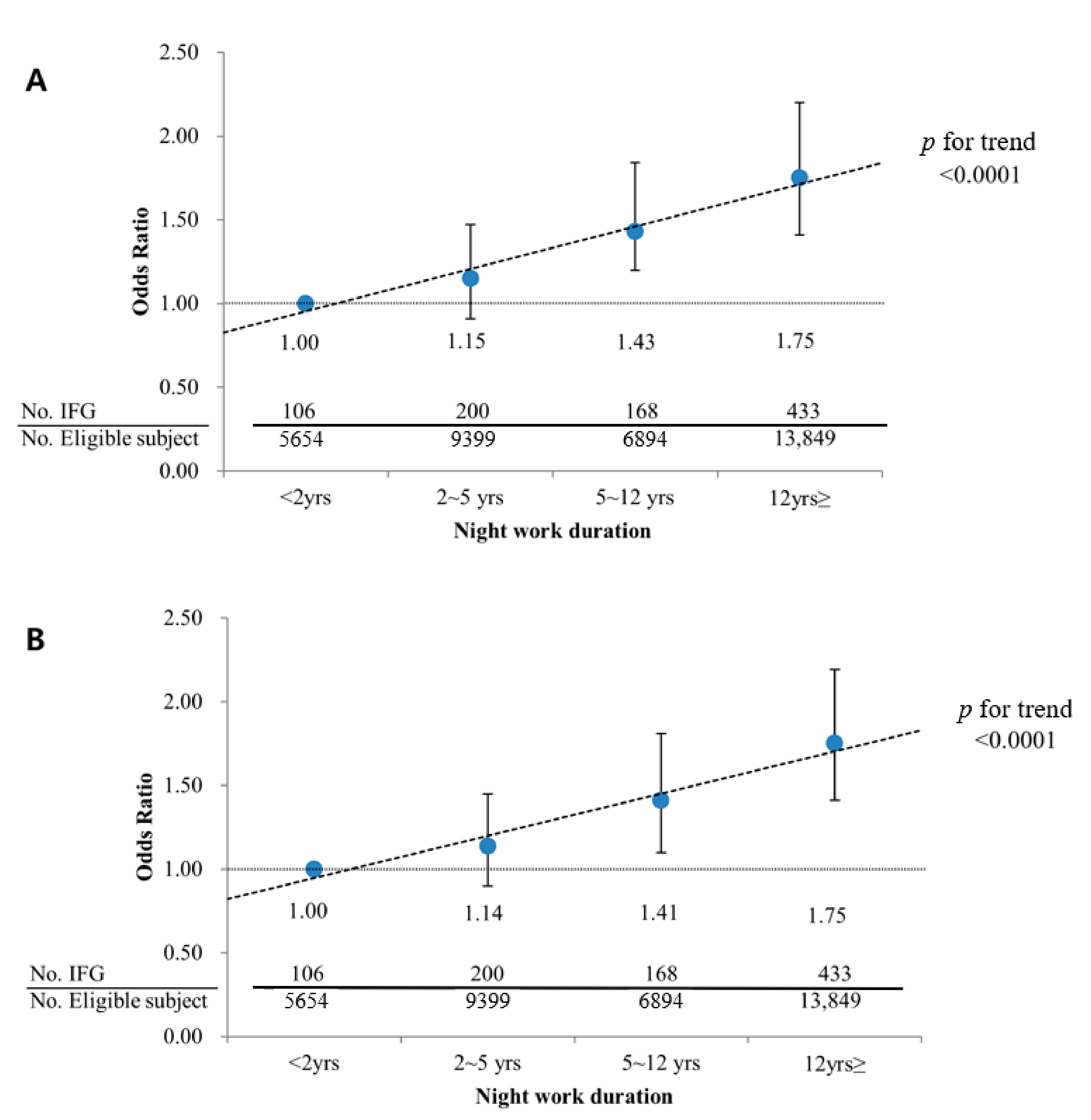
| <2 years | 5548 (15.90) | 106 (11.69) | 1.00 | 1.00 | 1.00 | |||
| 2~5 years | 9199 (26.37) | 200 (22.05) | 1.14 | 0.90–1.45 | 1.15 | 0.91–1.47 | 1.14 | 0.90–1.45 |
| 5~12years | 6726 (19.28) | 168 (18.52) | 1.31 * | 1.02–1.68 | 1.43 * | 1.20–1.84 | 1.41 * | 1.10–1.81 |
| ≥12 years | 13,416 (38.45) | 433 (47.74) | 1.69 * | 1.37–2.10 | 1.75 * | 1.41–2.20 | 1.75 * | 1.41–2.19 |
| Age * (years) | ||||||||
| 50.0 ± 7.1 | 49.9 ± 7.1 | 51.9 ± 7.4 | 1.04 * | 1.03–1.05 | 1.04 * | 1.03–1.05 | 1.04 * | 1.03–1.05 |
| Sex * | ||||||||
| Male | 27,401 (78.54) | 815 (89.86) | 1.00 | 1.00 | 1.00 | |||
| Female | 7488 (21.46) | 92 (10.14) | 0.41 * | 0.33–0.51 | 0.47 * | 0.37–0.61 | 0.46 * | 0.35–0.59 |
| Exercise | ||||||||
| Adequate | 18,589 (53.28) | 496 (54.69) | 1.00 | 1.00 | 1.00 | |||
| Lack of exercise | 16,300 (46.72) | 411 (45.31) | 0.95 | 0.83–1.08 | 1.07 | 0.94–1.23 | 1.05 | 0.92–1.20 |
| Drinking * | ||||||||
| Adequate | 26,858 (76.98) | 653 (72.00) | 1.00 | 1.00 | 1.00 | |||
| Heavy | 8031 (23.02) | 254 (28.00) | 1.30 * | 1.12–1.51 | 1.16 | 0.99–1.35 | 1.17 * | 1.00–1.37 |
| Smoking * | ||||||||
| Non-smoker | 14,190 (40.67) | 300 (33.08) | 1.00 | 1.00 | 1.00 | |||
| Ex-smoker | 10,283 (29.47) | 339 (37.38) | 1.56 * | 1.33–1.83 | 1.03 | 0.86–1.23 | 1.04 | 0.88–1.25 |
| Current-smoker | 10,416 (29.85) | 268 (29.55) | 1.22 * | 1.03–1.44 | 0.94 | 0.78–1.14 | 0.92 | 0.77–1.11 |
| History of hypertension * | ||||||||
| Normal | 30,461 (87.31) | 693 (76.41) | 1.00 | 1.00 | 1.00 | |||
| Hypertension | 4428 (12.69) | 214 (23.59) | 2.13 * | 1.81–2.48 | 1.53 * | 1.29–1.81 | 1.64 * | 1.38–1.93 |
| History of dyslipidemia | ||||||||
| Normal | 33,896 (97.15) | 880 (97.02) | 1.00 | 1.00 | 1.00 | |||
| Dyslipidemia | 993 (2.85) | 27 (2.98) | 1.05 | 0.69–1.51 | 0.82 | 0.54–1.19 | 0.83 | 0.54–1.20 |
| BMI * | ||||||||
| Normal | 12,231 (35.06) | 194 (21.39) | 1.00 | 1.00 | 1.00 | |||
| Overweight | 9788 (28.05) | 242 (26.68) | 1.56 * | 1.29–1.89 | 1.40 * | 1.16–1.70 | ||
| Obesity | 11,699 (33.53) | 415 (45.76) | 2.24 * | 1.89–2.66 | 1.95 * | 1.64–2.33 | ||
| Severe obesity | 1171 (3.36) | 56 (6.17) | 3.02 * | 2.21–4.05 | 2.88 * | 2.10–3.90 | ||
| Abdominal obesity * | ||||||||
| Normal | 28,600 (81.97) | 656 (72.33) | 1.00 | 1.00 | 1.00 | |||
| Abdominal obesity | 6289 (18.03) | 251 (27.67) | 1.74 * | 1.50–2.02 | 1.53 * | 1.31–1.78 | ||
| Total number | 34,889 (97.47) | 907 (2.53) | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.Y.; Lee, J.-W.; Choi, W.S.; Myong, J.-P. Dose-Response Relationship between Night Work and the Prevalence of Impaired Fasting Glucose: The Korean Worker’s Special Health Examination for Night Workers Cohort. Int. J. Environ. Res. Public Health 2021, 18, 1854. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041854
Lee JY, Lee J-W, Choi WS, Myong J-P. Dose-Response Relationship between Night Work and the Prevalence of Impaired Fasting Glucose: The Korean Worker’s Special Health Examination for Night Workers Cohort. International Journal of Environmental Research and Public Health. 2021; 18(4):1854. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041854
Chicago/Turabian StyleLee, Jae Yong, Ji-Won Lee, Won Seon Choi, and Jun-Pyo Myong. 2021. "Dose-Response Relationship between Night Work and the Prevalence of Impaired Fasting Glucose: The Korean Worker’s Special Health Examination for Night Workers Cohort" International Journal of Environmental Research and Public Health 18, no. 4: 1854. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041854