
“Who Are at Higher Sexual Risk?” Latent Class Analysis of Behavioral Intentions among Spanish Adolescents


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. Demographic Variables
2.2.2. Behavioral Intentions
2.2.3. Sexual Behavior
2.3. Procedure
2.4. Data Analyses
3. Results
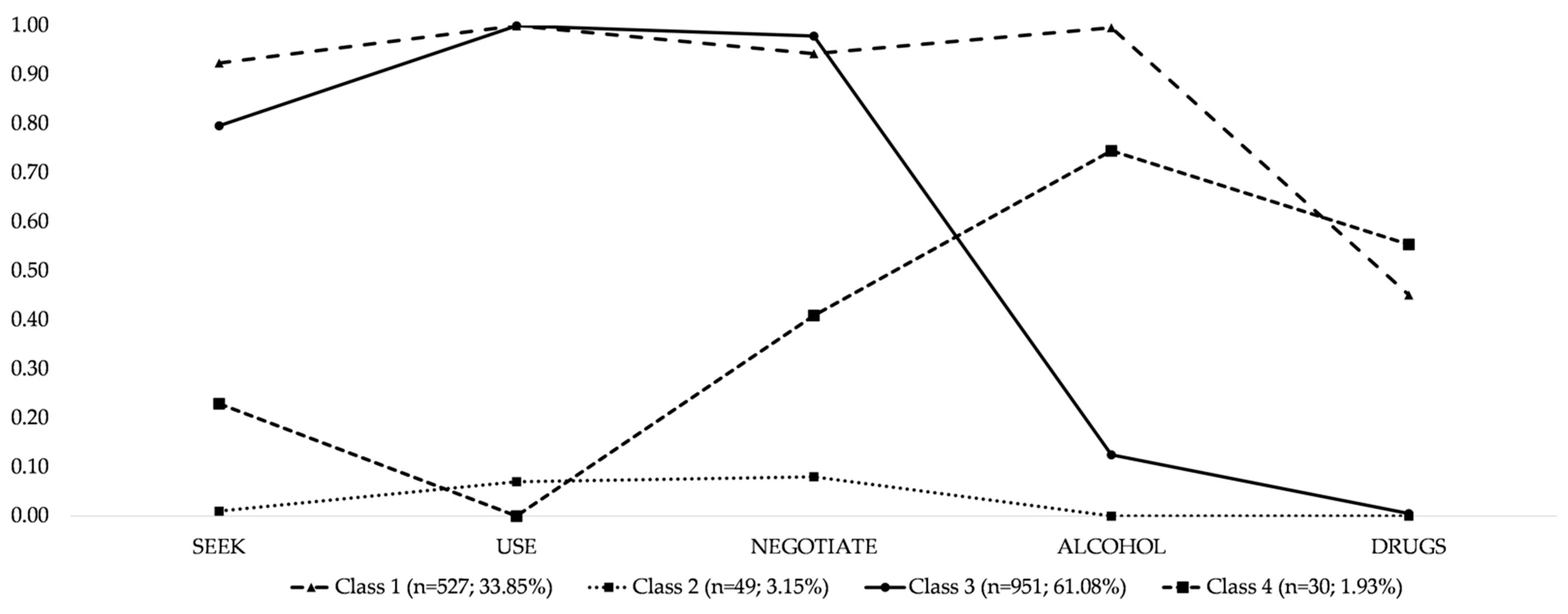
3.1. Latent Class Models
3.2. Association between Behavioral Intentions and Latent Classes
3.3. Predicting Latent Class Membership
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rowley, J.; Hoorn, S.V.; Korenromp, E.; Low, N.; Unemo, M.; Abu-Raddad, L.J.; Chico, R.M.; Smolak, A.; Newman, L.; Gottlieb, S.; et al. Chlamydia, gonorrhoea, trichomoniasis and syphilis: Global prevalence and incidence estimates, 2016. Bull. World Health Organ. 2019, 97, 548–562. [Google Scholar] [CrossRef]
- Amin, A. Addressing gender inequalities to improve the sexual and reproductive health and wellbeing of women living with HIV. J. Int. AIDS Soc. 2015, 18, 20302. [Google Scholar] [CrossRef]
- World Health Organization. Report on Global Sexually Transmitted Infection Surveillance. 2018. Updated 2018. Available online: https://apps.who.int/iris/bitstream/handle/10665/277258/9789241565691-eng.pdf?ua=1 (accessed on 3 November 2020).
- Looker, K.J.; Magaret, A.S.; Turner, K.M.; Vickerman, P.; Gottlieb, S.L.; Newman, L.M. Global estimates of prevalent and incident herpes simplex virus type 2 infections in 2012. PLoS ONE 2015, 10, e114989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Sanjosé, S.; Diaz, M.; Castellsagué, X.; Clifford, G.; Bruni, L.; Muñoz, N.; Bosch, F.X. Worldwide prevalence and genotype distribution of cervical human papillomavirus DNA in women with normal cytology: A meta-analysis. Lancet Infect. Dis. 2007, 7, 453–459. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control; WHO Regional Office for Europe (Eds.) HIV/AIDS Surveillance in Europe 2018–2017 Data; WHO Regional Office for Europe: Copenhagen, Danmark, 2018. [Google Scholar]
- Área de Vigilancia de VIH y Comportamientos de Riesgo (Ed.) Vigilancia Epidemiológica del VIH y sida en España 2017; Plan Nacional sobre el Sida-D.G. de Salud Pública, Calidad e Innovación/Centro Nacional de Epidemiología-ISCIII; Sistema de Información sobre Nuevos Diagnósticos de VIH y Registro Nacional de Casos de Sida: Madrid, Spain, 2018. [Google Scholar]
- Unidad de vigilancia del VIH, hepatitis y conductas de riesgo. Vigilancia Epidemiológica de las Infecciones de Transmisión Sexual en España, 2018. Centro Nacional de Epidemiología, Instituto de Salud Carlos III/Plan Nacional sobre el Sida, Dirección General de Salud Pública, Calidad e Innovación. 2020. Available online: https://www.mscbs.gob.es/ciudadanos/enfLesiones/enfTransmisibles/sida/vigilancia/Vigilancia_ITS_1995_2018_def.pdf (accessed on 8 November 2020).
- Avellaneda, C.N.; Dávalos, E. Identifying the macro-level drivers of adolescent fertility rate in latin america: The role of school-based sexuality education. Am. J. Sex. Educ. 2017, 12, 358–382. [Google Scholar] [CrossRef]
- Leppälahti, S.; Gissler, M.; Mentula, M.; Heikinheimo, O. Is teenage pregnancy an obstetric risk in a welfare society? A population-based study in finland, from 2006 to 2011. BMJ Open 2013, 3, e003225. [Google Scholar]
- INJUVE (Ed.) Informe Juventud en España 2016; Instituto de la Juventud: Madrid, Spain, 2017. [Google Scholar]
- Moreno, C.; Ramos, P.; Rivera, F.; Sánchez-Queija, I.; Jiménez-Iglesias, A.; García-Moya, I.; Fuchs, N. (Eds.) Los Estilos de Vida y la Salud de los Adolescentes Españoles a lo largo de La Primera década del Milenio. El Estudio Health Behaviour in School-Aged Children (HBSC) 2002–2006–2010; Ministerio de Sanidad, SERVICIOS Sociales e Igualdad: Madrid, Spain, 2013.
- Escribano, S.; Espada, J.; Morales, A.; Orgilés, M. Mediation analysis of an effective sexual health promotion intervention for spanish adolescents. AIDS Behav. 2015, 19, 1850–1859. [Google Scholar] [CrossRef]
- Morales, A.; Espada, J.P.; Orgilés, M. A 1-year follow-up evaluation of a sexual-health education program for spanish adolescents compared with a well-established program. Eur. J. Public Health 2016, 26, 35–41. [Google Scholar] [CrossRef] [Green Version]
- Ajzen, I. Theory of planned behavior. Handb. Theor. Soc. Psychol. Vol. One 2011, 1, 438. [Google Scholar]
- Ajzen, I. From intentions to actions: A theory of planned behavior. In Action-Control: From Cognition to Behavior; Kuhl, J., Beckman, J., Eds.; Springer: Heidelberg, Germany, 1985; pp. 11–39. [Google Scholar]
- Ajzen, I. The theory of planned behavior. Organ. Behav Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Armitage, C.J.; Conner, M. Efficacy of the theory of planned behaviour: A meta-analytic review. Br. J. Soc. Psychol. 2001, 40, 471–499. [Google Scholar] [CrossRef] [Green Version]
- Godin, G.; Kok, G. The theory of planned behavior: A review of its applications to health-related behaviors. Am. J. Health Promot. 1996, 11, 87–98. [Google Scholar] [CrossRef] [PubMed]
- Albarracin, D.; Johnson, B.T.; Fishbein, M.; Muellerleile, P.A. Theories of reasoned action and planned behavior as models of condom use: A meta-analysis. Psychol. Bull. 2001, 127, 142. [Google Scholar] [CrossRef] [Green Version]
- Espada, J.P.; Morales, A.; Guillén-Riquelme, A.; Ballester, R.; Orgilés, M. Predicting condom use in adolescents: A test of three socio-cognitive models using a structural equation modeling approach. BMC Public Health 2016, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarkar, N. Barriers to condom use. Eur. J. Contracept. Reprod. Health Care 2008, 13, 114–122. [Google Scholar] [CrossRef] [PubMed]
- Espada, J.P.; Morales, A. Comportamientos sexuales en nuestros jóvenes: De la salud al riesgo. In La Salud Afectivo-Sexual de la Juventud en España; Fuertes, A., González, E., Eds.; Rev. de Estud. de Juv.; Instituto de la Juventud: Madrid, Spain, 2019; pp. 31–45. Available online: http://www.injuve.es/sites/default/files/adjuntos/2020/01/revista_injuve_123.pdf (accessed on 30 October 2020).
- Espada, J.P.; Morales, A.; Orgiles, M.; Piqueras, J.A.; Carballo, J.L. Sexual behaviour under the influence of alcohol among spanish adolescents. Adicciones 2013, 25, 55–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seth, P.; Sales, J.M.; DiClemente, R.J.; Wingood, G.M.; Rose, E.; Patel, S.N. Longitudinal examination of alcohol use: A predictor of risky sexual behavior and trichomonas vaginalis among african-american female adolescents. Sex. Transm. Dis. 2011, 38, 96–101. [Google Scholar] [CrossRef]
- Diane, M.; Mary, M.; Gillmore, R.; Hoppe, M.J.; Gaylord, J.; Leigh, B.C.; Rainey, D.; Morrison, D.M.; Gillmore, M.R. Adolescent drinking and sex: Findings from a daily diary study. Perspect. Sex. Reprod. Health 2003, 35, 162–168. [Google Scholar] [CrossRef]
- Cooper, M.L. Alcohol use and risky sexual behavior among college students and youth: Evaluating the evidence. J. Stud. Alcohol Drugs. 2002, 101–117. [Google Scholar] [CrossRef] [Green Version]
- Lomba, L.; Apóstolo, J.; Mendes, F. Consumo de drogas, alcohol y conductas sexuales en los ambientes recreativos nocturnos de portugal drugs and alcohol consumption and sexual behaviours in night recreational settings in portugal. Adicciones 2009, 21, 309–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Methodology Center. Latent Class Analysis. Updated 2020. Available online: https://methodology.psu.edu/ra/lca (accessed on 17 October 2020).
- Castro-López, C.; Tenorio-Aguirre, A.J. Modelos de clases latentes aplicados a las encuestas de percepción ciudadana: Estudio de caso. Rev. Legis. de Estud. Soc. y de Opin. Pública 2010, 3, 187–200. [Google Scholar]
- Espada, J.P.; Escribano, S.; Orgilés, M.; Morales, A.; Guillén-Riquelme, A. Sexual risk behaviors increasing among adolescents over time: Comparison of two cohorts in spain. AIDS Care 2015, 27, 783–788. [Google Scholar] [CrossRef] [PubMed]
- Morales, A.; Vallejo-Medina, P.; Abello-Luque, D.; Saavedra-Roa, A.; García-Roncallo, P.; Gomez-Lugo, M.; García-Montaño, E.; Marchal-Bertrand, L.; Niebles-Charris, J.; Pérez-Pedraza, D.; et al. Sexual risk among colombian adolescents: Knowledge, attitudes, normative beliefs, perceived control, intention, and sexual behavior. BMC Public Health 2018, 18, 1377. [Google Scholar] [CrossRef]
- Boyce, W.; Torsheim, T.; Currie, C.; Zambon, A. The family affluence scale as a measure of national wealth: Validation of an adolescent self-report measure. Soc. Indic. Res. 2006, 78, 473–487. [Google Scholar] [CrossRef]
- Espada, J.P.; Morales, A.; Orgilés, M.; Jemmott, J.B.I.; Jemmott, L.S. Short-term evaluation of a skills-development sexual education program for spanish adolescents compared with a well-established program. J. Adolesc. Health 2015, 56, 30–37. [Google Scholar] [CrossRef]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 8th ed.; Muthén & Muthén: Los Angeles, CA, USA, 1998–2017. [Google Scholar]
- Lanza, S.T.; Cooper, B.R. Latent class analysis for developmental research. Child. Dev. Perspect. 2016, 10, 59–64. [Google Scholar] [CrossRef]
- Nylund, K.L.; Asparouhov, T.; Muthén, B.O. Deciding on the number of classes in latent class analysis and growth mixture modeling: A monte carlo simulation study. Struct. Equ. Model. 2007, 14, 535–569. [Google Scholar] [CrossRef]
- Tomczyk, S.; Isensee, B.; Hanewinkel, R. Latent classes of polysubstance use among adolescents-a systematic review. Drug Alcohol Depend. 2016, 160, 12–29. [Google Scholar] [CrossRef]
- Tomczyk, S.; Schomerus, G.; Stolzenburg, S.; Muehlan, H.; Schmidt, S. Who is seeking whom? A person-centred approach to help-seeking in adults with currently untreated mental health problems via latent class analysis. Soc. Psychiatry Psychiatr. Epidemiol. 2018, 53, 773–783. [Google Scholar] [CrossRef]
- Schreiber, J.B. Latent class analysis: An example for reporting results. Res. Soc. Adm. Pharm. 2017, 13, 1196–1201. [Google Scholar] [CrossRef]
- Fishbein, M.; Ajzen, I. Predicting and Changing Behavior: The Reasoned Action Approach; Taylor & Francis: Oxfordshire, UK, 2011. [Google Scholar]
- Morales, A.; Espada, J.P.; Orgilés, M.; Escribano, S.; Johnson, B.T.; Lightfoot, M. Interventions to reduce risk for sexually transmitted infections in adolescents: A meta-analysis of trials, 2008–2016. PLoS ONE 2018, 13, e0199421. [Google Scholar] [CrossRef]
- Morales, A.; Orgilés, M.; Espada, J.P. Sexually unexperienced adolescents benefit the most from a sexual education program for adolescents: A longitudinal cluster randomized controlled study. AIDS Educ. Prev. 2020, 32, 492–510. [Google Scholar]
- Dangerfield, D.T.; Harawa, N.T.; Smith, L.R.; Jeffries, W.L.; Baezconde-Garbanati, L.; Bluthenthal, R. Latent classes of sexual risk among black men who have sex with men and women. Arch. Sex. Behav. 2018, 47, 2071–2080. [Google Scholar] [CrossRef]


{kind=link}
| Females, N (%) | 760 (48.8) |
|---|---|
| Age, M ± SD | 14.87 ± 1.02 |
| Educational level, N (%) | |
| 9th grade | 835 (53.6) |
| 10th grade | 562 (36.1) |
| Curriculum adaptation—level 1 | 88 (5.7) |
| Curriculum adaptation—level 2 | 72 (4.6) |
| Socioeconomic status, N (%) | |
| Low | 521 (33.35) |
| Medium | 919 (59) |
| High | 117 (7.5) |
| Family situation, N (%) | |
| Married parents | 1144 (77.1) |
| Divorced parents | 309 (20.8) |
| Unmarried parents living together | 8 (0.5) |
| Single parent | 21 (1.4) |
| Orphan | 1 (0.1) |
| Behavioral intentions, M ± SD (range: 1–5) | |
| seek condoms | 3.62 ± 1.36 |
| condom use | 4.45 ± 0.96 |
| negotiate condom use | 4.27 ± 1.07 |
| have sex under alcohol influence | 2.18 ± 1.15 |
| have sex under drugs influence | 1.47 ± 0.94 |
| Sexually experienced *, N (%) | 506 (32.5) |
| Percentage of condom use, M ± SD | 85.13 (22.65) |
| 1 Class | 2 Classes | 3 Classes | 4 Classes | 5 Classes | 6 Classes | |
|---|---|---|---|---|---|---|
| Free parameters | 5 | 11 | 17 | 23 | 29 | Not identified |
| BLRT 1 | - | 479.59 *** | 423.45 *** | 38.96 *** | 5.98 | |
| AIC 2 | 6355.82 | 5888.23 | 5476.78 | 5449.82 | 5455.84 | |
| SSABIC 3 | 6366.69 | 5912.14 | 5513.74 | 5499.81 | 5518.88 | |
| Entropy | - | 1.00 | 0.86 | 0.88 | 0.89 | |
| ALCP 4 | 1.00 | 1.00 | 0.81 | 0.98 | 0.81 | |
| 1.00 | 0.99 | 0.94 | 0.90 | |||
| 0.98 | 0.98 | 0.64 | ||||
| 0.81 | 0.98 | |||||
| 0.90 |
| Total | Class 1 “Condom + Drugs” (n = 527) | Class 2 “Abstinent” (n = 49) | Class 3 “Condom + No Drugs” (n = 951) | Class 4 “No Condom + Drugs” (n = 30) | F/χ2 | E.S. | Direction | |
|---|---|---|---|---|---|---|---|---|
| Sociodemographics | ||||||||
| Females, N (%) | 760 (48.8) | 164 (31.1) | 25 (51) | 561 (59) | 10 (33.3) | 108.42 *** | 0.26 | 3 > 1 |
| Age, M ± SD | 14.87 ± 1.02 | 15.12 ± 1.04 | 14.82 ± 0.95 | 14.71 ± 0.98 | 15.30 ± 1.23 | 20.22 *** | 0.03 | 1 > 3 4 > 3 |
| Educational level, N (%) | ||||||||
| 9th grade | 835 (53.6) | 243 (46.1) | 30 (61.2) | 550 (57.8) | 12 (40) | 58.37 *** | 0.11 | 3 > 1 |
| 10th grade | 562 (36.1) | 204 (38.7) | 14 (28.6) | 335 (35.2) | 9 (30) | - | ||
| Curriculum adaptation—level 1 | 88 (5.7) | 34 (6.5) | 4 (8.2) | 45 (4.7) | 5 (16.7) | 4 > 3 | ||
| Curriculum adaptation—level 2 | 72 (4.6) | 46 (8.7) | 1 (2) | 21 (2.2) | 4 (13.3) | 4 > 3 4 > 1 | ||
| Socioeconomic status, N (%) | ||||||||
| Low | 521 (33.35) | 172 (32.6) | 19 (38.8) | 317 (33.3) | 13 (43.3) | 4.84 | - | - |
| Medium | 919 (59) | 307 (58.3) | 27 (55.1) | 570 (59.9) | 15 (50) | |||
| High | 117 (7.5) | 48 (9.1) | 3 (6.1) | 64 (6.7) | 2 (6.7) | |||
| Family situation, N (%) | ||||||||
| Married parents | 1144 (77.1) | 382 (76.2) | 36 (73.5) | 709 (78.3) | 17 (60.7) | 15.95 | - | - |
| Divorced parents | 309 (20.8) | 109 (21.8) | 13 (26.5) | 176 (19.4) | 11 (39.3) | |||
| Unmarried parents living together | 8 (0.5) | 0 (0) | 0 (0) | 8 (0.9) | 0 (0) | |||
| Single parent | 21 (1.4) | 10 (2) | 0 (0) | 11 (1.2) | 0 (0) | |||
| Orphan | 1 (0.1) | 0 (0) | 0 (0) | 1 (0.1) | 0 (0) | |||
| Behavioral intentions, M ± SD | ||||||||
| Seek condoms | 3.62 ± 1.36 | 4.10 ± 0.95 | 1.20 ± 0.40 | 1.83 ± 0.98 | 3.62 ± 1.36 | 111.10 *** | 0.17 | 1 > 2 1 > 3 1 > 4 3 > 2 4 > 3 |
| Condom use | 4.45 ± 0.96 | 4.46 ± 0.75 | 1.20 ± 0.40 | 4.68 ± 0.60 | 1.76 ± 0.43 | 610.22 *** | 0.54 | 1 > 2 3 > 1 1 > 4 3 > 2 4 > 2 3 > 4 |
| Negotiate condom use | 4.27 ± 1.07 | 4.19 ± 0.97 | 1.37 ± 0.72 | 4.53 ± 0.80 | 2.13 ± 1.07 | 269.08 *** | 0.34 | 1 > 2 3 > 1 1 > 4 3 > 2 4 > 2 3 > 4 |
| Have sex under alcohol influence | 2.18 ± 1.15 | 3.45 ± 0.70 | 1.16 ± 0.37 | 1.50 ± 0.62 | 3.30 ± 1.14 | 1069.65 *** | 0.67 | 1 > 2 1 > 3 3 > 2 4 > 2 4 > 3 |
| Have sex under drugs influence | 1.47 ± 0.94 | 2.06 ± 1.24 | 1.14 ± 0.35 | 1.12 ± 0.36 | 2.87 ± 1.54 | 184.23 *** | 0.26 | 1 > 2 1 > 3 4 > 1 4 > 2 4 > 3 |
| Sexually experienced *, N (%) | 506 (32.5) | 235 (44.6) | 14 (28.6) | 239 (25.1) | 18 (60) | 69.35 *** | 0.21 | 4 > 1 4 > 3 1 > 3 |
| Percentage of condom use, M ± SD | 85.13 (22.65) | 86.50 (20.05) | 50 (33.41) | 85.60 (23.18) | 56.42 (36.82) | 7.59 *** | 0.05 | 1 > 2 1 > 4 3 > 2 3 > 4 |
| Class 1 “Condom + Drugs” | Class 2 “Abstinent” | Class 3 “Condom + No Drugs” | Class 4 “No Condom + Drugs” | |
|---|---|---|---|---|
| n = 527 | n = 49 | n = 951 | n = 30 | |
| RPR [95% CI] | RPR [95% CI] | RPR [95% CI] | RPR [95% CI] | |
| Reference: Class 1 | ||||
| Sex | - | 2.36 [0.16, 33.95] | 0.29 [0.18, 0.47] *** | 1.69 [0.17, 16.28] |
| Age | - | 0.48 [0.12, 1.83] | 0.89 [0.70, 1.15] | 0.49 [0.19, 1.28] |
| Educational level | - | |||
| 1 = 9th grade | - | 1.30 [0, 2.30] | 0.93 [0.47, 1.86] | 0.27 [0.02, 2.74] |
| 2 = 10th grade | - | 1.92 [0.16, 22.09] | 0.97 [0.54, 1.74] | 0.22 [0.02, 2.50] |
| 3 = ref. | - | - | - | - |
| Sexual experience | - | 3.23 [0] | 0.79 [0.31, 2.02] | 1.22 [0.11, 12.75] |
| Condom use | - | 0.95 [0.91, 0.98] ** | 0.99 [0.98, 1.01] | 0.96 [0.93, 0.98] ** |
| Reference: Class 2 | ||||
| Sex | 0.42 [0.02, 6.09] | - | 0.12 [0.009, 1.81] | 0.72 [0.02, 21.96] |
| Age | 2.05 [0.54, 7.75] | - | 1.85 [0.49, 6.97] | 1.01 [0.20, 5.05] |
| Educational level | - | |||
| 1 = 9th grade | >99 ***a | - | >99 ***a | >99 ***a |
| 2 = 10th grade | 0.51 [0.04, 5.95] | - | 0.50 [0.04, 5.86] | 0.11 [0.004, 3.26] |
| 3 = ref. | - | - | - | - |
| Sexual experience | >99 ***a | - | >99 ***a | >99 ***a |
| Condom use | 1.05 [1.01, 1.09] ** | - | 1.05 [1.01, 1.09] ** | 1.01 [0.20, 5.05] |
| Reference: Class 3 | ||||
| Sex | 3.34 [2.11, 5.29] *** | 7.90 [0.55, 113.18] | - | 5.68 [0.59, 54.17] |
| Age | 1.11 [0.86, 1.42] | 0.95 [0.91, 0.98] ** | - | 0.55 [0.21, 1.43] |
| Educational level | - | |||
| 1 = 9th grade | 1.06 [0.53, 2.11] | 1.39 [0] | - | 0.29 [0.03, 2.96] |
| 2 = 10th grade | 1.02 [0.57, 1.84] | 1.97 [0.17, 22.95] | - | 0.23 [0.02, 2.59] |
| 3 = ref. | - | - | - | - |
| Sexual experience | 1.26 [0.49, 3.22] | 4.08 [4.08, 4.08] | - | 1.55 [0.14, 16.68] |
| Condom use | 1 [0.99, 1.01] | 0.95 [0.91, 0.98] ** | - | 0.96 [0.94, 0.98] ** |
| Reference: Class 4 | ||||
| Sex | 0.58 [0.06, 5.64] | 1.39 [0.04, 42.43] | 0.17 [0.01, 1.67] | - |
| Age | 2.02 [0.77, 5.27] | 0.98 [0.19, 4.89] | 1.03 [1.01, 1.06]** | - |
| Educational level | - | |||
| 1 = 9th grade | 3.58 [0.36, 35.22] | 4.69 [0] | 3.36 [0.33, 33.61] | - |
| 2 = 10th grade | 4.36 [0.40, 47.68] | 8.41 [0.30, 230.76] | 4.25 [0.38, 46.89] | - |
| 3 = ref. | - | - | - | - |
| Sexual experience | 0.81 [0.07, 8.47] | 2.63 [2.63, 2.63] | 0.64 [0.06, 6.94] | - |
| Condom use | 1.03 [1.01, 1.06] ** | 0.98 [0.19, 4.89] | 1.03 [1.01, 1.06] ** | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morales, A.; Tomczyk, S.; Orgilés, M.; Espada, J.P. “Who Are at Higher Sexual Risk?” Latent Class Analysis of Behavioral Intentions among Spanish Adolescents. Int. J. Environ. Res. Public Health 2021, 18, 1855. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041855
Morales A, Tomczyk S, Orgilés M, Espada JP. “Who Are at Higher Sexual Risk?” Latent Class Analysis of Behavioral Intentions among Spanish Adolescents. International Journal of Environmental Research and Public Health. 2021; 18(4):1855. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041855
Chicago/Turabian StyleMorales, Alexandra, Samuel Tomczyk, Mireia Orgilés, and José Pedro Espada. 2021. "“Who Are at Higher Sexual Risk?” Latent Class Analysis of Behavioral Intentions among Spanish Adolescents" International Journal of Environmental Research and Public Health 18, no. 4: 1855. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18041855