
The Unmet Needs of Community-Dwelling Stroke Survivors: A Systematic Review of Qualitative Studies

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Protocol and Registration
2.2. Search Strategy
- -
- Stroke (cva* or stroke* or poststroke* or post-stroke* or post stroke* or transient ischemic attack* or TIA* or ministroke* or mini stroke* or SAH or cerebral or cerebellar or brain* or vertebrobasilar or infarct* or ischemi* or thrombo* or apoplexy or emboli*);
- -
- Needs (need* or demand* or requirement* or wish* or experience or challenge*);
- -
- Community (community or home or outpatient*).
2.3. Selection Criteria
2.4. Selection of Articles for Inclusion
2.5. Data Extraction
2.6. Data Synthesis
2.7. Assessment Quality of Involved Studies
3. Results
3.1. Characteristics of Included Study
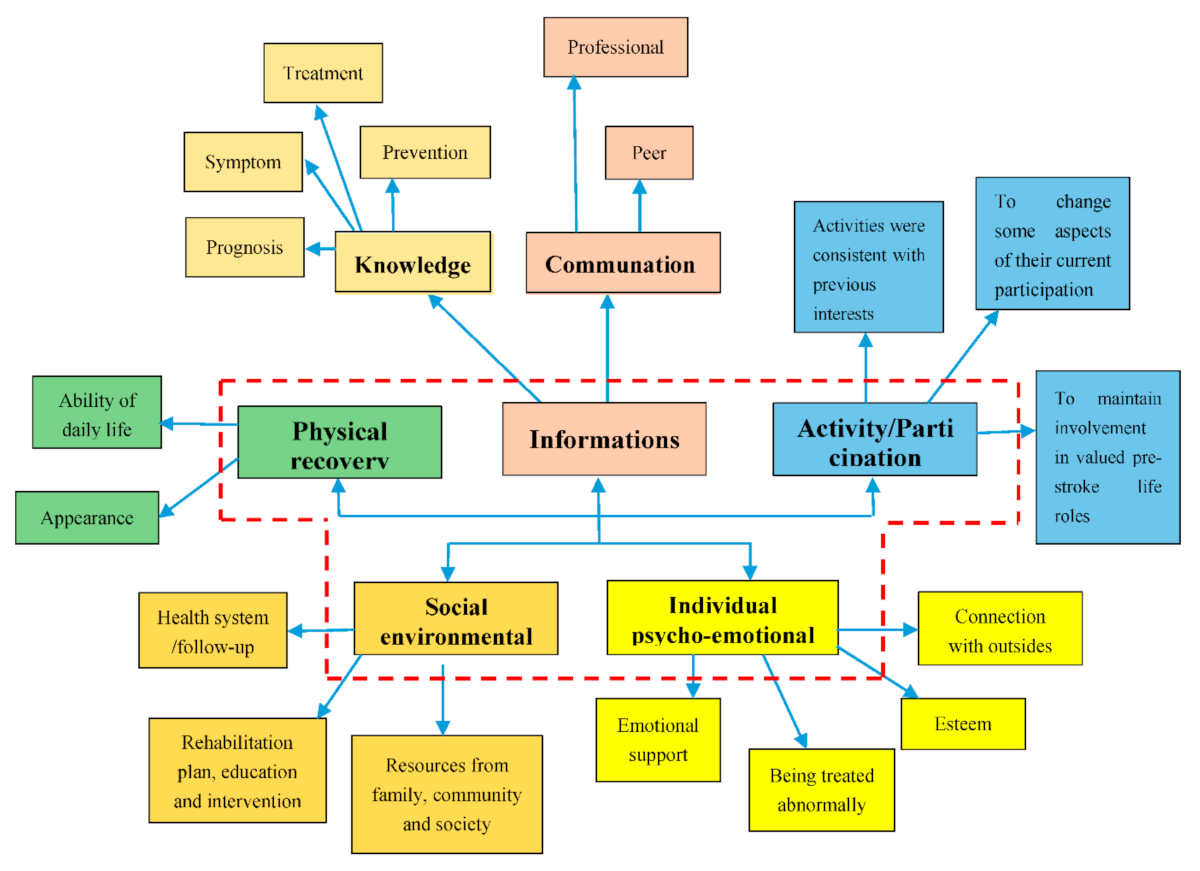
3.2. Meta-Synthesis
3.2.1. Stroke People in Community Have Unmet Needs for Disease-Related Information
Unmet Needs around Knowledge of Stroke Symptom, Treatment, Prevention, and Prognosis
Unmet Needs Regarding Information on Communication with Professional and Peer
3.2.2. Stroke People Have Unmet Physical Recovery and Activity/Participation Needs
Unmet Activity/Participation Needs
Unmet Physical Recovery Needs
3.2.3. Stroke People Have Unmet Needs for Social Environmental Resources
Unmet Health System/Follow-up Needs from Professionals
Unmet Family, Community, and Social Needs for Environment Resources
Unmet Rehabilitation Plan, Education, and Intervention Needs
3.2.4. Stroke People Have Unmet Individual Psycho-Emotional Support Needs
4. Discussion
Strengths and Limitations
5. Conclusions
- (1)
- Developing a management program for community-dwelling stroke survivors who do not live in institutionalized organizations to build a communication channel for patients and professionals.
- (2)
- It is necessary to provide scientific participation/daily activity/ physical recovery plans for patients with personalized unmet needs, which is the patient’s insurmountable knowledge gap especially for stroke survivors who have no access to professionals.
- (3)
- Regular comprehensive assessment, not only physical needs but psycho-emotional and social environmental resources, plus individual evaluation of unmet needs.
- (4)
- A long-term, continuous health service, which could propose practical suggestions or assistances.
- (5)
- We need to identify short-term needs and long-term needs, that is to say, some unmet needs may disappear after efforts while some unmet needs may reappear soon.
- (6)
- We need to compare the unmet needs from various perspectives (e.g., professional, caregivers, family members). To some extent, the perspectives from patients or caregivers are inconsistent with those of professionals. Then, we may design optimal coping strategies.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data availability statement
Conflicts of Interest
References
- Villa, R.F.; Ferrari, F.; Moretti, A. Post-stroke depression: Mechanisms and pharmacological treatment. Pharmacol. Ther. 2018, 184, 131–144. [Google Scholar] [CrossRef]
- Feigin, V.L.; Roth, G.A.; Naghavi, M.; Parmar, P.; Krishnamurthi, R.; Chugh, S.; Mensah, G.A.; Norrving, B.; Shiue, I.; Ng, M.; et al. Global burden of stroke and risk factors in 188 countries, during 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet Neurol. 2016, 15, 913–924. [Google Scholar] [CrossRef] [Green Version]
- Global Health Data Exchange. Global Burden of Disease Study 2017 (GBD 2017) Results [EB/OL]. Available online: http://ghdx.healthdata.org/gbd-results-tool (accessed on 20 March 2020).
- Avan, A.; Digaleh, H.; Napoli, M.D.; Stranges, S.; Behrouz, R.; Shojaeianbabaei, G.; Amiri, A.; Tabrizi, R.; Mokhber, N.; Spence, J.D.; et al. Socioeconomic status and stroke incidence, prevalence, mortality, and worldwide burden: An ecological analysis from the Global Burden of Disease Study 2017. BMC Med. 2019, 17, 191. [Google Scholar] [CrossRef] [PubMed]
- Thrift, A.G.; Thayabaranathan, T.; Howard, G.; Howard, V.J.; Rothwell, P.M.; Feigin, V.L.; Norrving, B.; Donnan, G.A.; Cadilhac, D.A. Global stroke statistics. Int. J. Stroke. 2017, 9, 13–32. [Google Scholar] [CrossRef]
- Mayo, N.E.; Hendlisz, J.; Goldberg, M.S.; Korner-Bitensky, N.; Becker, R.; Coopersmith, H. Destinations of stroke patients discharged from the Montreal area acute-care hospitals. Stroke 1989, 20, 351–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bettger, J.P.; Mccoy, L.; Smith, E.E.; Fonarow, G.C.; Schwamm, L.H.; Peterson, E.D. Contemporary Trends and Predictors of Postacute Service Use and Routine Discharge Home After Stroke. J. Am. Heart Assoc. 2015, 4, e001038. [Google Scholar] [CrossRef] [Green Version]
- Vecchia, C.D.; Préau, M.; Carpentier, C.; Viprey, M.; Haesebaert, J.; Termoz, A.; Dima, A.L.; Schott, A. Illness beliefs and emotional responses in mildly disabled stroke survivors: A qualitative study. PLoS ONE 2019, 14, e223681. [Google Scholar]
- Chen, Y.; Abel, K.T.; Janecek, J.T.; Chen, Y.; Zheng, K.; Cramer, S.C. Home-based technologies for stroke rehabilitation: A systematic review. Int. J. Med. Inf. 2019, 123, 11–22. [Google Scholar] [CrossRef]
- Mabire, C.; Bachnick, S.; Ausserhofer, D.; Simon, M. Patient readiness for hospital discharge and its relationship to discharge preparation and structural factors: A cross-sectional study. Int. J. Nurs. Stud. 2019, 90, 13–20. [Google Scholar] [CrossRef]
- Condon, C.; Lycan, S.; Duncan, P.; Bushnell, C. Reducing Readmissions after Stroke with a Structured Nurse Practitioner/Registered Nurse Transitional Stroke Program. Stroke 2016, 47, 1599–1604. [Google Scholar] [CrossRef] [Green Version]
- Mckevitt, C.; Fudge, N.; Redfern, J.; Sheldenkar, A.; Crichton, S.; Rudd, A.R.; Forster, A.; Young, J.; Nazareth, I.; Silver, L.E.; et al. Self-Reported Long-Term Needs After Stroke. Stroke 2011, 42, 1398–1403. [Google Scholar] [CrossRef] [Green Version]
- Andrew, N.E.; Kilkenny, M.; Naylor, R.; Purvis, T.; Lalor, E.; Moloczij, N.; Cadilhac, D.A. Understanding long-term unmet needs in Australian survivors of stroke. Int. J. Stroke 2014, A100, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Hawks, L.; Himmelstein, D.U.; Woolhandler, S.; Bor, D.H.; Gaffney, A.; McCormick, D. Trends in Unmet Need for Physician and Preventive Services in the United States, 1998–2017. JAMA Intern. Med. 2020, 180, 439. [Google Scholar] [CrossRef] [PubMed]
- Abrahamson, V.; Wilson, P.M. How unmet are unmet needs post-stroke? A policy analysis of the six-month review. BMC Health Serv. Res. 2019, 19, 480. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Olaiya, M.T.; Cadilhac, D.A.; Kim, J.; Nelson, M.R.; Srikanth, V.K.; Andrew, N.E.; Bladin, C.F.; Gerraty, R.P.; Fitzgerald, S.M.; Phan, T.; et al. Long-term unmet needs and associated factors in stroke or TIA survivors. Neurology 2017, 89, 68–75. [Google Scholar] [CrossRef]
- Jamison, J.; Ayerbe, L.; Di Tanna, G.L.; Sutton, S.; Mant, J.; De Simoni, A. Evaluating practical support stroke survivors get with medicines and unmet needs in primary care: A survey. BMJ Open 2018, 8, e19874. [Google Scholar] [CrossRef] [Green Version]
- Vincent, C.; Deaudelin, I.; Robichaud, L.; Rousseau, J.; Viscogliosi, C.; Talbot, L.R.; Desrosiers, J. Rehabilitation needs for older adults with stroke living at home: Perceptions of four populations. BMC Geriatr. 2007, 7, 20. [Google Scholar] [CrossRef] [Green Version]
- Appalasamy, J.R.; Subramanian, P.; Tan, K.M.; Seeta Ramaiah, S.; Joseph, J.P.; Chua, S.S. The Needs and Barriers of Medication-Taking Self-Efficacy among Poststroke Patients: Qualitative Study. JMIR Nursing 2019, 2, e14399. [Google Scholar] [CrossRef]
- Luker, J.; Lynch, E.; Bernhardsson, S.; Bennett, L.; Bernhardt, J. Stroke Survivors’ Experiences of Physical Rehabilitation: A Systematic Review of Qualitative Studies. Arch. Phys. Med. Rehabil. 2015, 96, 1698–1708. [Google Scholar] [CrossRef]
- Peoples, H.; Satink, T.; Steultjens, E. Stroke survivors’ experiences of rehabilitation: A systematic review of qualitative studies. Scand. J. Occup. Ther. 2011, 18, 163–171. [Google Scholar] [CrossRef]
- Aziz, N.A.; Pindus, D.M.; Mullis, R.; Walter, F.M.; Mant, J. Understanding stroke survivors’ and informal carers’ experiences of and need for primary care and community health services—A systematic review of the qualitative literature: Protocol. BMJ Open 2016, 6, e009244. [Google Scholar] [CrossRef]
- Luker, J.; Murray, C.; Lynch, E.; Bernhardsson, S.; Shannon, M.; Bernhardt, J. Carers’ Experiences, Needs, and Preferences during Inpatient Stroke Rehabilitation: A Systematic Review of Qualitative Studies. Arch. Phys. Med. Rehabil. 2017, 98, 1852–1862. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, N.; Mackenzie, A.; Cloud, G.C.; Wilson, N. Informal primary carers of stroke survivors living at home–challenges, satisfactions and coping: A systematic review of qualitative studies. Disabil. Rehabil. 2009, 31, 337–351. [Google Scholar] [CrossRef] [PubMed]
- Mckevitt, C.; Redfern, J.; Mold, F.; Wolfe, C. Qualitative Studies of Stroke. Stroke 2004, 35, 1499–1505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, T.; Zhang, B.; Deng, Y.; Fan, J.; Zhang, L.; Song, F. Long-term unmet needs after stroke: Systematic review of evidence from survey studies. BMJ Open 2019, 9, e28137. [Google Scholar] [CrossRef]
- Lin, B.; Ding, C.; Mei, Y.; Wang, P.; Ma, F.; Zhang, Z.X. Unmet care needs of community-dwelling stroke survivors: A protocol for systematic review and theme analysis of quantitative and qualitative studies. BMJ Open 2019, 9, e29160. [Google Scholar] [CrossRef] [PubMed]
- Joanna Briggs Institute. JBI Critical Appraisal Instrument for Qualitative Research [EB/OL]. Available online: https://wiki.joannabriggs.org/display/MANUAL/2.6.6+Assessment+of+methodological+quality (accessed on 29 March 2020).
- Pearson, M. Synthesizing Qualitative and Quantitative Health Evidence: A Guide to Methods; Pope, C., Mays, N., Popay, J., Eds.; Blackwell Publishing Ltd.: Oxford, UK, 2008; Volume 30, pp. 330–331. [Google Scholar]
- Thomas, J.; Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med. Res. Methodol. 2008, 8, 45. [Google Scholar] [CrossRef] [Green Version]
- Geyh, S.; Cieza, A.; Schouten, J.; Dickson, H.; Frommelt, P.; Omar, Z.; Kostanjsek, N.; Ring, H.; Stucki, G. ICF Core Sets for stroke. J. Rehabil. Med. 2004, 44, 135–141. [Google Scholar] [CrossRef]
- Karam, M.; Brault, I.; Van Durme, T.; Macq, J. Comparing interprofessional and interorganizational collaboration in healthcare: A systematic review of the qualitative research. Int. J. Nurs. Stud. 2018, 79, 70–83. [Google Scholar] [CrossRef] [PubMed]
- Lutz, B.J.; Young, M.E.; Cox, K.J.; Martz, C.; Creasy, K.R. The crisis of stroke: Experiences of patients and their family caregivers. Top. Stroke Rehabil. 2011, 18, 786–797. [Google Scholar] [CrossRef]
- Salisbury, L.; Wilkie, K.; Bulley, C.; Shiels, J. ‘After the stroke’: Patients’ and carers’ experiences of healthcare after stroke in Scotland. Health Soc. Care Community 2010, 18, 424–432. [Google Scholar] [CrossRef]
- Pringle, J.; Hendry, C.; Mclafferty, E.; Drummond, J. Stroke survivors with aphasia: Personal experiences of coming home. Br. J. Community Nurs. 2010, 15, 241–243, 245–247. [Google Scholar] [CrossRef] [PubMed]
- Wiles, R.; Pain, H.; Buckland, S.; McLellan, L. Providing appropriate information to patients and carers following a stroke. J. Adv. Nurs. 1998, 28, 794–801. [Google Scholar] [CrossRef]
- Mclean, J.; Roper-Hall, A.; Mayer, P.; Main, A. Service needs of stroke survivors and their informal carers: A pilot study. J. Adv. Nurs. 1991, 16, 559–564. [Google Scholar] [CrossRef] [PubMed]
- Yeung, E.H.L.; Szeto, A.; Richardson, D.; Lai, S.; Lim, E.; Cameron, J.I. The experiences and needs of Chinese-Canadian stroke survivors and family caregivers as they re-integrate into the community. Health Soc. Care Community 2015, 23, 523–531. [Google Scholar] [CrossRef]
- Kjork, E.K.; Gunnel, C.; Lundgren-Nilsson, A.; Sunnerhagen, K.S. Experiences, needs, and preferences for follow-up after stroke perceived by people with stroke and healthcare professionals: A focus group study. PLoS ONE 2019, 14, e223338. [Google Scholar] [CrossRef]
- Liddle, J.; Turpin, M.; Mckenna, K.; Kubus, T.; Lambley, S.; McCaffrey, K. The Experiences and Needs of People Who Cease Driving after Stroke. Brain Impair. 2009, 10, 271–281. [Google Scholar] [CrossRef]
- Klinke, M.E.; Hafsteinsdottir, T.B.; Thorsteinsson, B.; Jonsdottir, H. Living at home with eating difficulties following stroke: A phenomenological study of younger people’s experiences. J. Clin. Nurs. 2014, 23, 250–260. [Google Scholar] [CrossRef] [Green Version]
- White, J.H.; Patterson, K.; Jordan, L.A.; Magin, P.; Attia, J.; Sturm, J.W. The experience of urinary incontinence in stroke survivors: A follow-up qualitative study. Can. J. Occup. Ther. 2014, 81, 124–134. [Google Scholar] [CrossRef] [PubMed]
- Gard, G.; Pessah-Rasmussen, H.; Brogårdh, C.; Nilsson, Å.; Lindgren, I. Need for structured healthcare organization and support for return to work after stroke in Sweden: Experiences of stroke survivors. J. Rehabil. Med. 2019, 51, 741–748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poulin, V.; Carbonneau, H.; Provencher, V.; Rochette, A.; Giroux, D.; Verreault, C.; Turcotte, S. Participation in leisure activities to maintain cognitive health: Perceived educational needs of older adults with stroke. Soc. Leis. Soc. Particip. Leis. Act. Aging/Loisir et Société/Particip. Soc. Loisir et Vieil. Act. 2019, 42, 4–23. [Google Scholar] [CrossRef]
- Davoody, N.; Koch, S.; Krakau, I.; Hagglund, M. Post-discharge stroke patients’ information needs as input to proposing patient-centred eHealth services. BMC Med. Inform. Decis. Mak. 2016, 16, 66. [Google Scholar] [CrossRef] [Green Version]
- Pappadis, M.R.; Krishnan, S.; Hay, C.C.; Jones, B.; Sander, A.M.; Weller, S.C.; Reistetter, T.A. Lived experiences of chronic cognitive and mood symptoms among community-dwelling adults following stroke: A mixed-methods analysis. Aging Ment. Health. 2019, 23, 1227–1233. [Google Scholar] [CrossRef]
- Shipley, J.; Luker, J.; Thijs, V.; Bernhardt, J. The personal and social experiences of community-dwelling younger adults after stroke in Australia: A qualitative interview study. BMJ Open 2018, 8, e23525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shannon, R.L.; Forster, A.; Hawkins, R.J. A qualitative exploration of self-reported unmet need one year after stroke. Disabil. Rehabil. 2016, 38, 2000–2007. [Google Scholar] [CrossRef]
- Taule, T.; Strand, L.I.; Skouen, J.S.; Råheim, M. Striving for a life worth living: Stroke survivors’ experiences of home rehabilitation. Scand. J. Caring Sci. 2015, 29, 651–661. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simeone, S.; Savini, S.; Cohen, M.Z.; Alvaro, R.; Vellone, E. The experience of stroke survivors three months after being discharged home: A phenomenological investigation. Eur. J. Cardiovasc. Nurs. 2014, 14, 162–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinsen, R.; Kirkevold, M.; Sveen, U. Young and Midlife Stroke Survivors’ Experiences with the Health Services and Long-Term Follow-Up Needs. J. Neurosci. Nurs. 2015, 47, 27–35. [Google Scholar] [CrossRef] [Green Version]
- White, J.; Dickson, A.; Magin, P.; Tapley, A.; Attia, J.; Sturm, J.; Carter, G. Exploring the experience of psychological morbidity and service access in community dwelling stroke survivors: A follow-up study. Disabil. Rehabil. 2014, 36, 1600–1607. [Google Scholar] [CrossRef] [PubMed]
- Medin, J.; Larson, J.; von Arbin, M.; Wredling, R.; Tham, K. Elderly persons’ experience and management of eating situations 6 months after stroke. Disabil. Rehabil. 2010, 32, 1346–1353. [Google Scholar] [CrossRef] [Green Version]
- Lutz, B.J.; Chumbler, N.R.; Roland, K. Care Coordination/Home-Telehealth for Veterans with Stroke and Their Caregivers: Addressing an Unmet Need. Top. Stroke Rehabil. 2007, 14, 32–42. [Google Scholar] [CrossRef]
- Atler, K. The experiences of everyday activities post-stroke. Disabil. Rehabil. 2016, 38, 781–788. [Google Scholar] [CrossRef] [PubMed]
- King, A.J.L.; Evans, M.; Moore, T.H.M.; Paterson, C.; Sharp, D.; Persad, R.; Huntley, A.L. Prostate cancer and supportive care: A systematic review and qualitative synthesis of men’s experiences and unmet needs. Eur. J. Cancer Care 2015, 24, 618–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallacher, K.; Morrison, D.; Jani, B.; Macdonald, S.; May, C.R.; Montori, V.M. Uncovering Treatment Burden as a Key Concept for Stroke Care: A Systematic Review of Qualitative Research. PLoS Med. 2013, 6, e1001473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eames, S.; Hoffmann, T.; Worrall, L.; Read, S. Delivery styles and formats for different stroke information topics: Patient and carer preferences. Patient Educ. Couns. 2010, 84, e18–e23. [Google Scholar] [CrossRef] [PubMed]
- Walters, K.; Iliffe, S.; Orrell, M. An exploration of help-seeking behaviour in older people with unmet needs. Fam. Pract. 2001, 18, 277–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hou, S. Health Education: Theoretical Concepts, Effective Strategies and Core Competencies; SAGE Publications: Los Angeles, CA, USA, 2014; Volume 15, pp. 619–621. [Google Scholar]
- Segan, J.D.; Briggs, A.M.; Chou, L.; Connelly, K.L.; Seneviwickrama, M.; Sullivan, K.; Cicuttini, F.M.; Wluka, A.E. Patient-perceived health service needs in inflammatory arthritis: A systematic scoping review. Semin. Arthritis Rheum. 2018, 47, 765–777. [Google Scholar] [CrossRef] [Green Version]
- Satink, T.; Cup, E.H.; Ilott, I.; Prins, J.; De Swart, B.J.; Nijhuis-van Der Sanden, M.W. Patients‘ Views on the Impact of Stroke on Their Roles and Self: A Thematic Synthesis of Qualitative Studies. Arch. Phys. Med. Rehabil. 2013, 94, 1171–1183. [Google Scholar] [CrossRef]
- Wottrich, A.W.; Åström, K.; Löfgren, M. On parallel tracks: Newly home from hospital-people with stroke describe their expectations. Disabil. Rehabil. 2012, 34, 1218–1224. [Google Scholar] [CrossRef]
- Harrison, M.; Ryan, T.; Gardiner, C.; Jones, A. Psychological and emotional needs, assessment, and support post-stroke: A multi-perspective qualitative study. Top. Stroke Rehabil. 2017, 24, 119–125. [Google Scholar] [CrossRef]
- Valery, P.C.; Powell, E.; Moses, N.; Volk, M.L.; McPhail, S.M.; Clark, P.J.; Martin, J. Systematic review: Unmet supportive care needs in people diagnosed with chronic liver disease. BMJ Open 2015, 5, e7451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moghaddam, N.; Coxon, H.; Nabarro, S.; Hardy, B.; Cox, K. Unmet care needs in people living with advanced cancer: A systematic review. Support Care Cancer 2016, 24, 3609–3622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Groeneveld, I.F.; Arwert, H.J.; Goossens, P.H.; Vliet Vlieland, T.P.M. The Longer-term Unmet Needs after Stroke Questionnaire: Cross-Cultural Adaptation, Reliability, and Concurrent Validity in a Dutch Population. J. Stroke Cerebrovasc. Dis. 2018, 27, 267–275. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| First Author | Country | Population | Methodology | Data Collection | Research Content | Total Unmet Needs |
|---|---|---|---|---|---|---|
| Valérie Poulin [44] 2019 | Canada | 20 community-dwelling stroke people; range 60–88 years; discharged from rehabilitation units >12 months | Framework analysis | Mixed methods. Semi-structured interviews | Educational needs for support their participation in leisure activities | Tools and resources promoting active involvement, interactions, and opportunities for choice and control; engage in different personally meaningful activities; follow-up to address their educational needs with respect to participation in leisure activities that promote cognitive health. |
| Monique R. Pappadis [46] 2018 | United States | 40 community-dwelling older adults at least one-year post stroke; average (43% of the sample was 1–2 years post stroke) 65.1 years | Thematic content analysis | Mixed methods. Semi-structured interviews | Chronic post-stroke cognition and mood symptoms and goals | Unmet need for cognition or mood-related treatment prevailing need for additional speech/language services |
| Emma K. Kjo¨rk [39] 2019 | Sweden | 18 patients; range, 3 months to 7 years since stroke | Framework analysis | Focus group | Barriers to access appropriate treatment and support included difficulties in communicating one’s needs and lack of coherent follow-up | Equal access to health care services to satisfy their communicating needs; receiving support for avoiding negative feelings (e.g., emptiness and abandonment); need for comprehensive, planned, and tailored follow-up |
| Gunvor GARD [43] 2019 | Sweden | 20 Participants aged 52 (39–62); in 180 days after stroke onset. | Content analysis | Focus group | To explore stroke survivors’ experiences of healthcare-related facilitators and barriers concerning return to work after stroke. | Adequate rehabilitation content and timing facilitated return to work (RTW); lack of early information, regular contact, and a rehabilitation plan were barriers to RTW; insufficient communication between rehabilitation actors hindered RTW; lack of practical help and psychological support the family were barriers to RTW; requesting rehabilitation planning, healthcare information and coordination |
| Jamuna Rani Appalasamy [19] 2019 | Malaysia | 10 informants, aged 57(44–78) years, no detail period post-stroke | Inductive thematic analysis | In-depth individual interviews | To determine the fundamental needs and barriers of medication-taking self-efficacy | To gain insight into stroke recurrence and rationalize how the stroke occurred and why they must adhere to preventative medications. |
| Abrahamson, Vanessa [15] 2019 | England | 46 patients aged 28–88 years; 24 were followed for 6–12 months, 15 for 12–18 months, and 7 for less than 6 months. | Thematic analysis | Semi-structured interviews | To explore needs identified by patients | More intensity, frequency and duration of therapy; Information concerned with resuming work to work and financial; the need for ongoing support linked with the need for education along the care pathway; be referred to appropriate specialists when symptoms happened |
| Jessica Shipley [47] 2018 | Australia | 19 young participants aged 19 to 54 years at diagnosis and ranged from 6 months to 24 years post-stroke. | Rigorous qualitative descriptive analysis | In-depth semi-structured interviews | To examine the personal and social experiences of younger adults after stroke | Desiring normality and belonging; need for increased awareness of the many faces and forms of stroke |
| Shannon R.L [48] 2016 | England | 10 participants 78 (70–95) average 11 months after stroke | Thematic analysis | Semi-structured interviews | To identify stroke-survivor unmet needs | Information regarding other stroke people; communication with family doctor and peers |
| Nadia Davoody [45] 2016 | Sweden | 4 participants aged 65–85, time from first stroke >10 years | Content analysis | Focus groups | To explore post-discharge stroke patients’ information needs | To have access to health-related information concerned with their care and rehabilitation processes; Practical guidance through health care and community services. |
| Emily H. L [38] 2015 | Canada | 5 stroke survivors aged 68 (53–69), Months post discharge 6 (0.5–9) | Framework analysis | In-depth interviews | To determine the experiences and needs of Chinese stroke survivors and family caregivers as they return to community living | Information and training needs during the rehabilitation and return to community living phases; care environments adopted their original culture (communication with professionals, traditional Chinese healing methods, Chinese diet) |
| Tina Taule [49] 2015 | Norway | 8 participants (45–80 years), discharge from hospital<6 months | Framework analysis | Semi-structured interviews | To explore mild-to-moderate stroke survivors’ experiences | Hope for a life worth living (continued engagement in activities, altered body and emotional reactions); the trauma of a changed body: making sense of emotional Reactions (questions about uncertainties of life and death, e.g., being afraid of having another stroke); the challenge of cultivating mutual confidence |
| Silvio Simeone [50] 2014 | Italy | 15 patients aged 70 (34– 85 years); three months after being discharged home | Phenomenological methodology | Survey with open-ended question | To describe the experience of stroke survivors © | Need stay at safety; The house suit to my situations, physical and cognitive recovery; |
| Randi Martinsen [51] 2015 | Norway | 16 patients aged 48 (21–67 years) (8 patients had lived with the stroke for approximately 1.5 years. The other 8 participants had experienced stroke from 2 to 10 years) | Hermeneutic-phenomenological analysis | In-depth qualitative interviews | To explore young and midlife stroke survivors’ experiences with the health services and to identify long-term follow-up needs | To gain access to follow-up health services tailoring to the individual (e.g., sufficient information, timely and management intervention, instead of examination only); follow-up system had to be flexible to suit their family life situation and disease severity. |
| Jennifer H. White [42] 2014 | Australia | 8 participants with UI aged 69 to 88 years; in 4 years since first stroke. | Thematic analysis | Semi-structured interviews | To determine the experiences of community-dwelling stroke survivors living with UI/PSU | Insufficient advice and information from the health system to manage the unpredictable and persisting nature of UI/PSUI symptoms |
| Jennifer White [52] 2014 | Australia | 14 responders aged 73.43 (58–89) with an average of three years post-stroke | Grounded theory | Semi-structured interviews | To explore the physical and psycho-social functioning status of stroke survivors beyond 12 months post-stroke and to qualitatively explore the longer-term experiences of psychological morbidity and service access needs | Rely on other people to assist in maintaining involvement in valued pre-stroke life roles; management, monitoring, and interventions about symptoms; to access needed services when services and information were limited |
| Marianne E Klinke [41] 2014 | Iceland | 7 stroke survivors aged 53 (34–64) with eating difficulties; mean three years since the stroke | Phenomenological | In-depth interviews | To explore and describe the experience of eating and eating-related difficulties in stroke survivors living at home | Individualized long-term support from family; eating normally and safely not only at home; to maintain a good outward façade and to eat in a socially acceptable way |
| Barbara J. Lutz [33] 2011 | America | 19 recovering stroke patients, no detail period post-stroke | Grounded theory | Group and individual interview | To explore the needs of stroke patients and their family caregivers | Keep safety with the help of family (e.g., falling, picking up something); need for assistance with ADLs and IADLs; the support of family and/or friends |
| L. Salisbury [34] 2010 | America | 13 patients aged 64.37 (43–75 years), mean time since stroke was 4.63 years; | Interpretative phenomenological analysis | Semi-structured interviews | To explore stroke patients and cares’ experiences of the healthcare system | Positive community rehabilitation services; required encouragement to access leisure facilities and activity; enough follow up and backup car; continuous services and intervention |
| Jan Pringle [35] 2010 | England | 4 patients with aphasia, over 18 years of age, one month after discharge | Phenomenological approach | In-depth interviews and self-report diaries | To explore personal experiences of coming home | Talking with the therapists; having a reliance on others to fill limited ability; follow-up is still expected |
| J Ö RGEN MEDIN [53] 2010 | Sweden | 13 participants 6 months after last stroke | Grounded theory | Semi-structured interviews | To explore the experience and management of eating situations among persons affected by stroke | No embarrassing and undesirable due to needing help about eating; mastering of eating situations in front of unfamiliar people |
| Jacki Liddle [40] 2009 | Australia | 24 participants who had ceased driving, mean of 5.5 years following a stroke, aged 67 (50–83 years) | Phenomenological approach | Semi-structured interviews | To explore the needs and experiences of people who cease driving following a stroke | Information sharing was less effective in early recovery; a detailed explanation of stopping driving not just according to the renewal form; a lack of follow-up regarding the driving cessation process by health professionals; a lack of information given regarding alternative transport options and safely return to driving; the need for different types of transport and other lifestyle changes |
| Claude Vincent [18] 2007 | Canada | 17 persons aged from 65 to 85 years with over two years history | Framework analysis | Focus group | To explore partially met and unmet rehabilitation needs of older adults | Receiving home care assistance from the public health care system; motor activities |
| Rose Wiles [36] 1998 | England | 8 patients, no detail of age, 2–12 months post-discharge | Grounded theory | Semi-structured interview | To identify a range of information needs that patients and carers may have at three different phases post-stroke | Need for practical information relating to coping with day-to-day activities both in and outside the home; information regarding house adaptations; equipment and the services and resources available in the community. |
| Jacqueline McLean [37] 1991 | England | 20 patients, aged from 78 to 69. No detail period post-stroke | Content analysis | semi-structured interviews | To identify service needs of stroke survivors and their informal carers | Affective needs (emotionalism and communication); out-patient follow-up |
| Study | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Q8 | Q9 | Q10 |
|---|---|---|---|---|---|---|---|---|---|---|
| Valérie Poulin et al. [44] | Y | Y | Y | Y | Y | Y | UN | Y | Y | Y |
| Monique R. Pappadis et al. [46] | Y | Y | Y | Y | Y | Y | UN | Y | Y | Y |
| Emma K. Kj Ö rk et al. [39] | Y | Y | Y | Y | Y | Y | UN | Y | Y | Y |
| Gunvor GARD et al. [43] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Jamuna Rani Appalasamy et al. [19] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Abrahamson, Vanessa et al. [15] | Y | Y | Y | Y | Y | Y | N | Y | Y | Y |
| Jessica Shipley et al. [47] | Y | Y | Y | Y | Y | Y | UN | Y | Y | Y |
| Shannon R.L et al. [48] | Y | Y | Y | Y | Y | Y | N | Y | Y | Y |
| Nadia Davoody et al. [45] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Emily H. L et al. [38] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Tina Taule et al. [49] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Silvio Simeone et al. [50] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Randi Martinsen et al. [51] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Jennifer H. White et al. [42] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Jennifer White et al. [52] | Y | Y | Y | Y | Y | Y | UN | Y | Y | Y |
| Marianne E Klinke et al. [41] | Y | Y | Y | Y | Y | Y | UN | Y | Y | Y |
| Lutz, B J et al. [33] | Y | Y | Y | Y | Y | Y | UN | Y | Y | Y |
| L. Salisbury et al. [34] | Y | Y | Y | Y | Y | UN | Y | Y | Y | Y |
| Jan Pringle et al. [35] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| J Ö RGEN MEDIN et al. [53] | Y | Y | Y | Y | Y | N | Y | Y | Y | Y |
| Jacki Liddle et al. [40] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| Claude Vincent et al. [18] | Y | Y | Y | Y | Y | Y | Y | N | Y | Y |
| Rose Wiles et al. [36] | Y | Y | Y | Y | Y | UN | UN | Y | Y | Y |
| Jacqueline McLean et al. [37] | Y | Y | UN | Y | N | N | UN | N | Y | Y |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, Y.; Zhang, Z.; Lin, B.; Mei, Y.; Liu, Q.; Zhang, L.; Wang, W.; Li, Y.; Fu, Z. The Unmet Needs of Community-Dwelling Stroke Survivors: A Systematic Review of Qualitative Studies. Int. J. Environ. Res. Public Health 2021, 18, 2140. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18042140
Guo Y, Zhang Z, Lin B, Mei Y, Liu Q, Zhang L, Wang W, Li Y, Fu Z. The Unmet Needs of Community-Dwelling Stroke Survivors: A Systematic Review of Qualitative Studies. International Journal of Environmental Research and Public Health. 2021; 18(4):2140. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18042140
Chicago/Turabian StyleGuo, Yunfei, Zhenxiang Zhang, Beilei Lin, Yongxia Mei, Qingxuan Liu, Leyun Zhang, Wenna Wang, Yuan Li, and Zhongrong Fu. 2021. "The Unmet Needs of Community-Dwelling Stroke Survivors: A Systematic Review of Qualitative Studies" International Journal of Environmental Research and Public Health 18, no. 4: 2140. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18042140