
Tuberculosis and Non-Communicable Disease Multimorbidity: An Analysis of the World Health Survey in 48 Low- and Middle-Income Countries


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. The Survey
2.2. Variables
2.2.1. Tuberculosis
2.2.2. Non-Communicable Diseases (NCDs)
2.2.3. Control Variables
2.3. Statistical Analysis
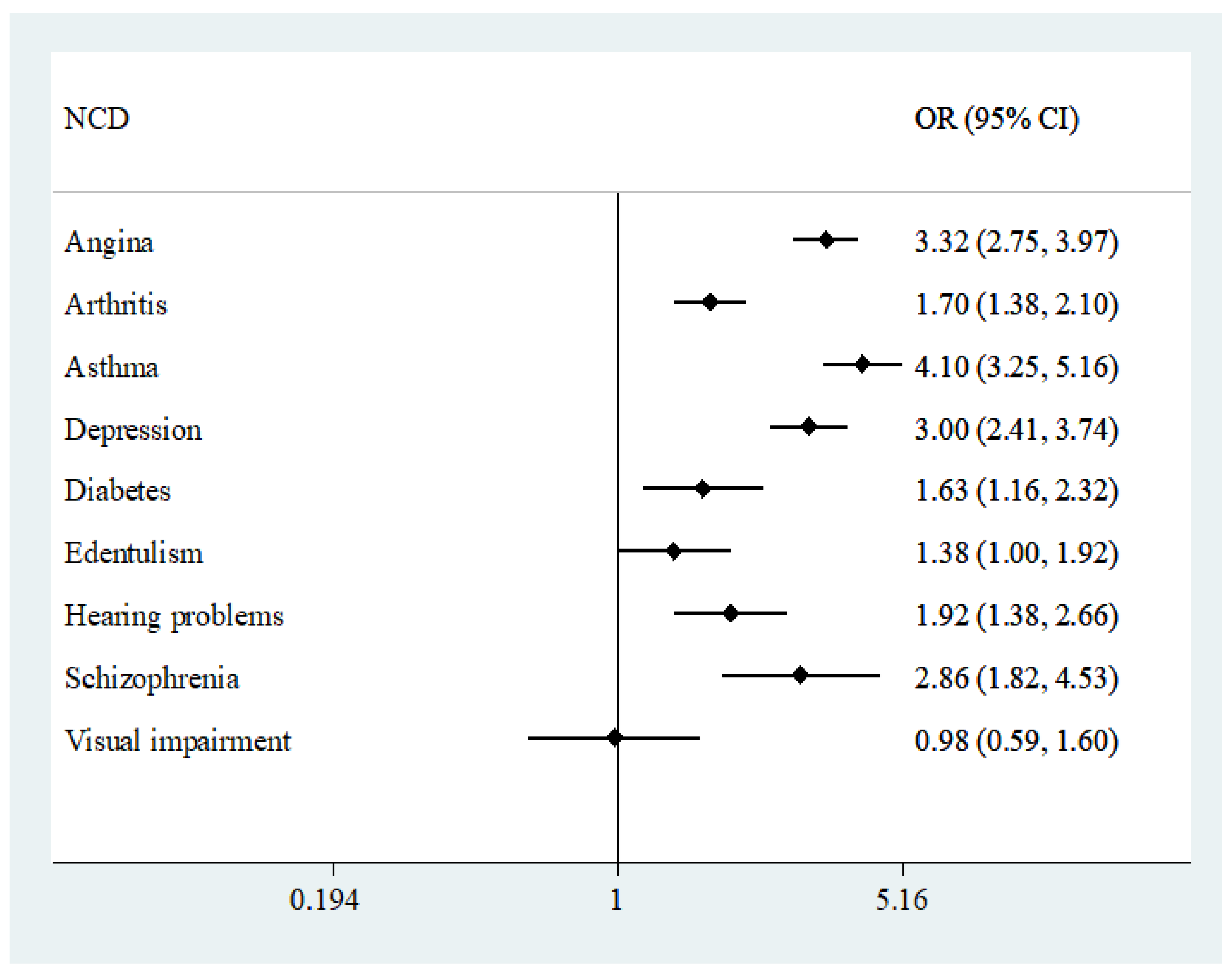
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country | Country-Income Level | n |
|---|---|---|
| Bangladesh | LIC | 5942 |
| Bosnia and Herzegovina | MIC | 1031 |
| Brazil | MIC | 5000 |
| Burkina Faso | LIC | 4948 |
| Chad | LIC | 4870 |
| China | MIC | 3994 |
| Comoros | LIC | 1836 |
| Croatia | MIC | 993 |
| Czech Republic | MIC | 949 |
| Dominican Republic | MIC | 5027 |
| Ecuador | MIC | 5675 |
| Estonia | MIC | 1020 |
| Ethiopia | LIC | 5089 |
| Georgia | MIC | 2950 |
| Ghana | LIC | 4165 |
| Hungary | MIC | 1419 |
| India | LIC | 10,687 |
| Ivory Coast | LIC | 3251 |
| Kazakhstan | MIC | 4499 |
| Kenya | LIC | 4640 |
| Laos | LIC | 4988 |
| Latvia | MIC | 929 |
| Malawi | LIC | 5551 |
| Malaysia | MIC | 6145 |
| Mali | LIC | 4886 |
| Mauritania | LIC | 3902 |
| Mauritius | MIC | 3968 |
| Mexico | MIC | 38,746 |
| Morocco | MIC | 5000 |
| Myanmar | LIC | 6045 |
| Namibia | MIC | 4379 |
| Nepal | LIC | 8820 |
| Pakistan | LIC | 6501 |
| Paraguay | MIC | 5288 |
| Philippines | MIC | 10,083 |
| Republic of Congo | LIC | 3075 |
| Russia | MIC | 4427 |
| Senegal | LIC | 3461 |
| Slovakia | MIC | 2535 |
| South Africa | MIC | 2629 |
| Sri Lanka | MIC | 6805 |
| Swaziland | MIC | 3117 |
| Tunisia | MIC | 5202 |
| Ukraine | MIC | 2860 |
| Uruguay | MIC | 2996 |
| Vietnam | LIC | 4174 |
| Zambia | LIC | 4165 |
| Zimbabwe | LIC | 4290 |

References
- World Health Organization. Tuberculosis. Available online: https://www.who.int/news-room/fact-sheets/detail/tuberculosis (accessed on 20 May 2020).
- Falzon, D.; Mirzayev, F.; Wares, F.; Baena, I.G.; Zignol, M.; Linh, N.; Weyer, K.; Jaramillo, E.; Floyd, K.; Raviglione, M. Multidrug-resistant tuberculosis around the world: What progress has been made? Eur. Respir. J. 2015, 45, 150–160. [Google Scholar] [CrossRef] [Green Version]
- Roche, S.; de Vries, E. Multimorbidity in a large district hospital: A descriptive cross-sectional study. S. Afr. Med J. 2017, 107, 1110–1115. [Google Scholar] [CrossRef]
- White, L.V.; Edwards, T.; Lee, N.; Castro, M.C.; Saludar, N.R.; Calapis, R.W.; Faguer, B.N.; Fuente, N.D.; Mayoga, F.; Saito, N.; et al. Patterns and predictors of co-morbidities in Tuberculosis: A cross-sectional study in the Philippines. Sci. Rep. 2020, 10, 41. [Google Scholar] [CrossRef]
- Hargreaves, J.R.; Boccia, D.; Evans, C.A.; Adato, M.; Petticrew, M.; Porter, J.D. The social determinants of tuberculosis: From evidence to action. Am. J. Public Health 2011, 101, 654–662. [Google Scholar] [CrossRef] [PubMed]
- Marais, B.J.; Lönnroth, K.; Lawn, S.D.; Migliori, G.B.; Mwaba, P.; Glaziou, P.; Bates, M.; Colagiuri, R.; Zijenah, L.; Swaminathan, S.; et al. Tuberculosis comorbidity with communicable and non- communicable diseases: Integrating health services and control efforts. Lancet Infect. Dis. 2013, 13, 436–448. [Google Scholar] [CrossRef] [Green Version]
- Bates, M.; Marais, B.J.; Zumla, A. Tuberculosis comorbidity with communicable and noncommunicable diseases. Cold Spring Harb. Perspect. Med. 2015, 5, a017889. [Google Scholar] [CrossRef] [Green Version]
- Peltzer, K. Tuberculosis non-communicable disease comorbidity and multimorbidity in public primary care patients in South Africa. Afr. J. Prim. Health Care Fam. Med. 2018, 10, e1–e6. [Google Scholar] [CrossRef] [PubMed]
- Beaglehole, R.; Bonita, R.; Alleyne, G.; Horton, R.; Li, L.; Lincoln, P.; Mbanya, J.C.; McKee, M.; Moodie, R.; Nishtar, S.; et al. UN high-level meeting on non- communicable diseases: Addressing four questions. Lancet 2011, 378, 449–455. [Google Scholar] [CrossRef]
- Vos, T.; Barber, R.M.; Bell, B.; Bertozzi-Villa, A.; Biryukov, S.; Bolliger, I.; Charlson, F.; Davis, A.; Degenhardt, L.; Dicker, D.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990-2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015, 386, 743–800. [Google Scholar] [CrossRef] [Green Version]
- Koyanagi, A.; Vancampfort, D.; Carvalho, A.F.; De Vvlder, J.E.; Haro, J.M.; Pizzol, D.; Veronese, N.; Stubbs, B. Depression comorbid with tuberculosis and its impact on health status: Cross-sectional analysis of community-based data from 48 low0- and middle-income countries. BMC Med. 2017, 15, 209. [Google Scholar] [CrossRef] [Green Version]
- Jeon, C.Y.; Murray, M.B. Diabetes mellitus increases the risk of active tuberculosis: A systematic review of 13 observational studies. PLoS Med. 2008, 5, e152. [Google Scholar]
- A Baker, M.; Harries, A.D.; Jeon, C.Y.; E Hart, J.; Kapur, A.; Lönnroth, K.; Ottmani, S.-E.; Goonesekera, S.D.; Murray, M.B. The impact of diabetes on tuberculosis treatment outcomes: A systematic review. BMC Med. 2011, 9, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevenson, C.R.; Forouhi, N.G.; Roglic, G.; Williams, B.G.; A Lauer, J.; Dye, C.; Unwin, N. Diabetes and tuberculosis: The impact of the diabetes epidemic on tuberculosis incidence. BMC Public Health 2007, 7, 234. [Google Scholar] [CrossRef] [Green Version]
- Van den Akker, M.B.F.; Roos, S.; Knottnerus, J.A. Comorbidity or multimorbidity: What’s in a name? A review of the literature. Eur. J. Gen. Pract. 1996, 2, 65–70. [Google Scholar] [CrossRef]
- Foguet-Boreu, Q.; Violán, C.; Rodríguez-Blanco, T.; Roso-Llorach, A.; Pons-Vigués, M.; Pujol-Ribera, E.; Gil, Y.C.; Valderas, J.M. Impact of multimorbidity: Acute morbidity, area of residency and use of health services across the life span in a region of south Europe. BMC Fam. Pract. 2014, 15, 55. [Google Scholar] [CrossRef] [Green Version]
- Stubbs, B.; Vancampfort, D.; Veronese, N.; Kahl, K.G.; Mitchell, A.J.; Lin, P.-Y.; Tseng, P.-T.; Mugisha, J.; Solmi, M.; Carvalho, A.F.; et al. Depression and physical health multimorbidity: Primay data and country-wide meta-analysis of population data from 190,593 people across 43 low- and middle-income countries. Psychol. Med. 2017, 47, 2107–2117. [Google Scholar] [CrossRef] [PubMed]
- France, E.F.; Wyke, S.; Gunn, J.M.; Mair, F.S.; McLean, G.; Mercer, S.W. Multimorbidity in primary care: A systematic review of prospective cohort studies. Br. J. Gen. Pract. 2012, 62, e297–e307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uijen, A.A.; van de Lisdonk, E.H. Multimorbidity in primary care: Prevalence and trend over the last 20 years. Eur. J. Gen. Pract. 2008, 14 (Suppl. S1), 28–32. [Google Scholar] [CrossRef] [PubMed]
- Salisbury, C.; Johnson, L.; Purdy, S.; Valderas, J.M.; Montgomery, A.A. Epidemiology and impact of multimorbidity in primary care: A retrospective cohort study. Br. J. Gen. Pract. 2011, 61, e12–e21. [Google Scholar] [CrossRef] [PubMed]
- Vancampfort, D.; Koyanagi, A.; Ward, P.; Rosenbaum, S.; Schuch, F.B.; Mugisha, J.; Richards, J.; Firth, J.; Stubbs, B. Chronic physical conditions, multimorbidity and physical activity across 46 low- and middle-income countries. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 6. [Google Scholar] [CrossRef] [PubMed]
- Melaku, Y.A.; Temesgen, A.M.; Deribew, A.; Tessema, G.A.; Deribe, K.; Sahle, B.W.; Abera, S.F.; Bekele, T.; Lemma, F.; Amare, A.T.; et al. The impact of dietary risk factors on the burden of non-communicable diseases in Ethiopia: Findings from the Global Burden of Disease study 2013. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thrush, A.; Hyder, A. The neglected burden of caregiving in low- and middle-income countries. Disabil. Health J. 2014, 7, 262–272. [Google Scholar] [CrossRef] [PubMed]
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Siegel, K.R.; Patel, S.A.; Ali, M.K. Non-communicable diseases in South Asia: Contemporary perspectives. Br. Med Bull. 2014, 111, 31–44. [Google Scholar] [CrossRef]
- Valenzuela-Jiménez, H.; Manrique-Hernández, E.F.; Idrovo, A.J. Association of tuberculosis with multimorbidity and social networks. J. Bras. de Pneumol. 2017, 43, 51–53. [Google Scholar] [CrossRef] [Green Version]
- Reis-Santos, B.; Gomes, T.; Macedo, L.R.; Horta, B.L.; Riley, L.W.; Maciel, E.L. Prevalence and patterns of multimorbidity among tuberculosis patients in Brazil: A cross-sectional study. Int. J. Equity Health 2013, 12, 1–8. Available online: http://www.equityhealthj.com/content/12/1/61 (accessed on 7 June 2020). [CrossRef] [Green Version]
- Adejumo, O.A.; Olusola-Faleye, B.; Adepoju, V.A.; Gidado, M.; O Onoh, M.; Adegboye, O.; Abdur-Razzaq, H.; Moronfolu, O.; Shogbamimu, Y. The pattern of comorbidity and its prevalence among drug-resistant tuberculosis patients at treatment initiation in Lagos, Nigeria. Trans. R. Soc. Trop. Med. Hyg. 2020, 114, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Schepisi, M.S.; Navarra, A.; Gomez, M.N.A.; Dudnyk, A.; Dyrhol-Riise, A.M.; Esteban, J.; Giorgetti, P.F.; Gualano, G.; Guglielmetti, L.; Heyckendorf, J.; et al. Burden and Characteristics of the Comorbidity Tuberculosis—Diabetes in Europe: TBnet Prevalence Survey and Case-Control Study. Open Forum Infect. Dis. 2018, 6, ofy337. [Google Scholar] [CrossRef]
- Song, A.T.W.; Schout, D.; Novaes, H.M.D.; Goldbaum, M. Clinical and epidemiological features of AIDS/tuberculosis comorbidity. Rev. Hosp. Clin. 2013, 58, 207–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Negin, J.; Abimbola, S.; Marais, B.J. Tuberculosis among older adults–time to take notice. Int. J. Infect. Dis. 2015, 32, 135–137. [Google Scholar] [CrossRef] [Green Version]
- Lehnert, T.; Heider, D.; Leicht, H.; Heinrich, S.; Corrieri, S.; Luppa, M.; Riedel-Heller, S.; König, H.-H. Review: Health Care Utilization and Costs of Elderly Persons with Multiple Chronic Conditions. Med Care Res. Rev. 2011, 68, 387–420. [Google Scholar] [CrossRef]
- Machado, V.D.S.S.; Valadares, A.L.R.; Costa-Paiva, L.H.; Osis, M.J.; Sousa, M.H.; Pinto-Neto, A.M. Aging, obesity, and multimorbidity in women 50 years or older: A population-based study. Menopause 2013, 20, 818–824. [Google Scholar] [CrossRef]
- Barnett, K.; Mercer, S.W.; Norbury, M.; Watt, G.; Wyke, S.; Guthrie, B. Epidemiology of multimorbidity and implications for health care, research, and medical education: A cross-sectional study. Lancet 2012, 380, 37–43. [Google Scholar] [CrossRef] [Green Version]
- Jani, B.D.; Hanlon, P.; Nicholl, B.I.; McQueenie, R.; Gallacher, K.I.; Lee, D.; Mair, F.S. Relationship between multimorbidity, demographic factors and mortality: Findings from the UK Biobank cohort. BMC Med. 2019, 17, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Gallo, J.J.; Hwang, S.; Joo, J.H.; Bogner, H.R.; Morales, K.H.; Bruce, M.L.; Reynolds, C.F. Multimorbidity, Depression, and Mortality in Primary Care: Randomized Clinical Trial of an Evidence-Based Depression Care Management Program on Mortality Risk. J. Gen. Intern. Med. 2016, 31, 380–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lange-Maia, B.S.; A Karvonen-Gutierrez, C.; Kazlauskaite, R.; Strotmeyer, E.S.; Karavolos, K.; Appelhans, B.M.; Janssen, I.; Avery, E.F.; A Dugan, S.; Kravitz, H.M. Impact of Chronic Medical Condition Development on Longitudinal Physical Function from Mid- to Early Late-Life: The Study of Women’s Health Across the Nation. Journals Gerontol. Ser. A Boil. Sci. Med Sci. 2019, 75, 1411–1417. [Google Scholar] [CrossRef]
- Fortin, M.; Lapointe, L.; Hudon, C.; Vanasse, A.; Ntetu, A.L.; Maltais, D. Multimorbidity and quality of life in primary care: A systematic review. Heal. Qual. Life Outcomes 2004, 2, 51. [Google Scholar] [CrossRef] [Green Version]
- Fortin, M.; Stewart, M.; Poitras, M.-E.; Almirall, J.; Maddocks, H. A Systematic Review of Prevalence Studies on Multimorbidity: Toward a More Uniform Methodology. Ann. Fam. Med. 2012, 10, 142–151. [Google Scholar] [CrossRef]
- Williams, J.S.; Egede, L.E. The Association Between Multimorbidity and Quality of Life, Health Status and Functional Disability. Am. J. Med Sci. 2016, 352, 45–52. [Google Scholar] [CrossRef]
- Gijsen, R.; Hoeymans, N.; Schellevis, F.G.; Ruwaard, D.; Satariano, W.A.; van den Bos, G.A. Causes and consequences of comorbidity: A Review. J. Clin. Epidemiol. 2001, 54, 661–674. [Google Scholar] [CrossRef]
- Alaba, O.; Chola, L. The social determinants of multimorbidity in South Africa. Int. J. Equity Health 2013, 12, 63. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization World Health Survey. Available online: https://www.who.int/healthinfo/survey/en/ (accessed on 6 May 2020).
- Kish, L. A procedure for objective respondent selection within the household. J. Am. Stat. Assoc. 2012, 44, 380–387. [Google Scholar] [CrossRef]
- Nuevo, R.; Chatterji, S.; Verdes, E.; Naidoo, N.; Arango, C.; Ayuso-Mateos, J.L. The continuum of psychotic symptoms in the general population: A cross-national study. Schizophr. Bull. 2012, 38, 475–485. [Google Scholar] [CrossRef] [Green Version]
- Turner, A.G. Sampling strategies. In Handbook on Designing of Household Sample Surveys; United Nations Statistics Division: Geneva, Switzerland, 2003. [Google Scholar]
- Goldhaber-Fiebert, J.D.; Jeon, C.Y.; Cohen, T.; Murray, M.B. Diabetes mellitus and tuberculosis in countries with high tuberculosis burdens: Individual risks and social determinants. Int. J. Epidemiol. 2011, 40, 417–428. [Google Scholar] [CrossRef] [Green Version]
- Stubbs, B.; Koyanagi, A.; Veronese, N.; Vancampfort, D.; Solmi, M.; Gaughran, F.; Carvalho, A.F.; Lally, J.; Mitchell, A.J.; Mugisha, J.; et al. Physical multimorbidity and psychosis: Comprehensive cross sectional analysis including 242,952 people across 48 low- and middle-income countries. BMC Med. 2016, 14, 189. [Google Scholar] [CrossRef] [PubMed]
- Vancampfort, D.; Koyanagi, A.; Ward, P.B.; Veronese, N.; Carvalho, A.F.; Solmi, M.; Mugisha, J.; Rosenbaum, S.; De Hert, M.; Stubbs, B. Perceived Stress and Its Relationship With Chronic Medical Conditions and Multimorbidity Among 229,293 Community-Dwelling Adults in 44 Low- and Middle-Income Countries. Am. J. Epidemiol. 2017, 186, 979–989. [Google Scholar] [CrossRef] [PubMed]
- Rose, G.A. The diagnosis of ischaemic heart pain and intermittent claudication in field surveys*. Bull. World Health Organ. 1962, 27, 645–658. [Google Scholar] [PubMed]
- Loerbroks, A.; Herr, R.M.; Subramanian, S.; A Bosch, J. The association of asthma and wheezing with major depressive episodes: An analysis of 245 727 women and men from 57 countries. Int. J. Epidemiol. 2012, 41, 1436–1444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cifuentes, M.; Sembajwe, G.; Tak, S.; Gore, R.; Kriebel, D.; Punnett, L. The association of major depressive episodes with income inequality and the human development index. Soc. Sci. Med. 2008, 67, 529–539. [Google Scholar] [CrossRef]
- Freeman, E.E.; Roy-Gagnon, M.-H.; Samson, É.; Haddad, S.; Aubin, M.-J.; Vela, C.; Zunzunegui, M.V. The Global Burden of Visual Difficulty in Low, Middle, and High Income Countries. PLoS ONE 2013, 8, e63315. [Google Scholar] [CrossRef] [Green Version]
- Patra, J.; Jha, P.; Rehm, J.; Suraweera, W. Tobacco Smoking, Alcohol Drinking, Diabetes, Low Body Mass Index and the Risk of Self-Reported Symptoms of Active Tuberculosis: Individual Participant Data (IPD) Meta-Analyses of 72,684 Individuals in 14 High Tuberculosis Burden Countries. PLoS ONE 2014, 9, e96433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vancampfort, D.; Stubbs, B.; Hallgren, M.; Koyanagi, A. Physical activity correlates in heavy episodic drinkers: Data from 46 low- and middle-income countries. Ment. Heal. Phys. Act. 2017, 13, 163–170. [Google Scholar] [CrossRef] [Green Version]
- Cooper, C. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar]
- Koyanagi, A.; Oh, H.; Stickley, A.; Haro, J.M.; De Vylder, J. Risk and functional significance of psychotic experiences among individuals with depression in 44 low- and middle-income countries. Psychol. Med. 2016, 46, 2655–2665. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, R.M. A Caution Regarding Rules of Thumb for Variance Inflation Factors. Qual. Quant. 2007, 41, 673–690. [Google Scholar] [CrossRef]
- Lawn, S.D.; Zumla, A.I. Tuberculosis. Lancet 2011, 378, 57–72. [Google Scholar] [CrossRef]
- Sweetland, A.C.; Kritski, A.; Oquendo, M.A.; Sublette, M.E.; Pala, A.N.; Silva, L.R.B.; Karpati, A.; Silva, E.C.; Moraes, M.O.; E Silva, J.R.L.; et al. Addressing the tuberculosis–depression syndemic to end the tuberculosis epidemic. Int. J. Tuberc. Lung Dis. 2017, 21, 852–861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacob, L.; Oh, H.; Shin, J.I.; Haro, J.M.; Vancampfort, D.; Stubbs, B.; E Jackson, S.; Smith, L.; Koyanagi, A. Informal Caregiving, Chronic Physical Conditions, and Physical Multimorbidity in 48 Low- and Middle-Income Countries. J. Gerontol. Ser. A Boil. Sci. Med. Sci. 2020, 75, 1572–1578. [Google Scholar] [CrossRef] [Green Version]
- Ahmadi, B.; Alimohammadian, M.; Yaseri, M.; Majidi, A.; Boreiri, M.; Islami, F.; Poustchi, H.; Derakhshan, M.H.; Feizesani, A.; Pourshams, A.; et al. Multimorbidity: Epidemiology and risk factors in the Golestan Cohort study. Iran. Med. 2016, 95, e2756. [Google Scholar] [CrossRef]
- Ho, A.; Collins, S.R.; Davis, K.; Doty, M.M. A look at working-age caregivers’ roles, health concerns, and need for support. Issue Brief 2005, 854, 1–12. [Google Scholar]
- Leive, A.; Xu, K. Coping with out-of-pocket health payments: Empirical evidence from 15 African countries. Bull. World Health Organ. 2008, 86, 849–856. [Google Scholar] [CrossRef] [PubMed]
- Kankeu, H.T.; Saksena, P.; Xu, K.; Evans, D.B. The financial burden from non-communicable diseases in low- and middle-income countries: A literature review. Health Res. Policy Syst. 2013, 11, 31. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The Global Burden of Disease: 2004 Update; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Oh, K.H.; Kim, H.J.; Kim, M.H. Non-communicable diseases and risk of tuberculosis in Korea. Int. J. Tuberc. Lung Dis. 2016, 20, 973–977. [Google Scholar] [CrossRef] [PubMed]
- Niazi, A.K.; Kalra, S. Diabetes and tuberculosis: A review of the role of optimal glycemic control. J. Diabetes Metab. Disord. 2012, 11, 28. [Google Scholar] [CrossRef] [Green Version]
- Jeon, C.Y.; Harries, A.D.; Baker, M.A.; Hart, J.E.; Kapur, A.; Lönnroth, K.; Ottmani, S.-E.; Goonesekera, S.; Murray, M.B. Bi-directional screening for tuberculosis and diabetes: A systematic review. Trop. Med. Int. Health 2010, 15, 1300–1314. [Google Scholar] [CrossRef]
- Baghaei, P.; Marjani, M.; Javanmard, P.; Tabarsi, P.; Masjedi, M.R. Diabetes mellitus and tuberculosis facts and controversies. J. Diabetes Metab. Disord. 2013, 12, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ottmani, S.E.; Murray, M.B.; Jeon, C.Y.; Baker, M.A.; Kapur, A.; Lonnroth, K.; Harries, A.D. Consultation meeting on tuberculosis and diabetes mellitus: Meeting summary and recommendations. Int. J. Tuberc. Lung Dis. 2010, 14, 1513–1517. [Google Scholar]
- Hansel, N.N.; Wu, A.W.; Chang, B.; Diette, G.B. Quality of life in tuberculosis: Patient and provider perspectives. Qual. Life Res. 2004, 13, 639–652. [Google Scholar] [CrossRef]
- Courtwright, A.; Turner, A.N. Tuberculosis and Stigmatization: Pathways and Interventions. Public Health Rep. 2010, 125 (Suppl. S4), 34–42. [Google Scholar] [CrossRef] [Green Version]
- Maes, M.; Kubera, M.; Obuchowiczwa, E.; Goehler, L.; Brzeszcz, J. Depression’s multiple comorbidities explained by (neuro)inflammatory and oxidative & nitrosative stress pathways. Neuroendocrinol. Lett. 2011, 32, 7–24. [Google Scholar]
- Oh, K.H.; Choi, H.; Kim, E.J.; Kim, H.J.; Cho, S.I. Depression and risk of tuberculosis: A nationwide population-based cohort study. Int. J. Tuberc. Lung Dis. 2017, 21, 804–809. [Google Scholar] [CrossRef]
- DiMatteo, M.R.; Lepper, H.S.; Croghan, T.W. Depression Is a Risk Factor for Noncompliance With Medical Treatment meta-analysis of the effects of anxiety and depression on patient adherence. Arch. Intern. Med. 2000, 160, 2101–2107. [Google Scholar] [CrossRef]
- Doherty, A.M.; Kelly, J.; McDonald, C.; O’Dywer, A.M.; Keane, J.; Cooney, J. A review of the interplay between tuberculosis and mental health. Gen. Hosp. Psychiatry 2013, 35, 398–406. [Google Scholar] [CrossRef]
- Aamir, S. Aisha Co-morbid anxiety and depression among pulmonary tuberculosis patients. J. Coll. Physicians Surg. Pak. 2010, 20, 703–704. [Google Scholar] [CrossRef] [PubMed]
- Khraishi, M.; Macdonald, D.; Rampakakis, E.; Vaillancourt, J.; Sampalis, J.S. Prevalence of patient-reported comorbidities in early and established psoriatic arthritis cohorts. Clin. Rheumatol. 2011, 30, 877–885. [Google Scholar] [CrossRef]
- Cazzola, M.; Calzetta, L.; Bettoncelli, G.; Novelli, L.; Cricelli, C.; Rogliani, P. Asthma and comorbid medical illness. Eur. Respir. J. 2010, 38, 42–49. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jespersen, L.; Abildstrøm, S.Z.; Hvelplund, A.; Prescott, E. Persistent angina: Highly prevalent and associated with long-term anxiety, depression, low physical functioning, and quality of life in stable angina pectoris. Clin. Res. Cardiol. 2013, 102, 571–581. [Google Scholar] [CrossRef] [PubMed]
- Matcham, F.; Rayner, L.; Steer, S.; Hotopf, M. The prevalence of depression in rheumatoid arthritis: A systematic review and meta-analysis. Rheumatol. 2013, 52, 2136–2148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balhara, Y.P.S.; Anwar, N.; Kuppili, P.P. Depression and physical noncommunicable diseases: The need for an integrated approach. WHO South-East Asia J. Public Health 2017, 6, 12–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendenhall, E.; Kohrt, B.A.; Norris, S.A.; Ndetei, D.; Prabhakaran, D. Non-communicable disease syndemics: Poverty, depression, and diabetes among low-income populations. Lancet 2017, 389, 951–963. [Google Scholar] [CrossRef] [Green Version]
- Mugisha, J.; Abdulmalik, J.; Hanlon, C.; Petersen, I.; Lund, C.; Upadhaya, N.; Ahuja, S.; Shidhaye, R.; Mntambo, N.; Alem, A.; et al. Health systems context(s) for integrating mental health into primary health care in six Emerald countries: A situation analysis. Int. J. Ment. Health Syst. 2017, 11, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seiglie, J.A.; Marcus, M.-E.; Ebert, C.; Prodromidis, N.; Geldsetzer, P.; Theilmann, M.; Agoudavi, K.; Andall-Brereton, G.; Aryal, K.K.; Bicaba, B.W.; et al. Diabetes Prevalence and Its Relationship With Education, Wealth, and BMI in 29 Low- and Middle-Income Countries. Diabetes Care 2020, 43, 767–775. [Google Scholar] [CrossRef] [PubMed]
- Aldridge, R.W.; Story, A.; Hwang, S.W.; Nordentoft, M.; Luchenski, S.A.; Hartwell, G.; Tweed, J.E.; Lewer, D.; Katikireddi, S.V.; Hayward, A.C. Morbidity and mortality in homeless individuals, prisoners, sex workers and individuals with substance use disorders in high-income countries: A systematic review and meta-anaysis. Lancet 2018, 391, 241–250. [Google Scholar] [CrossRef] [Green Version]
- Graham, L.; Fischbacher, C.M.; Stockton, D.; Fraswer, A.; Fleming, M.; Greig, K. Understanding extreme mortality among prisoners: A national cohort study in Scotland using data linkage. Eur. J. Public Health 2015, 25, 879–885. [Google Scholar] [CrossRef] [Green Version]





| Tuberculosis | |||||
|---|---|---|---|---|---|
| Characteristic | Overall | No | Yes | p-Value a | |
| Age (years) | Mean (SD) | 38.4 (16.0) | 35.5 (16.0) | 43.4 (17.1) | <0.001 |
| Sex | Male | 49.2 | 49.1 | 54.0 | 0.010 |
| Female | 50.8 | 50.9 | 46.0 | ||
| Wealth | Poorest | 20.5 | 20.3 | 31.7 | <0.001 |
| Poorer | 20.0 | 19.9 | 22.6 | ||
| Middle | 20.0 | 20.0 | 17.7 | ||
| Richer | 19.8 | 19.9 | 16.6 | ||
| Richest | 19.8 | 19.9 | 11.4 | ||
| Education | No formal | 25.2 | 24.9 | 43.9 | <0.001 |
| Primary | 31.8 | 31.7 | 34.2 | ||
| Secondary | 33.1 | 33.4 | 19.4 | ||
| Tertiary | 9.9 | 10.0 | 2.5 | ||
| Smoking | No | 72.8 | 72.9 | 63.0 | <0.001 |
| Yes | 27.2 | 27.1 | 37.0 | ||
| Heavy drinking | No | 97.9 | 98.0 | 97.6 | 0.354 |
| Yes | 2.1 | 2.0 | 2.4 | ||
| Angina | No | 85.4 | 85.8 | 60.3 | <0.001 |
| Yes | 14.6 | 14.2 | 39.7 | ||
| Arthritis | No | 87.1 | 87.3 | 74.5 | <0.001 |
| Yes | 12.9 | 12.7 | 25.5 | ||
| Asthma | No | 94.6 | 94.9 | 78.2 | <0.001 |
| Yes | 5.4 | 5.1 | 21.8 | ||
| Diabetes | No | 96.9 | 96.9 | 93.4 | <0.001 |
| Yes | 3.1 | 3.1 | 6.6 | ||
| Depression | No | 92.9 | 93.2 | 75.8 | <0.001 |
| Yes | 7.1 | 6.8 | 24.2 | ||
| Edentulism | No | 93.7 | 93.8 | 89.5 | <0.001 |
| Yes | 6.3 | 6.2 | 10.5 | ||
| Hearing problems | No | 96.5 | 96.6 | 91.6 | <0.001 |
| Yes | 3.5 | 3.4 | 8.4 | ||
| Schizophrenia | No | 98.9 | 99.0 | 95.5 | <0.001 |
| Yes | 1.1 | 1.0 | 4.5 | ||
| Visual impairment | No | 98.6 | 98.6 | 97.8 | 0.030 |
| Yes | 1.4 | 1.4 | 2.2 | ||
| No. of NCD | 0 | 65.6 | 65.6 | 31.2 | <0.001 |
| 1 | 21.8 | 21.8 | 29.2 | ||
| 2 | 8.4 | 8.4 | 20.4 | ||
| 3 | 3.0 | 3.0 | 11.3 | ||
| 4 | 0.9 | 0.9 | 4.6 | ||
| ≥5 | 0.3 | 0.3 | 3.3 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stubbs, B.; Siddiqi, K.; Elsey, H.; Siddiqi, N.; Ma, R.; Romano, E.; Siddiqi, S.; Koyanagi, A. Tuberculosis and Non-Communicable Disease Multimorbidity: An Analysis of the World Health Survey in 48 Low- and Middle-Income Countries. Int. J. Environ. Res. Public Health 2021, 18, 2439. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052439
Stubbs B, Siddiqi K, Elsey H, Siddiqi N, Ma R, Romano E, Siddiqi S, Koyanagi A. Tuberculosis and Non-Communicable Disease Multimorbidity: An Analysis of the World Health Survey in 48 Low- and Middle-Income Countries. International Journal of Environmental Research and Public Health. 2021; 18(5):2439. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052439
Chicago/Turabian StyleStubbs, Brendon, Kamran Siddiqi, Helen Elsey, Najma Siddiqi, Ruimin Ma, Eugenia Romano, Sameen Siddiqi, and Ai Koyanagi. 2021. "Tuberculosis and Non-Communicable Disease Multimorbidity: An Analysis of the World Health Survey in 48 Low- and Middle-Income Countries" International Journal of Environmental Research and Public Health 18, no. 5: 2439. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052439