
Cultural Identity Conflict Informs Engagement with Self-Management Behaviours for South Asian Patients Living with Type-2 Diabetes: A Critical Interpretative Synthesis of Qualitative Research Studies


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Literature Search and Eligibility
2.3. Data Extraction and Critical Appraisal
2.4. Analytical Procedure
3. Results
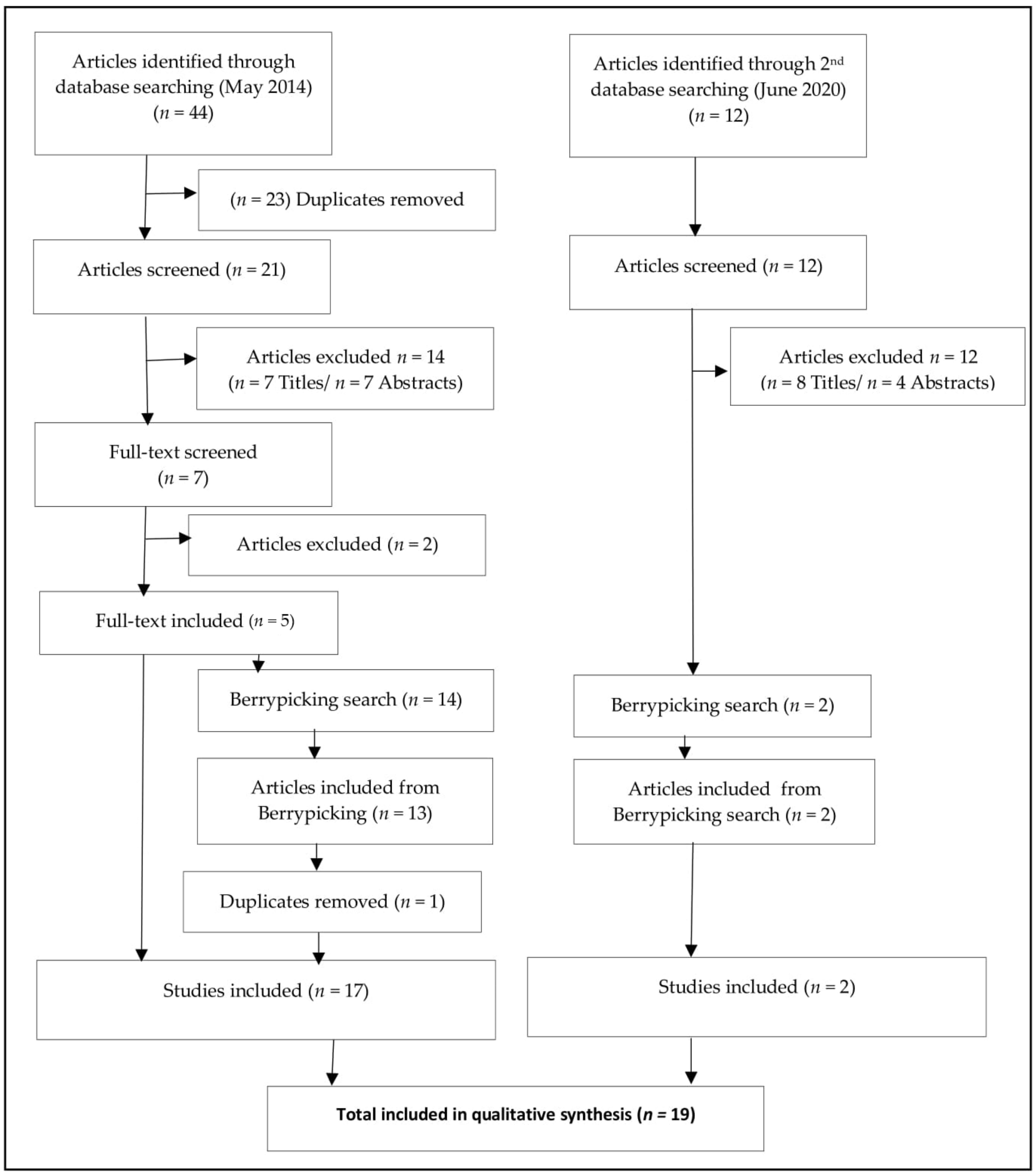
3.1. Search Results and Article Appraisal
3.2. Description of Studies
4. Analysis
4.1. Critical Interpretative Synthesis
4.2. Synthesising Argument 1: Decisional Conflict for Self-Management Behaviours
4.2.1. Diet
4.2.2. Physical Activity (PA)
4.2.3. Medication
4.3. Synthesising Argument 2: T2D Management Strategies and Factors Influencing Conflict
4.3.1. Social Conflict
4.3.2. Religious Obligations
4.3.3. Healthcare Delivery
4.3.4. Health Beliefs, Language, and Literacy
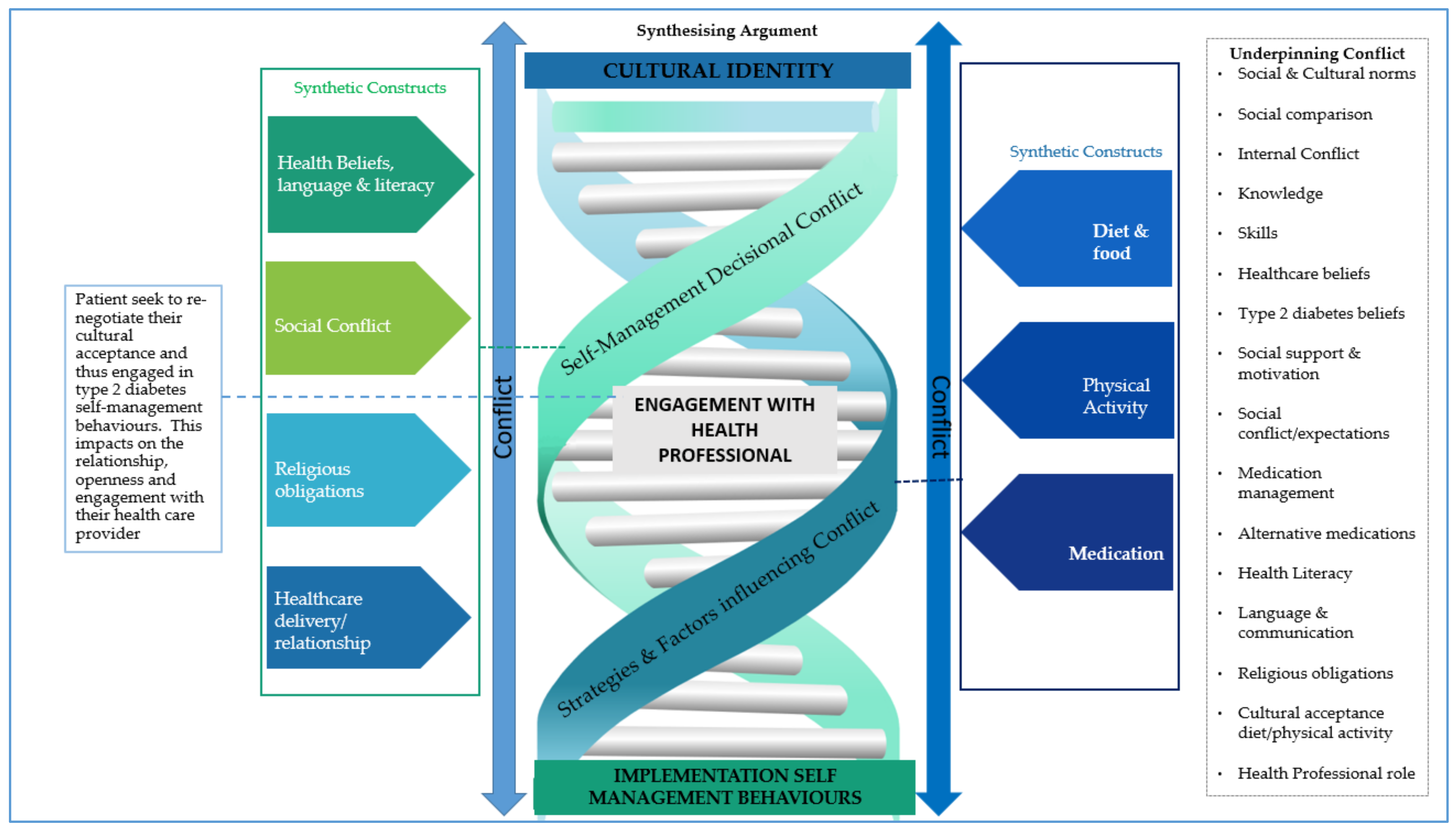
5. Synthesising Argument—Cultural Conflict vs. T2D Management
6. Discussion
6.1. Interpretation
6.2. Relevance to Clinical Practice
6.3. Ethnic Minorities, COVID-19, and T2D
6.4. Future Research
6.5. Strengths and Limitations of the Review
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Office of National Statistics. Ethnicity and National Identity in England and Wales. 2011. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/culturalidentity/ethnicity/articles/ethnicityandnationalidentityinenglandandwales/2012-12-11 (accessed on 8 January 2017).
- Rees, P.; Wohland, P.; Norman, P. The United Kingdom’s multi-ethnic future: How fast is it arriving. In Applied Spatial Modelling and Planning; Lombard, J., Stern, E., Clarke, G.P., Eds.; Routledge: London, UK, 2016; pp. 157–171. [Google Scholar]
- Rees, P.H.; Wohland, P.; Norman, P.; Lomax, N.; Clark, S.D. Population projections by ethnicity: Challenges and solutions for the United Kingdom. In The frontiers of Applied Demography; Springer: Cham, Switzerland, 2017; pp. 383–408. ISBN 978-3-319-43327-1. [Google Scholar]
- Hanif, W.; Karamat, M.A. Cultural aspects. In Diabetes UK and South Asian Health Foundation Recommendations on Diabetes Research Priorities for British South Asians; Diabetes UK: London, UK, 2009; pp. 27–28. [Google Scholar]
- Peach, C. Islam, ethnicity and South Asian religions in the London 2001 census. Trans. Inst. Br. Geogr. 2006, 31, 353–370. [Google Scholar] [CrossRef]
- O’Brien, R.; Potter-Collins, A. 2011 Census Analysis: Ethnicity and Religion of the Non-UK Born Population in England and Wales; Office for National Statistics. 2011. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/culturalidentity/ethnicity/articles/2011censusanalysisethnicityandreligionofthenonukbornpopulationinenglandandwales/2015-06-18 (accessed on 4 January 2017).
- Senior, P.A.; Bhopal, R. Ethnicity as a variable in epidemiological research. BMJ 1994, 309, 327–330. [Google Scholar] [CrossRef] [Green Version]
- Bhatnagar, P.; Shaw, A.; Foster, C. Generational differences in the physical activity of UK South Asians: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 96. [Google Scholar] [CrossRef] [Green Version]
- Mohan, V.; Cooper, M.E.; Matthews, D.R.; Khunti, K. The Standard of Care in Type 2 Diabetes: Re-evaluating the treatment Paradigm. Diabetes Ther. 2019, 10, 1–13. [Google Scholar] [CrossRef] [Green Version]
- International Diabetes Federation. IDF Diabetes Atlas 8th Edition. Available online: https://www.diabetesatlas.org/upload/resources/previous/files/8/IDF_DA_8e-EN-final.pdf (accessed on 28 April 2018).
- World Health Organization. Global Report on Type 2 Diabetes; World Health Organization: Geneva, Switzerland, 2016; Available online: http://www.who.int/mediacentre/factsheets/fs312/en/ (accessed on 3 March 2016).
- Piper, C.; Marossy, A.; Griffiths, Z.; Adegboye, A. Evaluation of a type 2 diabetes prevention program using a commercial weight management provider for non-diabetic hyperglycemic patients referred by primary care in the UK. BMJ Open Diabetes Res. Care 2017, 5, e000418. [Google Scholar] [CrossRef] [Green Version]
- Bhopal, R.S. A four-stage model explaining the higher risk of Type 2 diabetes mellitus in South Asians compared with European populations. Diabet. Med. 2013, 30, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Gujral, U.P.; Pradeepa, R.; Weber, M.B.; Narayan, K.M.; Mohan, V. Type 2 diabetes in South Asians: Similarities and differences with white Caucasian and other populations. Ann. N. Y. Acad. Sci. 2013, 1281, 51–63. [Google Scholar] [CrossRef]
- Meeks, K.A.; Freitas-Da-Silva, D.; Adeyemo, A.; Beune, E.J.; Modesti, P.A.; Stronks, K.; Zafarmand, M.H.; Agyemang, C. Disparities in type 2 diabetes prevalence among ethnic minority groups resident in Europe: A systematic review and meta-analysis. Intern. Emerg. Med. 2016, 11, 327–340. [Google Scholar] [CrossRef]
- Modesti, P.A.; Perticone, F.; Parati, G.; Rosei, E.A.; Prisco, D. Chronic disease in the ethnic minority and migrant groups: Time for a paradigm shift in Europe. Intern. Emerg. Med. 2016, 11, 295–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sattar, N.; Gill, J.M. Type 2 diabetes in migrant south Asians: Mechanisms, mitigation, and management. Lancet Diabetes Endocrinol. 2015, 3, 1004–1016. [Google Scholar] [CrossRef] [Green Version]
- Tillin, T.; Hughes, A.D.; Mayet, J.; Whincup, P.; Sattar, N.; Forouhi, N.G.; McKeigue, P.M.; Chaturvedi, N. The relationship between metabolic risk factors and incident cardiovascular disease in Europeans, South Asians, and African Caribbeans: SABRE (Southall and Brent Revisited)—A prospective population-based study. J. Am. Coll. Cardiol. 2013, 61, 1777–1786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Department of Health and Social Care. Prevention Is Better than Cure: Our Vision to Help You Live Well for Longer. 2018. Available online: https://www.gov.uk/government/publications/prevention-is-better-than-cure-our-vision-to-help-you-live-well-for-longer (accessed on 3 January 2021).
- Wilmot, E.; Idris, I. Early onset type 2 diabetes: Risk factors, clinical impact and management. Ther. Adv. Chronic. Dis. 2014, 5, 234–244. [Google Scholar] [CrossRef] [Green Version]
- Khunti, K.; Routen, A.; Patel, K.; Ali, S.; Gill, P.; Banerjee, A.; Lad, A.; Patel, V.; Hanif, W. COVID-19 in Black, Asian and Minority Ethnic Populations: An Evidence Review and Recommendations from the South Asian Health Foundation; South Asian Health Foundation. Available online: https://static1.squarespace.com/static/5944e54ab3db2b94bb077ceb/t/5f059972f6680542c546897f/1594202487799/Covid19_SAHF_Final+for+Release.pdf (accessed on 5 January 2021).
- Caballero, A.E.; Ceriello, A.; Misra, A.; Aschner, P.; McDonnell, M.E.; Hassanein, M.; Ji, L.; Mbanya, J.C.; Fonseca, V.A. COVID-19 in people living with diabetes: An international consensus. J. Diabetes Complicat. 2020, 34, 107671. [Google Scholar] [CrossRef]
- Holman, N.; Knighton, P.; Kar, P.; O’Keefe, J.; Curley, M.; Weaver, A.; Barron, E.; Bakhai, C.; Khunti, K.; Wareham, N.J.; et al. Risk factors for COVID-19-related mortality in people with type 1 and type 2 diabetes in England: A population-based cohort study. Lancet Diabetes Endocrinol. 2020, 8, 823–833. [Google Scholar] [CrossRef]
- NHS England. Supporting Self-Management/Self Care 2017. Available online: http://www.nice.org.uk/guidance/ng28 (accessed on 5 January 2018).
- National Institute for Health and Care Excellence. Type 2 Diabetes in Adults: Management. 2017. Available online: https://www.nice.org.uk/guidance/ng28 (accessed on 1 May 2018).
- Public Health England. Public Health Outcomes Framework: Health Equity Report—Focus on Ethnicity. 2017. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/733093/PHOF_Health_Equity_Report.pdf (accessed on 1 May 2018).
- Rhodes, P.; Nocon, A. A problem of communication? Diabetes care among Bangladeshi people in Bradford. Health Soc. Care Community 2003, 11, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Stone, M.; Pound, E.; Pancholi, A.; Farooqi, A.; Khunti, K. Empowering patients with diabetes: A qualitative primary care study focusing on South Asians in Leicester, UK. Fam. Pract. 2005, 22, 647–652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Estacio, E.V.; McKinley, R.K.; Saidy-Khan, S.; Karic, T.; Clark, L.; Kurth, J. Health literacy: Why it matters to South Asian men with diabetes. Prim. Health Care Res. Dev. 2015, 16, 214–218. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. The Management of Type 2 Diabetes. 2015. Available online: http://www.nice.org.uk/guidance/ng28 (accessed on 4 January 2017).
- Khunti, K.; Kumar, S.; Brodie, J. Diabetes UK and South Asian Health Foundation Recommendations on Diabetes Research Priorities for British South Asians. Available online: https://www.diabetes.org.uk/resources-s3/2017-11/south_asian_report.pdf (accessed on 8 August 2014).
- Potluri, R.; Pichaipillai, L.; Rayasamudra, S.; Ravi, A.; Uppal, H.; Lavu, D.; Chandran, S. Type 2 diabetes in young South Asian patients leads to increased cardiovascular comorbidity and decreased survival. Diabet. Med. 2014, 31, P307. [Google Scholar]
- Umeh, K.F. Ethnic inequalities in doctor-patient communication regarding personal care plans: The mediating effects of positive mental wellbeing. Ethn. Health 2019, 24, 57–72. [Google Scholar] [CrossRef]
- Zeh, P.; Cannaby, A.M.; Sandhu, H.K.; Warwick, J.; Sturt, J.A. A cross-sectional survey of general practice health workers’ perceptions of their provision of culturally competent services to ethnic minority people with diabetes. Prim. Care Diabetes 2018, 12, 501–509. [Google Scholar] [CrossRef] [Green Version]
- Mohajan, H.K. Qualitative research methodology in social sciences and related subjects. J. Econ. Dev. Environ. People 2018, 7, 23–48. [Google Scholar] [CrossRef] [Green Version]
- Barnett-Page, E.; Thomas, J. Methods for the synthesis of qualitative research: A critical review. BMC Med. Res. Methodol. 2009, 9, 59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavers, D.; Habets, L.; Cunningham-Burley, S.; Watson, E.; Banks, E.; Campbell, C. Living with and beyond cancer with comorbid illness: A qualitative systematic review and evidence synthesis. J. Cancer Surviv. 2019, 13, 148–159. [Google Scholar] [CrossRef] [Green Version]
- Houghton, C.; Meskell, P.; Delaney, H.; Smalle, M.; Glenton, C.; Booth, A.; Chan, X.H.S.; Devane, D.; Biesty, L.M. Barriers and facilitators to healthcare workers’ adherence with infection prevention and control (IPC) guidelines for respiratory infectious diseases: A rapid qualitative evidence synthesis. Cochrane Database Syst. Rev. 2020, 4, CD013582. [Google Scholar] [CrossRef] [PubMed]
- Fleming, E.; Gillibrand, W. An exploration of culture, diabetes, and nursing in the South Asian community: A metasynthesis of qualitative studies. J. Transcult. Nurs. 2009, 20, 146–155. [Google Scholar] [CrossRef]
- Sohal, T.; Sohal, P.; King-Shier, K.M.; Khan, N.A. Barriers and Facilitators for Type-2 Diabetes Management in South Asians: A Systematic Review. PLoS ONE 2015, 10, e0136202. [Google Scholar] [CrossRef] [Green Version]
- Darlington, F.; Norman, P.; Ballas, D.; Exeter, D.J. Exploring ethnic inequalities in health: Evidence from the Health Survey for England, 1998–2011. Divers. Equal. Health Care 2015, 12, 54–65. [Google Scholar] [CrossRef]
- Owen, D. Future Identities: Changing Identities in the UK—The Next 10 Years; Government Office for Science: London, UK, 2013. Available online: https://www.gov.uk/government/publications/future-identities-changing-identities-in-the-uk (accessed on 6 June 2020).
- Allcock, C.; Dormon, F.; Taunt, R.; Dixon, J. Constructive Comfort: Accelerating Change in the NHS. Policy Analysis; The Health Foundation: London, UK, 2015; Available online: http://www.health.org.uk/sites/default/files/ConstructiveComfortAcceleratingChangeInTheNHS.pdf (accessed on 6 June 2020).
- Appleby, J. 10 Crucial Trends: Quality in the NHS 2009 to 2017; Quality Watch; The Nuffield Trust: London, UK, 2017; Volume 2020, Available online: https://www.nuffieldtrust.org.uk/news-item/10-crucial-trends-quality-in-the-nhs-2009-to-2017 (accessed on 6 June 2020).
- Dixon-Woods, M.; Cavers, D.; Agarwal, S.; Annandale, E.; Arthur, A.; Harvey, J.; Hsu, R.; Katbamna, S.; Olsen, R.; Smith, L.; et al. Conducting a critical interpretive synthesis of the literature on access to healthcare by vulnerable groups. BMC Med. Res. Methodol. 2006, 6, 35. [Google Scholar] [CrossRef]
- Gough, D.; Thomas, J. Commonality and diversity in reviews. In An Introduction to Systematic Reviews; Gough, D., Oliver, S., Thomas, J., Eds.; Sage Publications Ltd.: London, UK, 2017; pp. 43–70. ISBN 9781473929432. [Google Scholar]
- Dixon-Woods, M.; Agarwal, S.; Jones, D.; Young, B.; Sutton, A. Synthesising qualitative and quantitative evidence: A review of possible methods. J. Health Serv. Res. Policy 2005, 10, 45–53. [Google Scholar] [CrossRef]
- Tong, A.; Flemming, K.; McInnes, E.; Oliver, S.; Craig, J. Enhancing transparency in reporting the synthesis of qualitative research: ENTREQ. BMC Med. Res. Methodol. 2012, 12, 181. [Google Scholar] [CrossRef] [Green Version]
- Saini, M.; Shlonsky, A. Systematic Synthesis of Qualitative Research, 1st ed.; Oxford University Press: New York, NY, USA, 2012; ISBN 9780195387216. [Google Scholar]
- Bates, M.J. The design of browsing and berrypicking techniques for the online search interface. Online Rev. 1989, 13, 407–424. [Google Scholar] [CrossRef] [Green Version]
- Critical Appraisal Skills Programme (CASP). Qualitative Research: Appraisal Tool. 10 Questions to Help You Make Sense of Qualitative Research. Available online: www.phru.nhs.uk/Doc_Links/Qualitative_Appraisal_Tool.pdf (accessed on 10 May 2014).
- Corbin, J.M.; Strauss, A. Grounded theory research: Procedures, canons, and evaluative criteria. Qual. Sociol. 1990, 13, 3–21. [Google Scholar] [CrossRef]
- Drisko, J.W. Strengthening qualitative studies and reports. J. Soc. Work Educ. 1997, 33, 185–187. [Google Scholar] [CrossRef]
- Zhao, X.; Davey, G. Contesting modernity: Tobacco use and romanticism among older Dai farmers in Xishuangbanna, China. Soc. Health Illn. 2015, 37, 1173–1190. [Google Scholar] [CrossRef]
- Starks, H.; Trinidad, S.B. Choose your method: A comparison of phenomenology, discourse analysis, and grounded theory. Qual. Health Res. 2007, 17, 1372–1380. [Google Scholar] [CrossRef]
- Lawton, J.; Ahmad, N.; Hallowell, N.; Hanna, L.; Douglas, M. Perceptions and experiences of taking oral hypoglycaemic agents among people of Pakistani and Indian origin: Qualitative study. BMJ 2005, 330, 1247. [Google Scholar] [CrossRef] [Green Version]
- Lawton, J.; Ahmad, N.; Hanna, L.; Douglas, M.; Hallowell, N. ‘I can’t do any serious exercise’: Barriers to physical activity amongst people of Pakistani and Indian origin with Type 2 diabetes. Health Educ. Res. 2006, 21, 43–54. [Google Scholar] [CrossRef]
- Lawton, J.; Ahmad, N.; Hanna, L.; Douglas, M.; Bains, H.; Hallowell, N. ‘We should change ourselves, but we can’t’: Accounts of food and eating practices amongst British Pakistanis and Indians with type 2 diabetes. Ethn. Health 2008, 13, 305–319. [Google Scholar] [CrossRef] [Green Version]
- Bissell, P.; May, C.R.; Noyce, P.R. From compliance to concordance: Barriers to accomplishing a re-framed model of health care interactions. Soc. Sci. Med. 2004, 58, 851–862. [Google Scholar] [CrossRef]
- Macaden, L. Risk Perception among Older South Asians with Type 2 Diabetes in the United Kingdom; Northumbria University: Newcastle, UK, 2009. [Google Scholar]
- Choudhury, S.M.; Brophy, S.; Williams, R. Understanding and beliefs of diabetes in the UK Bangladeshi population. Diabet. Med. 2009, 26, 636–640. [Google Scholar] [CrossRef] [PubMed]
- Lucas, A.; Murray, E.; Kinra, S. Heath beliefs of UK South Asians related to lifestyle diseases: A review of qualitative literature. J. Obes. 2013, 827674. [Google Scholar] [CrossRef] [Green Version]
- Mu’Min Chowdhury, A.; Helman, C.; Greenhalgh, T. Food beliefs and practices among British Bangladeshis with diabetes: Implications for health education. Anthropol. Med. 2000, 7, 209–226. [Google Scholar] [CrossRef]
- Macaden, L.; Clarke, C.L. Risk perception among older South Asian people in the UK with type 2 diabetes. Int. J. Older People Nurs. 2006, 1, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Macaden, L.; Clarke, C.L. The influence of locus of control on risk perception in older South Asian people with Type 2 diabetes in the UK. J. Nurs. Healthc. Chronic Illn. 2010, 2, 144–152. [Google Scholar] [CrossRef]
- Duthie-Nurse, G. An anthropological study into the views on diet and disease of a sample of Hindu Gujarati-speaking women with type 2 diabetes. Pract. Diabetes Int. 1998, 15, 109–111. [Google Scholar] [CrossRef]
- Fleming, E.; Carter, B.; Pettigrew, J. The influence of culture on diabetes self-management: Perspectives of Gujarati Muslim men who reside in northwest England. J. Clin. Nurs. 2008, 17, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Greenhalgh, T.; Helman, C.; Chowdhury, A.M. Health beliefs and folk models of diabetes in British Bangladeshis: A qualitative study. BMJ 1998, 316, 978–983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gumbler, L. Knowledge gaps and other barriers in type 2 diabetes management: Findings from interviews with South Asian women. Diabetes Prim. Care 2014, 16, 86–91. [Google Scholar]
- Jepson, R.; Harris, F.M.; Bowes, A.; Robertson, R.; Avan, G.; Sheikh, A. Physical activity in South Asians: An in-depth qualitative study to explore motivations and facilitators. PLoS ONE 2012, 7, e45333. [Google Scholar] [CrossRef] [Green Version]
- Kelleher, D.; Islam, S. “How should I live?” Bangladeshi people and non-insulin-dependent diabetes. In Researching Cultural Differences in Health; Kelleher, D., Hiller, S., Eds.; Routledge: London, UK, 1996; pp. 220–237. ISBN 9780415111836. [Google Scholar]
- Khajuria, S.; Thomas, J. Traditional Indian beliefs about the dietary management of diabetes—An exploratory study of the implications for the management of Gujarati diabetics in Britain. J. Hum. Nutr. Diet. 1992, 5, 311–321. [Google Scholar] [CrossRef]
- Majeed-Ariss, R.; Jackson, C.; Knapp, P.; Cheater, F.M. British-Pakistani women’s perspectives of diabetes self-management: The role of identity. J. Clin. Nurs. 2015, 24, 2571–2580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, V.; Iliffe, S. An exploratory study into the health beliefs and behaviours of British Indians with type II diabetes. Prim. Health Care Res. Dev. 2017, 18, 97–103. [Google Scholar] [CrossRef] [Green Version]
- Pardhan, S.; Nakafero, G.; Raman, R.; Sapkota, R. Barriers to diabetes awareness and self-help are influenced by people’s demographics: Perspectives of South Asians with type 2 diabetes. Ethn. Health 2020, 25, 843–861. [Google Scholar] [CrossRef]
- Prinjha, S.; Ricci-Cabello, I.; Newhouse, N.; Farmer, A. British South Asian Patients’ Perspectives on the Relevance and Acceptability of Mobile Health Text Messaging to Support Medication Adherence for Type 2 Diabetes: Qualitative Study. JMIR Mhealth Uhealth 2020, 8, e15789. [Google Scholar] [CrossRef] [PubMed]
- Public Health England. Government Dietary Recommendations. Government Recommendations for Energy and Nutrients for Males and Females Aged 1–18 Years and 19+ Years. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/618167/government_dietary_recommendations.pdf (accessed on 6 June 2020).
- Schreffler, G. Situating bhangra dance: A critical introduction. South Asian Hist. Cult. 2013, 4, 384–412. [Google Scholar] [CrossRef]
- Barnes, J. Pharmacovigilance of herbal medicines: A UK perspective. Drug Saf. 2003, 26, 829–851. [Google Scholar] [CrossRef]
- Vickers, K.A.; Jolly, K.B.; Greenfield, S.M. Herbal medicine: Women’s views, knowledge and interaction with doctors: A qualitative study. BMC Complement. Altern. Med. 2006, 6, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janis, I.L.; Mann, L. Decision Making: A Psychological Analysis of Conflict, Choice, and Commitment; Free Press: New York, NY, USA, 1977. [Google Scholar]
- Riaz, M.N.; Chaudry, M.M. Halal Food Production, 1st ed.; CRC Press: Boca Raton, FL, USA, 2003; ISBN 9781587160295. [Google Scholar]
- Soon, J.M.; Chandia, M.; Regenstein, J.M. Halal integrity in the food supply chain. Br. Food J. 2017, 119, 39–51. [Google Scholar] [CrossRef]
- Frost, J.; Garside, R.; Cooper, C.; Britten, N. A qualitative synthesis of diabetes self-management strategies for long term medical outcomes and quality of life in the UK. BMC Health Serv. Res. 2014, 14, 348. [Google Scholar] [CrossRef] [Green Version]
- Munster, V.J.; Koopmans, M.; van Doremalen, N.; van Riel, D.; de Wit, E. A novel coronavirus emerging in China—Key questions for impact assessment. N. Engl. J. Med. 2020, 382, 692–694. [Google Scholar] [CrossRef] [PubMed]
- Our World in Data. Coronavirus (COVID-19) Deaths. Available online: https://ourworldindata.org/covid-deaths#what-is-the-total-number-of-confirmed-deaths (accessed on 3 February 2021).
- Public Health England. Deaths in United Kingdom. Available online: https://coronavirus.data.gov.uk/details/deaths (accessed on 3 February 2021).
- Gupta, R.; Ghosh, A.; Singh, A.K.; Misra, A. Clinical considerations for patients with diabetes in times of COVID-19 epidemic. Diabetes Metab. Syndr. 2020, 14, 211. [Google Scholar] [CrossRef]
- Khunti, K.; Singh, A.K.; Pareek, M.; Hanif, W. Is ethnicity linked to incidence or outcomes of covid-19? BMJ 2020, 369, m1548. [Google Scholar] [CrossRef] [Green Version]
- Sze, S.; Pan, D.; Nevill, C.R.; Gray, L.J.; Martin, C.A.; Nazareth, J.; Minhas, J.S.; Divall, P.; Khunti, K.; Abrams, K.R. Ethnicity and clinical outcomes in COVID-19: A systematic review and meta-analysis. EClinicalMedicine 2020, 100630. [Google Scholar] [CrossRef]
- Treweek, S.; Forouhi, N.G.; Narayan, K.V.; Khunti, K. COVID-19 and ethnicity: Who will research results apply to? The Lancet 2020, 395, 1955–1957. [Google Scholar] [CrossRef]
- Taher, N.; Huda, M.S.; Chowdhury, T.A. COVID-19 and diabetes: What have we learned so far? Clin. Med. 2020, 20, e87. [Google Scholar] [CrossRef]
- Hambling, C.; Patel, D.; Turner, B. COVID-19 and diabetes: Update for primary care in response to the ongoing coronavirus pandemic. Diabetes Prim. Care 2021, 23, 9–12. [Google Scholar]
- Association of British Clinical Diabetologists. Concise Advice on Inpatient Diabetes during COVID-19—Front Door Guidance. Available online: https://abcd.care/resource/concise-advice-inpatient-diabetes-during-covid-19-front-door-guidance (accessed on 3 February 2021).
- Hanif, S.; Ali, S.; Hassanein, M.; Khunti, K.; Hanif, W. Managing People with Diabetes Fasting for Ramadan During the COVID-19 Pandemic: A South Asian Health Foundation Update. Diabet. Med. 2020, 37, 1094–1102. [Google Scholar] [CrossRef] [PubMed]
- Robertson, E.; Reeve, K.S.; Niedzwiedz, C.L.; Moore, J.; Blake, M.; Green, M.; Katikireddi, S.V.; Benzeval, M.J. Predictors of COVID-19 vaccine hesitancy in the UK Household Longitudinal Study. medRxiv 2020, 20248899. [Google Scholar] [CrossRef]
- Public Health England. Beyond the Data: Understanding the Impact of COVID-19 on BAME Groups. June 2020. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/892376/COVID_stake-holder_engagement_synthesis_beyond_the_data.pdf (accessed on 3 February 2021).
- Ricci-Cabello, I.; Ruiz-Perez, I.; Rojas-Garcia, A.; Pastor, G.; Rodriguez-Barranco, M.; Goncalves, D.C. Characteristics and effectiveness of diabetes self-management educational programs targeted to racial/ethnic minority groups: A systematic review, meta-analysis and meta-regression. BMC Endocr. Disord. 2014, 14, 60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhurji, N.; Javer, J.; Gasevic, D.; Khan, N.A. Improving management of type 2 diabetes in South Asian patients: A systematic review of intervention studies. BMJ Open 2016, 6, e008986. [Google Scholar] [CrossRef] [PubMed]
- Kossarova, L.; Blunt, I.; Bardsley, M. Focus on: International Comparisons of Healthcare Quality–Appendices; The Health Foundation and the Nuffield Trust. Available online: https://www.nuffieldtrust.org.uk/files/2018-10/1540242826_qualitywatch-international-comparisons-appendices.pdf (accessed on 18 December 2020).
- Ali, S.H.; Misra, S.; Parekh, N.; Murphy, B.; DiClemente, R.J. Preventing Type 2 Diabetes among South Asian Americans through community-based lifestyle interventions: A systematic review. Prev. Med. Rep. 2020, 20, 101182. [Google Scholar] [CrossRef] [PubMed]
- Aronson, R.; Chu, L.; Joseph, N.; Brown, R. Prevalence and risk Evaluation of Diabetic complications of the foot among Adults with type 1 and type 2 diabetes in a Large Canadian population (PEDAL study). Can. J. Diabetes 2020, in press. [Google Scholar] [CrossRef] [PubMed]
- Veenstra, G.; Vas, M.; Sutherland, D.K. Asian-White health inequalities in Canada: Intersections with immigration. J. Immigr. Minority Health 2020, 22, 300–306. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Reference, Author, Year of Publication | Purpose/Objectives | Sample Size | Location | Method of Data Collection | Data Analysis | Main Results/Key Findings |
|---|---|---|---|---|---|---|
| Khajuria and Thomas (1992) [72] | Explore the extent to which traditional beliefs about diet, health and diabetes, as described in the classics of Ayurvedic medicine, are held by Indian (Gujarati) diabetics in Britain. | 28 Gujarati, Hindu, vegetarian, patients with diabetes | Diabetic clinics at two London Hospitals. (England) | Interviews | No clear indication as to which analysis applied, however, results are shown in themes |
|
| Kelleher and Islam (1994) [71] | To understand and describe how Bangladeshi people with diabetes attempt to integrate a traditional and religious rule-governed system of eating with modern medicine. | 40 Bangladeshi, 25 males and 15 females, varying ages. 30 family members | One health centre in the Tower Hamlets district. (England) | Interviews and Observations | Preliminary analysis on a selected sample of n = 20, 12 men and 8 females. Unknown how the sample was selected for analysis. |
|
| Chowdhury et al. (2000) [63] | Report on the food beliefs and classification system of British Bangladeshis. | 40 informants with diabetes, all immigrants from the Sylhet region of Bangladesh | Inner-city areas of Tower Hamlets, Newham or Islington in London. (England) | Audiotaped narrative, Semi-structured interviews,Focus groups,Construction of genogram, Pile sorting exercises,Structured vignette method,Feedback of preliminary constructs to focus groups,Study of patients’ general practice case notes | Anthropological analysis.No quotes from participants as evidence. Interpretative commentary with reference to the previous evidence base. |
|
| Bissell et al. (2004) [59] | Explore the relevance of a re-framed consultation with a small group of English speaking patients of Pakistani origin with a diagnosis of T2D | 21 Pakistani origin participants | Two primary practices and one secondary care diabetes centre located in the northwest of England. | Semi-structured interviews | Grounded theory |
|
| Lawton et al. (2005) [56] | To explore British Pakistani and British Indian patients’ perceptions and experiences of taking OHAs. | 32 patients of Pakistani and Indian origin with T2D. | Primary care and community sources in Edinburgh, Scotland. | An observational cross-sectional study using in-depth interviews in English or Punjabi. | Grounded theory |
|
| Macden and Clarke (2006) [64] | Developed knowledge of the experiences of South Asian people with diabetes in the UK in relation to socio-cultural and dietary practices, religion and ageing influences on the perception and understanding of risks. | Ethnic health development workers, health professionals and 20 SA men and women with T2D. | North East England. | Focus group interviews and one-to-one interviews | Grounded theory |
|
| Lawton et al. (2006) [57] | Explore patient perceptions and experiences of undertaking PA as part of their diabetes care. | 32 participants (Indian, n = 9; Pakistani, n= 23). | Five general practises in Edinburgh. (Scotland) | Semi-structured interviews | Grounded theory |
|
| Lawton et al. (2008) [58] | To look at food and eating practices from Pakistanis and Indians’ perspectives with T2D, their perceptions of the barriers and facilitators to dietary change, and the social and cultural factors informing their accounts. | 23 Pakistanis (22 Muslims, one Christian) and nine Indians (four Hindus, five Sikhs) | Five general practices in Edinburgh | Semi-structured interviews | Grounded theory |
|
| Choudhury et al. (2009) [61] | Examine the understanding beliefs of people with T2D from the Bangladeshi community living in the UK. | 14 Bangladeshis | Swansea or Birmingham (Wales/England) | Structured Interviews | Theme analysis |
|
| Macaden and Clarke (2010) [65] | To analyse risk perception among older SA people with T2Din the UK. | Ten Health development workers, seven individual interviews with practitioners (three physicians, three nurse specialists and a dietitian); 20 interviews with UK-resident older SAs (nine men and eleven women) with T2D | North East of England. | Two focus group interviews with health development workers, seven individual interviews with practitioners | Grounded theory with its theoretical foundations drawn from Symbolic Interactionism. |
|
| Jepson et al. (2012) [70] | Explore the barriers, motivators and facilitators to SA adults undertaking PA, with the broader aim of guiding the development of future interventions and services. | 59 Bangladeshi, Indian and Pakistani participants 10 Key Informants | Urban areas of Scotland, Aberdeen, Glasgow and Edinburgh. | Focus group discussions with participants and semi-structured interviews with key informants, | Thematic analysis |
|
| Gumbler (2014) [69] | Investigate whether there was a knowledge gap among SA women with T2D about diabetes development and management. | Six SA women | Warwickshire or in Birmingham | semi-structured interviews | No clear indication as to which analysis was used, however, results are shown in themes |
|
| Majeed-Ariss et al. (2015) [73] | To explore the effects of T2Don British-Pakistani Women’s identity and its relationship with self-management. | 15 British-Pakistani women with T2D. | Teesside, England | Face-to-face semi-structured English and Urdu language interviews | Thematic analysis |
|
| Fleming, Carter, Pettigrew. (2008) [67] | To present the findings of a study which explored the influence of culture on (type 2) diabetes self-management in Gujarati Muslim men who reside in northwest England. | 5 Gujarati Muslim men | Northwest England | A case-study approach | Topic and analytic coding |
|
| Greenhalgh et al. (1998) [68] | To explore the experience of diabetes in British Bangladeshis, since successful management of diabetes requires attention not just to observable behaviour but to the underlying attitudes and belief systems which drive that behaviour. | 40 British Bangladeshi patients | Three general practices in East London | Audiotaped narrative Semi-structured interview Focus group discussion Construction of genogram Pile sorting exercises Structured vignette method Feedback of preliminary constructs to focus groups Study of patients’ general practice case notes | No clear indication as to which analysis was used |
|
| Duthie-Nurse (1998) [66] | The patients’ views of illness and how it was treated, with particular regard to diet | 20 Hindu SA women | Diabetes Clinic, St Georges Hospital, South West London | Open and closed-ended interviews | No clear indication as to which analysis was used |
|
| Patel and Iliffe (2016) [74] | To explore the influence of health beliefs and behaviours on diabetes management in British Indians, as successful management of diabetes is dependent on underlying cultural beliefs and behaviours. | 10 British Indians | General Practice in North West London | Semi-structured interviews Pile sorting exercise | Thematic analysis |
|
| Pardhan et al. (2018) [75] | To determine whether diabetes awareness and self-help barriers differ in South Asian participants of different demographic characteristics (age, gender, and literacy) with type 2 diabetes living in the United Kingdom. | 35 participants, 26 were Pakistani, 5 Nepalese and 4 Indians | Five focus groups in community centres in Peterborough and one focus group in a research facility at Anglia Ruskin University, Cambridge campus. | Six Focus group discussions | Thematic analysis |
|
| Prinjha, Ricci-Cabello et al. (2020) [76] | Aimed to explore British South Asian patients’ perceptions and views with T2D on mobile health SMS text messaging to support medication adherence, aimed at the general UK population. | A diverse sample of 67 participants (Indian, Pakistani, Bangladeshi, and Sri Lankan) | Community centres in Leicester | Eight Focus group discussion | Thematic analysis |
|
| Synthesising Argument | Synthetic Construct (Themes Developed from the Analysis of Articles) | Supporting Evidence from Studies |
|---|---|---|
| Cultural Conflict vs. T2D Management | ||
| Decisional Conflict for Self-management Behaviours | Diet and food
|
|
Physical Activity
|
| |
Medication
|
| |
| Management Strategies and Factors Influencing Conflict | Social Conflict
|
|
| Religious obligations | [57,58,63,64,66] | |
| Healthcare delivery/relationship | [56,58,59,61,65,67,71,74,75] | |
Health Beliefs, language and literacy
|
| |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patel, T.; Umeh, K.; Poole, H.; Vaja, I.; Newson, L. Cultural Identity Conflict Informs Engagement with Self-Management Behaviours for South Asian Patients Living with Type-2 Diabetes: A Critical Interpretative Synthesis of Qualitative Research Studies. Int. J. Environ. Res. Public Health 2021, 18, 2641. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052641
Patel T, Umeh K, Poole H, Vaja I, Newson L. Cultural Identity Conflict Informs Engagement with Self-Management Behaviours for South Asian Patients Living with Type-2 Diabetes: A Critical Interpretative Synthesis of Qualitative Research Studies. International Journal of Environmental Research and Public Health. 2021; 18(5):2641. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052641
Chicago/Turabian StylePatel, Tasneem, Kanayo Umeh, Helen Poole, Ishfaq Vaja, and Lisa Newson. 2021. "Cultural Identity Conflict Informs Engagement with Self-Management Behaviours for South Asian Patients Living with Type-2 Diabetes: A Critical Interpretative Synthesis of Qualitative Research Studies" International Journal of Environmental Research and Public Health 18, no. 5: 2641. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052641