
Associated Factors and Survival Outcomes for Breast Conserving Surgery versus Mastectomy among New Zealand Women with Early-Stage Breast Cancer

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
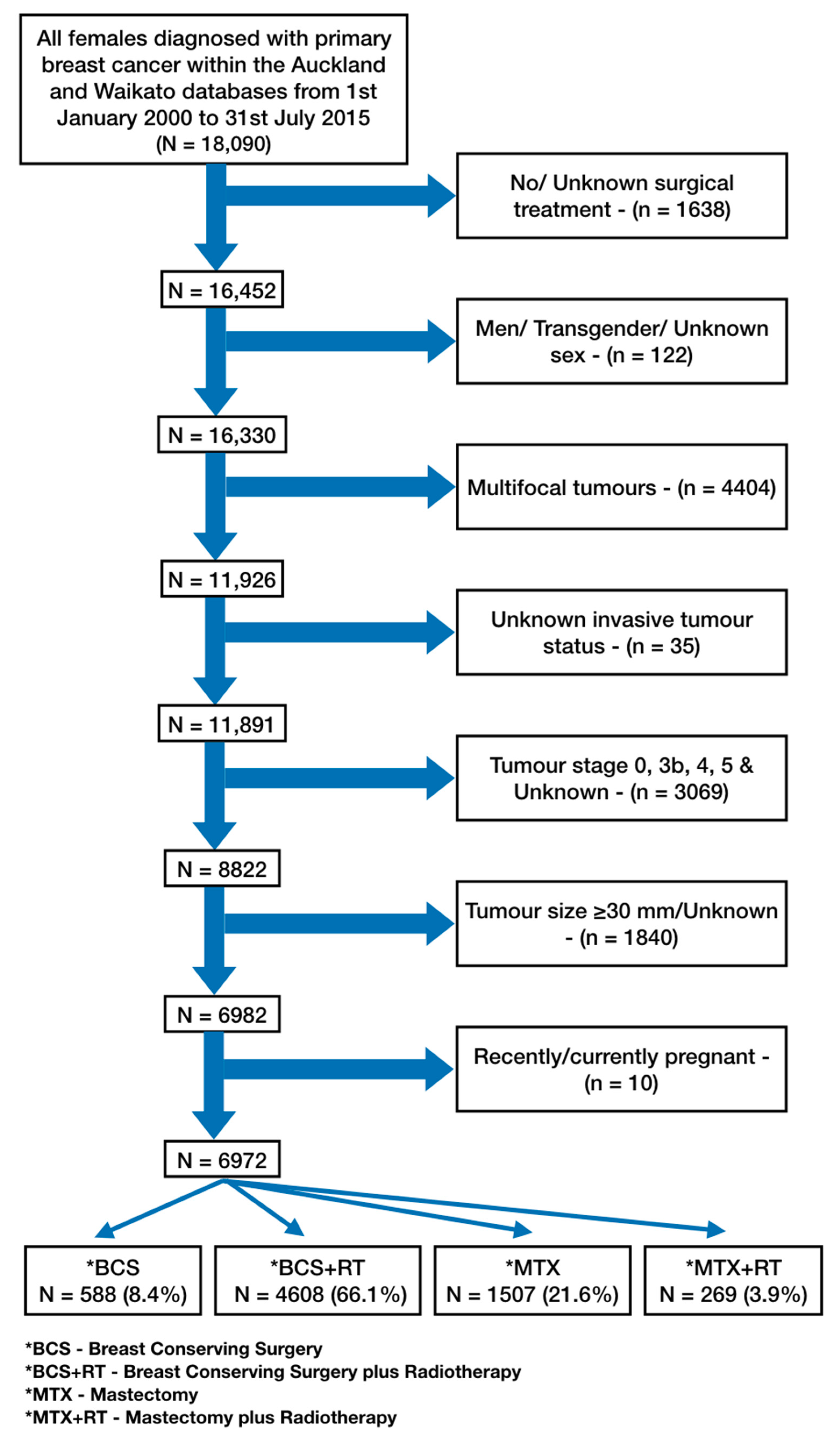
2.1. Study Population
2.2. Data Sources
2.3. Variables of Interest
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Factors Associated with the Receipt of BCS + RT
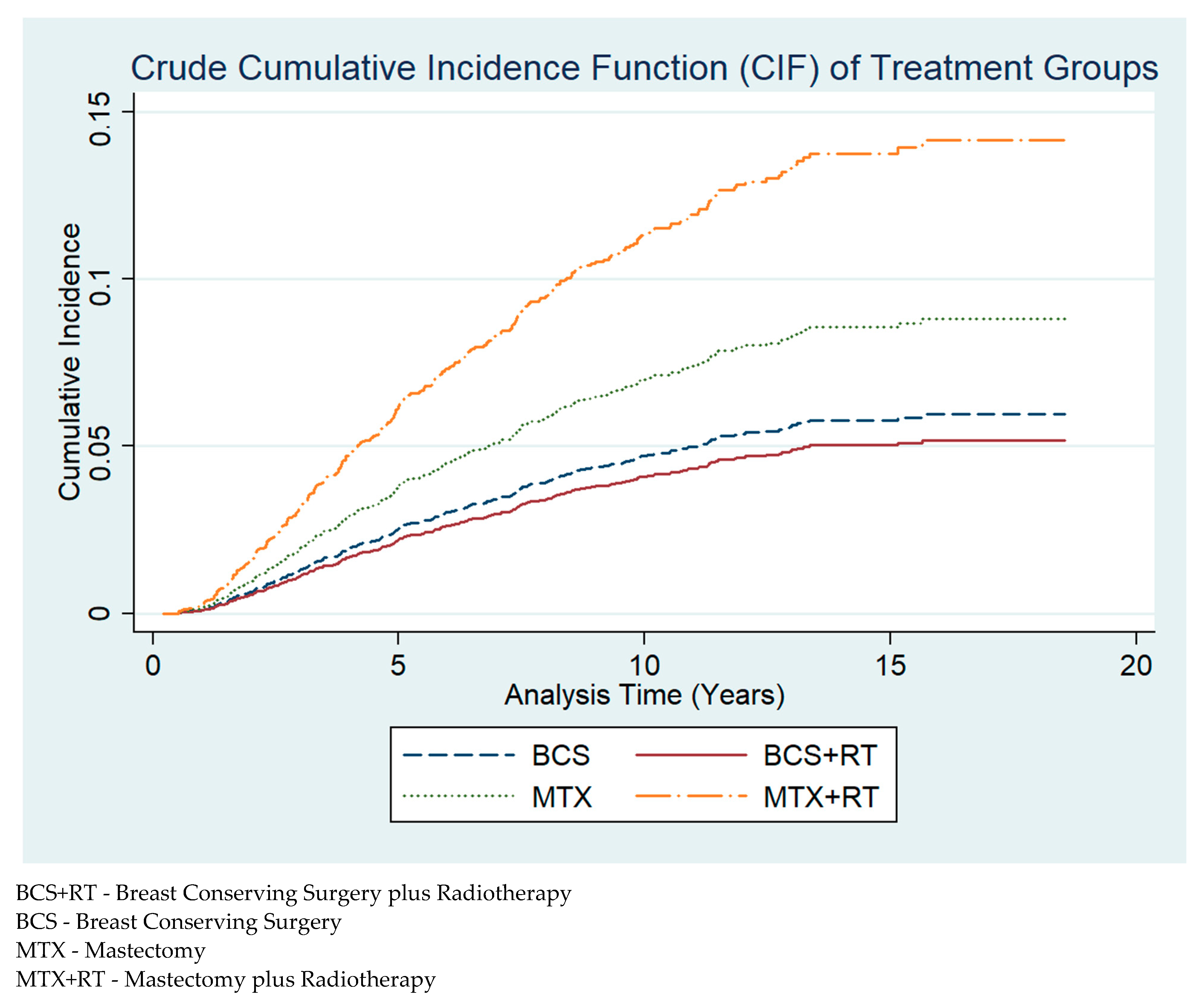
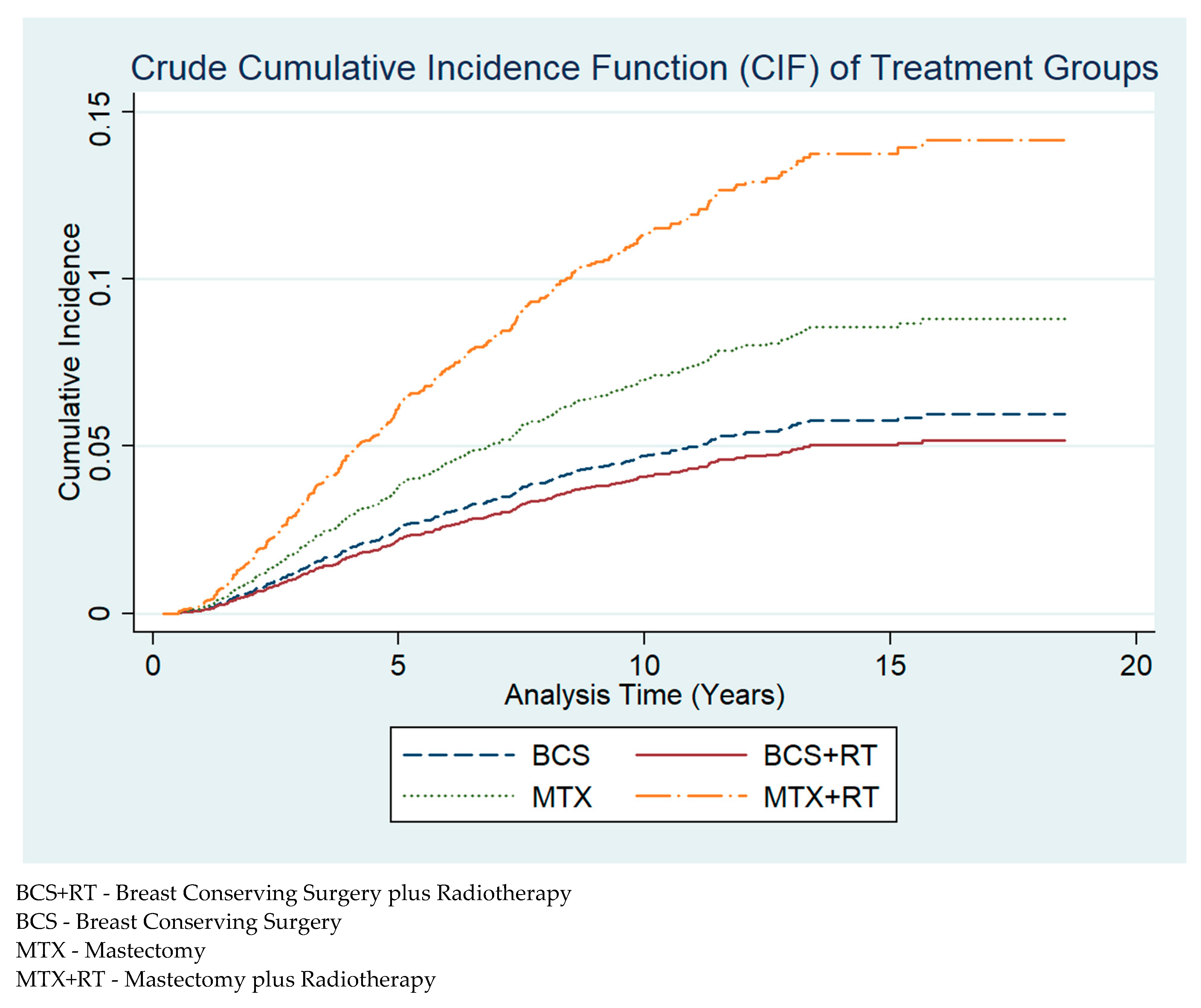
3.3. Breast Cancer-Specific Death
4. Discussion
4.1. Main Findings
4.2. Interpretation
4.3. Strengths
4.4. Limitations
4.5. Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Factors | Total | BCS 1 | BCS + RT 2 | MTX 3 | MTX + RT 4 | ||||
|---|---|---|---|---|---|---|---|---|---|
| No. | Row% | No. | Row% | No. | Row% | No. | Row% | ||
| Total No. | 6972 | 588 | 8.4 | 4608 | 66.1 | 1507 | 21.6 | 269 | 3.9 |
| DEMOGRAPHIC VARIABLES | |||||||||
| Median Age | 58 (50–66) 5 | 58 (49–68) 5 | 58 (50–65) 5 | 61 (51–71) 5 | 53 (45–63) 5 | ||||
| Age Group | |||||||||
| <45 | 789 | 78 | 9.9 | 475 | 60.2 | 172 | 21.8 | 64 | 8.1 |
| 45–59 | 3006 | 236 | 7.9 | 2124 | 70.7 | 531 | 17.7 | 115 | 3.8 |
| 60–74 | 2538 | 184 | 7.2 | 1767 | 69.6 | 523 | 20.6 | 64 | 2.5 |
| 75+ | 639 | 90 | 14.1 | 242 | 37.9 | 281 | 44.0 | 26 | 4.1 |
| Ethnicity | |||||||||
| European | 5180 | 429 | 8.3 | 3495 | 67.5 | 1063 | 20.5 | 193 | 3.7 |
| Māori | 653 | 50 | 7.7 | 427 | 65.4 | 139 | 21.3 | 37 | 5.7 |
| Pacific | 229 | 29 | 12.7 | 142 | 62.0 | 53 | 23.1 | 5 | 2.2 |
| Other | 715 | 58 | 8.1 | 410 | 57.3 | 218 | 30.5 | 29 | 4.1 |
| Unknown | 195 | 22 | 11.3 | 134 | 68.7 | 34 | 17.4 | 5 | 2.6 |
| NZ Deprivation | |||||||||
| 1–2 | 1534 | 140 | 9.1 | 1021 | 66.6 | 307 | 20.0 | 66 | 4.3 |
| 3–4 | 1394 | 108 | 7.7 | 954 | 68.4 | 296 | 21.2 | 36 | 2.6 |
| 5–6 | 1415 | 118 | 8.3 | 940 | 66.4 | 298 | 21.1 | 59 | 4.2 |
| 7–8 | 1121 | 80 | 7.1 | 760 | 67.8 | 233 | 20.8 | 48 | 4.3 |
| 9–10 | 1289 | 117 | 9.1 | 792 | 61.4 | 326 | 25.3 | 54 | 4.2 |
| Unknown | 219 | 25 | 11.4 | 141 | 64.4 | 47 | 21.5 | 6 | 2.7 |
| Main Urban Areas | |||||||||
| Urban | 6252 | 515 | 8.2 | 4112 | 65.8 | 1377 | 22.0 | 248 | 4.0 |
| Rural | 496 | 46 | 9.3 | 353 | 71.2 | 81 | 16.3 | 16 | 3.2 |
| Unknown | 224 | 27 | 12.1 | 143 | 63.8 | 49 | 21.9 | 5 | 2.2 |
| Region | |||||||||
| Auckland | 5479 | 468 | 8.5 | 3526 | 64.4 | 1287 | 23.5 | 198 | 3.6 |
| Waikato | 1493 | 120 | 8.0 | 1082 | 72.5 | 220 | 14.7 | 71 | 4.8 |
| Public/Private | |||||||||
| Public | 2245 | 170 | 7.6 | 1574 | 70.1 | 416 | 18.5 | 85 | 3.8 |
| Private | 4727 | 418 | 8.8 | 3034 | 64.2 | 1091 | 23.1 | 184 | 3.9 |
| CLINICAL VARIABLES | |||||||||
| Year of Diagnosis | |||||||||
| 2000–2004 | 1861 | 143 | 7.7 | 1165 | 62.6 | 456 | 24.5 | 97 | 5.2 |
| 2005–2009 | 2240 | 148 | 6.6 | 1520 | 67.9 | 489 | 21.8 | 83 | 3.7 |
| 2010–2015 | 2871 | 297 | 10.3 | 1923 | 67.0 | 562 | 19.6 | 89 | 3.1 |
| Screen-Detected/Symptomatic | |||||||||
| Screen-Detected | 3605 | 283 | 7.9 | 2675 | 74.2 | 587 | 16.3 | 60 | 1.7 |
| Symptomatic | 3367 | 305 | 9.1 | 1933 | 57.4 | 920 | 27.3 | 209 | 6.2 |
| Stage | |||||||||
| IA | 4521 | 434 | 9.6 | 3192 | 70.6 | 854 | 18.9 | 41 | 0.9 |
| IB | 193 | 17 | 8.8 | 133 | 68.9 | 37 | 19.2 | 6 | 3.1 |
| IIA | 1587 | 104 | 6.6 | 963 | 60.7 | 452 | 28.5 | 68 | 4.3 |
| IIB | 446 | 27 | 6.1 | 208 | 46.6 | 149 | 33.4 | 62 | 13.9 |
| IIIA | 225 | 6 | 2.7 | 112 | 49.8 | 15 | 6.7 | 92 | 40.9 |
| Grade | |||||||||
| 1 | 2191 | 218 | 9.9 | 1572 | 71.7 | 373 | 17.0 | 28 | 1.3 |
| 2 | 3182 | 251 | 7.9 | 2050 | 64.4 | 756 | 23.8 | 125 | 3.9 |
| 3 | 1545 | 109 | 7.1 | 960 | 62.1 | 362 | 23.4 | 114 | 7.4 |
| Unknown | 54 | 10 | 18.5 | 26 | 48.1 | 16 | 29.6 | 2 | 3.7 |
| Hormone Receptor Status | |||||||||
| ER 6 and PR 7 negative | 1018 | 72 | 7.1 | 600 | 58.9 | 264 | 25.9 | 82 | 8.1 |
| ER 6 and PR 7 positive | 4801 | 413 | 8.6 | 3270 | 68.1 | 975 | 20.3 | 143 | 3.0 |
| ER 6 or PR 7 positive | 1016 | 90 | 8.9 | 661 | 65.1 | 227 | 22.3 | 38 | 3.7 |
| Unknown | 137 | 13 | 9.5 | 77 | 56.2 | 41 | 29.9 | 6 | 4.4 |
| Histology | |||||||||
| Ductal | 5909 | 472 | 8.0 | 3912 | 66.2 | 1286 | 21.8 | 239 | 4.0 |
| Lobular | 567 | 45 | 7.9 | 361 | 63.7 | 140 | 24.7 | 21 | 3.7 |
| Other | 496 | 71 | 14.3 | 335 | 67.5 | 81 | 16.3 | 9 | 1.8 |
| Tumour Size (mm) | |||||||||
| <20 | 4847 | 445 | 9.2 | 3452 | 71.2 | 859 | 17.7 | 91 | 1.9 |
| ≥20–≤50 | 2125 | 143 | 6.7 | 1156 | 54.4 | 648 | 30.5 | 178 | 8.4 |
| Positive Lymph Node | |||||||||
| 0 | 5453 | 498 | 9.1 | 3717 | 68.2 | 1169 | 21.4 | 69 | 1.3 |
| 1–3 | 1295 | 85 | 6.6 | 779 | 60.2 | 323 | 24.9 | 108 | 8.3 |
| 4+ | 224 | 5 | 2.2 | 112 | 50.0 | 15 | 6.7 | 92 | 41.1 |
| Lympho-vascular Invasion | |||||||||
| Yes | 5799 | 508 | 8.8 | 3885 | 67.0 | 1254 | 21.6 | 152 | 2.6 |
| No | 1173 | 80 | 6.8 | 723 | 61.6 | 253 | 21.6 | 117 | 10.0 |
| SYSTEMIC TREATMENT VARIABLES | |||||||||
| Systemic Treatment | |||||||||
| None | 2303 | 275 | 11.9 | 1464 | 63.6 | 545 | 23.7 | 19 | 0.8 |
| Both | 932 | 44 | 4.7 | 602 | 64.6 | 180 | 19.3 | 106 | 11.4 |
| Chemotherapy | 711 | 47 | 6.6 | 449 | 63.2 | 141 | 19.8 | 74 | 10.4 |
| Hormonal therapy | 2961 | 204 | 6.9 | 2064 | 69.7 | 624 | 21.1 | 69 | 2.3 |
| Unknown | 65 | 18 | 27.7 | 29 | 44.6 | 17 | 26.2 | 1 | 1.5 |
References
- International Agency for Research on Cancer. Estimated Number of Deaths in 2018, Worldwide, Females, All Ages. In Estim. Number Deaths 2018 Worldw. Females Ages. 2018. Available online: https://gco.iarc.fr/today/online-analysis-table?v=2018&mode=cancer&mode_population=countries&population=900&populations=&key=asr&sex=2&cancer=39&type=1&statistic=5&prevalence=0&population_group=18&ages_group%5B%5D=0&ages_group%5B%5D=17&group_cancer=1&include_nmsc=1&include_nmsc_other=1#collapse-group-0-5 (accessed on 26 June 2020).
- Ministry of Health. Management of Early Breast Cancer—Evidence-based Best Practice Guideline; Ministry of Health: Wellington, New Zealand, 2009.
- Nationaal Borstkanker Overleg Nederland (NBON). Dutch Breast Cancer Guidelines; NABON: Utrecht, The Netherlands, 2012. [Google Scholar]
- National Comprehensive Cancer Network. NCCN Guidelines for Patients Invasive Breast Cancer; Harbourside Press: Huntington, NY, USA, 2020. [Google Scholar]
- National Health Commission of the People’s Republic of China. Chinese guidelines for diagnosis and treatment of breast cancer 2018 (English version). Chin. J. Cancer Res. 2019, 31, 259–277. [Google Scholar] [CrossRef]
- Litière, S.; Werutsky, G.; Fentiman, I.S.; Rutgers, E.; Christiaens, M.-R.; Van Limbergen, E.; Baaijens, M.H.A.; Bogaerts, J.; Bartelink, H. Breast conserving therapy versus mastectomy for stage I–II breast cancer: 20 year follow-up of the EORTC 10801 phase 3 randomised trial. Lancet Oncol. 2012, 13, 412–419. [Google Scholar] [CrossRef]
- Veronesi, U.; Cascinelli, N.; Mariani, L.; Greco, M.; Saccozzi, R.; Luini, A.; Aguilar, M.; Marubini, E. Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. N. Engl. J. Med. 2002, 347, 1227–1232. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, S.; Pappas, L.; Neumayer, L.; Kokeny, K.; Agarwal, J. Effect of breast conservation therapy vs mastectomy on disease-specific survival for early-stage breast cancer. JAMA Surg. 2014, 149, 267–274. [Google Scholar] [CrossRef] [Green Version]
- Onitilo, A.A.; Engel, J.M.; Stankowski, R.V.; Doi, S.A. Survival comparisons for breast conserving surgery and mastectomy revisited: Community experience and the role of radiation therapy. Clin. Med. Res. 2015, 13, 65–73. [Google Scholar] [CrossRef] [Green Version]
- Morris, C.R.; Cohen, R.; Schlag, R.; Wright, W.E. Increasing trends in the use of breast-conserving surgery in California. Am. J. Public Health 2000, 90, 281–284. [Google Scholar] [PubMed] [Green Version]
- Albain, K.S.; Green, S.R.; Lichter, A.S.; Hutchins, L.F.; Wood, W.C.; Henderson, I.C.; Ingle, J.N.; O’Sullivan, J.; Osborne, C.K.; Martino, S. Influence of patient characteristics, socioeconomic factors, geography, and systemic risk on the use of breast-sparing treatment in women enrolled in adjuvant breast cancer studies: An analysis of two intergroup trials. J. Clin. Oncol. 1996, 14, 3009–3017. [Google Scholar] [CrossRef]
- Elwood, J.M.; Marshall, R.J.; Tin Tin, S.; Barrios, M.E.; Harvey, V.J. Bias in survival estimates created by a requirement for consent to enter a clinical breast cancer registry. Cancer Epidemiol. 2019, 58, 178–183. [Google Scholar] [CrossRef]
- Seneviratne, S.; Campbell, I.; Scott, N.; Shirley, R.; Peni, T.; Lawrenson, R. Accuracy and completeness of the New Zealand Cancer Registry for staging of invasive breast cancer. Cancer Epidemiol. 2014, 38, 638–644. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health. New Zealand Cancer Registry; Ministry of Health: Wellington, New Zealand, 2014.
- Ministry of Health. Mortality Collection Data Dictionary Version 1.7; Ministry of Health: Wellington, New Zealand, 2017.
- Gurney, J.; Sarfati, D.; Dennett, E.; Koea, J. The completeness of cancer treatment data on the National Health Collections. N. Z. Med. J. 2013, 126, 69–74. [Google Scholar] [PubMed]
- Neave, L.; Harvey, V.; Benjamin, C.; Thompson, P.; Pellett, O.; Whitlock, J.; Jones, W.; Poole, G. The Auckland breast cancer register: A special project of the Auckland breast cancer study group. N. Z. Med. J. 2003, 116, 1–12. [Google Scholar]
- Chen, K.; Liu, J.; Zhu, L.; Su, F.; Song, E.; Jacobs, L.K. Comparative effectiveness study of breast-conserving surgery and mastectomy in the general population: A NCDB analysis. Oncotarget 2015, 6, 40127–40140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Maaren, M.C.; de Munck, L.; de Bock, G.H.; Jobsen, J.J.; van Dalen, T.; Linn, S.C.; Poortmans, P.; Strobbe, L.J.A.; Siesling, S. 10 year survival after breast-conserving surgery plus radiotherapy compared with mastectomy in early breast cancer in the Netherlands: A population-based study. Lancet Oncol. 2016, 17, 1158–1170. [Google Scholar] [CrossRef]
- Exeter, D.J.; Shackleton, N.; Browne, M.; Zhao, J.; Lee, A.; Crengle, S. Different domains of deprivation and their relationship with obesity in New Zealand 4-year-old children. Pediatr. Obes. 2019, 14, e12520. [Google Scholar] [CrossRef]
- Lau, B.; Cole, S.R.; Gange, S.J. Competing risk regression models for epidemiologic data. Am. J. Epidemiol. 2009, 170, 244–256. [Google Scholar] [CrossRef]
- Donoghoe, M.W.; Gebski, V. The importance of censoring in competing risks analysis of the subdistribution hazard. BMC Med. Res. Methodol. 2017, 17, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lasry, J.-C.M.; Margolese, R.G.; Poisson, R.; Shibata, H.; Fleischer, D.; LaFleur, D.; Legault, S.; Taillefer, S. Depression and body image following mastectomy and lumpectomy. J. Chronic Dis. 1987, 40, 529–534. [Google Scholar] [CrossRef]
- Bigby, J.; Holmes, M.D. Disparities across the breast cancer continuum. Cancer Causes Control. 2005, 16, 35–44. [Google Scholar] [CrossRef]
- Ambroggi, M.; Biasini, C.; Del Giovane, C.; Fornari, F.; Cavanna, L. Distance as a Barrier to Cancer Diagnosis and Treatment: Review of the Literature. Oncologist 2015, 20, 1378–1385. [Google Scholar] [CrossRef] [Green Version]
- Goel, V.; Olivotto, I.; Hislop, T.G.; Sawka, C.; Coldman, A.; Holowaty, E.J. Patterns of initial management of node-negative breast cancer in two Canadian provinces. Can. Med Assoc. J. 1997, 156, 25–35. [Google Scholar]
- Gu, J.; Groot, G.; Boden, C.; Busch, A.; Holtslander, L.; Lim, H. Review of Factors Influencing Women’s Choice of Mastectomy Versus Breast Conserving Therapy in Early Stage Breast Cancer: A Systematic Review. Clin. Breast Cancer 2018, 18, e539–e554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samet, J.M.; Hunt, W.C.; Farrow, D.C. Determinants of receiving breast-conserving surgery. The surveillance, epidemiology, and end results program, 1983–1986. Cancer 1994, 73, 2344–2351. [Google Scholar] [CrossRef]
- Tin Tin, S.; Elwood, J.M.; Lawrenson, R.; Campbell, I.; Harvey, V.; Seneviratne, S. Differences in breast cancer survival between public and private care in New Zealand: Which factors contribute? PLoS ONE 2016, 11, e0153206. [Google Scholar] [CrossRef] [PubMed]
- Churilla, T.M.; Donnelly, P.E.; Leatherman, E.R.; Adonizio, C.S.; Peters, C.A. Total Mastectomy or Breast Conservation Therapy? How Radiation Oncologist Accessibility Determines Treatment Choice and Quality: A SEER Data-base Analysis. Breast J. 2015, 21, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Hartmann-Johnsen, O.J.; Kåresen, R.; Schlichting, E.; Nygård, J.F. Survival is better after breast conserving therapy than mastectomy for early stage breast cancer: A registry-based follow-up study of Norwegian women primary operated between 1998 and 2008. Ann. Surg. Oncol. 2015, 22, 3836–3845. [Google Scholar] [CrossRef] [Green Version]
- Hwang, E.S.; Lichtensztajn, D.Y.; Gomez, S.L.; Fowble, B.; Clarke, C.A. Survival after lumpectomy and mastectomy for early stage invasive breast cancer: The effect of age and hormone receptor status. Cancer 2013, 119, 1402–1411. [Google Scholar] [CrossRef] [Green Version]
- Hofvind, S.; Holen, A.; Aas, T.; Roman, M.; Sebuødegård, S.; Akslen, L.A. Women treated with breast conserving surgery do better than those with mastectomy independent of detection mode, prognostic and predictive tumor characteristics. Eur. J. Surg. Oncol. EJSO 2015, 41, 1417–1422. [Google Scholar] [CrossRef] [PubMed]
- Urruticoechea, A.; Smith, I.E.; Dowsett, M. Proliferation marker Ki-67 in early breast cancer. J. Clin. Oncol. 2005, 23, 7212–7220. [Google Scholar] [CrossRef] [PubMed]
- Connor, J.; Kydd, R.; MacLennan, B.; Shield, K.; Rehm, J. Alcohol-attributable cancer deaths under 80 years of age in New Zealand. Drug Alcohol. Rev. 2016, 36, 415–423. [Google Scholar] [CrossRef] [Green Version]
- Fang, S.-Y.; Shu, B.-C.; Chang, Y.-J. The effect of breast reconstruction surgery on body image among women after mastectomy: A meta-analysis. Breast Cancer Res. Treat. 2012, 137, 13–21. [Google Scholar] [CrossRef]
- Faermann, R.; Sperber, F.; Schneebaum, S.; Barsuk, D. Tumor-to-breast volume ratio as measured on MRI: A possible predictor of breast-conserving surgery versus mastectomy. Sat 2014, 30, 20. [Google Scholar]

| Covariates | Crude OR | Adjusted OR |
|---|---|---|
| DEMOGRAPHIC VARIABLES | ||
| Age | ||
| <45 | 1.00 | 1.00 |
| 45–59 | 1.59 (1.35–1.87) | 1.14 (0.96–1.36) |
| 60–74 | 1.52 (1.28–1.79) | 1.01 (0.84–1.22) |
| 75+ | 0.40 (0.33–0.50) | 0.34 (0.27–0.43) |
| Ethnicity | ||
| European | 1.00 | 1.00 |
| Maori | 0.91 (0.77–1.08) | 0.91 (0.75–1.10) |
| Pacific | 0.79 (0.60–1.03) | 0.94 (0.70–1.27) |
| Asian | 0.58 (0.49–0.69) | 0.58 (0.48–0.69) |
| Other | 1.12 (0.76–0.65) | 1.02 (0.68–1.53) |
| Unknown | 1.06 (0.78–1.44) | 1.02 (0.74–1.41) |
| NZ Deprivation | ||
| 1–2 | 1.00 | 1.00 |
| 3–4 | 1.09 (0.93–1.27) | 1.16 (0.99–1.37) |
| 5–6 | 0.99 (0.85–1.16) | 1.00 (0.85–1.18) |
| 7–8 | 1.06 (0.90–1.25) | 1.04 (0.87–1.25) |
| 9–10 | 0.80 (0.69–0.93) | 0.76 (0.64–0.91) |
| Unknown | 0.91 (0.68–1.22) | 1.10 (0.38–3.20) |
| Urban Rural | ||
| Urban | 1.00 | 1.00 |
| Rural | 1.28 (1.05–1.57) | 0.97 (0.78–1.20) |
| Unknown | 0.92 (0.70–1.21) | 0.94 (0.33–2.70) |
| Region | ||
| Auckland | 1.00 | 1.00 |
| Waikato | 1.46 (1.29–1.65) | 1.97 (1.70–2.29) |
| Public/Private Treatment | ||
| Private | 1.00 | 1.00 |
| Public | 0.76 (0.69–0.85) | 0.79 (0.70–0.89) |
| CLINICOPATHOLOGICAL VARIABLES | ||
| Year of Diagnosis | ||
| 2000–2004 | 1.00 | 1.00 |
| 2005–2009 | 1.26 (1.11–1.44) | 1.24 (1.08–1.42) |
| 2010–2015 | 1.21 (1.07–1.37) | 1.18 (1.03–1.35) |
| Screened/Symptomatic | ||
| Screened | 1.00 | 1.00 |
| Symptomatic | 0.47 (0.42–0.52) | 0.60 (0.54–0.68) |
| Grade | ||
| 1 | 1.00 | 1.00 |
| 2 | 0.71 (0.63–0.80) | 0.90 (0.78–1.02) |
| 3 | 0.65 (0.56–0.74) | 1.09 (0.91–1.31) |
| Unknown | 0.37 (0.21–0.63) | 0.45 (0.25–0.81) |
| Hormone Receptor Status | ||
| ER 5- and PR 6-positive | 1.00 | 1.00 |
| ER 5- and PR 6-negative | 1.49 (1.30–1.71) | 0.68 (0.57–0.81) |
| ER 5- or PR 6-positive | 1.03 (1.08–1.55) | 0.89 (0.76–1.03) |
| Unknown | 0.89 (0.62–1.28) | 0.53 (0.36–0.78) |
| Histology | ||
| Ductal | 1.00 | 1.00 |
| Lobular | 0.89 (0.75–1.07) | 0.89 (0.73–1.09) |
| Others | 1.06 (0.87–1.29) | 1.04 (0.84–1.29) |
| Tumour Size | ||
| <20 mm | 1.00 | 1.00 |
| ≥20–≤50 mm | 0.48 (0.43–0.54) | 0.63 (0.56–0.71) |
| Positive Lymph Node Status | ||
| 0 | 1.00 | 1.00 |
| 1–3 | 0.71 (0.62–0.80) | 0.83 (0.72–0.95) |
| 4+ | 0.47 (0.36–0.61) | 0.60 (0.44–0.80) |
| Lymphovascular Invasion | ||
| No | 1.00 | 1.00 |
| Yes | 0.79 (0.70–0.90) | 1.01 (0.87–1.17) |
| Factors | Total | BCS 1 | BCS + RT 2 | MTX 3 | MTX + RT 4 | ||||
|---|---|---|---|---|---|---|---|---|---|
| No. | Col% | No. | Col% | No. | Col% | No. | Col% | ||
| Total No. | 6972 | 588 | 100.0 | 4608 | 100.0 | 1507 | 100.0 | 269 | 100.0 |
| DEMOGRAPHIC VARIABLES | |||||||||
| Median Age | 58 (50–66) 5 | 58 (49–68) 5 | 58 (50–65) 5 | 61 (51–71) 5 | 53 (45–63) 5 | ||||
| Age Group | |||||||||
| <45 | 789 | 78 | 13.3 | 475 | 10.3 | 172 | 11.4 | 64 | 23.8 |
| 45–59 | 3006 | 236 | 40.1 | 2124 | 46.1 | 531 | 35.2 | 115 | 42.8 |
| 60–74 | 2538 | 184 | 31.3 | 1767 | 38.3 | 523 | 34.7 | 64 | 23.8 |
| 75+ | 639 | 90 | 15.3 | 242 | 5.3 | 281 | 18.6 | 26 | 9.7 |
| Ethnicity | |||||||||
| European | 5180 | 429 | 73.0 | 3495 | 75.8 | 1063 | 70.5 | 193 | 71.7 |
| Māori | 653 | 50 | 8.5 | 427 | 9.3 | 139 | 9.2 | 37 | 13.8 |
| Pacific | 229 | 29 | 4.9 | 142 | 3.1 | 53 | 3.5 | 5 | 1.9 |
| Other | 715 | 58 | 9.9 | 410 | 8.9 | 218 | 14.5 | 29 | 10.8 |
| Unknown | 195 | 22 | 3.7 | 134 | 2.9 | 34 | 2.3 | 5 | 1.9 |
| NZ Deprivation | |||||||||
| 1–2 | 1534 | 140 | 23.8 | 1021 | 22.2 | 307 | 20.4 | 66 | 24.5 |
| 3–4 | 1394 | 108 | 18.4 | 954 | 20.7 | 296 | 19.6 | 36 | 13.4 |
| 5–6 | 1415 | 118 | 20.1 | 940 | 20.4 | 298 | 19.8 | 59 | 21.9 |
| 7–8 | 1121 | 80 | 13.6 | 760 | 16.5 | 233 | 15.5 | 48 | 17.8 |
| 9–10 | 1289 | 117 | 19.9 | 792 | 17.2 | 326 | 21.6 | 54 | 20.1 |
| Unknown | 219 | 25 | 4.3 | 141 | 3.1 | 47 | 3.1 | 6 | 2.2 |
| Main Urban Areas | |||||||||
| Urban | 6252 | 515 | 87.6 | 4112 | 89.2 | 1377 | 91.4 | 248 | 92.2 |
| Rural | 496 | 46 | 7.8 | 353 | 7.7 | 81 | 5.4 | 16 | 5.9 |
| Unknown | 224 | 27 | 4.6 | 143 | 3.1 | 49 | 3.3 | 5 | 1.9 |
| Region | |||||||||
| Auckland | 5479 | 468 | 79.6 | 3526 | 76.5 | 1287 | 85.4 | 198 | 73.6 |
| Waikato | 1493 | 120 | 20.4 | 1082 | 23.5 | 220 | 14.6 | 71 | 26.4 |
| Public/Private | |||||||||
| Public | 2245 | 170 | 28.9 | 1574 | 34.2 | 416 | 27.6 | 85 | 31.6 |
| Private | 4727 | 418 | 71.1 | 3034 | 65.8 | 1091 | 72.4 | 184 | 68.4 |
| CLINICAL VARIABLES | |||||||||
| Year of Diagnosis | |||||||||
| 2000–2004 | 1861 | 143 | 24.3 | 1165 | 25.3 | 456 | 30.3 | 97 | 36.1 |
| 2005–2009 | 2240 | 148 | 25.2 | 1520 | 33.0 | 489 | 32.4 | 83 | 30.9 |
| 2010–2015 | 2871 | 297 | 50.5 | 1923 | 41.7 | 562 | 37.3 | 89 | 33.1 |
| Screen-Detected/Symptomatic | |||||||||
| Screen-Detected | 3605 | 283 | 48.1 | 2675 | 58.1 | 587 | 39.0 | 60 | 22.3 |
| Symptomatic | 3367 | 305 | 51.9 | 1933 | 41.9 | 920 | 61.0 | 209 | 77.7 |
| Stage | |||||||||
| IA | 4521 | 434 | 73.8 | 3192 | 69.3 | 854 | 56.7 | 41 | 15.2 |
| IB | 193 | 17 | 2.9 | 133 | 2.9 | 37 | 2.5 | 6 | 2.2 |
| IIA | 1587 | 104 | 17.7 | 963 | 20.9 | 452 | 30.0 | 68 | 25.3 |
| IIB | 446 | 27 | 4.6 | 208 | 4.5 | 149 | 9.9 | 62 | 23.0 |
| IIIA | 225 | 6 | 1.0 | 112 | 2.4 | 15 | 1.0 | 92 | 34.2 |
| Grade | |||||||||
| 1 | 2191 | 218 | 37.1 | 1572 | 34.1 | 373 | 24.8 | 28 | 10.4 |
| 2 | 3182 | 251 | 42.7 | 2050 | 44.5 | 756 | 50.2 | 125 | 46.5 |
| 3 | 1545 | 109 | 18.5 | 960 | 20.8 | 362 | 24.0 | 114 | 42.4 |
| Unknown | 54 | 10 | 1.7 | 26 | 0.6 | 16 | 1.1 | 2 | 0.7 |
| Hormone Receptor Status | |||||||||
| ER 6 and PR 7 negative | 1018 | 72 | 12.2 | 600 | 13.0 | 264 | 17.5 | 82 | 30.5 |
| ER 6 and PR 7 positive | 4801 | 413 | 70.2 | 3270 | 71.0 | 975 | 64.7 | 143 | 53.2 |
| ER 6 or PR 7 positive | 1016 | 90 | 15.3 | 661 | 14.3 | 227 | 15.1 | 38 | 14.1 |
| Unknown | 137 | 13 | 2.2 | 77 | 1.7 | 41 | 2.7 | 6 | 2.2 |
| Histology | |||||||||
| Ductal | 5909 | 472 | 80.3 | 3912 | 84.9 | 1286 | 85.3 | 239 | 88.8 |
| Lobular | 567 | 45 | 7.7 | 361 | 7.8 | 140 | 9.3 | 21 | 7.8 |
| Other | 496 | 71 | 12.1 | 335 | 7.3 | 81 | 5.4 | 9 | 3.3 |
| Tumour Size (mm) | |||||||||
| <20 | 4847 | 445 | 75.7 | 3452 | 74.9 | 859 | 57.0 | 91 | 33.8 |
| ≥20–≤50 | 2125 | 143 | 24.3 | 1156 | 25.1 | 648 | 43.0 | 178 | 66.2 |
| Positive Lymph Node | |||||||||
| 0 | 5453 | 498 | 84.7 | 3717 | 80.7 | 1169 | 77.6 | 69 | 25.7 |
| 1–3 | 1295 | 85 | 14.5 | 779 | 16.9 | 323 | 21.4 | 108 | 40.1 |
| 4+ | 224 | 5 | 0.9 | 112 | 2.4 | 15 | 1.0 | 92 | 34.2 |
| Lympho-vascular Invasion | |||||||||
| Yes | 5799 | 508 | 86.4 | 3885 | 84.3 | 1254 | 83.2 | 152 | 56.5 |
| No | 1173 | 80 | 13.6 | 723 | 15.7 | 253 | 16.8 | 117 | 43.5 |
| SYSTEMIC TREATMENT VARIABLES | |||||||||
| Systemic Treatment | |||||||||
| None | 2303 | 275 | 46.8 | 1464 | 31.8 | 545 | 36.2 | 19 | 7.1 |
| Both | 932 | 44 | 7.5 | 602 | 13.1 | 180 | 11.9 | 106 | 39.4 |
| Chemotherapy | 711 | 47 | 8.0 | 449 | 9.7 | 141 | 9.4 | 74 | 27.5 |
| Hormonal therapy | 2961 | 204 | 34.7 | 2064 | 44.8 | 624 | 41.4 | 69 | 25.7 |
| Unknown | 65 | 18 | 3.1 | 29 | 0.6 | 17 | 1.1 | 1 | 0.4 |
| Type of Loco-Regional Treatment | Crude HR (95% CI) | Adjusted HR (95% CI) 1 | Adjusted HR (95% CI) 2 | Adjusted HR (95% CI) 3 |
|---|---|---|---|---|
| BCS + RT 4 | 1.00 | 1.00 | 1.00 | 1.00 |
| BCS 5 | 1.16 (0.75–1.78) | 1.13 (0.73–1.76) | 1.21 (0.77–1.88) | 1.11 (0.71–1.75) |
| MTX 6 | 1.73 (1.35–2.22) | 1.78 (1.37–2.30) | 1.45 (1.10–1.90) | 1.38 1.05–1.82) |
| MTX + RT 7 | 2.87 (1.93–4.27) | 2.73 (1.82–4.09) | 1.02 (0.65–1.60) | 1.05 (0.66–1.67) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abrahimi, M.S.; Elwood, M.; Lawrenson, R.; Campbell, I.; Tin Tin, S. Associated Factors and Survival Outcomes for Breast Conserving Surgery versus Mastectomy among New Zealand Women with Early-Stage Breast Cancer. Int. J. Environ. Res. Public Health 2021, 18, 2738. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052738
Abrahimi MS, Elwood M, Lawrenson R, Campbell I, Tin Tin S. Associated Factors and Survival Outcomes for Breast Conserving Surgery versus Mastectomy among New Zealand Women with Early-Stage Breast Cancer. International Journal of Environmental Research and Public Health. 2021; 18(5):2738. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052738
Chicago/Turabian StyleAbrahimi, Mohammad Shoaib, Mark Elwood, Ross Lawrenson, Ian Campbell, and Sandar Tin Tin. 2021. "Associated Factors and Survival Outcomes for Breast Conserving Surgery versus Mastectomy among New Zealand Women with Early-Stage Breast Cancer" International Journal of Environmental Research and Public Health 18, no. 5: 2738. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18052738