
Nicotine Replacement Therapy during Pregnancy and Child Health Outcomes: A Systematic Review

 , ,
, ,  ,
,  and
and
Abstract
:1. Introduction
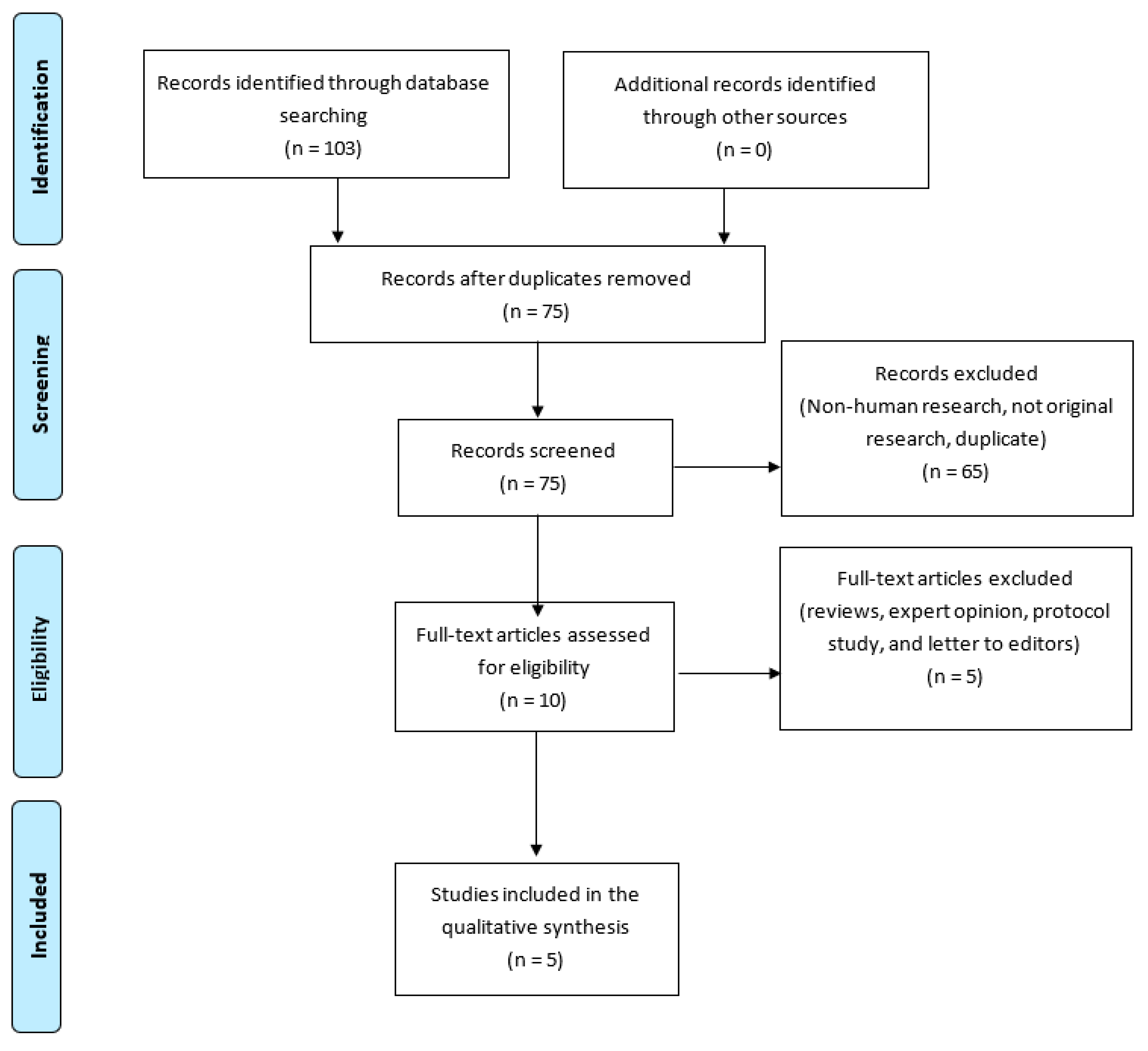
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria and Main Outcome Measures
2.3. Data Extraction
3. Results
3.1. Infantile Colic
3.2. Infant Impairment (Disability and/or Behavior and Development Problems)
3.3. Attention-Deficit/Hyperactivity Disorder (ADHD)
3.4. Major Congenital Anomalies
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Diguisto, C.; Dochez, V. Conséquences du tabagisme actif chez la femme enceinte—Rapport d’experts et recommandations CNGOF-SFT sur la prise en charge du tabagisme en cours de grossesse. Gynécologie Obs. Fertil. Sénologie 2020, 48, 559–566. [Google Scholar] [CrossRef]
- Lange, S.; Probst, C.; Rehm, J.; Popova, S. National, regional, and global prevalence of smoking during pregnancy in the general population: A systematic review and meta-analysis. Lancet Glob. Health 2018, 6, e769–e776. [Google Scholar] [CrossRef] [Green Version]
- Lumley, J.; Chamberlain, C.; Dowswell, T.; Oliver, S.; Oakley, L.; Watson, L. Interventions for promoting smoking cessation during pregnancy. Cochrane Database Syst. Rev. 2009, CD001055. [Google Scholar] [CrossRef]
- Perinatal Statistics-Parturients, Delivers and Newborns-THL. Finnish Institute for Health and Welfare (THL), Finland n.d. Available online: https://thl.fi/en/web/thlfi-en/statistics/statistics-by-topic/sexual-and-reproductive-health/parturients-deliveries-and-births/perinatal-statistics-parturients-delivers-and-newborns (accessed on 7 February 2021).
- Grangé, G.; Vayssiere, C.; Borgne, A.; Ouazana, A.; L’Huillier, J.-P.; Valensi, P.; Peiffer, G.; Aubin, H.-J.; Renon, D.; Thomas, D.; et al. Description of tobacco addiction in pregnant women. Eur. J. Obstet. Gynecol. Reprod. Biol. 2005, 120, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Kapaya, M.; Tong, V.; Ding, H. Nicotine replacement therapy and other interventions for pregnant smokers: Pregnancy Risk Assessment Monitoring System, 2009–2010. Prev. Med. 2015, 78, 92–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Havard, A.; Jorm, L.R.; Preen, D.; Daube, M.; Kemp, A.; Einarsdóttir, K.; Randall, D.; Tran, D.T. The Smoking MUMS (Maternal Use of Medications and Safety) Study: Protocol for a population-based cohort study using linked administrative data. BMJ Open 2013, 3, e003692. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartmann-Boyce, J.; Chepkin, S.C.; Ye, W.; Bullen, C.; Lancaster, T. Nicotine replacement therapy versus control for smoking cessation. Cochrane Database Syst. Rev. 2018, 5, CD000146. [Google Scholar] [CrossRef]
- Blanc, J.; Koch, A. Prise en charge médicamenteuse du tabagisme en cours de grossesse—Rapport d’experts et recommandations CNGOF-SFT sur la prise en charge du tabagisme en cours de grossesse. Gynécologie Obs. Fertil. Sénologie 2020, 48, 604–611. [Google Scholar] [CrossRef]
- Claire, R.; Chamberlain, C.; Davey, M.-A.; Cooper, S.E.; Berlin, I.; Leonardi-Bee, J.; Coleman, T. Pharmacological interventions for promoting smoking cessation during pregnancy. Cochrane Database Syst. Rev. 2020, 2020, CD010078. [Google Scholar] [CrossRef] [Green Version]
- Falk, L.; Nordberg, A.; Seiger, A.; Kjældgaard, A.; Hellström-Lindahl, E. Smoking during early pregnancy affects the expression pattern of both nicotinic and muscarinic acetylcholine receptors in human first trimester brainstem and cerebellum. Neurosci. 2005, 132, 389–397. [Google Scholar] [CrossRef] [Green Version]
- Hellström-Lindahl, E.; Seiger, Å.; Kjældgaard, A.; Nordberg, A. Nicotine-induced alterations in the expression of nicotinic receptors in primary cultures from human prenatal brain. Neuroscience 2001, 105, 527–534. [Google Scholar] [CrossRef]
- Janssen, R.; Oudijk, M.A. Concerns about the safety of nicotine replacement therapy during pregnancy on lung development in children. Am. J. Obstet. Gynecol. 2017, 216, 327–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Genedani, S.; Bernardi, M.; Bertolini, A. Sex-linked differences in avoidance learning in the offspring of rats treated with nicotine during pregnancy. Psychopharmacology 1983, 80, 93–95. [Google Scholar] [CrossRef]
- Levin, E.D.; Briggs, S.J.; Christopher, N.; Rose, J.E. Prenatal nicotine exposure and cognitive performance in rats. Neurotoxicol. Teratol. 1993, 15, 251–260. [Google Scholar] [CrossRef]
- Siu, A.L. Behavioral and Pharmacotherapy Interventions for Tobacco Smoking Cessation in Adults, Including Pregnant Women: U.S. Preventive Services Task Force Recommendation Statement. Ann. Intern. Med. 2015, 163, 622–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patnode, C.D.; Henderson, J.T.; Coppola, E.L.; Melnikow, J.; Durbin, S.; Thomas, R.G. Interventions for Tobacco Cessation in Adults, Including Pregnant Persons. JAMA 2021, 325, 280–298. [Google Scholar] [CrossRef]
- Force, U.P.S.T.; Krist, A.H.; Davidson, K.W.; Mangione, C.M.; Barry, M.J.; Cabana, M.; Caughey, A.B.; Donahue, K.; Doubeni, C.A.; Epling, J.W.; et al. Interventions for Tobacco Smoking Cessation in Adults, Including Pregnant Persons. JAMA 2021, 325, 265–279. [Google Scholar] [CrossRef]
- Coleman, T.; Britton, J.; Thornton, J. Nicotine replacement therapy in pregnancy. BMJ 2004, 328, 965–966. [Google Scholar] [CrossRef]
- Smoking and Pregnancy. Royal College of Obstetricians & Gynaecologists n.d. Available online: https://www.rcog.org.uk/en/patients/patient-leaflets/smoking-and-pregnancy/ (accessed on 9 January 2021).
- American College of Obstetricians and Gynecologists. Tobacco and Nicotine Cessation during Pregnancy; ACOG Committee Opinion No 807; American College of Obstetricians and Gynecologists: Washington, DC, USA, 2020; Volume 135, pp. e221–e299. [Google Scholar]
- Grangé, G.; Berlin, I.; Bretelle, F.; Bertholdt, C.; Berveiller, P.; Blanc, J.; Diguisto, C.; Dochez, V.; Garabedian, C.; Guerby, P.; et al. Rapport d’experts et recommandations CNGOF-SFT sur la prise en charge du tabagisme en cours de grossesse—Texte court. Gynécologie Obs. Fertil. Sénologie 2020, 48, 539–545. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. For the PRISMA Group Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Milidou, I.; Henriksen, T.B.; Jensen, M.S.; Olsen, J.; Søndergaard, C. Nicotine Replacement Therapy During Pregnancy and Infantile Colic in the Offspring. Pediatrics 2012, 129, e652–e658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, S.; Taggar, J.; Lewis, S.; Marlow, N.; Dickinson, A.; Whitemore, R.; Coleman, T. Effect of nicotine patches in pregnancy on infant and maternal outcomes at 2 years: Follow-up from the randomised, double-blind, placebo-controlled SNAP trial. Lancet Respir. Med. 2014, 2, 728–737. [Google Scholar] [CrossRef]
- Iyen, B.; Vaz, L.R.; Taggar, J.; Cooper, S.; Lewis, S.; Coleman, T. Is the apparently protective effect of maternal nicotine replacement therapy (NRT) used in pregnancy on infant development explained by smoking cessation?: Secondary analyses of a randomised controlled trial. BMJ Open 2019, 9, e024923. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhalwani, N.N.; Szatkowski, L.; Coleman, T.; Fiaschi, L.; Tata, L.J. Nicotine Replacement Therapy in Pregnancy and Major Congenital Anomalies in Offspring. Pediatrics 2015, 135, 859–867. [Google Scholar] [CrossRef] [Green Version]
- Zhu, J.L.; Olsen, J.; Liew, Z.; Li, J.; Niclasen, J.; Obel, C. Parental Smoking During Pregnancy and ADHD in Children: The Danish National Birth Cohort. Pediatrics 2014, 134, e382–e388. [Google Scholar] [CrossRef] [Green Version]
- Coleman, T.; Cooper, S.; Thornton, J.G.; Grainge, M.J.; Watts, K.; Britton, J.; Lewis, S. A Randomized Trial of Nicotine-Replacement Therapy Patches in Pregnancy. N. Engl. J. Med. 2012, 366, 808–818. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cooper, S.; Lewis, S.; Thornton, J.G.; Marlow, N.; Watts, K.; Britton, J.; Grainge, M.J.; Taggar, J.; Essex, H.; Parrott, S.; et al. The SNAP trial: A randomised placebo-controlled trial of nicotine replacement therapy in pregnancy—Clinical effectiveness and safety until 2 years after delivery, with economic evaluation. Health Technol. Assess. 2014, 18, 1–128. [Google Scholar] [CrossRef] [Green Version]
- Abbott, L.C.; Winzer-Serhan, U.H. Smoking during pregnancy: Lessons learned from epidemiological studies and experimental studies using animal models. Crit. Rev. Toxicol. 2012, 42, 279–303. [Google Scholar] [CrossRef]
- Cohen, G.; Roux, J.-C.; Grailhe, R.; Malcolm, G.; Changeux, J.-P.; Lagercrantz, H. From The Cover: Perinatal exposure to nicotine causes deficits associated with a loss of nicotinic receptor function. Proc. Natl. Acad. Sci. USA 2005, 102, 3817–3821. [Google Scholar] [CrossRef] [Green Version]
- Slotkin, T.; Lappi, S.; McCook, E.; Lorber, B.; Seidler, F. Loss of neonatal hypoxia tolerance after prenatal nicotine exposure: Implications for sudden infant death syndrome. Brain Res. Bull. 1995, 38, 69–75. [Google Scholar] [CrossRef]
- Luck, W.; Nau, H.; Hansen, R.; Steldinger, R. Extent of Nicotine and Cotinine Transfer to the Human Fetus, Placenta and Amniotic Fluid of Smoking Mothers. Dev. Pharmacol. Ther. 1985, 8, 384–395. [Google Scholar] [CrossRef]
- Pastrakuljic, A.; Schwartz, R.; Simone, C.; Derewlany, L.O.; Knie, B.; Koren, G. Transplacental transfer and biotransformation studies of nicotine in the human placental cotyledon perfused in vitro. Life Sci. 1998, 63, 2333–2342. [Google Scholar] [CrossRef]
- Jacob, N.; Golmard, J.-L.; Berlin, I. Fetal exposure to tobacco: Nicotine and cotinine concentration in amniotic fluid and maternal saliva. J. Matern. Neonatal Med. 2016, 30, 233–239. [Google Scholar] [CrossRef]
- Berveiller, P.; Rault, E.; Guerby, P. Données physiologiques et psychologiques influençant le comportement tabagique de la femme enceinte—Rapport d’experts et recommandations CNGOF-SFT sur la prise en charge du tabagisme en cours de grossesse. Gynécologie Obs. Fertil. Sénologie 2020, 48, 551–558. [Google Scholar] [CrossRef]
- E De Long, N.; Barra, N.G.; Hardy, D.B.; Holloway, A.C. Is it safe to use smoking cessation therapeutics during pregnancy? Expert Opin. Drug Saf. 2014, 13, 1721–1731. [Google Scholar] [CrossRef]
- Petre, M.A.; Petrik, J.; Ellis, R.; Inman, M.D.; Holloway, A.C.; Labiris, N.R. Fetal and Neonatal Exposure to Nicotine Disrupts Postnatal Lung Development in Rats: Role of VEGF and Its Receptors. Int. J. Toxicol. 2011, 30, 244–252. [Google Scholar] [CrossRef] [Green Version]
- Sekhon, H.; Proskocil, B.; Clark, J.; Spindel, E. Prenatal nicotine exposure increases connective tissue expression in foetal monkey pulmonary vessels. Eur. Respir. J. 2004, 23, 906–915. [Google Scholar] [CrossRef] [PubMed]
- Brose, L.S.; McEwen, A.; West, R. Association between nicotine replacement therapy use in pregnancy and smoking cessation. Drug Alcohol Depend. 2013, 132, 660–664. [Google Scholar] [CrossRef] [PubMed]
- Flamant, C.; Branger, B.; Tich, S.N.T.; De La Rochebrochard, E.; Savagner, C.; Berlie, I.; Rozé, J.-C. Parent-Completed Developmental Screening in Premature Children: A Valid Tool for Follow-Up Programs. PLoS ONE 2011, 6, e20004. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors | Year of Publication | Country | Type | Sample Size | Period of Inclusion | Main Outcomes | Secondary Outcomes |
|---|---|---|---|---|---|---|---|
| Milidou et al. [24] | 2012 | Denmark | Population-based cohort study | 63,128 mother-infant dyads | 1996–2002 | Infantile colic 1 | - |
| Cooper et al. [25] | 2014 | The Midlands and North-West England | Multicenter RCT “SNAP Trial” | 888 infants | 1 May 2007 to 1 February 2010 | Survival without developmental impairment 2 | Infant respirator symptoms, smoking outcomes |
| Zhu et al. [28] | 2014 | Denmark | Population-based cohort study linked to national registers | 84,803 children | 1996–2002 (pregnancy) and 7-year follow-up | Attention-deficit/Hyperactivity disorder 3 | - |
| Dhalwani et al. [27] | 2015 | United Kingdom | Retrospective cohort from prospectively collected data (The Health Improvement Network) with linked mother-child primary care records | 192,498 live-born children and 5535 children with at least 1 Major congenital anomalies | January 2001 to December 2012 | Major congenital anomalies 4 | - |
| Iyen et al. [26] | 2019 | The Midlands and North-West England | Secondary analysis of a Multicenter RCT “SNAP Trial” 5 | 884 infants | 1 May 2007 to 1 February 2010 | Infant development | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blanc, J.; Tosello, B.; Ekblad, M.O.; Berlin, I.; Netter, A. Nicotine Replacement Therapy during Pregnancy and Child Health Outcomes: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 4004. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084004
Blanc J, Tosello B, Ekblad MO, Berlin I, Netter A. Nicotine Replacement Therapy during Pregnancy and Child Health Outcomes: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(8):4004. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084004
Chicago/Turabian StyleBlanc, Julie, Barthélémy Tosello, Mikael O. Ekblad, Ivan Berlin, and Antoine Netter. 2021. "Nicotine Replacement Therapy during Pregnancy and Child Health Outcomes: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 8: 4004. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18084004