
Inequalities in the Global Burden of Chronic Kidney Disease Due to Type 2 Diabetes Mellitus: An Analysis of Trends from 1990 to 2019



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Socioeconomic Status
2.3. Gini Coefficient
2.4. Statistical Analysis
3. Results
3.1. Trends in Global Burden of CKD over Time
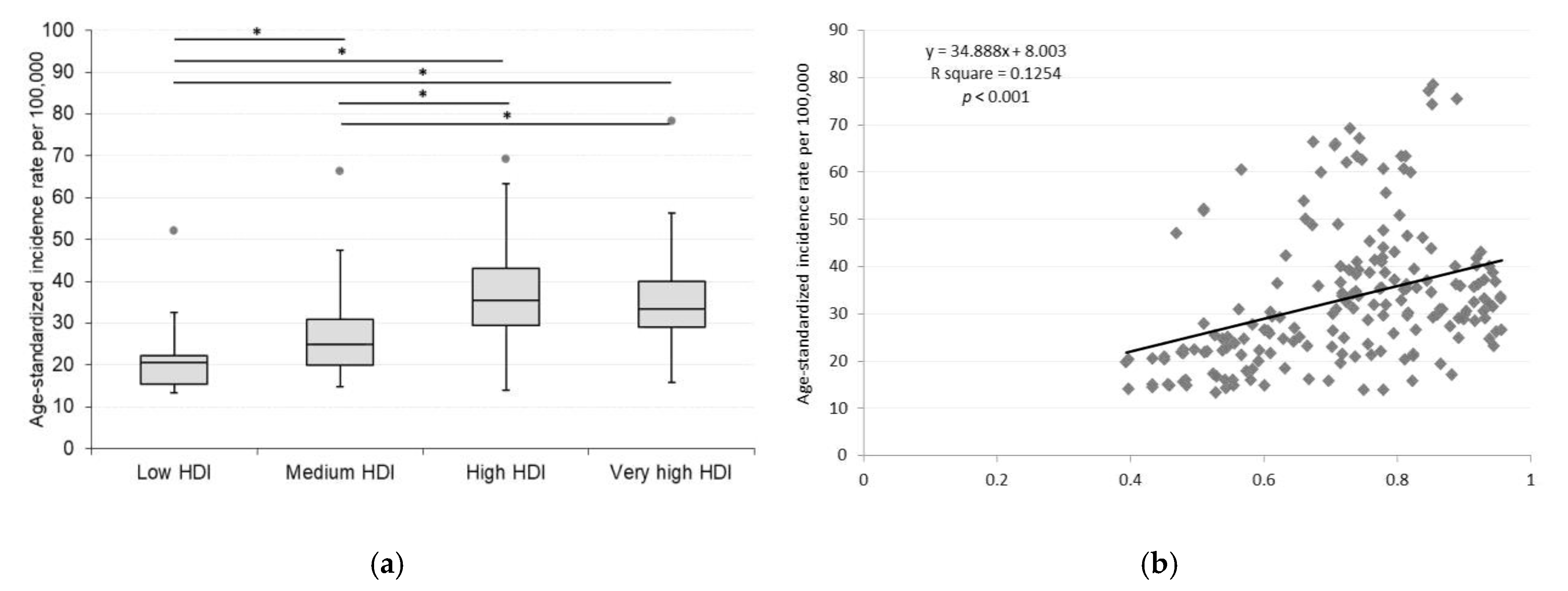
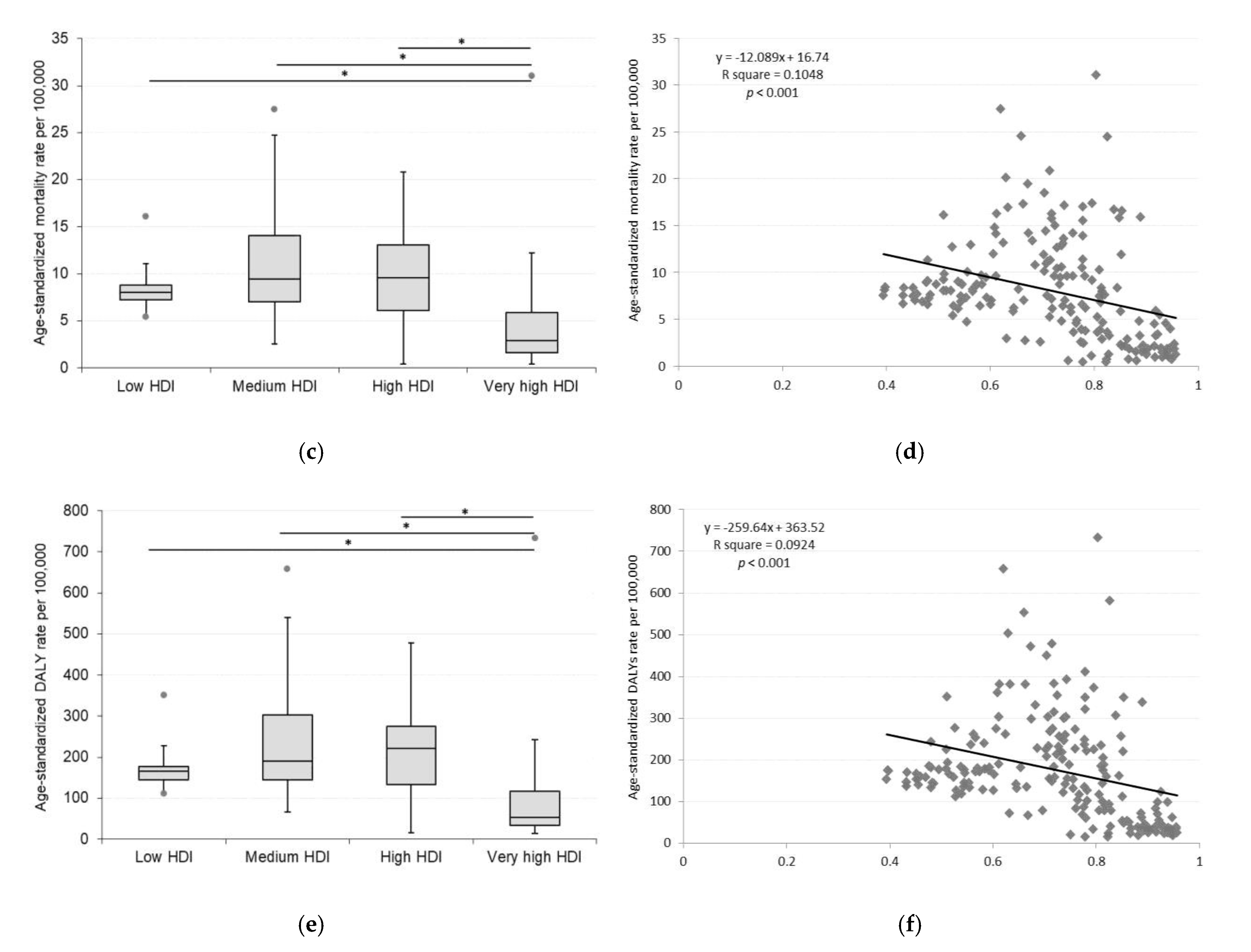
3.2. Current Disease Burden of CKD According to HDI
3.3. Trends in CKD Incidence, Mortality, and DALYs Rates Across HDI Groups Over Time
3.4. Global Health Inequality Related to CKD
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- International Diabetes Federation IDF Diabetes Atlas, 9th ed.; International Diabetes Federation: Brussels, Belgium, 2019.
- Zhang, X.-X.; Kong, J.; Yun, K. Prevalence of Diabetic Nephropathy among Patients with Type 2 Diabetes Mellitus in China: A Meta-Analysis of Observational Studies. J. Diabetes Res. 2020, 2020, e2315607. [Google Scholar] [CrossRef] [Green Version]
- Ritz, E.; Rychlík, I.; Locatelli, F.; Halimi, S. End-Stage Renal Failure in Type 2 Diabetes: A Medical Catastrophe of Worldwide Dimensions. Am. J. Kidney Dis. 1999, 34, 795–808. [Google Scholar] [CrossRef]
- Wu, A.Y.T.; Kong, N.C.T.; de Leon, F.A.; Pan, C.Y.; Tai, T.Y.; Yeung, V.T.F.; Yoo, S.J.; Rouillon, A.; Weir, M.R. An Alarmingly High Prevalence of Diabetic Nephropathy in Asian Type 2 Diabetic Patients: The MicroAlbuminuria Prevalence (MAP) Study. Diabetologia 2005, 48, 17–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bommer, J. Prevalence and Socio-Economic Aspects of Chronic Kidney Disease. Nephrol Dial Transpl. 2002, 17 (Suppl. 11), 8–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanifer, J.W.; Muiru, A.; Jafar, T.H.; Patel, U.D. Chronic Kidney Disease in Low- and Middle-Income Countries. Nephrol. Dial. Transplant. 2016, 31, 868–874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ameh, O.I.; Ekrikpo, U.E.; Kengne, A.-P. Preventing CKD in Low- and Middle-Income Countries: A Call for Urgent Action. Kidney Int. Rep. 2020, 5, 255–262. [Google Scholar] [CrossRef] [Green Version]
- Nahas, A.M.E.; Bello, A.K. Chronic Kidney Disease: The Global Challenge. Lancet 2005, 365, 331–340. [Google Scholar] [CrossRef]
- McCall, D.T.; Sauaia, A.; Hamman, R.F.; Reusch, J.E.; Barton, P. Are Low-Income Elderly Patients at Risk for Poor Diabetes Care? Diabetes Care 2004, 27, 1060–1065. [Google Scholar] [CrossRef] [Green Version]
- Association, A.D. Standards of Medical Care in Diabetes—2017: Summary of Revisions. Diabetes Care 2017, 40, S4–S5. [Google Scholar] [CrossRef] [Green Version]
- Tatulashvili, S.; Fagherazzi, G.; Dow, C.; Cohen, R.; Fosse, S.; Bihan, H. Socioeconomic Inequalities and Type 2 Diabetes Complications: A Systematic Review. Diabetes Metab. 2020, 46, 89–99. [Google Scholar] [CrossRef]
- Global Burden of Disease Collaborative Network: Institute for Health Metrics and Evaluation (IHME) Global Health Data Exchange. Global Burden of Disease Study 2019 (GBD 2019) Results; Institute for Health Metrics and Evaluation: Seattle, WA, USA, 2019. [Google Scholar]
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; et al. Global Burden of 369 Diseases and Injuries in 204 Countries and Territories, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Murray, C.J.L.; Aravkin, A.Y.; Zheng, P.; Abbafati, C.; Abbas, K.M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abdelalim, A.; Abdollahi, M.; Abdollahpour, I.; et al. Global Burden of 87 Risk Factors in 204 Countries and Territories, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef]
- World Health Organization. Department of Data and Analytics Division of Data, Analytics and Delivery for Impact WHO Methods and Data Sources for Global Burden of Disease Estimates2000–2019; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- UNDP. Human Development Report 2019: Beyond Income, beyond Averages, beyond Today: Inequalities in Human Development in the 21st Century; United Nations Development Programme: New York, NY, USA, 2019; ISBN 978-92-1-126439-5. [Google Scholar]
- Bleichrodt, H.; van Doorslaer, E. A Welfare Economics Foundation for Health Inequality Measurement. J. Health Econ. 2006, 25, 945–957. [Google Scholar] [CrossRef] [Green Version]
- Pan American Health Organization Measuring Health Inequalities: Gini Coefficient and Concentration Index. Epidemiol. Bull. 2001, 22, 3–4.
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation Tests for Joinpoint Regression with Applications to Cancer Rates. Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- National Cancer Institute. Surveillance Epidemiology and End Results (SEER) Program. Methods & Tools: Joinpoint Trend Analysis; National Cancer Institute: Bethesda, MD, USA, 2020. [Google Scholar]
- Peng, C.; Xu, X.; Chen, W.; Li, X.; Yi, X.; Ding, Y.; Yu, N.; Lu, J. Epidemiological Variations in the Global Burden of Psoriasis, an Analysis With Trends From 1990 to 2017. Front Med. 2021, 8, 585634. [Google Scholar] [CrossRef]
- Wang, D.; Jiang, Y.; He, M.; Scheetz, J.; Wang, W. Disparities in the Global Burden of Age-Related Macular Degeneration: An Analysis of Trends from 1990 to 2015. Curr. Eye Res. 2019, 44, 657–663. [Google Scholar] [CrossRef]
- Hu, K.; Ding, P.; Wu, Y.; Tian, W.; Pan, T.; Zhang, S. Global Patterns and Trends in the Breast Cancer Incidence and Mortality According to Sociodemographic Indices: An Observational Study Based on the Global Burden of Diseases. BMJ Open 2019, 9, e028461. [Google Scholar] [CrossRef]
- Misra, A.; Gopalan, H.; Jayawardena, R.; Hills, A.P.; Soares, M.; Reza-Albarrán, A.A.; Ramaiya, K.L. Diabetes in Developing Countries. J. Diabetes 2019, 11, 522–539. [Google Scholar] [CrossRef]
- van Dam, R.M. The Epidemiology of Lifestyle and Risk for Type 2 Diabetes. Eur. J. Epidemiol. 2003, 18, 1115–1125. [Google Scholar] [CrossRef]
- Beran, D.; Yudkin, J.S.; Courten, M. de Access to Care for Patients With Insulin-Requiring Diabetes in Developing Countries: Case Studies of Mozambique and Zambia. Diabetes Care 2005, 28, 2136–2140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolf, G.; Busch, M.; Müller, N.; Müller, U.A. Association between Socioeconomic Status and Renal Function in a Population of German Patients with Diabetic Nephropathy Treated at a Tertiary Centre. Nephrol. Dial. Transpl. 2011, 26, 4017–4023. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byrne, C.; Nedelman, J.; Luke, R.G. Race, Socioeconomic Status, and the Development of End-Stage Renal Disease. Am. J. Kidney Dis. 1994, 23, 16–22. [Google Scholar] [CrossRef]
- Young, E.W.; Mauger, E.A.; Jiang, K.H.; Port, F.K.; Wolfe, R.A. Socioeconomic Status and End-Stage Renal Disease in the United States. Kidney Int. 1994, 45, 907–911. [Google Scholar] [CrossRef] [Green Version]
- Bello, A.K.; Peters, J.; Rigby, J.; Rahman, A.A.; El Nahas, M. Socioeconomic Status and Chronic Kidney Disease at Presentation to a Renal Service in the United Kingdom. Clin. J. Am. Soc. Nephrol. 2008, 3, 1316–1323. [Google Scholar] [CrossRef]
- Drey, N.; Roderick, P.; Mullee, M.; Rogerson, M. A Population-Based Study of the Incidence and Outcomes of Diagnosed Chronic Kidney Disease. Am. J. Kidney Dis. 2003, 42, 677–684. [Google Scholar] [CrossRef]
- Fored, C.M.; Ejerblad, E.; Fryzek, J.P.; Lambe, M.; Lindblad, P.; Nyrén, O.; Elinder, C.-G. Socio-Economic Status and Chronic Renal Failure: A Population-Based Case-Control Study in Sweden. Nephrol. Dial. Transpl. 2003, 18, 82–88. [Google Scholar] [CrossRef] [Green Version]
- Shoham, D.A.; Vupputuri, S.; Kshirsagar, A.V. Chronic Kidney Disease and Life Course Socioeconomic Status: A Review. Adv. Chronic Kidney Dis. 2005, 12, 56–63. [Google Scholar] [CrossRef]
- Wardle, J.; Steptoe, A. Socioeconomic Differences in Attitudes and Beliefs about Healthy Lifestyles. J. Epidemiol. Community Health 2003, 57, 440–443. [Google Scholar] [CrossRef] [Green Version]
- van Dieren, S.; Beulens, J.W.J.; van der Schouw, Y.T.; Grobbee, D.E.; Neal, B. The Global Burden of Diabetes and Its Complications: An Emerging Pandemic. Eur J. Cardiovasc Prev Rehabil 2010, 17 (Suppl. 1), S3–S8. [Google Scholar] [CrossRef]
- Lajoie, J. Understanding the Measurement of Global Burden of Disease; National Collaborating Centre for Infectious Diseases: Winnipeg, MB, Canada, 2015; ISBN 978-1-927988-10-7. [Google Scholar]
- Trivedi, H.S.; Pang, M.M.H.; Campbell, A.; Saab, P. Slowing the Progression of Chronic Renal Failure: Economic Benefits and Patients’ Perspectives. Am. J. Kidney Dis. 2002, 39, 721–729. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| INCIDENCE | Trend 1 | Trend 2 | Trend 3 | Trend 4 | 1990–2019 | ||||
| Period | APC (%) | Period | APC (%) | Period | APC (%) | Period | APC (%) | AAPC (%) | |
| Low HDI | 1990–1999 | 0.5 * | 1999–2007 | 1.5 * | 2007–2015 | 1.0 * | 2015–2019 | 1.9 * | 1.1 * |
| Middle HDI | 1990–2002 | 1.3 * | 2002–2014 | 1.4 * | 2014–2017 | 1.7 * | 2017–2019 | 1.4 * | 1.4 * |
| High HDI | 1990–1995 | 2.2 * | 1995–2004 | 1.8 * | 2004–2013 | 1.3 * | 2013–2019 | 1.1 * | 1.5 * |
| Very high HDI | 1990–1993 | 1.5 * | 1993–1999 | 1.3 * | 1999–2004 | 1.1 * | 2004–2019 | 0.6 * | 0.9 * |
| MORTALITY | Trend 1 | Trend 2 | Trend 3 | Trend 4 | 1990–2019 | ||||
| Period | APC (%) | Period | APC (%) | Period | APC (%) | Period | APC (%) | AAPC (%) | |
| Low HDI | 1990–1995 | −0.1 | 1995–1999 | −0.4 * | 1999–2003 | 0.0 | 2003–2019 | −0.1 * | −0.1 * |
| Middle HDI | 1990–2004 | 1.7 * | 2004–2010 | 0.2 * | 2010–2014 | 0.6 * | 2014–2019 | −0.2 * | 0.9 * |
| High HDI | 1990–1994 | 0.9 * | 1994–2002 | 1.6 * | 2002–2016 | 0.5 * | 2016–2019 | −0.4 | 0.8 * |
| Very high HDI | 1990–1995 | 0.5 | 1995–2006 | 1.5 * | 2006–2010 | 0.0 | 2010–2019 | −0.8 * | 0.4 * |
| DALYs | Trend 1 | Trend 2 | Trend 3 | Trend 4 | 1990–2019 | ||||
| Period | APC (%) | Period | APC (%) | Period | APC (%) | Period | APC (%) | AAPC (%) | |
| Low HDI | 1990–1995 | −0.1 | 1995–2000 | −0.5 * | 2000–2003 | 0.1 | 2003–2019 | −0.1 * | −0.2 * |
| Middle HDI | 1990–2004 | 1.5 * | 2004–2010 | 0.1 | 2010–2015 | 0.5 * | 2015–2019 | −0.5 * | 0.7 * |
| High HDI | 1990–1992 | 0.8 | 1992–2002 | 1.4 * | 2002–2016 | 0.4 * | 2016–2019 | −0.2 | 0.7 * |
| Very high HDI | 1990–1994 | 0.4 | 1994–2006 | 1.2 * | 2006–2009 | 0.0 | 2009–2019 | −0.8 * | 0.3 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kovács, N.; Nagy, A.; Dombrádi, V.; Bíró, K. Inequalities in the Global Burden of Chronic Kidney Disease Due to Type 2 Diabetes Mellitus: An Analysis of Trends from 1990 to 2019. Int. J. Environ. Res. Public Health 2021, 18, 4723. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094723
Kovács N, Nagy A, Dombrádi V, Bíró K. Inequalities in the Global Burden of Chronic Kidney Disease Due to Type 2 Diabetes Mellitus: An Analysis of Trends from 1990 to 2019. International Journal of Environmental Research and Public Health. 2021; 18(9):4723. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094723
Chicago/Turabian StyleKovács, Nóra, Attila Nagy, Viktor Dombrádi, and Klára Bíró. 2021. "Inequalities in the Global Burden of Chronic Kidney Disease Due to Type 2 Diabetes Mellitus: An Analysis of Trends from 1990 to 2019" International Journal of Environmental Research and Public Health 18, no. 9: 4723. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094723