
Illicit Drug Use and Associated Problems in the Nightlife Scene: A Potential Setting for Prevention

 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Statistical Analysis
2.3. Dropout Analysis
3. Results
3.1. The Study Population: Demographics and Attendance at Nightlife Events
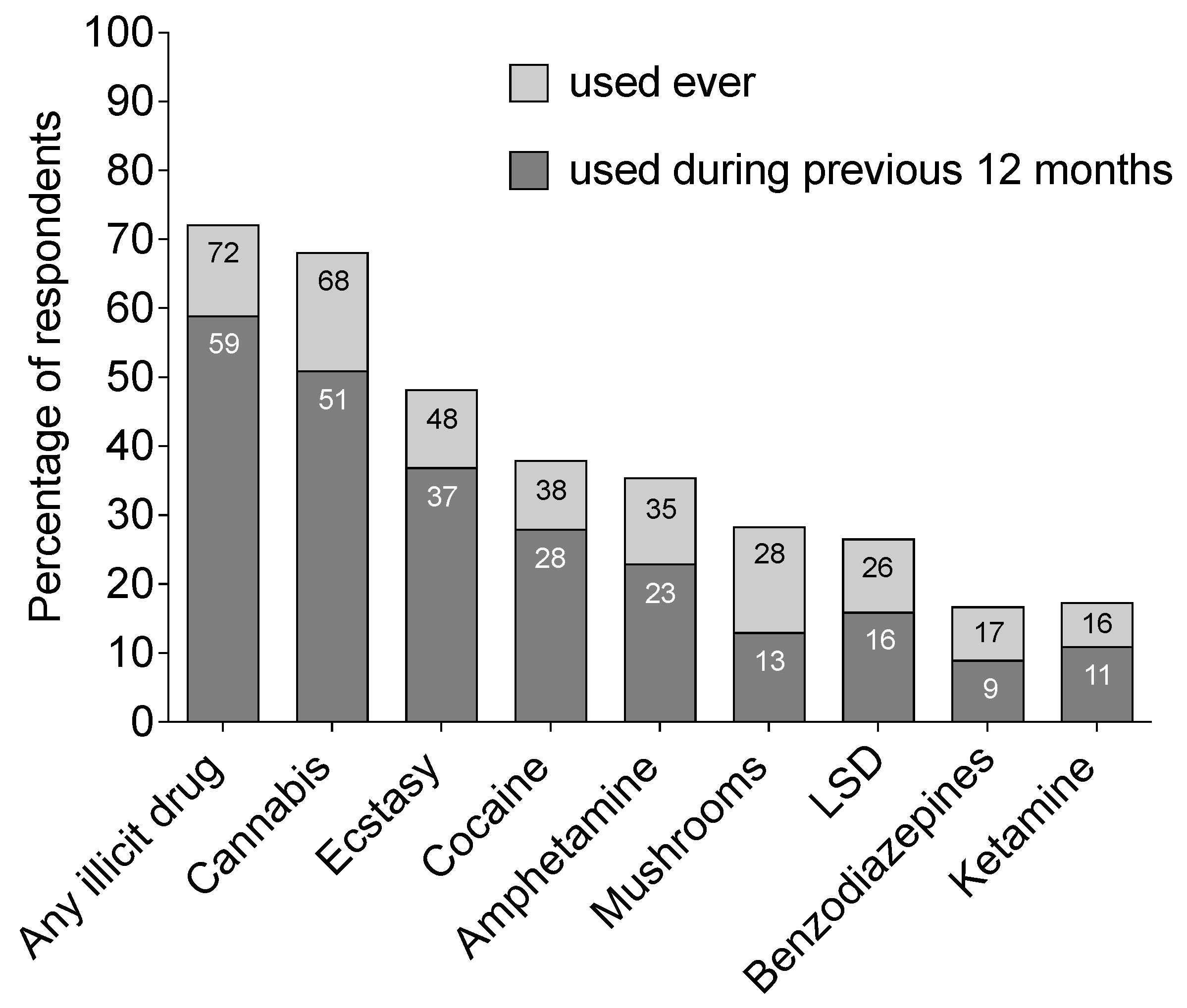
3.2. Prevalence of Drug Use
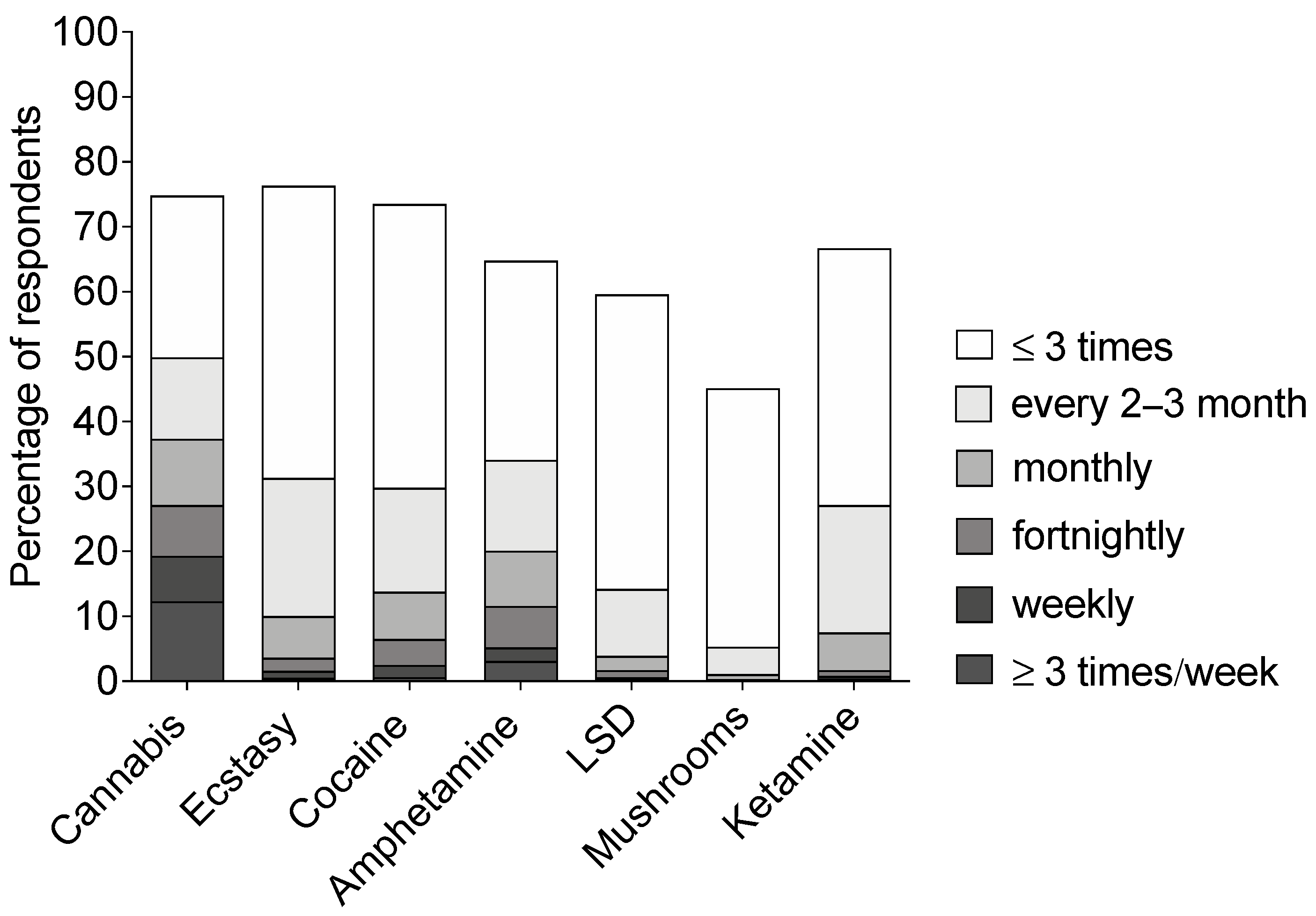
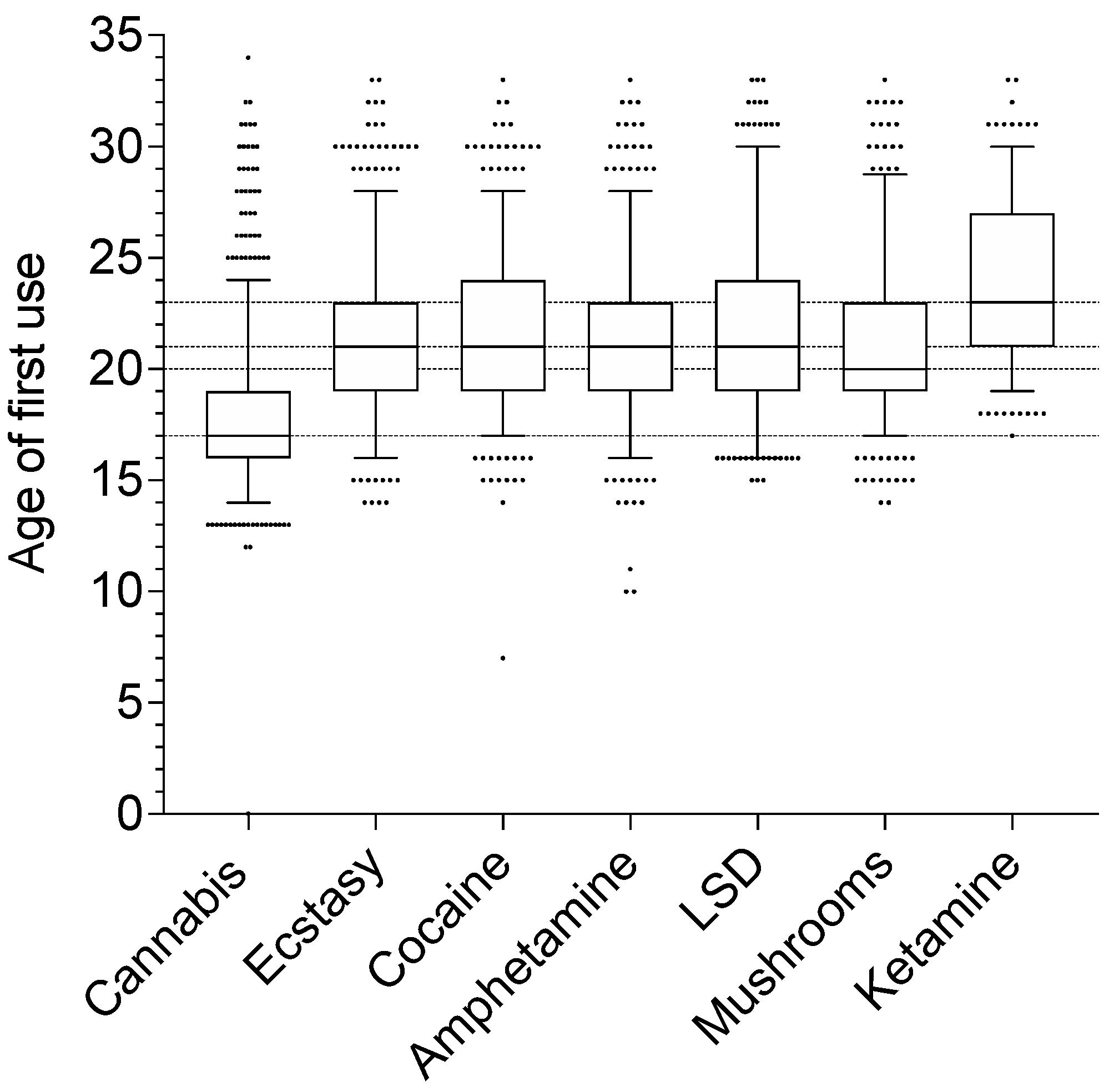
3.3. Setting and Frequency of Drug Use
3.4. Factors Associated with Illicit Drug Use
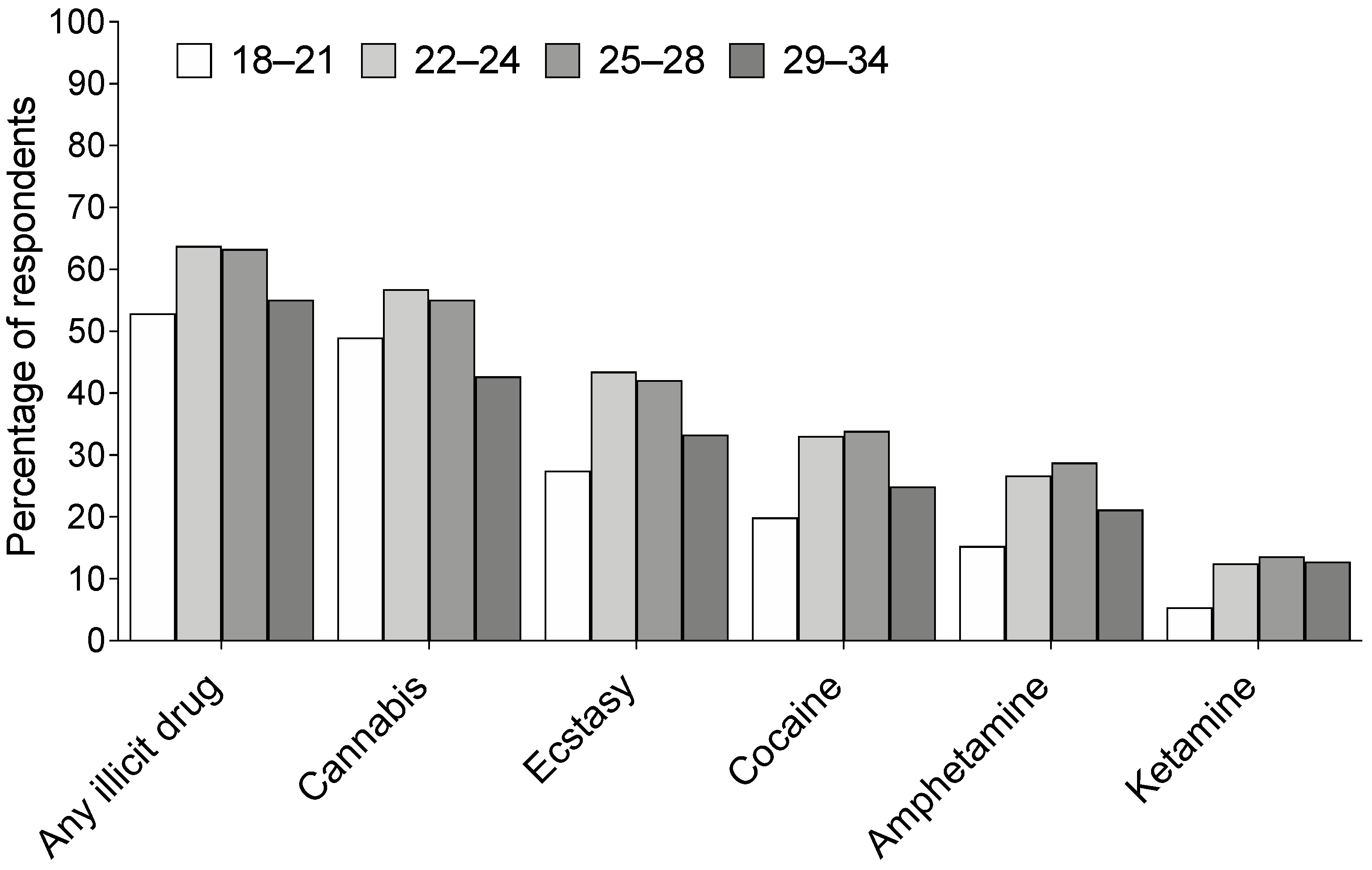
3.4.1. Age and Gender
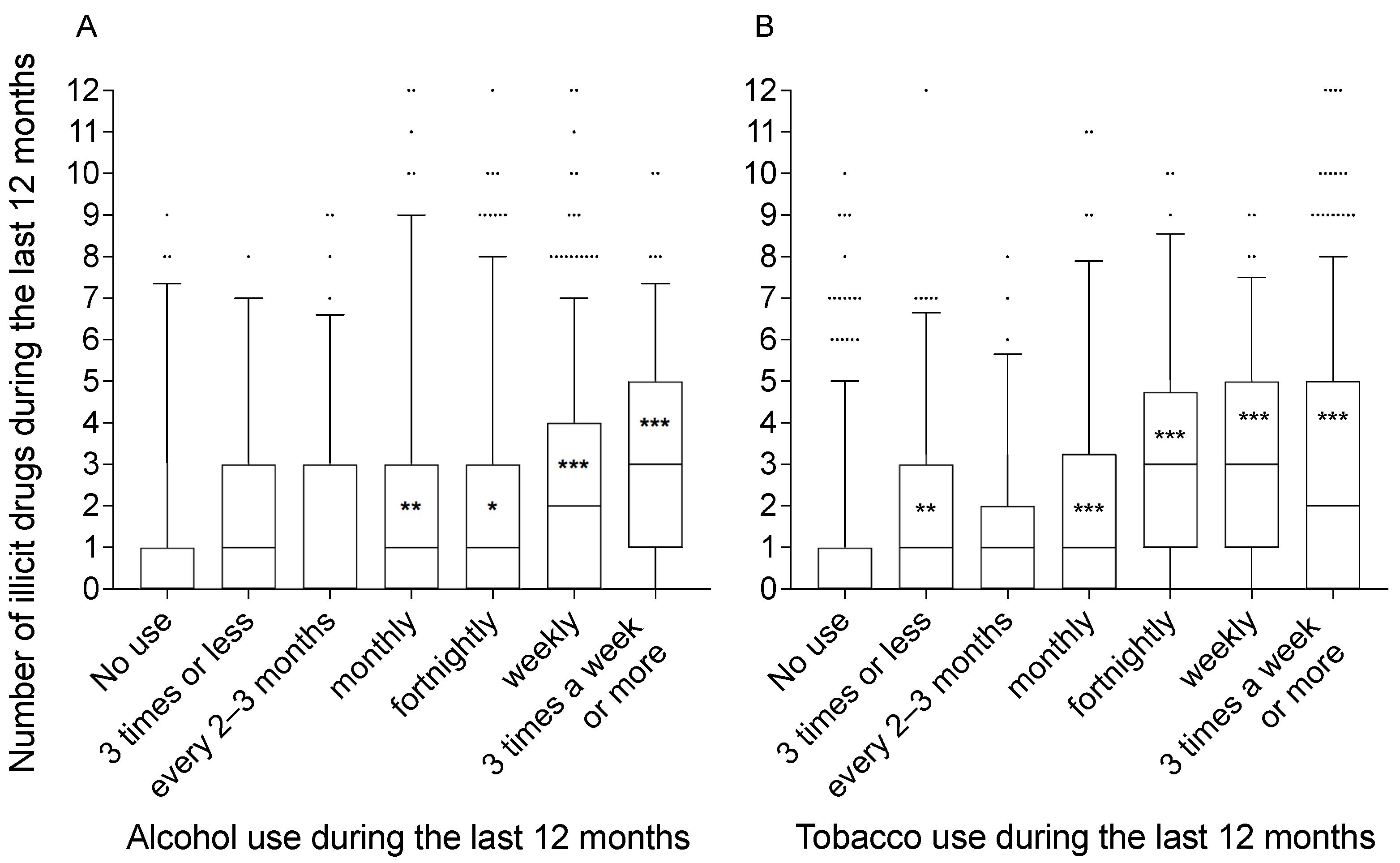
3.4.2. Frequency of Use of Alcohol and Tobacco
3.4.3. Factors Associated with Illicit Drug Use
3.5. Consequences of Drug Use
3.6. The Drug Use Disorder Identification Test (DUDIT)
4. Discussion
4.1. Prevalence of Illicit Drug Use and Settings Where Drugs Are Used
4.2. Factors Associated with Drug Use
4.3. Consequences
4.4. Implications for Prevention
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Degenhardt, L.; Hall, W. Extent of illicit drug use and dependence, and their contribution to the global burden of disease. Lancet 2012, 379, 55–70. [Google Scholar] [CrossRef]
- Connell, C.M.; Gilreath, T.D.; Hansen, N.B. A multiprocess latent class analysis of the co-occurrence of substance use and sexual risk behavior among adolescents. J. Stud. Alcohol Drugs 2009, 70, 943–951. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morley, K.I.; Lynskey, M.T.; Moran, P.; Borschmann, R.; Winstock, A.R. Polysubstance use, mental health and high-risk behaviours: Results from the 2012 Global Drug Survey. Drug Alcohol Rev. 2015, 34, 427–437. [Google Scholar] [CrossRef]
- Chinet, L.; Stéphan, P.; Zobel, F.; Halfon, O. Party drug use in techno nights: A field survey among French-speaking Swiss attendees. Pharmacol. Biochem. Behav. 2007, 86, 284–289. [Google Scholar] [CrossRef] [PubMed]
- Taurah, L.; Chandler, C.; Sanders, G. Depression, impulsiveness, sleep, and memory in past and present polydrug users of 3,4-methylenedioxymethamphetamine (MDMA, ecstasy). Psychopharmacology 2014, 231, 737–751. [Google Scholar] [CrossRef]
- Connor, J.P.; Gullo, M.J.; White, A.; Kelly, A.B. Polysubstance use: Diagnostic challenges, patterns of use and health. Curr. Opin. Psychiatry 2014, 27, 269–275. [Google Scholar] [CrossRef] [Green Version]
- Arria, A.M.; Caldeira, K.M.; Bugbee, B.A.; Vincent, K.B.; O’Grady, K.E. Marijuana use trajectories during college predict health outcomes nine years post-matriculation. Drug Alcohol Depend. 2016, 159, 158–165. [Google Scholar] [CrossRef] [Green Version]
- Parrott, A.C. Why all stimulant drugs are damaging to recreational users: An empirical overview and psychobiological explanation. Hum. Psychopharmacol. 2015, 30, 213–224. [Google Scholar] [CrossRef]
- EMCDDA. European Drug Report 2020: Trends and Developments; EMCDDA: Lisbon, Portugal, 2020. [Google Scholar]
- EMCDDA. Sweden Country Drug Report 2019; European Monitoring Centre for Drugs and Drug Addiction: Lisbon, Portugal, 2019. [Google Scholar]
- Tossmann, P.; Boldt, S.; Tensil, M.D. The use of drugs within the techno party scene in European metropolitan cities. Eur. Addict. Res. 2001, 7, 2–23. [Google Scholar] [CrossRef]
- Winstock, A.R.; Griffiths, P.; Stewart, D. Drugs and the dance music scene: A survey of current drug use patterns among a sample of dance music enthusiasts in the UK. Drug Alcohol Depend. 2001, 64, 9–17. [Google Scholar] [CrossRef]
- Van Havere, T.; Vanderplasschen, W.; Lammertyn, J.; Broekaert, E.; Bellis, M. Drug use and nightlife: More than just dance music. Subst. Abuse Treat. Prev. Policy 2011, 6, 18. [Google Scholar] [CrossRef] [Green Version]
- Hesse, M.; Tutenges, S.; Schliewe, S. The use of tobacco and cannabis at an international music festival. Eur. Addict. Res. 2010, 16, 208–212. [Google Scholar] [CrossRef] [PubMed]
- Sañudo, A.; Andreoni, S.; Sanchez, Z.M. Polydrug use among nightclub patrons in a megacity: A latent class analysis. Int. J. Drug Policy 2015, 26, 1207–1214. [Google Scholar] [CrossRef]
- Palamar, J.J.; Keyes, K.M. Trends in drug use among electronic dance music party attendees in New York City, 2016–2019. Drug Alcohol Depend. 2020, 209, 107889. [Google Scholar] [CrossRef] [PubMed]
- Gripenberg Abdon, J.; Wallin, E.; Andréasson, S. The “Clubs against Drugs” program in Stockholm, Sweden: Two cross-sectional surveys examining drug use among staff at licensed premises. Subst. Abuse Treat. Prev. Policy 2011, 6, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gripenberg-Abdon, J.; Elgán, T.H.; Wallin, E.; Shaafati, M.; Beck, O.; Andréasson, S. Measuring substance use in the club setting: A feasibility study using biochemical markers. Subst. Abuse Treat. Prev. Policy 2012, 7, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buvik, K.; Bye, E.K.; Gripenberg, J. Alcohol and drug use among staff at licensed premises in Norway. Scand. J. Public Health 2019, 47, 393–399. [Google Scholar] [CrossRef]
- Nordfjærn, T.; Bretteville-Jensen, A.L.; Edland-Gryt, M.; Gripenberg, J. Risky substance use among young adults in the nightlife arena: An underused setting for risk-reducing interventions? Scand. J. Public Health 2016, 44, 638–645. [Google Scholar] [CrossRef]
- Bretteville-Jensen, A.L.; Burdzovic Andreas, J.; Gjersing, L.; Øiestad, E.L.; Gjerde, H. Identification and Assessment of Drug-User Groups Among Nightlife Attendees: Self-Reports, Breathalyzer-Tests and Oral Fluid Drug Tests. Eur. Addict. Res. 2019, 25, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Gjerde, H.; Gjersing, L.; Furuhaugen, H.; Bretteville-Jensen, A.L. Correspondence between Oral Fluid Drug Test Results and Self-Reported Illicit Drug Use among Music Festival Attendees. Subst. Use Misuse 2019, 54, 1337–1344. [Google Scholar] [CrossRef]
- Gjersing, L.; Bretteville-Jensen, A.L.; Furuhaugen, H.; Gjerde, H. Illegal substance use among 1309 music festival attendees: An investigation using oral fluid sample drug tests, breathalysers and questionnaires. Scand. J. Public Health 2019, 47, 400–407. [Google Scholar] [CrossRef]
- Van Havere, T.; Lammertyn, J.; Vanderplasschen, W.; Bellis, M.; Rosiers, J.; Broekaert, E. Illicit drug use in the flemish nightlife scene between 2003 and 2009. Eur. Addict. Res. 2012, 18, 153–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, P.; Curtis, A.; Jenkinson, R.; Droste, N.; Bowe, S.J.; Pennay, A. Drug use in Australian nightlife settings: Estimation of prevalence and validity of self-report. Addiction 2015, 110, 1803–1810. [Google Scholar] [CrossRef]
- Fernández-Calderón, F.; Cleland, C.M.; Palamar, J.J. Polysubstance use profiles among electronic dance music party attendees in New York City and their relation to use of new psychoactive substances. Addict. Behav. 2018, 78, 85–93. [Google Scholar] [CrossRef]
- Bijlsma, L.; Celma, A.; Castiglioni, S.; Salgueiro-González, N.; Bou-Iserte, L.; Baz-Lomba, J.A.; Reid, M.J.; Dias, M.J.; Lopes, A.; Matias, J.; et al. Monitoring psychoactive substance use at six European festivals through wastewater and pooled urine analysis. Sci. Total Environ. 2020, 725, 138376. [Google Scholar] [CrossRef] [PubMed]
- Di Forti, M.; Quattrone, D.; Freeman, T.P.; Tripoli, G.; Gayer-Anderson, C.; Quigley, H.; Rodriguez, V.; Jongsma, H.E.; Ferraro, L.; La Cascia, C.; et al. The contribution of cannabis use to variation in the incidence of psychotic disorder across Europe (EU-GEI): A multicentre case-control study. Lancet Psychiatry 2019, 6, 427–436. [Google Scholar] [CrossRef] [Green Version]
- Parrott, A.C. Human psychobiology of MDMA or “Ecstasy”: An overview of 25 years of empirical research. Hum. Psychopharmacol. 2013, 28, 289–307. [Google Scholar] [CrossRef]
- Rigg, K.K.; Sharp, A. Deaths related to MDMA (ecstasy/molly): Prevalence, root causes, and harm reduction interventions. J. Subst. Use 2018, 23, 345–352. [Google Scholar] [CrossRef]
- Mounteney, J.; Griffiths, P.; Bo, A.; Cunningham, A.; Matias, J.; Pirona, A. Nine reasons why ecstasy is not quite what it used to be. Int. J. Drug Policy 2018, 51, 36–41. [Google Scholar] [CrossRef]
- Vasica, G.; Tennant, C.C. Cocaine use and cardiovascular complications. Med. J. Aust. 2002, 177, 260–262. [Google Scholar] [CrossRef]
- Soar, K.; Parrott, A.; Turner, J. Attributions for psychobiological changes in ecstasy/MDMA and other polydrug users. J. Psychopharmacol. 2009, 23, 745–758. [Google Scholar] [CrossRef] [Green Version]
- Rodgers, J.; Buchanan, T.; Pearson, C.; Parrott, A.C.; Ling, J.; Hefferman, T.M.; Scholey, A.B. Differential experiences of the psychobiological sequelae of ecstasy use: Quantitative and qualitative data from an internet study. J. Psychopharmacol. 2006, 20, 437–446. [Google Scholar] [CrossRef]
- Parrott, A.C.; Hayley, A.C.; Downey, L.A. Recreational stimulants, herbal, and spice cannabis: The core psychobiological processes that underlie their damaging effects. Hum. Psychopharmacol. 2017, 32, e2594. [Google Scholar] [CrossRef] [Green Version]
- Harro, J. Neuropsychiatric adverse effects of amphetamine and methamphetamine. Int. Rev. Neurobiol. 2015, 120, 179–204. [Google Scholar] [CrossRef]
- Smith, G.W.; Farrell, M.; Bunting, B.P.; Houston, J.E.; Shevlin, M. Patterns of polydrug use in Great Britain: Findings from a national household population survey. Drug Alcohol Depend. 2011, 113, 222–228. [Google Scholar] [CrossRef]
- Quek, L.-H.; Chan, G.C.K.; White, A.; Connor, J.P.; Baker, P.J.; Saunders, J.B.; Kelly, A.B. Concurrent and simultaneous polydrug use: Latent class analysis of an Australian nationally representative sample of young adults. Front. Public Health 2013, 1, 61. [Google Scholar] [CrossRef] [Green Version]
- Grov, C.; Kelly, B.C.; Parsons, J.T. Polydrug use among club-going young adults recruited through time-space sampling. Subst. Use Misuse 2009, 44, 848–864. [Google Scholar] [CrossRef]
- Miller, B.A.; Byrnes, H.F.; Branner, A.C.; Voas, R.; Johnson, M.B. Assessment of club patrons’ alcohol and drug use: The use of biological markers. Am. J. Prev. Med. 2013, 45, 637–643. [Google Scholar] [CrossRef]
- Mohr, A.L.A.; Friscia, M.; Yeakel, J.K.; Logan, B.K. Use of synthetic stimulants and hallucinogens in a cohort of electronic dance music festival attendees. Forensic Sci. Int. 2018, 282, 168–178. [Google Scholar] [CrossRef] [PubMed]
- McKetin, R.; Chalmers, J.; Sunderland, M.; Bright, D.A. Recreational drug use and binge drinking: Stimulant but not cannabis intoxication is associated with excessive alcohol consumption. Drug Alcohol Rev. 2014, 33, 436–445. [Google Scholar] [CrossRef]
- Byrnes, H.F.; Miller, B.A.; Bourdeau, B.; Johnson, M.B. Impact of group cohesion among drinking groups at nightclubs on risk from alcohol and other drug use. J. Drug Issues 2019, 49, 668–679. [Google Scholar] [CrossRef]
- Palamar, J.J.; Acosta, P.; Le, A.; Cleland, C.M.; Nelson, L.S. Adverse drug-related effects among electronic dance music party attendees. Int. J. Drug Policy 2019, 73, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Calderón, F.; Vidal-Giné, C.; Rojas-Tejada, A.J.; Lozano-Rojas, Ó.M. Patterns of Simultaneous Polysubstance Use among Partygoers: Correlates and Differences in Adverse Acute Effects Experienced. J. Psychoact. Drugs 2020, 52, 344–356. [Google Scholar] [CrossRef] [PubMed]
- Wagner, D.; Koester, P.; Becker, B.; Gouzoulis-Mayfrank, E.; Hellmich, M.; Daumann, J. A longitudinal study of self-reported psychopathology in early ecstasy and amphetamine users. Psychopharmacology 2015, 232, 897–905. [Google Scholar] [CrossRef] [PubMed]
- Verheyden, S.L.; Maidment, R.; Curran, H.V. Quitting ecstasy: An investigation of why people stop taking the drug and their subsequent mental health. J. Psychopharmacol. 2003, 17, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Scott, L.A.; Roxburgh, A.; Bruno, R.; Matthews, A.; Burns, L. The impact of comorbid cannabis and methamphetamine use on mental health among regular ecstasy users. Addict. Behav. 2012, 37, 1058–1062. [Google Scholar] [CrossRef]
- Ogeil, R.P.; Rajaratnam, S.M.W.; Broadbear, J.H. Male and female ecstasy users: Differences in patterns of use, sleep quality and mental health outcomes. Drug Alcohol Depend. 2013, 132, 223–230. [Google Scholar] [CrossRef]
- Maxwell, J.C. Party drugs: Properties, prevalence, patterns, and problems. Subst. Use Misuse 2005, 40, 1203–1240. [Google Scholar] [CrossRef]
- Fernández-Calderón, F.; Díaz-Batanero, C.; Barratt, M.J.; Palamar, J.J. Harm reduction strategies related to dosing and their relation to harms among festival attendees who use multiple drugs. Drug Alcohol Rev. 2019, 38, 57–67. [Google Scholar] [CrossRef] [Green Version]
- Van Havere, T.; Vanderplasschen, W.; Broekaert, E.; De Bourdeaudhui, I. The influence of age and gender on party drug use among young adults attending dance events, clubs, and rock festivals in Belgium. Subst. Use Misuse 2009, 44, 1899–1915. [Google Scholar] [CrossRef]
- Parsons, J.T.; Grov, C.; Kelly, B.C. Club drug use and dependence among young adults recruited through time-space sampling. Public Health Rep. 2009, 124, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Ramo, D.E.; Grov, C.; Delucchi, K.; Kelly, B.C.; Parsons, J.T. Typology of club drug use among young adults recruited using time-space sampling. Drug Alcohol Depend. 2010, 107, 119–127. [Google Scholar] [CrossRef] [Green Version]
- Parsons, J.T.; Kelly, B.C.; Wells, B.E. Differences in club drug use between heterosexual and lesbian/bisexual females. Addict. Behav. 2006, 31, 2344–2349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strandberg, A.K.; Elgán, T.H.; Feltmann, K.; Jayaram Lindström, N.; Gripenberg, J. Illicit Drugs in the Nightlife Setting: Changes in Employee Perceptions and Drug Use over a Fifteen-Year Period. Subst. Use Misuse 2020, 55, 2116–2128. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, W. Mental health, sensation seeking and drug use patterns: A longitudinal study. Br. J. Addict. 1991, 86, 195–204. [Google Scholar] [CrossRef] [PubMed]
- Martin, C.A.; Kelly, T.H.; Rayens, M.K.; Brogli, B.R.; Brenzel, A.; Smith, W.J.; Omar, H.A. Sensation seeking, puberty, and nicotine, alcohol, and marijuana use in adolescence. J. Am. Acad. Child. Adolesc. Psychiatry 2002, 41, 1495–1502. [Google Scholar] [CrossRef]
- Yanovitzky, I. Sensation seeking and adolescent drug use: The mediating role of association with deviant peers and pro-drug discussions. Health Commun. 2005, 17, 67–89. [Google Scholar] [CrossRef]
- Palamar, J.J.; Acosta, P.; Sherman, S.; Ompad, D.C.; Cleland, C.M. Self-reported use of novel psychoactive substances among attendees of electronic dance music venues. Am. J. Drug Alcohol Abuse 2016, 42, 624–632. [Google Scholar] [CrossRef] [Green Version]
- Hesse, M.; Tutenges, S. Music and substance preferences among festival attendants. Drugs Alcohol Today 2012, 12, 82–88. [Google Scholar] [CrossRef]
- Schierenbeck, T.; Riemann, D.; Berger, M.; Hornyak, M. Effect of illicit recreational drugs upon sleep: Cocaine, ecstasy and marijuana. Sleep Med. Rev. 2008, 12, 381–389. [Google Scholar] [CrossRef]
- Nnadi, C.U.; Mimiko, O.A.; McCurtis, H.L.; Cadet, J.L. Neuropsychiatric effects of cocaine use disorders. J. Natl. Med. Assoc. 2005, 97, 1504–1515. [Google Scholar]
- O’Brien, M.S.; Wu, L.-T.; Anthony, J.C. Cocaine use and the occurrence of panic attacks in the community: A case-crossover approach. Subst. Use Misuse 2005, 40, 285–297. [Google Scholar] [CrossRef]
- Müller, F.; Brändle, R.; Liechti, M.E.; Borgwardt, S. Neuroimaging of chronic MDMA (“ecstasy”) effects: A meta-analysis. Neurosci. Biobehav. Rev. 2019, 96, 10–20. [Google Scholar] [CrossRef]
- Bellis, M.A.; Hughes, K.; Calafat, A.; Juan, M.; Ramon, A.; Rodriguez, J.A.; Mendes, F.; Schnitzer, S.; Phillips-Howard, P. Sexual uses of alcohol and drugs and the associated health risks: A cross sectional study of young people in nine European cities. BMC Public Health 2008, 8, 155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calafat, A.; Blay, N.; Juan, M.; Adrover, D.; Bellis, M.A.; Hughes, K.; Stocco, P.; Siamou, I.; Mendes, F.; Bohrn, K. Traffic risk behaviors at nightlife: Drinking, taking drugs, driving, and use of public transport by young people. Traffic Inj. Prev. 2009, 10, 162–169. [Google Scholar] [CrossRef]
- Schnitzer, S.; Bellis, M.A.; Anderson, Z.; Hughes, K.; Calafat, A.; Juan, M.; Kokkevi, A. Nightlife violence: A gender-specific view on risk factors for violence in nightlife settings: A cross-sectional study in nine European countries. J. Interpers. Violence 2010, 25, 1094–1112. [Google Scholar] [CrossRef] [PubMed]
- Gripenberg Abdon, J.; Wallin, E.; Andréasson, S. Long-term effects of a community-based intervention: 5-year follow-up of “Clubs against Drugs”. Addiction 2011, 106, 1997–2004. [Google Scholar] [CrossRef] [PubMed]
- Holder, H.D. Community prevention of alcohol problems. Addict. Behav. 2000, 25, 843–859. [Google Scholar] [CrossRef]
- Holder, H.D. Alcohol and the Community: A Systems Approach to Prevention; Cambridge University Press: Cambridge, UK, 1998; ISBN 9780521035040. [Google Scholar]
- Wallin, E.; Andreásson, S. Can I have a beer, please? A study of alcohol service to young adults on licensed premises in Stockholm. Prev. Sci. 2004, 5, 221–229. [Google Scholar] [CrossRef]
- Månsdotter, A.M.; Rydberg, M.K.; Wallin, E.; Lindholm, L.A.; Andréasson, S. A cost-effectiveness analysis of alcohol prevention targeting licensed premises. Eur. J. Public Health 2007, 17, 618–623. [Google Scholar] [CrossRef] [Green Version]
- Wallin, E.; Gripenberg, J.; Andréasson, S. Overserving at licensed premises in Stockholm: Effects of a community action program. J. Stud. Alcohol 2005, 66, 806–814. [Google Scholar] [CrossRef]
- Trolldal, B.; Haggård, U.; Guldbrandsson, K. Factors associated with implementation of a multicomponent responsible beverage service program--results from two surveys in 290 Swedish municipalities. Subst. Abuse Treat. Prev. Policy 2013, 8, 11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurtz, S.P.; Buttram, M.E.; Pagano, M.E.; Surratt, H.L. A randomized trial of brief assessment interventions for young adults who use drugs in the club scene. J. Subst. Abuse Treat. 2017, 78, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Dick, S.; Whelan, E.; Davoren, M.P.; Dockray, S.; Heavin, C.; Linehan, C.; Byrne, M. A systematic review of the effectiveness of digital interventions for illicit substance misuse harm reduction in third-level students. BMC Public Health 2019, 19, 1244. [Google Scholar] [CrossRef] [Green Version]
- Arnaud, N.; Baldus, C.; Elgán, T.H.; De Paepe, N.; Tønnesen, H.; Csémy, L.; Thomasius, R. Effectiveness of a Web-Based Screening and Fully Automated Brief Motivational Intervention for Adolescent Substance Use: A Randomized Controlled Trial. J. Med. Internet Res. 2016, 18, e103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnaud, N.; Bröning, S.; Drechsel, M.; Thomasius, R.; Baldus, C. Web-based screening and brief intervention for poly-drug use among teenagers: Study protocol of a multicentre two-arm randomized controlled trial. BMC Public Health 2012, 12, 826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnaud, N.; Baldus, C.; Elgán, T.H.; Tønnesen, H.; Paepe, N.D.; Csemy, L.; Thomasius, R. Moderators of Outcome in a Web-Based Substance Use Intervention for Adolescents. Sucht 2015, 61, 377–387. [Google Scholar] [CrossRef]
- Feltmann, K.; Elgán, T.H.; Gripenberg, J. High levels of alcohol intoxication and strong support for restrictive alcohol policies among music festival visitors. Subst. Abuse Treat. Prev. Policy 2019, 14, 15. [Google Scholar] [CrossRef] [Green Version]
- Waldron, J.; Grabski, M.; Freeman, T.P.; Mokrysz, C.; Hindocha, C.; Measham, F.; van Beek, R.; van der Pol, P.; Hauspie, B.; Dirkx, N.; et al. How do online and offline sampling compare in a multinational study of drug use and nightlife behaviour? Int. J. Drug Policy 2020, 82, 102812. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Characteristics | % (n) |
|---|---|
| Gender | |
| Male | 72.3 (991) |
| Female | 25.9 (355) |
| Other | 1.8 (25) |
| Occupation 1,4 | |
| Full time work | 44.7 (613) |
| Part time work | 18.0 (247) |
| Student | 37.2 (510) |
| Neither education, employment, nor training | 5.7 (78) |
| Urbanicity 1 | |
| Large town/city | 60.8 (834) |
| Small to mid-sized town | 29.6 (406) |
| Rural/countryside | 7.9 (108) |
| Education 2,4 | |
| Completed primary school | 97.2 (1333) |
| Currently attending high school | 6.7 (92) |
| Completed high school | 90.7 (1244) |
| Currently attending university | 29.0 (397) |
| Completed university degree | 23.0 (316) |
| Relationship status 1 | |
| Single | 51.7 (709) |
| Married or in a civil partnership | 3.3 (45) |
| Divorced or separated | 0.5 (7) |
| In a relationship, not living with partner | 17.7 (242) |
| In a relationship and living with partner | 25.2 (345) |
| Sexual orientation 3 | |
| Men attracted to women | 67.5 (926) |
| Women attracted to men | 19.5 (268) |
| Women attracted equally to men and women | 3.7 (51) |
| Men attracted to men | 2.3 (31) |
| Women attracted to women | 1.1 (15) |
| Men attracted equally to men and women | 0.9 (12) |
| Women not attracted to either men or women | 0.1 (2) |
| Substance | Lifetime % (n) | Last 12 Months % (n) |
|---|---|---|
| Synthetic Cannabinoids | 16.0 (219) | 1.1 (15) |
| Synthetic Hallucinogens | 14.1 (193) | 5.3 (73) |
| Prescription Opioids | 13.9 (190) | 7.1 (97) |
| DMT 1 | 8.8 (120) | 3.9 (53) |
| Mephedrone | 5.0 (68) | 0.5 (7) |
| GHB 2 | 3.4 (47) | 1.5 (21) |
| Synthetic Dissociatives | 3.3 (45) | 0.7 (10) |
| 4-FA/4-FMP 3 | 2.0 (27) | 1.0 (14) |
| Heroin | 1.5 (20) | 0.4 (5) |
| Substance (n Respondents) | Night- Clubs | Pub/ Bars | Licensed Festivals | Illegal Festivals | Public Spaces | House Party 1 | At Home 2 |
|---|---|---|---|---|---|---|---|
| Cannabis (692) 3 | 0.6 | 0.7 | 3.2 | 3.2 | 8.5 | 14.9 | 65.0 |
| Ecstasy (498) 4 | 19.1 | 0.2 | 26.9 | 35.1 | 0.2 | 8.6 | 8.4 |
| Cocaine (380) 5 | 38.9 | 7.6 | 7.6 | 10.3 | - | 24.5 | 9.2 |
| Amphetamine (311) 6 | 17.4 | 3.9 | 12.2 | 29.6 | 1.9 | 11.3 | 15.1 |
| LSD (214) 7 | 2.8 | - | 10.7 | 8.9 | 10.7 | 2.3 | 60.3 |
| Mushrooms (173) 8 | 1.2 | 0.6 | 8.1 | 6.4 | 18.5 | 9.2 | 49.7 |
| Ketamine (149) | 13.4 | 1.3 | 20.1 | 24.2 | 1.3 | 16.8 | 22.8 |
| Drug Use during the Last 12 Months | Males % (n) | Females % (n) | X2 (df = 1), p-Value |
|---|---|---|---|
| Any illicit drug | 56.4 (559) | 64.8 (230) | 7.57, 0.006 |
| Cannabis | 49.8 (494) | 53.5 (190) | 1.41, 0.235 |
| Ecstasy | 34.7 (344) | 42.5 (151) | 6.88, 0.009 |
| Cocaine | 26.2 (260) | 32.7 (116) | 5.39, 0.020 |
| Amphetamine | 21.3 (211) | 26.8 (95) | 4.45, 0.035 |
| LSD | 15.4 (153) | 15.5 (55) | 0.00, 0.981 |
| Magic Mushrooms | 12.4 (123) | 12.7 (45) | 0.02, 0.897 |
| Ketamine | 10.0 (99) | 13.0 (46) | 2.40, 0.122 |
| Factors | Wald | OR | 95% CI | p-Value |
|---|---|---|---|---|
| Age | 3.00 | 0.97 | 0.94–1.00 | 0.083 |
| Gender | 3.05 | 0.76 | 0.57–1.03 | 0.081 |
| Occupation | ||||
| Full time work | 0.02 | 1.03 | 0.66–1.61 | 0.902 |
| Part time work | 2.02 | 1.36 | 0.89–2.09 | 0.155 |
| Student | 0.10 | 0.93 | 0.59–1.48 | 0.757 |
| Higher education 1 | 1.31 | 0.519 | ||
| Number of events attended 2 | 0.14 | 1.00 | 1.00–1.01 | 0.705 |
| Ever visited an illegal festival | 110.29 | 4.77 | 3.56–6.38 | <0.001 |
| Visited club ≥ monthly 2 | 0.96 | 0.86 | 0.63–1.17 | 0.328 |
| Visited legal festival ≥ monthly 2 | 0.65 | 1.17 | 0.80–1.70 | 0.420 |
| Visited pub ≥ monthly 2 | 2.12 | 1.29 | 0.92–1.82 | 0.146 |
| Visited house party ≥ monthly 2 | 0.24 | 0.93 | 0.71–1.23 | 0.626 |
| Tobacco consumption ever | 14.92 | 2.14 | 1.45–3.14 | <0.001 |
| Alcohol at least fortnightly 2 | 5.19 | 1.48 | 1.06–2.08 | 0.023 |
| Tobacco at least fortnightly 2 | 37.79 | 2.52 | 1.88–3.38 | <0.001 |
| Motives to go out 3: | ||||
| Friends are going | 0.03 | 0.97 | 0.70–1.36 | 0.875 |
| To meet new people | 0.83 | 0.88 | 0.67–1.16 | 0.363 |
| To seek excitement | 21.50 | 1.99 | 1.49–2.67 | <0.001 |
| To open up to friends | 0.05 | 1.03 | 0.78–1.36 | 0.824 |
| To drink alcohol | 0.02 | 0.98 | 0.73–1.31 | 0.889 |
| To escape daily life | 7.16 | 1.46 | 1.11–1.93 | 0.007 |
| To explore mind | 4.25 | 1.38 | 1.02–1.87 | 0.039 |
| To cope with problems | 0.84 | 0.87 | 0.64–1.18 | 0.361 |
| To see an artist | 7.06 | 0.64 | 0.46–0.89 | 0.008 |
| Experienced Consequences (n Respondents) | Percentage of Respondents | Median (Interquartile Range) |
|---|---|---|
| Enhanced perception, enjoyment of music (755) | 95.4 | 8 (6–10) |
| Closeness to others (716) | 95.0 | 7 (5–9) |
| Feelings of love and empathy (747) | 94.9 | 7 (5–9) |
| Intense pleasure (741) | 94.6 | 7 (5–9) |
| Making new friends (704) | 92.0 | 6 (4–8) |
| Expanded consciousness (693) | 91.5 | 6 (4–8) |
| Reduced inhibitions (671) | 91.1 | 5 (3–7) |
| Increased sense of enlightenment (652) | 90.2 | 6 (3–8) |
| Low mood or anxiety in days afterwards (564) | 77.8 | 3 (2–5) |
| Memory loss (570) | 76.1 | 3 (2–5) |
| Agitation (530) | 74.2 | 3 (2–5) |
| Spending money you cannot afford to (481) | 64.7 | 3 (2–5) |
| Problems with sleep in days after use (443) | 60.7 | 2 (1–5) |
| Effect of the drug not as expected (417) | 60.0 | 2 (1–3) |
| Vomiting (464) | 58.8 | 2 (1–3) |
| Palpitations (436) | 58.5 | 2 (1–4) |
| Overheating (421) | 58.4 | 2 (1–4) |
| Panic attacks or anxiety (452) | 57.1 | 2 (1–3.25) |
| Driven/been driven by someone under the influence of alcohol/drugs (373) | 45.0 | 2 (1–3) |
| Arguments with friends (367) | 44.7 | 1 (1–3) |
| Sexual activity you later regret (367) | 40.3 | 2 (1–4) |
| Aggression/victim of aggression (372) | 39.8 | 1 (1–3) |
| Accidents (374) | 38.2 | 1 (1–2) |
| Missing work or important commitments (361) | 38.2 | 2 (1–4) |
| Breathing difficulties (346) | 31.5 | 1 (1–3) |
| Legal problems (e.g., being arrested) (320) | 27.8 | 2 (1–4) |
| Problems with a bouncer (314) | 27.4 | 1 (1–4) |
| Inability to move (298) | 24.8 | 1.5 (1–3) |
| Fainting or collapsing (310) | 20.0 | 1 (1–2) |
| Seeking or receiving emergency medical treatment (287) | 15.3 | 1 (1–3) |
| DUDIT 1–2 | Never | ≤Monthly | 2–4 Times a Month | 2–3 Times a Week | ≥4 Times a Week |
| Drug use 1 frequency | 13.4 | 52.5 | 19.0 | 6.1 | 9.0 |
| Polydrug use 2 | 40.7 | 46.7 | 10.1 | 1.6 | 0.9 |
| DUDIT 3 | None | 1–2 Times | 3–4 Times | 5–6 Times | ≥7 Times |
| Times drug taking 3 | 12.4 | 65.8 | 15.4 | 4.3 | 2.1 |
| DUDIT 4–9 | Never | <Monthly | Monthly | Weekly | Daily |
| Heavily influenced | 27.1 | 54.6 | 12.7 | 4.2 | 1.5 |
| Strong craving that cannot be resisted | 75.5 | 16.9 | 4.5 | 1.6 | 1.6 |
| Unable to stop once started 4 | 82.7 | 11.9 | 3.4 | 0.9 | 1.1 |
| Neglected to do something 4 | 61.1 | 29.2 | 6.4 | 2.7 | 0.6 |
| Drug morning after use 4 | 84.5 | 10.5 | 3.1 | 1.1 | 0.8 |
| Guilt, bad conscience 4 | 51.6 | 37.2 | 6.6 | 3.1 | 1.3 |
| DUDIT 10–11 | No | Yes, but not over the Past Year | Yes, over the Past Year | ||
| Hurt 5 yourself or others | 77.4 | 14.6 | 8.0 | ||
| Advice to stop 6 | 67.9 | 19.0 | 13.0 | ||
| DUDIT Drugs | % (n) |
|---|---|
| No response | 6 (53) |
| Cannabis | 43.6 (388) |
| Ecstasy | 15.9 (141) |
| Alcohol 1 | 11.0 (98) |
| Amphetamine | 7.1 (63) |
| Cocaine | 7.0 (62) |
| Nitrous oxide | 2.2 (20) |
| Tobacco 1 | 1.6 (14) |
| LSD | 1.2 (11) |
| Prescription Opioids | 0.8 (7) |
| Heroin/Opiates | 0.7 (6) |
| Ketamine | 0.6 (5) |
| Magic Mushrooms | 0.3 (3) |
| Benzodiazepines | 0.3 (3) |
| Others 2 | 1.7 (15) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feltmann, K.; Elgán, T.H.; Strandberg, A.K.; Kvillemo, P.; Jayaram-Lindström, N.; Grabski, M.; Waldron, J.; Freeman, T.; Curran, H.V.; Gripenberg, J. Illicit Drug Use and Associated Problems in the Nightlife Scene: A Potential Setting for Prevention. Int. J. Environ. Res. Public Health 2021, 18, 4789. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094789
Feltmann K, Elgán TH, Strandberg AK, Kvillemo P, Jayaram-Lindström N, Grabski M, Waldron J, Freeman T, Curran HV, Gripenberg J. Illicit Drug Use and Associated Problems in the Nightlife Scene: A Potential Setting for Prevention. International Journal of Environmental Research and Public Health. 2021; 18(9):4789. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094789
Chicago/Turabian StyleFeltmann, Kristin, Tobias H. Elgán, Anna K. Strandberg, Pia Kvillemo, Nitya Jayaram-Lindström, Meryem Grabski, Jon Waldron, Tom Freeman, Helen Valerie Curran, and Johanna Gripenberg. 2021. "Illicit Drug Use and Associated Problems in the Nightlife Scene: A Potential Setting for Prevention" International Journal of Environmental Research and Public Health 18, no. 9: 4789. https://0-doi-org.brum.beds.ac.uk/10.3390/ijerph18094789